1. Introduction
The COVID-19 pandemic presented unprecedented challenges to youth mental health. The Centers for Disease Control and Prevention [
1] of the United States conducted research on the impact of the COVID-19 pandemic on high school students’ mental health. The CDC found that a high percentage of high school students reported experiencing mental health challenges during the peak of the pandemic in 2020, and a 2021 follow-up survey found that the students were still experiencing significant mental health and well-being challenges. Additionally, longitudinal data revealed that the percentages of high school students experiencing poor mental health, persistent feelings of hopelessness, and suicide attempts and suicidal thoughts were significantly higher in 2021 compared to 2013 [
1]. These types of trends are not isolated to high school students; as one example, Shanaker et al. [
2] also found that mental health emergency department visits in children 5–17 years old with a mental health diagnosis increased by 27% early in the pandemic, followed by a 4% monthly increase through February 2021.
In order to prevent and address the concerning youth mental health needs, the National Academies of Science, Engineering, and Medicine [
3] outlines a continuum of care for mental, emotional, and behavioral interventions that begins with promotion, continues to prevention, followed by treatment, and ends with maintenance. For promotion, societal, community, individual, and family tools are recommended to foster mental, emotional, and behavioral health. For prevention, universal, selective, and indicated tools are recommended to improve MEB development and health. For instance, prevention strategies can be universally designed to teach social and emotional skills through curriculums that promote cognitive-behavioral and mindfulness practices, as well as skill-based strategies that focus on reducing risky behaviors such as bullying, substance use, and suicidal thoughts. Prevention strategies also include the establishment of positive school environments to assist teachers, staff, and school culture to implement anti-discriminatory disciplinary practices while also providing resources to low socioeconomic families. The treatment component includes case identification and treatment of disorders, while the maintenance component focuses on long-term treatment and after-care. A Student Assistance Program (SAP) is one service delivery mechanism for schools and community partners to systematically deliver such a continuum to support wellness for all students.
2. Student Assistance Programs
A SAP is a comprehensive school-based framework for providing a variety of prevention and intervention supports to youth to reduce non-academic barriers to learning and improve mental and behavioral health [
4]. Developed out of the Employee Assistance Model, SAP services typically involve a team to support planning, problem-solving, and case management, as well as a system to provide education, prevention, early identification, referral, intervention, and guided support services [
4]. Although study design limitations prevent causal conclusions from being drawn, previous research suggests that SAPs have been associated with improved academic achievement [
5]; social skills, school bonding, and relationships [
6]; and attendance and graduation status [
7]. Furthermore, SAP implementation has been associated with decreased antisocial behavior [
6], substance use [
5,
6,
8], suspensions [
7,
8], and arrests [
8].
SAMHSA recommends that schools integrate and align their SAP with existing school initiatives [
4]. For instance, MTSS is a proactive framework that schools can adopt to support students’ academic and social–emotional needs through screening, progress monitoring, a multi-tiered prevention system, and data-based decision-making [
9]. MTSS is often thought of as an umbrella that “houses” and aligns various tiered service delivery models such as Positive Behavioral Interventions and Supports (PBIS) and Response to Intervention (RTI) [
10]. Importantly, a SAP can also use an MTSS to organize the continuum of care. As shown in
Table 1, this often involves providing services within three tiers of support, based on the intensity and types of student needs. It has been recommended within the Positive Behavioral Interventions and Supports (PBIS) framework that approximately 80% of students receive Tier 1 supports alone, 15% of students would benefit from Tier 2 supports, and 5% of students are in need of Tier 3 intervention and services [
11]. However, more recently, Weist et al. [
12] recommend that schools adjust expectations given the rising mental health need that was exacerbated by the COVID-19 pandemic and prepare for higher proportions of youth with intensive mental health needs. The authors also noted the fluidity in needs across schools and communities and recommended flexibility in tiered supports based on identified needs.
In addition to using a tiered system, SAPs can be aligned with other school-wide initiatives such as PBIS, Restorative Practices, Social–Emotional Learning (SEL), and wellness programming. To use PBIS as an example, when aligned and integrated, a SAP has the potential to enhance PBIS outcomes through a more significant emphasis on Tier 2 and 3, along with a greater focus on substance use disorders or internalizing mental health concerns [
13]. In order to ensure a SAP is aligned with and integrated with other initiatives, it is necessary to identify connections between and among programs and to consider the ways in which a SAP can strengthen existing services (e.g., through a more intense focus on Tier 3, mental health, and wellness supports). Furthermore, if it is necessary to retain multiple teams to lead different programs or initiatives in the school, it can be helpful to identify a liaison from each to facilitate effective communication across teams and initiatives.
In order to ensure the effective planning, implementation, evaluation, and alignment of SAP processes, it is recommended that any school implementing a SAP have a leadership team to guide the efforts. Often referred to as a Student Assistance Team (SAT), this team meets regularly to review referrals, gather information, develop strategies, and link students to interventions, while also providing support and follow-up services [
13]. It is recommended that this team is composed of at least four members including an administrator and other relevant school staff (e.g., teacher, counselor, psychologist, nurse, social worker). Additionally, liaisons from county behavioral health and drug and alcohol systems may also attend meetings to ensure collaboration and continuity of care [
13]. Typically, the SAT would play an important role in planning for the universal screening processes and integrated systems that we will discuss next.
