Abstract
Behavioral problems cause limitations in the social skills of children without disabilities and affect the functionality of children with disabilities. The Emirati child adaptation scale (ECAS) was developed in the UAE to provide reliable and valid information on the behavioral adaptation skills in children with and without intellectual disability (ID). The scale’s item pool consists of 651 items that identify behavioral adaptation deficits across the 10 domain–skill areas of communication, pre-academic, listening, social, self-care, self-orientation, motor skills, operational society, life, and health and safety. The scale was administered to 1542 children with disabilities and 920 children without disabilities. The scale is deemed essential, as it enables psychologists, special education teachers, health professionals, and researchers to implement a reliable psychometric tool of adaptive and behavioral functioning of 1–18-year-old individuals. The development and structure of the Emirati child adaptation scale is described and discussed.
1. Introduction
In recent years, research has focused on capturing the right conditions to ensure (as much as possible) the equal participation of people with intellectual disabilities in education, vocational, and especially social. Based on the prevailing socioeconomic–political conditions, various scientific approaches have been proposed, which over the years have been rejected, redefined or have been the impetus for the formation of modern theories concerning people with mental disabilities. Unlike in the past, now, the emphasis is on Issues related to their quality of life. There is also a gradual change in their education. There is a shift in education from cognitive skills to social and self-determination skills. The possibility for the maximum possible independence and social relations become a primary issue as they are related to their quality of life and their wider development and prosperity. Therefore, recording the social dimensions of the problems they face, the effort of deinstitutionalization and integration into the community and the strengthening of the capacity for self-determination are long-term, demanding tasks [].
Self-determination is a concept that reflects the belief that all people with or without disabilities have the right to personal choice, autonomy, and self-realization to ensure a better quality of life. A person’s self-determination is a basic condition for his personal and social development, independence, sense of control over his life and his degree of satisfaction from everyday life. Thus, the concept of quality of life is inextricably linked to self-determination as it is directly related to the individual’s choices. In people with intellectual problems, stigma seems to cover a wide range of their social characteristics and significantly affects the way they react and are active in social interactions. Stigma is also associated with dependence on the family environment and with a wide range of social behaviors that they face throughout their lives due to their reduced mental abilities. For this reason, self-determination, which is the ability to have personal control, to form goals, values, and choices according to personal desires and expectations, to recognize and evaluate needs, to effectively manage negative evaluations and reactions of others towards them, emerges as a major issue in individuals with ID education and training []. Based on self-identification and social relationships of people with intellectual disabilities, deficits in these areas affect their quality of life and the way they are treated by people with typical development. People with intellectual problems have difficulty or inability to connect events with specific emotional reactions and the regulation of behavior based on previous experiences, which have a negative effect on their social integration. On the other hand, the environment does not offer opportunities for these individuals to establish and maintain social relationships, resulting in a vicious circle between their deficit and the effects of the alleged stigma.
Intellectual disability (ID) is “a pervasive developmental disorder with sub-average intellectual level and significant deficits in adaptive and behavioral functioning that prevent an individual from conforming with the social and cultural norms of his/her social group” according to DSM-V []. The deficits on multiple cognitive and behavioral domains, e.g., abstract reasoning and problem solving [], communication, selective attention [], working memory [], academic problems [], self-care, work, health, and home-living [] assign the disorder a complex mental profile []. Individuals reflect the adaptive functioning skills of a 6–7- and 11-year-old [] and tend to display aggressive and antisocial behaviors [], which are three times more severe in adolescents and children than of people without disabilities []. Moreover, they show deficits in conceptual skills such as designing and organizing and using abstract concepts; social skills, such as general behavior, feelings about themselves, understanding others, problem solving, influencing others, following the rules of law enforcement, and practical skills, including management home and personal care, money management, telephone use, travel, staying safe and healthy, following programs and routines, and maintaining a professional life []. Limitations on self-care skills and in social relationships as well as behavioral exaggerations are common features of people with intellectual disability. Additionally, they need extensive support with basic self-care skills such as dressing, feeding, and hygiene [].
According to Horvat et al. [], behavior identification focuses on two main points: (a) behavioral problems and (b) adaptability. Identifying behavioral problems includes the types of corresponding behavior that occur, their frequency as well as their intensity. From the identification of adaptability, information is generated regarding the ability of the child to perform specific skills when needed as well as the frequency and the way he adapts to the requirements of the environment. Adaptive behavior is “the ability to respond successfully, according to our age and social group, to the social demands for promoting our personal independence, as well as to the need to develop interpersonal relationships” []. Adaptive skills need daily activities to support our personal and social self-efficacy []. Based on the above concerns regarding the quality of life of these individuals, their ability for self-determination and their social integration, the purpose and objectives of developing the Emirati child adaptation scale (ECAS) were formulated.