2.1. Universal Screening
SAPs typically rely on referral and early warning system data to identify students for additional support [
14]; however, recently the Ohio SAP model recommended integrating universal social, emotional, and behavioral (SEB) screening into SAP procedures [
13]. Universal screening involves systematically assessing the social, emotional, and/or behavioral functioning of all students in a population with the goal of identifying students who would benefit from additional support [
15]. When schools collect universal screening data, the results can also be used to guide and evaluate Tier 1 efforts. Eklund and Dowdy [
16] examined the added benefit of universal screening in a sample of elementary students and found that the majority of students identified with social, emotional, and behavioral risk were not identified on traditional referral methods. Universal screening promotes early identification and intervention rather than waiting for the need to intensify and warrant a referral to the SAP.
Although universal screening offers promise for SAP early identification efforts, previous research has noted several planning and implementation barriers. For instance, Bruhn et al. [
17] surveyed school administrators about universal screening practices and found that only 13% reported conducting universal social, emotional, and behavioral screening, and that access and awareness barriers prevented implementation (e.g., lack of resources, access to screening tools, support systems for identified students, lack of awareness about screening). Based on these findings, schools would benefit from additional support, guidance, and decision-making models for conducting universal screening and accessing resources.
In addition to the lack of implementation and barriers, administering universal screening in and of itself may not lead to additional students receiving interventions and support. Splett et al. [
18] followed intervention practices for six elementary schools initially conducting universal screening and found that many students identified on the social, emotional, and behavioral screening measures still did not receive services by the end of the year, particularly students with low-to-moderate risk who were well-suited for Tier 2 early intervention. The authors noted the need to attend to implementation factors and decision-making models for using the data. To support schools in using results to guide intervention decisions, Romer et al. [
15] recommend that schools proactively develop a protocol for how the screening data will be used to identify students and offer support. For instance, protocols can indicate when the data will be reviewed, thresholds or cut-offs for identifying concerns, which data will be used, and follow-up actions. Most importantly, results should be used to guide the continuum of support.
When planning a SAP within an MTSS, it is critical to use data-based decision-making to support strategic prevention planning alongside early identification and referral systems. Universal screening data provide one such mechanism to aid in systematic data-based decision-making. However, with previous research noting screening implementation barriers and difficulty serving newly identified students, additional examples of schools successfully conducting universal screening and using the results to implement a continuum of support post-COVID-19 are warranted.
2.2. Integrated Systems
In addition to challenges in conducting universal screening, SAPs within an MTSS face difficulties with the bifurcated systems of schools and community-based supports. Given that youth mental health support incorporates schools, community mental health organizations, and primary-care providers, there are inherent differences in their goals, processes, cultures, legal obligations, and funding systems [
19,
20]. These differences result in separate systems for screening, referral, and intervention/treatment that can hinder the ability to offer a continuum of mental health services to youth and families. As such, previous research has found that many referred students do not receive services and support [
21,
22] and that providing mental health services in schools increases the likelihood of a successful referral, as youth are six times more likely to receive mental health support in schools compared to community settings [
23].
The Interconnected Systems Framework model was developed to address these challenges and support the systematic integration of school mental health systems and services with PBIS systems and school practices [
24]. The Interconnected Systems Framework Implementation Guide [
24] describes the importance of developing a single system of delivery that integrates education and mental/behavioral health systems. In this system, multi-disciplinary teams, representing both school and community-based providers, use data to plan and implement a continuum of evidence-based mental health supports. The ISF further recommends developing a single Request for Assistance process for identifying and referring students who would benefit from additional school and/or community-based support.
3. Purpose
Given the challenges of implementing a wellness MTSS within a SAP, it is critical to proactively develop an integrated system that promotes data-based decision-making. In a school district and building, disjointed systems often compete for time, energy, and resources. This fragmented approach leads to ineffective processes that hinder a school’s ability to deliver prevention, identify student needs and risks early, link students to a continuum of supports, and provide guided support and maintenance.
The purpose of this article is to provide a case example of Marysville Exempted Village School District’s efforts to use a SAP as a service delivery model to integrate systems and data to deliver a continuum of support. With the rising mental health need that was exacerbated by COVID-19 [
25], describing one district’s model with screening and intervention data can assist other schools in planning their own continuum of support within a SAP. The goal is to elucidate the process of systems change within a SAP framework and highlight systematic data-based decision-making and integrative systems. We will also report the percentages of students who are identified on wellness benchmarking and screening tools in addition to the percentage referred for additional support. Next, we will provide a case example of an integrative systems approach to supporting student wellness.