1.1. Purpose
In the Middle East, the number of people with intellectual disabilities is slightly higher than the worldwide figures of 2.5–3% []. Although there are ongoing efforts in the UAE to promote educational and social programs that cater for the needs and rights of individuals with intellectual disability and several special education schools are present [], the diagnosis of intellectual disability using a nationally normed assessment tool has not yet been pursued. Intellectual scales are the only methods that have been used to diagnose intellectual disability and its degrees of severity, and to determine the appropriate educational placements for students with intellectual disability. IQ test scores continue to be used as the primary criterion in special education decision-making []. By the mid-1900s, professionals in the field required that adaptive behaviors should be included as a critical component in the diagnosis of intellectual disability [,,]. This concern was reflected in the American Association of Mental Deficiency (AAMD) classification of intellectual disability, which requires the presence of deficits in adaptive behavior as a criterion for the diagnosis of intellectual disability [].
There are several reliable and valid scales in the international literature that identify psychosocial problems in children and assess their behavior [,] such as the Vineland adaptive behavior scale (VABS) [], strengths and difficulties questionnaire (SDQ) [], and the child behavior checklist (CBCL) [], among others. The accurate and consistent diagnosis of intellectual disability requires the availability of a nondiscriminatory, objective assessment tool, which is nationally normed. Therefore, a nationally normed cognitive ability scale and adaptive behavior scale [] was developed considering multiple factors such as individuals in the UAE’s ethnicity, race, gender, age, and socioeconomic status in the norming process of developing the instrument []. The study’s purpose of diagnosing and assessing an individual’s level of intellectual disability and deficits accurately and consistently is threefold: (1) to determine a person’s educational, professional, and social development; (2) to facilitate decision making on issues of eligibility for special education services and educational placements; and (3) to promote the inclusion and advocacy for the rights of individuals with intellectual disability.
In the UAE, psychological, social, communication, and special education services for individuals with disabilities are being rapidly established and significantly improved. Providing special services to individuals with ID must rely on accurate and consistent assessment tools for problem identification, planning, monitoring, and evaluation [,]. The need of locally normed psychological and educational assessment instruments in the UAE is of crucial importance as lack of valid tools of diagnosis of adaptive behavior skills in children with ID results in poor case identification. The adaptive behavior scale was designed as a rating scale for use with Emirati children (aged 1–18) in the UAE to provide psychometrically sound measurement of their adaptive behavior skills required to meet local society’s expectations. ECAS has psychometric properties of face, content, convergent, divergent, and construct validities as well as high test–retest and inter-rater reliability. This scale is used by psychologists, special education teachers, health professionals, and researchers to (a) implement diagnosis and classification of disability; (b) facilitate issues of eligibility for special education provision and services; (c) develop effective individual intervention plans; (d) monitor and evaluate intervention services; and (e) investigate related variables to adaptive functioning and behavior in ID.
For developing ECAS, the researchers explored the literature on psychometrically sound standardized tests for the diagnosis and assessment of ID. The intent was to generate information from different sources and weigh the evidence derived from descriptive, inferential, and theoretical data. Sources of information included literature from peer-reviewed journals; manuals on adaptive behavior instruments; and feedback from professionals with experience in assessing adaptive behavior. Additionally, four adaptive behavior scales were reviewed to develop ECAS: (1) the adaptive behavior scales—residential and community, second edition (ABS-RC:2) [] (b), (2) the AAMR adaptive behavior scale—school: second edition (ABS-S: 2) []; (3) the developmental assessment for individuals with severe disabilities, third edition (DASH-3) []; and (4) the Vineland social maturity scale (VSMS) [].
1.2. In the Following Sections, We Describe the Two Main Phases of Data Collection and Analyses That Led to the Final ECAS
1.2.1. Design/Methodology/Approach
The framework and methods employed to carry out the research are described in the next section. It outlines the techniques and procedures used to collect and analyze the data and justifies the decision-making process.
1.2.2. Data Collection—ECAS Initial Form (Appendix A)
The research assistants were trained by the authors to administer the ECAS, collect data, and establish its psychometric properties. Test–retest reliability and internal consistency were investigated by administering the initial form of the ECAS to ninety (90) children without disabilities and sixty (60) children with disabilities. Item analyses were used to identify nondiscriminating or inadequate items. The children were selected through stratified random sampling from general and special education schools across the UAE. A second, independent sample of ninety (90) children without disabilities and sixty (60) children with disabilities were administered a revised version of the scale based on data acquired from the first administration. Additionally, the criterion validity of the initial form of the ECAS was established by administering the scale to one hundred eighty (180) children without disabilities and one hundred twenty (120) children with disabilities, aged 4–18-years-old using stratified random sampling.
The ECAS was developed to assess the adaptive behavior of individuals between the ages of 1 and 18 years, inclusive. The ECAS initial version used in Phase 1 consisted of the following domains: 1. communication; 2. self-care; 3. home living; 4. social skills; 5. appropriate use of resources in the community; 6. self-direction; 7. health and safety; and 8. applying academic skills in life, leisure, and work. These domains were transformed into items. Each item reflected observable specific target behaviors congruent with UAE culture. In this phase, the researchers developed an initial item pool designed to measure adaptive behaviors expected by children in the UAE according to their developmental and chronological age and gender. The domains and the items included in ECAS were rated by professors in special education and psychology, and by special and regular education teachers. These professionals rated each item based on (a) the degree it reflects the skill that is supposed to be measured; (b) the precision of language; (c) the clinical significance; and (d) the ability to observe the target skill [].
How the Study Was Conducted
The study was conducted in two phases, with the first phase involving 90 children without disabilities and 60 children with disabilities, selected through stratified random sampling from general and special education schools across the UAE. The initial form of the ECAS was administered to these children to investigate test–retest reliability and internal consistency. Item analyses were used to identify nondiscriminating or inadequate items. The second phase of the study involved a second independent sample of 90 children without disabilities and 60 children with disabilities who were administered a revised version of the scale based on data acquired from the first administration. Additionally, the criterion validity of the initial form of the ECAS was established by administering the scale to 180 children without disabilities and 120 children with disabilities aged 4–18 years old, through stratified random sampling. The ECAS was developed based on the domains of communication, self-care, home living, social skills, appropriate use of resources in the community, self-direction, health and safety, and applying academic skills in life, leisure, and work. The domains and items of the ECAS were rated by professors in special education and psychology, as well as special and regular education teachers, based on their ability to observe the target skill, the degree to which they reflect the skill that is supposed to be measured, the precision of language, and clinical significance. The final version of the ECAS was developed to ensure congruence with the domains and definition of adaptive behavior identified by the American Association on Mental Retardation (AAMR) and the Diagnostic and Statistical Manual of Mental Disorders, DSM-V. The researchers reviewed current research related to adaptive behavior and various adaptive behavior scales normed in different cultures to develop the domains and items of the ECAS. The ECAS was administered through an interview by school professionals, including school psychologists, teachers, and/or social workers. The scale consists of 651 items covering 10 areas appropriate for each of the 11 age levels for 1–6-year-old children and 13 age levels in 7–18-year-old participants. The study showed that the ECAS has good psychometric properties and can accurately measure adaptive behavior in children in the UAE.
1.3. ECAS Final Form
The final form of the ECAS was structured and developed to ensure congruence with the domains and definition of adaptive behavior identified by the American Association on Mental Retardation (AAMR) [] and the Diagnostic and Statistical Manual of Mental Disorders, DSM-V []. The domains and items of the ECAS were developed after the researchers reviewed current research related to adaptive behavior and various adaptive behavior scales normed in different cultures, e.g., the Arabic version of the AAMD adaptive behavior scale: manual and Bahraini norms [], the adaptive behavior assessment system II [], and the scales of independent behavior []. All members of the team who developed the scale are Arabic native speakers who lived in the country for many years and who have similar culture to the UAE culture. Examples of the items from ECAS that reflect the UAE culture include the following. Items relating to community use (ages 1–6 years) include going to the mosque and how to behave inside the mosque. In addition, some items are related to how to greet people in Islamic culture, wear traditional UAE clothes, etc. For the 7–18 years age group there are some items in relation to UAE culture such as enjoying gifts received during Islamic festive season and having friends of the same gender. Finally, all the materials used are culturally specific, e.g., clothes, etc. The ECAS was constructed to offer accurate information about substantial limitations in adaptive behavior and to differentiate between individuals who do and do not have intellectual disability. The ECAS measures child behaviors and skills in 10 areas from age 1 to 6 and the changes in child behavior and skills every 6 months; additionally, from age 7 to 18, it measures the changes in behavior and skills every consecutive year. Thus, specific items are used to cover a 6-month interval and a 1-year interval, respectively. The ECAS was developed to be administered through an interview by school professionals including school psychologists, teachers, and/or social workers. The ECAS is an individually administered standardized test of adaptive behavior skill domains including communication, pre-academic skills, listening skills, social skills, selfcare, self-orientation, motor skills, operational society skills, life skills, and health and safety skills. Each area was covered by approximately 33 items appropriate for each of the 11 age levels for 1–6-year-olds and 33 items appropriate for each of the 13 age levels in 7–18-year-old participants. The scale consists of 651 items for 1–18-year-olds (Table 1).