4. Case Example
Context and Participants
This case example took place in one suburban school district in the Midwest. The school district has five elementary schools (K-4), one intermediate school (5–6), one middle school (7–8), one high school (9–12), and one Science, Technology, Engineering and Mathematics early college high school (9–12). With 5285 students, the majority of students are white and non-Hispanic (82.2%), followed by the next majority being Hispanic (6.7%). In 2022–2023, 19.4% of students were reported to be economically disadvantaged, 17.7% of students had disabilities, and 1.8% of students were English Language Learners. The student attendance rate is 93.5% while the graduation rate is 97.8%. The district employs over 300 teachers and 200 additional support staff (e.g., custodians, administrative staff, bus drivers). The employee attendance rate is 93.4% with an average of 15 years of experience. The district mission is to “Innovate—Collaborate—Inspire” and the vision is that “Each child at Marysville Schools will be challenged, prepared, and empowered through innovation, collaboration, and inspiration. Innovation to ignite their curiosity, collaboration to strengthen their capacity, inspiration to empower their confidence and fortitude toward the future”.
Prior to 2017–2018, the district used an informal approach to student wellness where students were referred to counseling support during times of crisis or high needs. This resulted in a reactive approach that relied on perception rather than data. Further, supports were fragmented, and follow-up for referred students was not systematic and consistent. In 2017–2018, several school and community suicides, in addition to experiencing success with academic MTSS frameworks, prompted the district to take a more systematic approach to student wellness.
To improve wellness, the district created an SEL wellness steering committee that included the principal, intervention specialist, classroom teachers, school psychologist, school counselor, occupational therapist, and speech–language pathologist representation. A total of 28 different K-12 staff served on the steering team. To develop a strategic approach to student wellness, the committee first created a mission and vision of “every student at Marysville Schools will have a felt sense of safety, hope, and agency, opportunities to develop character traits and assets, experience a personal sense of belonging within the school community, and the desire to be the most that they can be”. The committee identified key tenants and concepts that would promote the mission and vision including safe spaces and structures, supportive climate and culture, character and asset development, and school connectedness. This new approach prioritized programming and planning driven by data (universal screening and diagnostic data), differentiated and diffused individualized intervention, systems coordination, and prevention programming and evidence-based practices.
In the next section, we will describe the systematic integrative SAP approach that occurred during the 2022–2023 school year. We will organize activities according to the Interconnected Systems Framework components of an integrated system, a continuum of supports with mechanisms for data-based decision-making, and program evaluation [
24].
5. Integrated System Features
Several organizational structures and systems were in place to guide and support the systematic approach. First, staffing and leadership were key features. After the steering committee outlined the vision and key concepts, the district Director of Continuous Improvement led efforts to enact the vision. This coordinator is responsible for directing, coordinating, and provisioning academic and non-academic support and intervention services.
In addition to the Director of Continuous Improvement, School Navigators were critical personnel. A local behavioral health agency, Maryhaven, hired and supervised School Navigators who were embedded in school buildings as contracted staff members at a ratio of 1:1600 students. The district used cost sharing between the school district, Maryhaven, and the county mental health and recovery board. To overcome typical barriers to outside providers working in schools, the district provided office spaces within the buildings that they served, equipped with technology and Student Information System (SIS) access. When possible, the School Navigators provided extended hours to meet the needs of working caregivers. The expected responsibilities included case management with students receiving therapeutic services; screenings, diagnostics, and risk assessment; crisis response and management; brief intervention and prevention; and communication and collaboration with administrators and School Counselors for care coordination (as allowed with releases of information).
In 2021–2022, the district served as one of 80 pilot schools/districts for the Ohio School Wellness Initiative to test and initially implement the Ohio SAP and Staff Wellness model frameworks. Through serving as a pilot school, Marysville received a stipend, participated in regular regional communities of practice meetings, attended conferences and trainings, and received resources and guidance on the Ohio model frameworks. To support the SAP, the Director of Continuous Improvement served as the SAP Coordinator for the district, and each school building created a Care Coordination team (analogous to a Student Assistance Team) that typically included the School Counselor, School Psychologist, School Navigator, administrator representation, and teacher personnel (when relevant). The district focused on creating multiple pathways to support. This team completed a screening review, conducted referral intake, initiated the triage process, scoped supports, and monitored progress. For each student that was identified for care coordination, one person from the team was identified as the case manager. This case manager collected caregiver consent and led the follow-up process, including calling or meeting with the family. In order to encourage parental/guardian involvement, the district created parent resources and guidance, such as a guidebook and curated relevant resources, that were distributed to parents during the follow-up process.
To support the sustainability of the SAP within an MTSS, the district created a fiscally lean approach with competitive and braided funding streams. For instance, the district applied for and received state and federal grants, used county mental health and recovery funding, and used district permanent improvement funds. Specifically, the district worked with the Mental Health and Recovery Board of Union County to provide information and data for competitive grants, and the ESSR and Ohio Department of Education Wellness Funds were used to purchase materials, curriculum, and software. Further, the Mental Health and Recovery Board of Union County often purchased training materials.
6. Continuum of Support
Below we will describe the general continuum of supports for 2022–2023, although specific practices varied by building. We use the MTSS framework to present and organize activities.
6.1. Universal Prevention
Prevention Tier 1 programming was centered on the universal development of self-regulation, interpersonal effectiveness, distress tolerance, mindfulness, emotional regulation, and suicide prevention. The leadership team outlined specific programs that aligned with district wellness goals and priorities. For instance, the Signs of Suicide Curriculum [
26] was implemented with 6th–9th-grade students, Too Good for Drugs [
27] was implemented with 4th–6th-grade students, DBT Skills in Schools [
28,
29] was implemented with 5th–6th-grade students, and Second Step [
30] was implemented for 7th–8th-grade students. Further, buildings offered PAX Training Tools [
31] on an ad-hoc basis for parents/caregivers, and the Director of Continuous Improvement provided K-6 teachers with SEL Kernels [
32] materials from EASEL Labs.
For grades K-4, the district used Ohio SEL state learning standards [
33] to develop critical learning targets with a teacher guide and SEL-aligned learning progressions, assessment methods, activities and lessons, teaching practices, and book lists. This systematic approach to SEL prevention programming mimics the clear planning process for academic learning targets [
34].
6.2. Tier 1 Data Collection
To monitor Tier 1 needs and identify students for Tier 2 and 3 support, the district used a bifurcated process that allowed for a referral to be submitted at any point but also administered universal screenings that occurred at regular intervals (fall, winter, spring). Specifically, universal screening was administered to all students; suicide risk screening was completed in select grade levels; and parents, staff, or students could complete a referral form. To obtain parental consent for these screenings, the district provided a comprehensive opt-out process to parents at the beginning of each school year that allowed families to opt their child out of all non-academic, non-state required programming (e.g., suicide prevention and screening, social–emotional curricula, substance use, and abuse prevention). Below we will discuss each of these Tier 1 data collection approaches in more detail.
7. Universal Screening K-6: SELweb
The district administered the SELweb Early Elementary [
35] to all kindergarten-3rd-grade students and the Late Elementary version was administered to 4th–6th-grade students. SELweb is a computer-based diagnostic performance-based assessment of social and emotional competence. Students complete the assessment in approximately 30–40 min. For the Early Elementary version, there are four subtests: Emotion Recognition, Social Perspective-Taking, Social Problem-Solving, and Self-Control, whereas the Late Elementary version includes Understanding Others, Social Problem-Solving, Self-Control, and Self-Awareness subtests [
35]. SELweb provides an overall SEL score and subtest scores in a standard score format with a mean of 100 and a standard deviation of 15. Scores at or above 115 indicate “well above average” performance, scores between 90–114 are in the average range, scores between 70 and 89 signify “below average” performance, and scores below 70 indicate “well below average” performance [
35]. According to the test developers, the internal consistency evidence is moderate-to-high (0.78–0.94 for early elementary and 0.80–0.94 for late elementary).
The district administered the SELweb performance assessment to all K-6-grade students during the fall, between September and October, the winter, between December and January, and the spring, between March and April. After the assessment was administered, the team reviewed the aggregate classroom-level results to determine if any skill clusters showed less than 80% of students at or above the benchmark expectations. In classrooms where this was the case, the team would then plan lessons that specifically supported the development of the identified skills (e.g., Tier 1 intervention opportunities include using a book that is read aloud to the class with specific questions, using an aligned second step lesson). The team also reviewed individual student data to evaluate if poor academic performances were also in conjunction with poor SELweb performances. These opportunities were more so provided for Tier 2/3 intervention. The results were then used for core programming, intervention selection, community coordination, and program evaluation.
Table 2 presents aggregate summary data from 2022–2023. A greater proportion of students were identified on the Late Elementary measure (23.46%) compared to the Early Elementary measure (15.40%). On the Early Elementary and Late Elementary measures, self-control was the greatest area of need, with less than 80% of screened students at or above expectations, and social problem-solving emerged as an additional area of need for Late Elementary.
8. Universal Screening 7–10: Sense of School Membership Scale
The district administered the Sense of School Membership Scale (SSMS) to all 7th–10th-grade students to measure students’ connection to their school community. The measure is based on Goodenow’s [
36] Psychological Sense of School Membership (PSSM) scale. Given that one of the district’s wellness goals is for students to “experience a personal sense of belonging within the school community”, this measure was selected to assess student perception of school belonging. Students responded to 18 items that measured their sense of belonging in their school on a scale from 1 (
Not at all true) to 5 (
Completely true). Scores on each item were summed to create a composite score. For the PSSM, Goodenow [
36] reported adequate internal consistency (Cronbach’s alpha range 0.77–0.88) and construct validity evidence of psychological school membership significantly correlated with teacher-rated perception of effort and student-rated school motivation and grades.
For interpretation, high scores indicated greater school belonging, and scores were contextualized with additional information. Scores that were lower than one standard deviation from the mean indicated low levels of school connectedness. The results were used to monitor progress toward the district wellness goal and identify students who would benefit from support and services aimed at improving school connectedness. More specifically, grade level/content area teachers used these results to better support their students through exploring extracurriculars, clubs, and elective courses to increase school connectedness. The building wellness/SAP and Building Leadership Team reviewed these results to help ensure that students were being supported and brought them to discussion at department/grade level meetings.