Table 1.
Adaptive domain–skill area classifications.
The application of ECAS differs depending upon the age of the child and the speed of the examinee’s response. The older the child is, the estimated time for applying the scale decreases. For example, children from 4.5 to six years of age take from 25 min to 40 min to be tested, as well as children aged 7–18; while children aged one to three years take about an hour to be tested.
1.4. Participants
The scale was field-tested in 2019–2020 to obtain the norms and to assess its psychometric properties. The researchers who developed the Emirati child adaptation scale (ECAS) protected the participants’ privacy and confidentiality, and they implemented measures to ensure that the data collected were secure. Ethical approvals were obtained from the Ministry of Education, UAE, and the Internal Research Grants College Research Committee at the United Arab Emirates University (UAEU) before conducting the study. This ensured that the study adhered to ethical guidelines on privacy and confidentiality. Moreover, the researchers obtained informed consent from the parents or guardians of the children before administering the ECAS. This ensured that the parents or guardians were aware of the nature of the study and that their children’s data would be used for research purposes. Furthermore, the researchers used secure methods to collect and store the data. The ECAS was administered to the children in a private and confidential setting, and the responses were recorded anonymously. The data collected were stored securely and were only accessed by authorized personnel, who were involved in the study.
Demographic information on the participants’ Emirate, gender, and nationality are presented below (Table 2). The total calibration sample consisted of 920 children without disabilities and 1542 children with disabilities. The data were collected from 404, 1—6-year-old female and male children across the seven Emirates in the UAE, who are enrolled in regular and special education schools across the UAE. More than half of the participants were Emiratis while the rest were other Arabs. An almost equal number of females and males participated in the sample. The participants were enrolled in regular and special education schools across the seven Emirates and were selected using a stratified random sampling process. The sample included 1542 children with disabilities (599 females and 943 males) and 920 children without disabilities (478 males and 442 females).
Table 2.
Demographics of 1–6-year-old participants.
Additional data were collected from 516 mixed-gendered children, aged 7–18 across the seven Emirates in the UAE. Approximately half of the participants were Emiratis (49.2%) while the rest were other Arabs. Almost equal numbers of boys and girls (52.7% vs. 47.3%) participated in the application (Table 3).
Table 3.
Demographics of 7–18-year-old participants.
Most of the children with disabilities (56%) had a moderate level of disability, with 22% at a mild level, and a 20% at a severe level. A 2% was at the unidentified level of disability (Table 4).
Table 4.
Degree of disability.
The participating children with disabilities had several different disabilities and disorders (Table 5). Most children had ID (34.1%) and 31.1% were on autism spectrum disorder (ASD), 18.6% had multiple disabilities, and a few had sensory impairments (visual/hearing), ADHD, psycho–emotional disorders, and SLDs.
Table 5.
Types of disability.
The general characteristics of the ECAS are shown in Table 6.
Table 6.
ECAS characteristics.
2. ECAS Rating System
The assessed individual’s typical performance on each behavioral item is using the following rating system (Table 7).
Table 7.
ECAS rating scale.
How the Survey Was Administered to the Participants
The researchers used a stratified random sampling method to select a total of 540 participants, which included 270 children without disabilities and 270 children with disabilities. The participants were between the ages of 4 and 18 years old, and they were selected from general and special education schools across the UAE. The research assistants who administered the ECAS were trained by the authors of the study to administer the test, collect data, and establish its psychometric properties. The initial form of the ECAS was administered to 90 children without disabilities and 60 children with disabilities to investigate test–retest reliability and internal consistency. Additionally, item analyses were used to identify nondiscriminating or inadequate items. A second, independent sample of 90 children without disabilities and 60 children with disabilities were administered a revised version of the scale based on data acquired from the first administration. The criterion validity of the initial form of the ECAS was established by administering the scale to 180 children without disabilities and 120 children with disabilities. The ECAS was designed to be administered through an interview by school professionals including school psychologists, teachers, and/or social workers. The scale consists of 651 items, which are appropriate for each of the 11 age levels for 1–6-year-old participants, and 33 items appropriate for each of the 13 age levels for 7–18-year-old participants. The application of the scale differs depending on the age of the child and the speed of the examinee’s response. Children aged 4.5 to 6 years, as well as children aged 7–18, take from 25 to 40 min to be tested, while children aged one to three years take about an hour to be tested. The survey was administered to the participants through trained research assistants who conducted interviews using the standardized ECAS test. The validity and reliability of the test were established through various analyses, including test–retest reliability, internal consistency, and item analyses.
Initially a parent completes the scale based on their child’s performance. In the case that a parent does not have adequate information about their child’s performance, the examiner conducts the assessment by observing the child and completing the scale. Items used a three-point scale. If the behavior is normal and repetitive the child is assigned 2 points; if the behavior appears occasionally or with help the child is assigned 1 point; and if the behavior is not shown, the child is assigned 0 points. The individual is assigned 2 points when he/she performs the task completely successfully and continuously; when doing the task without any assistance; if they were able to perform the task in the past, but no longer need to do it now, when performing the task in a different way due to disability. The individual is assigned 1 point when he/she is performing part of a task without assistance; when they perform the whole task with help; when they complete the task, but slowly and incompletely. A (0) score is assigned when the individual does not perform the task or any part of it; when the individual does not respond to the examiner’s instructions to perform the task; if he/she is not trained to perform the skill; someone else performs the task for him/her. A score (CR) applies when there is a sensory or motor deficit that prevents the child from performing the task; in the event that the child is prohibited from performing the task, such as if the parents usually prevent children from ascending the stairs on their own. Finally, (NA) score is assigned if the scale items are higher than the age of the examinee or the child; if the task requires higher abilities than the child’s ability to do; and, if the task comprises a specific element that is not present in the child’s environment, such as a shoe or a specific outfit. If the parent or the child themself is the one who responds to the task or phrase in the scale, they must be provided with the necessary information that enables them to understand the meaning and intent of the phrase or scale item. Caution should be taken in not providing him/her with information that affects his/her response or actions. The examiner must read each phrase of the scale that needs the opinion of parent or caregiver, then, choose the answer that fits and matches the child’s behavior by placing the answer in the designated space, as shown in Table 8.
Table 8.
Examiner’s procedures.
In terms of the “base” and “ceiling” for each domain of the ECAS, the rule for the basal level is calculated when the child gets a score of (2) in five successive items/phrases. The ceiling is calculated when the child gets a score of (0) in five successive items/phrases. Sometimes it is impossible to determine a base or a ceiling; when the child does not obtain a score of (2) in five successive items of any domain, this domain does not contain a “basal”; and when the child does not score (0) in five successive paragraphs of any domain, this domain does not contain a “ceiling.” If the symbol (CR) or (NA) appears five times or more in any domain of the scale, one should consult another colleague and repeat this domain.
3. Statistics
The test–retest reliability was tested with Pearson coefficient r. The Cronbach’s index was used to determine the internal consistency of the factors. The internal reliability of each subscale was assessed using Cronbach’s alpha. This measure is not a statistical test; thus, it does not have a significance level. Cronbach’s alpha values range between 0 and 1 where values close to 1 indicate high levels of internal reliability. The cutoff score (0.50) was used as the minimum acceptable level. Structural validity testing was performed with analysis of variance (ANOVA) for independent samples to determine whether there is a statistically significant difference at point 0.05 level between: (a) boys and girls and (b) children with and without disabilities. The structure of ECAS was investigated with Pearson’s r correlations between the domains and the total score. The reliability of each subscale and descriptive statistics, and z-scores are used for the calculation and interpretation of scoring. For example, the reliability of the subscale in the adaptive behavior communication skills is calculated below (Table 9).
Table 9.
Reliability, descriptive statistics, and z-scores of the communication subscales.
Reliability is an indirect measure of accuracy in the measurement process. Given the small number of items in each subscale (which is three items) the reliability values obtained for all subscales in the communication area are acceptable. The interpretation and calculation of each child’s score is based on the scores compared using standardized scores (Z-scores). For example, if a child is 60 months old and achieved 5 in the communication scale, then their Z-Score will be calculated as follows. Z-Score = (5 − 3.5)/1.9, which is 0.79, which is the child’s Z-Score. The Z-scores were transformed to remove the negative values using the following formula. The formula uses a mean = 100 and a SD = 15. After applying the formula on 0.79, the following results: Z-transformed = 100 + 15 (0.79) = 111.9, which is the child’s final score in the domain of communication. This means that the child’s communication skills are above the average of his same age peers.
4. Gender Differences
Males and females were compared on each of the 11 subscales (12 Months, 18 Months, 24 Months, 30 Months, 36 Months, 42 Months, 48 Months, 54 Months, 60 Months, 66 Months, 72 Months) on the 10 areas (communication, pre-academic skills, listening skills, social skills, selfcare, self-orientation, motor skills, social skills, life skills, health and safety skills) using independent t-tests. The results indicated that no gender differences have been observed in all subscales in all areas.