Table 2 presents aggregate summary data from 2022–2023.
9. Universal Screening 6–9: Ask Suicide Questions Questionnaire
To identify students with potential suicide risk, students in grades 6 and 9 were administered the Ask Suicide-Questions Questionnaire [
37], which is a component of the Signs of Suicide™ (SOS) program [
38] and was created by Nationwide Children’s Hospital. The ASQ is a 4-item, self-report, suicide-risk screening assessment measure where students respond with a yes or no to each item. With its brief nature, this self-report takes approximately 2 min to complete, and any item answered “yes” is flagged for suicidal ideation and/or intent. The overall SOS implementation included a dual-measure approach using the SOS content and its specific component, the ASQ. For students who were not opted out of the program, the ASQ was administered as well as a separate opportunity where students could respond with a “yes” or “no” on a slip called a “Response Card”. This card asked, “would you like to talk to someone because you have a concern for yourself or a friend?”. The ASQ data were then matched to the Response Card and evaluated by a triage process: (a) any flags on the ASQ become a triage priority, (b) any hits on the ASQ that also included a “yes” on item 5 take the highest priority, or (c) no hits on the ASQ but a “yes” on the Response Card take lower/mild priority. Students who indicated that they would like to talk to someone about a concern for a friend then open the triage process for the friend in concern if not previously identified through the ASQ and Response Card. In comparison to the Suicidal Ideation Questionnaire, the ASQ demonstrated a sensitivity of 100% and specificity of 91% for youth in outpatient settings [
39].
The triage team reviewed the data in real-time by matching all ASQ results to Response Card responses, prioritizing students based on patterns of ASQ and Response Card responses, and conducting support strategies in order of priority, tracking outcomes, and recommendations (e.g., parent contact, referred for risk assessment, safety plan, follow-up in 2 weeks). As the data were reviewed, staff called students from their classrooms and led them to the triage area. In order to mask the intent of pulling students, runners indicated that the students would be providing feedback and survey responses after the content was delivered [
40]. The team then used clinical staff to conduct risk assessments, make referrals, and develop safety plans while pending triage outcomes. Safety plans, such as a sharps ban or a check-in person, were then managed by school personnel.
Table 2 presents aggregate summary data from 2022–2023. Parents of at-risk students were notified after the screening and triage, but prior to the risk assessment.
9.1. Referral
In addition to universal screening, students could also be identified through traditional referral processes. The Care Coordination Team (e.g., Administrator, School Psychologist, School Counselor, School Navigator, Teaching Personnel) at each building leads the referral process, which involves referral, intervention, monitoring, and care support. The district has a Care Coordination referral form that includes standardized questions for protective factors, risk factors, and behaviors of concern. The behaviors of concern align directly with the local community-based provider’s referral, so the district and community partners are able to streamline paperwork. The form is available electronically for staff to complete, and then the Care Coordination team processes the referral. There were two buildings that already had a preexisting referral process, and the district augmented those referrals with items from the Care Coordination referral. After a referral is received, the Care Coordination team then completes documentation to indicate who received the referral, whether or not parent(s) and/or caregiver(s) were contacted, the type of contact, and the triage level. The Care Coordination Team can add comments on the documentation sheet. The team must also check all boxes that apply to the outcomes and recommended actions of the situation. The options include the following: parent granted consent for screening, Brief Intervention and Referral to Treatment (SBIRT), parent declined consent for SBIRT, referred for school navigation, SBIRT screening completed, referral to service coordination, maintain current services and interventions, connect with school activities and programs, connect with advisor and/or mentor at school, diagnostic assessment completed, and case management started.
9.2. Interventions and Supports
After a student was referred for support or identified on the universal screener, the Care Coordination Team reviewed existing and additional data to identify student needs. For instance, the team considered math and literacy foundations benchmark and performance data (e.g., grades, state assessment scores), teacher/parent reports, overall and domain-specific risk on screening measures, attendance data, and case history (i.e., previous referrals and historical interventions). The team also identified a case manager for each referral to lead the intake and monitoring process.
To promote systematic and data-based intervention decision-making, the district created an intervention decision-making framework (see
Table 3). In this framework, the Care Coordination teams considered an identified student’s skills, competence, and performance when selecting a type of intervention. For instance, if a student displayed low social–emotional skills and low performance, then the team selected a social–emotional skill-building intervention; whereas, if a student exhibited high skills on the SELweb Assessment but their social–emotional performance was low, then the team planned an intervention to rehearse and reinforce the targeted skill (e.g., social skills or self-management).
School Navigators, Psychologists, and Counselors typically implement school-based social, emotional, and behavioral interventions, such as Zones of Regulation [
41] for social awareness and emotional regulation skill-building interventions, brief solution-focused intervention and case management, social inclusion supports (e.g., lunch social skills group, mutual interest clubs, friendship groups), and the Modular Approach to Therapy for Children with Anxiety, Depression, Trauma, or Conduct Problems [
42]. School mental health professionals also use the Managing and Adapting Practice [
43] to identify evidence-based practices for a variety of youth mental health challenges.