5. Normality Distribution Tests
To test whether the distributions of the results are normal or not, the Shapiro–Wilk test of normality was applied on the results from all subscales in all age categories. Findings indicated that most distributions are NOT normal. An example from these results is the results of the health and safety skills, which has 10 distributions for the 11 age categories. As the results reveal (Table 10), only one distribution (24 months) is normally distributed. An example of the distributions is represented graphically in Figure 1.
Table 10.
Normality tests of the results of the health and safety skills subscales: example.
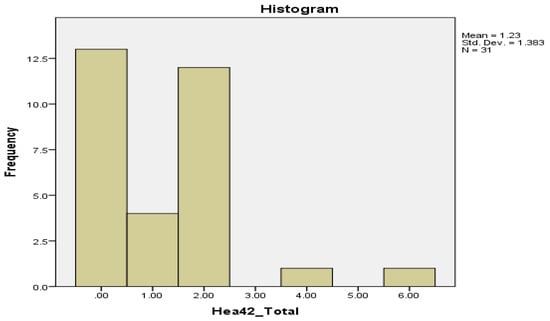
Figure 1.
The distribution of the scores of the subscale communication for age (42 months).
The distribution is not close to the normal distribution; it is positively skewed.
6. The ECAS Discriminant Validity Analysis and Reliability
The ability of the scale to discriminate among the different ages was assessed using the analysis of variance (ANOVA). The results indicated that most subscales have discriminant validity, and they were able to discriminate the different ages. Most of the ANOVA results as measured by the F-test were significant (at 0.05), which indicate significant differences among the results of different ages. The subscales have high discriminant validity. The reliability of the ECAS is assessed since the scale is measuring the child’s adaptation across 10 domains that assess participant’s adaptation from 12 to 72 months of age in communication skills, pre-academic skills, enjoyment skills, social skills, selfcare skills, self-orientation skills, motor skills, social skills, life skills, and health and safety skills. Each subscale has 3 items so the total number of items for the adaptation scale for each age is approximately 30 items. All reliability values are very high. This means that the ECAS is reliable for all ages from 12 months (1 year) to 72 months (6 years) and from 7–18 years and could be used to accurately assess children’s adaptation skills in the UAE.
7. Findings
Table 11 shows the correlation between the existence of disability/normal based on general diagnoses and the existence of delay/normal based on the results of the adaptive behavior scale (any deficiency in adaptive behavior requires a delay in two or more domains of the scale, 97.60%). Table 11 shows the degree of an examinee’s performance (high; delayed; normal) on tasks of the skill-related areas (e.g., merriment/enjoyment skills; Appendix A) that corresponds to his/her chronological age.
Table 11.
Delays in the scale’s domains by disability.
8. Originality
Behavioral problems could cause deficient social skills in children without disabilities and affect the functionality of children with disabilities []. It is essential to have a valid and reliable research tool to assess the adaptive behavior of students with and without disabilities in the UAE, for the early detection of maladaptive behaviors.
9. Discussion
The final ECAS instrument is a 323-item and 331-item scale providing a comprehensive adaptive behavior assessment for diagnosing intellectual disability (ID) for individuals 1 to 18 years of age. The ECAS provides standard scores for communication, pre-academic, listening, social, selfcare, self-orientation, motor, social, life, and health and safety adaptive behavior skills on a metric with a mean of 100 and standard deviation of 15 (Appendix A). It needs to be indicated that the efficacy of the ECAS to plan on interventions or its sensitivity to measure changes in adaptive behavior are not known. Further research is needed to establish the psychometric properties of the ECAS, including its reliability and validity. Validity studies should compare scores obtained on the ECAS with other established standardized scales of adaptive behavior and measure the scale’s inter-respondent concordance. The ECAS is a promising, standardized adaptive behavior scale that provides individual standard scores in the 10 adaptive behavior domains. Furthermore, the aim is for ECAS to be distributed to children with different special needs by teachers and parents to test the scale’s efficacy.
High discriminant validity is established in most subscales, and they were able to discriminate the different ages as most of the ANOVA results were significant (at 0.05), indicating significant differences among the results of different ages. Additionally, the high correlation between the total scores and between the domains support the assumption that the ECAS measures what it aims to measure, i.e., adaptive functioning. In terms of the ECAS reliability, all reliability values are very high for ages 1–18 indicating that the scale could accurately assess children behavior adaptation skills in the UAE.
Author Contributions
Conceptualization, H.E. and E.E.; Methodology, E.E.; Investigation, A.S.; Data curation, E.E.; Writing—original draft, O.A., E.E. and H.E.; Supervision, O.A.; Project administration, A.S. and M.A.; Funding acquisition, O.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by UPAR grant fund, grant number R21014 and The APC was funded by the College of Education, United Arab Emirates University.