When planning the intervention tier, the team considered the frequency, duration, and intensity of the concern and matched the support to the level of need. Tier 3 interventions were implemented more frequently with a higher level of intensity, monitoring, case management, and support, and were individualized as needed. The Care Coordination team led student care coordination after students received support/intervention. The systematic process relied on an intake process, communication with families and the referring staff member (when applicable), monitoring and aligning student care, and evaluating student progress.
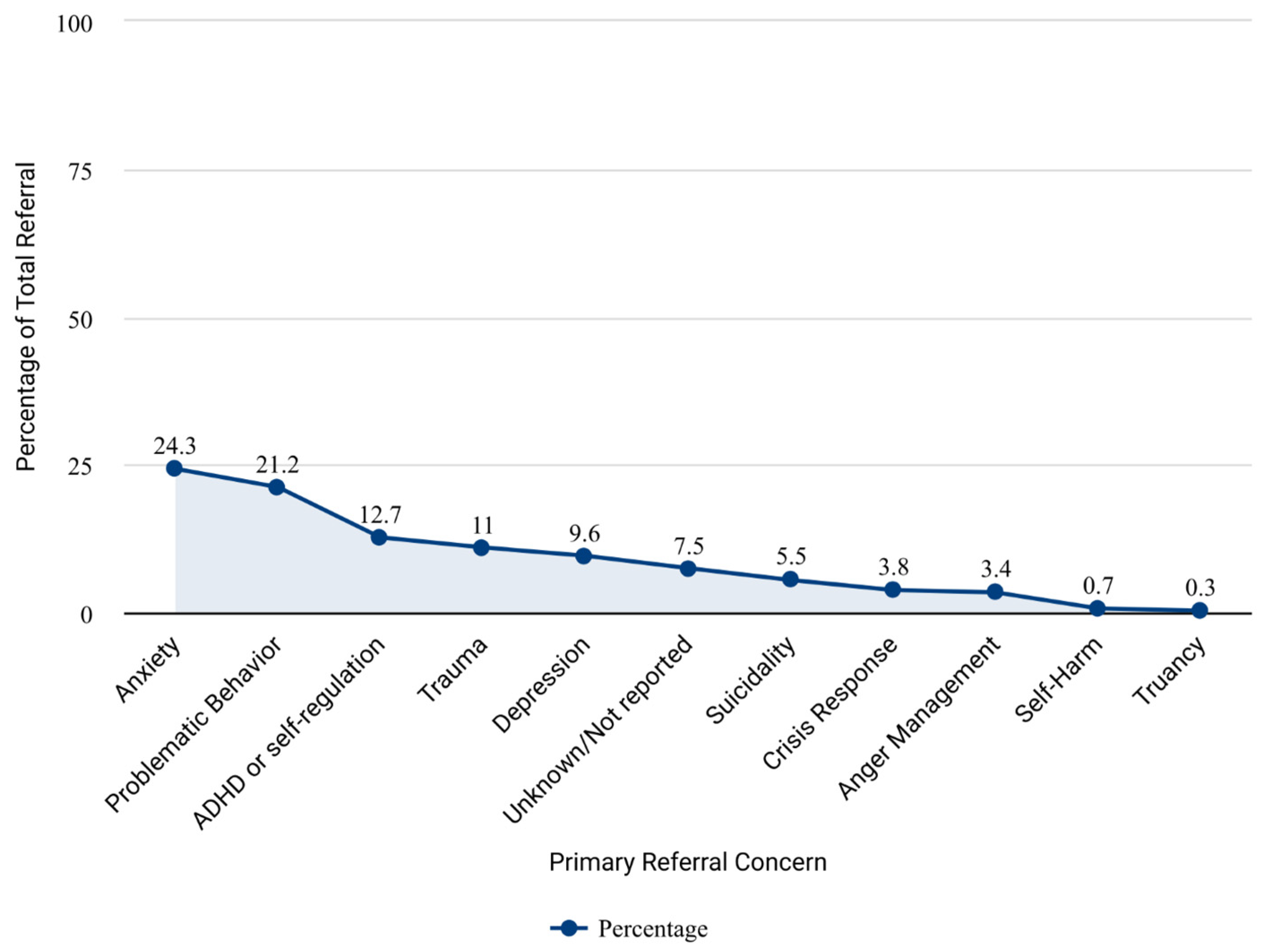
During the 2022–2023 school year, 292 students in grades K-12 were referred for behavioral health services, and 100% received school-based supports. Of those, 271 (93%) were involved with community-based mental health services in addition to school-based supports (e.g., case management and follow-up). Of those students involved with mental/behavioral health services, 121 (41%) also received academic intervention services (intervention and/or special education services).
Figure 1 presents the frequency of primary referral concerns with the most prominent reasons being anxiety (24.3% of referrals), behavior concerns (21.2% of referrals), attention or self-regulation (12.7% of referrals), and trauma (11.0% of referrals).
10. Community Supports
The district collaborated with community agencies to align the school request for assistance process with the community behavioral health referral process to create an integrated system. In this integrated system, checkboxes and follow-up actions were aligned to make transitioning between school and community supports seamless. School Navigators received completed referrals and collaborated with school Care Coordination Teams to determine the next steps. If additional support was warranted based on the level of need, then the School Navigator provided a link to community-based mental health services and assisted with the consent process to provide a warm handoff (i.e., directly connect the family with the service agency and clarify the referral process). The district, School Navigators, and community behavioral referral agencies also created a Release of Information process to create a standardized system and process for proactively obtaining a release to share information and data. Even when students received supports through behavioral health agencies, the Care Coordination team still provided monitoring and case management.
11. Program Evaluation and Next Steps
Since beginning the wellness task force in 2018–2019, the Marysville Exempted Village has made substantial progress in developing a continuum of support and integrating systems. To continue improving the wellness approach, the Director of Continuous Improvement leads program evaluation and continued planning efforts. Specifically, the district maintains a referral database to monitor all referred students, which students received interventions and services, and outcomes from supports. Further, the district collects feedback from administrators and the building Care Coordination teams to enhance efforts and monitor aggregate and subgroup performance on the SELweb during each screening window.
Based on these evaluation efforts, the district identified early identification and substance use and misuse as continued areas for improvement. To further improve early identification, the district is building ecosystems with preventative technology in schools to assist with early identification (e.g., flagging concerning words and phrases on district devices, using digital hall passes for vape detection). Marysville also identified early identification prior to major school transitions as a priority and will begin administering the ASQ in grades 6, 8, and 10 as students transition to new buildings in grades 7, 9, and 11. Additionally, the district will add substance use and misuse prevention modules. To support continued efforts, the district is partnering with the Mental Health Recovery Board for a Substance Abuse and Mental Health Services Administration Project AWARE (Advancing Wellness and Resiliency in Education) Grant.
12. Discussion
As schools work toward addressing the post-COVID youth mental health crisis [
1], SAPs implemented within an MTSS can serve as a service delivery model to proactively offer a continuum of supports. A SAP involves education and building awareness, prevention, early identification, referral, intervention, and guided support services [
4]. To enhance SAP early identification efforts, schools can administer universal screening measures to benchmark social, emotional, and behavioral functioning and use results in addition to typical referral processes and existing data (e.g., academic achievement, attendance, office discipline referrals). Universal screening aids prevention programming and allows SAPs to identify risk as soon as possible for tiered service delivery [
15]. However, previous research noted barriers to implementing universal screening, including challenges with access and awareness [
17], as well as using results to serve newly identified students [
18]. In addition to screening challenges, schools may have difficulty implementing a SAP due to bifurcated education and community mental health systems [
20]. This article provides a case example of one district’s efforts to create a system that integrates universal screening data and school and community structures supporting students’ wellness within a multi-tiered framework.
Marysville Exempted Village School District developed a districtwide approach to proactively supporting student wellness, identifying needs through universal screening and referral processes, and using Care Coordination teams (analogous to a Student Assistance Team) to review data and referrals, plan interventions, link students to outside services when appropriate, and provide ongoing support and follow-up. The district used strategic planning to create a continuum of supports with data-based decision-making.
The district used universal screening data to plan and evaluate Tier 1 SEL promotion and prevention efforts. The results suggested that self-control was the greatest area of need on the SELweb for early and late elementary. A greater proportion of students were identified on the late elementary version compared to the early elementary version, but the results still aligned with PBIS expectations that approximately 20% of students would benefit from Tier 2 and 3 supports [
11]. However, the district is in year six of planning and implementing a wellness continuum of supports, so it is unknown if rates would be higher with less prevention and intervention in place.
To overcome access barriers to implementing screening [
17], the district focused on diverse streams of funding to pay for the screening tool and contracted with an outside provider to fund a School Navigator role. The School Navigators collaborated with school-based mental health professionals to triage results and provide school-based interventions and support. The Navigators also assisted students with the greatest needs in getting connected with community-based supports. Having this additional support role assisted with overcoming barriers and using the screening results. To address awareness barriers [
17], the district connected universal screening to the district student wellness mission and educated all Care Coordination teams about universal screening and the decision-making process for planning interventions and Tier 1 supports based on the results. Further, the decision-making process for intervention planning supports intervention validity, which is the “extent to which assessment results can be used to guide the selection of interventions and evaluation of outcomes” [
44] (p. 15). Creating an intervention data-based decision-making heuristic can aid other districts that may struggle when initially implementing universal screening [
18].