Institutional Review Board Statement
The study was approved by and conducted in accordance with the ethical guidelines of the College Research Committee, the Office of the Assistant Dean for Research and Graduate Studies at the United Arab Emirates University, and the Ministry of Education, UAE.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

Figure A1.
Exemplar of the scale.
References
- Baird, A.M. The Self-Determined Student: Teaching Students with Exceptional Needs Self-Determination Through Class-Wide Self-Monitoring. 2020. Available online: https://core.ac.uk/download/pdf/327257855.pdf (accessed on 10 September 2021).
- Garrels, V. Promoting Self-Determination for Adolescents with Mild Intellectual Disability. Validation of a Self-Determination Measure and Evaluation of an Educational Intervention. Ph.D. Thesis, University of Oslo, Oslo, Norway, 2019. Available online: https://www.duo.uio.no/handle/10852/71552 (accessed on 12 September 2021).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Soenen, S.; Van Berckelaer-Onnes, I.; Scholte, E. Patterns of intellectual, adaptive and behavioral functioning in individuals with mild mental retardation. Res. Dev. Disabil. 2009, 30, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Bergen, A.E.; Mosley, J.L. Attention and attentional shift efficiency in individuals with and without mental retardation. Am. J. Ment. Retard. 1994, 98, 688–743. [Google Scholar]
- Van der Molen, M.J.; Van Luit, J.E.H.; Jongmans, M.J.; Van der Molen, M.W. Verbal working memory in children with mild intellectual disabilities. J. Intellect. Disabil. Res. 2007, 51, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.J. An Introduction to the Nature and Needs of Students with Mild Disabilities: Mild Mental Retardation, Behavior Disorders, and Learning Disabilities; Charles C Thomas Publisher: Springfield, IL, USA, 1996. [Google Scholar]
- Fuijara, G.T. Continuum of intellectual disability: Demographic evidence for the “forgotten generation”. Ment. Retard. 2003, 41, 420–429. [Google Scholar] [CrossRef]
- Schalock, R.; Luckasson, R.; Shogren, K. The renaming of intellectual disability: Understanding the change to the term intellectual disability. Intellect. Dev. Disabil. 2007, 45, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Kraijer, D.W.; Plas, J.J. Handboek Psychodiagnostiek en Beperkte Begaafdheid; Harcourt: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Wallander, J.L.; Dekker, M.C.; Koot, H.M. Psychopathology in children and adolescents with intellectual disability: Measurement, prevalence, course and risk. In International Review of Research in Mental Retardation; Glidden, L.M., Ed.; Academic Press: Oakland, CA, USA, 2003; pp. 93–134. [Google Scholar]
- Leaf, J.B.; Ferguson, J.L.; Milne, C.; Cihon, J.H. Social behavior for individuals with intellectual disabilities and dual diagnosis: Common deficits and assessment tools. In Handbook of Dual Diagnosis: Assessment and Treatment in Persons with Intellectual Disorders; Springer: Berlin/Heidelberg, Germany, 2020; pp. 411–427. [Google Scholar]
- Patel, D.R.; Cabral, M.D.; Ho, A.; Merrick, J. A clinical primer on intellectual disability. Transl. Pediatr. 2020, 9 (Suppl. S1), S23. [Google Scholar] [CrossRef]
- Horvat, M.; Kelly, L.; Block, M.; Croce, R. Developmental and Adapted Physical Activity Assessment, 2E; Human Kinetics: Champaign, IL, USA, 2018. [Google Scholar]
- Brown, F.; Snell, M.E. Meaningful assessment. In Instruction of Students with Severe Disabilities, 5th ed.; Snell, M.E., Brown, F., Eds.; Merrill/Prentice Hall: Upper Saddle River, NJ, USA, 2000; pp. 67–114. [Google Scholar]
- Doll, E.A. Measurement of Social Competence: A Manual for the Vineland Social Maturity Scale; Educational Publishers: Minneapolis, MN, USA, 1953. [Google Scholar]
- Middle East Health. Mentally Disabled Children in the Middle East and Their Integration into Society. 2011. Available online: http://www.middleeasthealthmag.com/cgi-bin/index.cgi?http://www.middleeasthealthmag.com/jul2011/feature5.htm (accessed on 20 October 2021).