The district also carefully planned to integrate school and community mental health systems in order to prevent common collaboration challenges [
19,
20]. For instance, the district collaborated with local community mental health agencies to align the referral form and process to reduce redundancy and allow School Navigators to efficiently link students to outside services rather than waiting for caregivers to complete a separate process. This can prevent the barrier of restricted coordination mechanisms that often limit school mental health collaboration [
20]. Additionally, the district organized a multidisciplinary teaming process in each building with the School Navigator serving as a representative for both the school and local community mental health agency. This relates to the work of Reaves et al. [
45] which found that the use of a multidisciplinary team and the presence of a community provider on the team was associated with greater service provision for students presenting concerns, particularly for Tier 2 supports. Previous research has noted that many referrals to community agencies are unsuccessful due to low rates of consent and treatment initiation, particularly for students identified on universal screening measures [
22,
46]. To prevent this challenge, School Navigators provided a warm handoff to actively introduce families to the agency and process and describe the intake process. Based on district data, the primary referral concerns were anxiety, problematic behavior, and self-regulation. Kerr et al. found that adolescent mental health needs are steadily rising, especially after the impacts of COVID-19 [
25]. After a referral, the school Care Coordination team and case manager provided ongoing support and follow-up.
As the disconnect between school and community mental health systems is one of the greatest challenges in school mental health [
20], Marysville provides an example of an integrated system that successfully linked referrals with interventions and supports, as 100% of students referred for Care Coordination received supports and 93% received community-based supports in addition to supports from the Care Coordination Team. Comparatively, previous research found that low rates of referred youth received follow-up supports [
21,
22] and that providing mental health services in schools in an integrated system can increase the likelihood of a successful referral [
23]. Through embedding community-based supports into the structure of the school setting, Marysville overcame the common barriers and low rates of access typically found in youth mental health research.
13. Implications for Practice
Marysville Exempted Village School District provides an example of integrating systems, using data-based decision-making, and carefully designing a continuum of supports. For schools interested in planning and implementing a wellness continuum of supports, they can form a steering committee to oversee the initial strategic planning and develop a mission and vision to guide the work. Another initial step is to conduct a needs assessment and map existing resources to identify gaps in offering a continuum of supports to address needs and promote wellness [
47]. Marysville identified the need to offer additional brief school-based interventions and a support mechanism to connect students to community-based behavioral health providers. To assist in addressing these needs, Marysville used cost sharing to fund the new position of a School Navigator. Other districts may consider similarly contracting with local behavioral health agencies to create a school-based role (i.e., a School Navigator) that can serve on Care Coordination teams, offer brief school-based interventions, link students in need with community-based providers, and provide ongoing support and monitoring. As discussed in the Interconnected Systems Framework guiding document [
24], districts can create a single system of delivery that integrates education and mental/behavioral health systems with a unified Request for Assistance Process to aid collaboration and overcome barriers [
24]. A critical element to Marysville’s success in implementing a data-based continuum of supports is using diverse funding streams that capitalize on the strategic use of district, local, and grant funds, which aligns with the National Center for School Mental Health’s [
47] recommendation for diverse and leveraged funding to advance comprehensive school mental health systems.
Ideally, creating a School Navigator role will assist schools in preventing and overcoming barriers to implementing universal screening, and facilitate the use of the data to plan interventions. As access barriers will be reduced, the School Navigator can collaborate with school mental health professionals to review the data and offer interventions to students in need. When planning to serve newly identified students, schools can develop a procedural framework that outlines tiered decision-making based on the proportion of students identified [
48]. In this model, a school would first identify serviceable base rates (e.g., the proportion of students demonstrating risk) for Tier 2 interventions and create a plan for addressing needs above that proportion with schoolwide and classroom-based supports. Further, it is critical to center equity when implementing universal screening, which includes reflecting on dimensions of systemic change, identifying strengths and stressors at the individual, group, and community levels, dismantling structural oppression, and promoting wellness for minoritized youth [
49].
14. Limitations and Directions for Future Research
Although this case example highlights the work of one school district in integrating their systems and data within a SAP framework, it is not without limitations. For example, this article reports on the macro-level implementation of various SAP components, but the degree to which each was implemented with fidelity was not assessed rigorously. Furthermore, although outcomes of the strategies implemented are monitored by the school district, the outcome data were not collected as part of a rigorous research design that could allow causal inferences to be drawn, and are also not fully presented herein due to the aims of this article. Additionally, the case example focuses on one suburban school district in the Midwest, which had a commitment from key leaders for the work as well as access to resources to support the work; the model may need to be adapted for other school districts that do not have these elements in place. Future research may aim to replicate the integrated data-based system in comparison to school mental health practices-as-usual with a detailed process and outcome evaluation. Further, qualitative approaches may assist in exploring implementation barriers, facilitators, and strategies.
15. Conclusions
Given the increasing youth mental health need that was exacerbated by COVID-19, it is critical for districts to plan and implement a continuum of support to address needs and promote social–emotional wellness. SAPs aligned with an MTSS can serve as one service delivery model to integrate systems and data to deliver a continuum of supports. This article provides an example of one district’s approach to implementing a SAP with universal screening to guide tiered decision-making and integrated school and community support structures. Strategic planning, the use of diverse funding, and a School Navigator role to integrate school and community systems aided Marysville’s continuum of support. As districts work towards implementing a proactive system of support, case examples can elucidate the process of change and clarify expected levels of need, although further research is needed.






{kind=link}