- Reschly, D.J.; Ward, S.M. Use of adaptive behavior measures and overrepresentation of black students in programs for students with mild intellectual disability. Am. J. Intellect. Disabil. 1991, 96, 257–268. [Google Scholar]
- Harrison, P.L.; Robinson, B. Best practices in the assessment of adaptive behavior. In Best Practices in School Psychology; Thomas, A., Grimes, J., Eds.; NASP: Washington, DC, USA, 1995; Volume 3. [Google Scholar]
- Harrison, P.L.; Boney, T.L. Adaptive behavior assessment. In Best Practices in School Psychology, 4th ed.; Thomas, A., Grimes, J., Eds.; National Association of School Psychologists: Bethesda, MD, USA, 2002; pp. 1167–1180. [Google Scholar]
- Greenspan, S. Reconsidering the diagnosis and treatment of very young children with autistic spectrum or pervasive developmental disorder. Am. J. Intellect. Disabil. 1995, 98, 544–549. [Google Scholar]
- Heber, R. A Manual on Terminology and Classification in Intellectual Disability, American Journal of Mental Deficiency: Monograph Supplement, 2nd ed.; American Association on Mental Deficiency: Albany, NY, USA, 1961. [Google Scholar]
- Kamphaus, R.W. Conceptual and psychometric issues in the assessment of adaptive behavior. J. Spec. Educ. 1987, 21, 27–35. [Google Scholar] [CrossRef]
- Keller, H.R. Children’s adaptive behaviors: Measure and source generalizability. J. Psychoeduc. Assess. 1988, 6, 371–389. [Google Scholar] [CrossRef]
- Sparrow, S.S.; Balla, D.A.; Cicchetti, D.V. Vineland Adaptive Behavior Scales Interview Edition: Survey Form Manual; American Guidance Service: Pines, MN, USA, 1984. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M. Child Behavior Checklist for Ages 4–18; ASEBA (Achenback System of Empirically Based Assessment): Burlington, VT, USA, 1991. [Google Scholar]
- Bruininks, R.H.; Thurlow, M.; Gilman, C.J. Adaptive behavior and mental retardation. J. Spec. Educ. 1987, 21, 69–88. [Google Scholar] [CrossRef]
- Meares, P.A. Assessing the Adaptive Behavior of Youths: Multicultural responsive. Soc. Work 2008, 53, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Chafouleas, S.M.; Christ, T.J.; Riley-Tillman, T.C.; Briesch, A.M.; Chanese, J.A. Generalizability and dependability of direct behavior ratings to assess social behavior of professionals. Sch. Psychol. Rev. 2007, 36, 63–79. [Google Scholar] [CrossRef]
- Salvia, J.; Ysseldyke, J.E. Assessment in Special and Remedial Education, 5th ed.; Houghton Mifflin: Boston, MA, USA, 1991. [Google Scholar]
- Nihira, K.; Leland, H.; Lambert, N.M. ABS-RC: 2: AAMR Adaptive Behavior Scale: Residential and Community; Pro-ed: Austin, TX, USA, 1993. [Google Scholar]
- Lambert, N.; Nihira, K.; Leland, H. AAMR Adaptive Behavior Scale-School, 2nd ed.; American Association on Mental Retardation: Austin, TX, USA, 1993. [Google Scholar]
- Dykes, M.K.; Mruzek, D.W. Developmental Assessment for the Severely Handicapped, DASH-3, 3rd ed.; PRO-ED: Austin, TX, USA, 2012. [Google Scholar]
- Doll, E.A. Preliminary standardization of the Vineland Social Maturity Scale. Am. J. Orthopsychiatry 1936, 6, 283. [Google Scholar] [CrossRef]
- Hosp, J.L.; Howell, K.W.; Hosp, M.K. Characteristics of Behavior Ratings Scales. J. Posit. Behav. Interv. 2003, 5, 2001–2008. [Google Scholar] [CrossRef]
- American Association on Mental Retardation (AAMR). Definitions, Classifications, and Systems of Supports, 9th ed.; American Association on Intellectual and Developmental Disabilities: Silver Spring, MD, USA, 1992. [Google Scholar]
- Jarrar, J.M. Arabic Version of AAMD Arabic Behaviour Scale, Manual and Bahraini Norms; Hope Institute: Manama, Bahrain, 1985. [Google Scholar]
- Harrison, P.; Oakland, T. Adaptive Behavior Assessment System-II; Harcourt Assessment: San Antonio, TX, USA, 2003. [Google Scholar]
- Bruininks, R.H.; Woodcock, R.W.; Weatherman, R.F.; Hill, B.K. Scale of Independent Behavior Revised; Riverside Publishing: Chicago, IL, USA, 1996. [Google Scholar]
- Brossard-Racine, M.; Shevell, M.; Snider, L.; Bélanger, S.A.; Majnemer, A. Motor skills of children newly diagnosed with Attention Deficit Hyperactivity Disorder prior to and following treatment with stimulant medication. Res. Dev. Disabil. 2012, 33, 2080–2087. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).