


How School-Based Wellbeing Interventions, Socioeconomic Status, and Gender Impact Anxiety Development in Middle Childhood

 ,
,
Abstract
:1. Introduction
1.1. Anxiety in Middle Childhood
1.2. Anxiety and Socioeconomic Status
1.3. Socioeconomic Status in Schools and Families in Ireland
1.4. Wellbeing Interventions and Anxiety in Middle Childhood
1.5. Developmental Perspective on Anxiety in Middle Childhood
1.6. The Current Study
- To what extent does socioeconomic status impact the development of children’s anxiety? To investigate this issue, we were interested in examining the impact of both individual family SES and low-income schooling, in line with Bronfenbrenner’s bioecological model of multiple nested developmental contexts [35,36]
- To what extent do wellbeing interventions and gender impact the development of children’s anxiety? We were interested in examining whether wellbeing interventions had a stronger impact for girls versus boys, based on inconclusive findings in the literature on the effectiveness of wellbeing interventions in relation to gender [39]
- To what extent do wellbeing interventions moderate the impact of socioeconomic status on the development of children’s anxiety? This third research question builds on questions 1 and 2 to identify whether the potential associations between SES and anxiety development could be influenced by wellbeing interventions. This question builds on previous research where wellbeing interventions were observed to have potential to prevent or delay the manifestation of mental health difficulties [16] We endeavoured to investigate whether wellbeing interventions were equally as effective for children of both low and high SES, while we were also interested to see whether a negative SES–anxiety relationship would be observed.
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.2.1. Anxiety
2.2.2. Individual Socioeconomic Status
2.2.3. Low-Income Schooling
2.2.4. Wellbeing Interventions
2.3. Analysis Plan
3. Results
3.1. Changes in Anxiety across Time
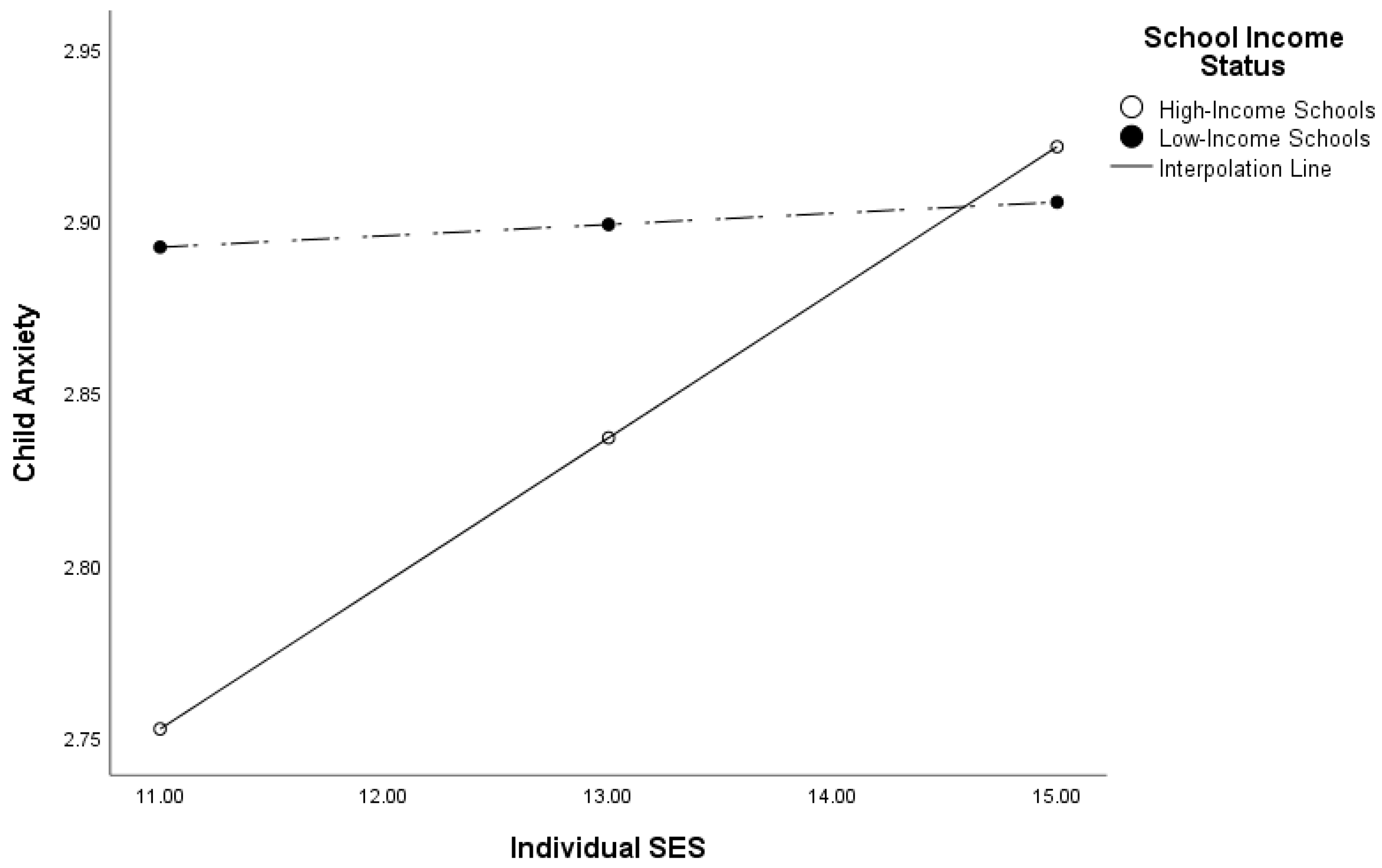
3.2. Moderation Analysis One
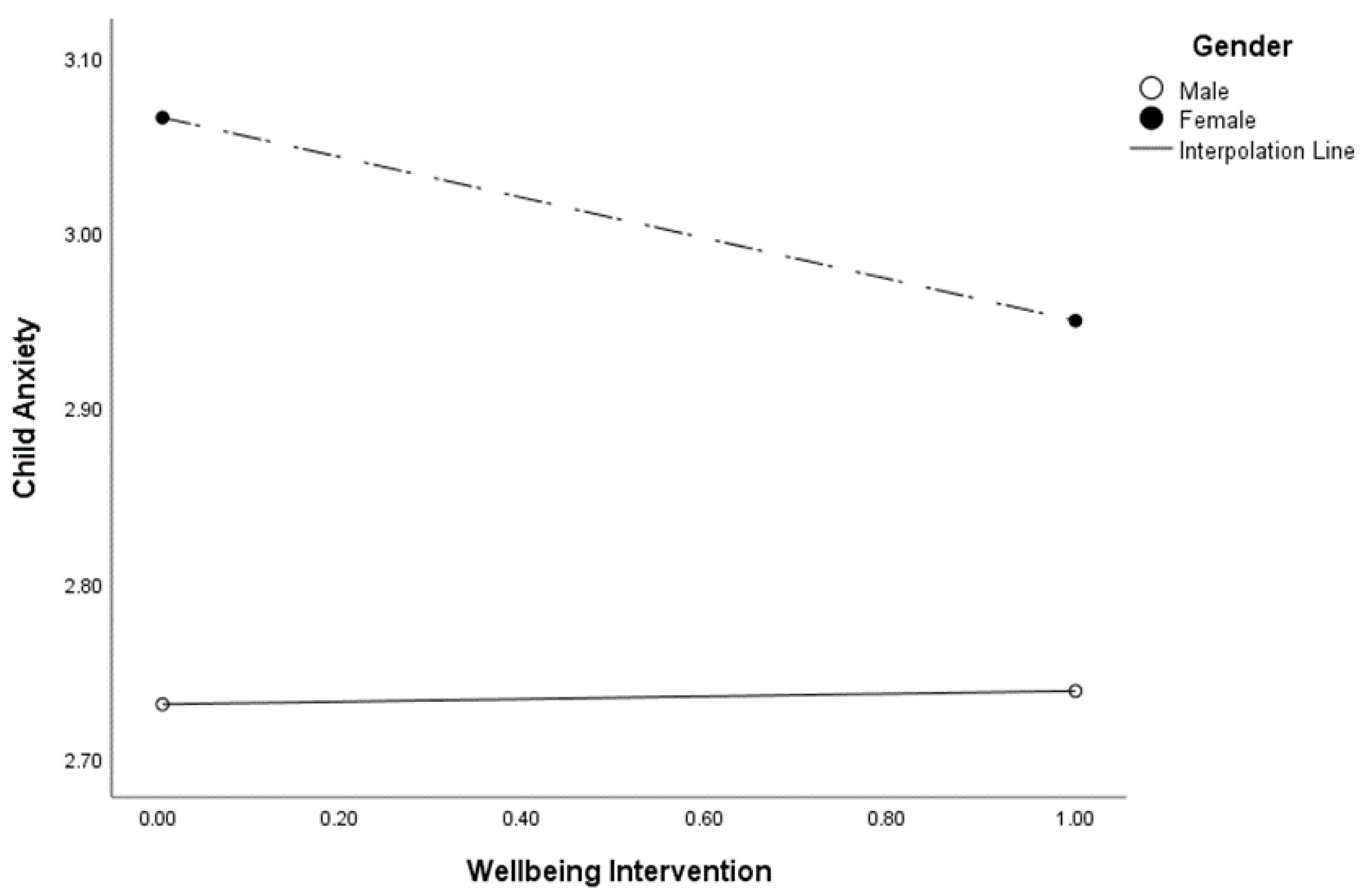
3.3. Moderation Analysis Two
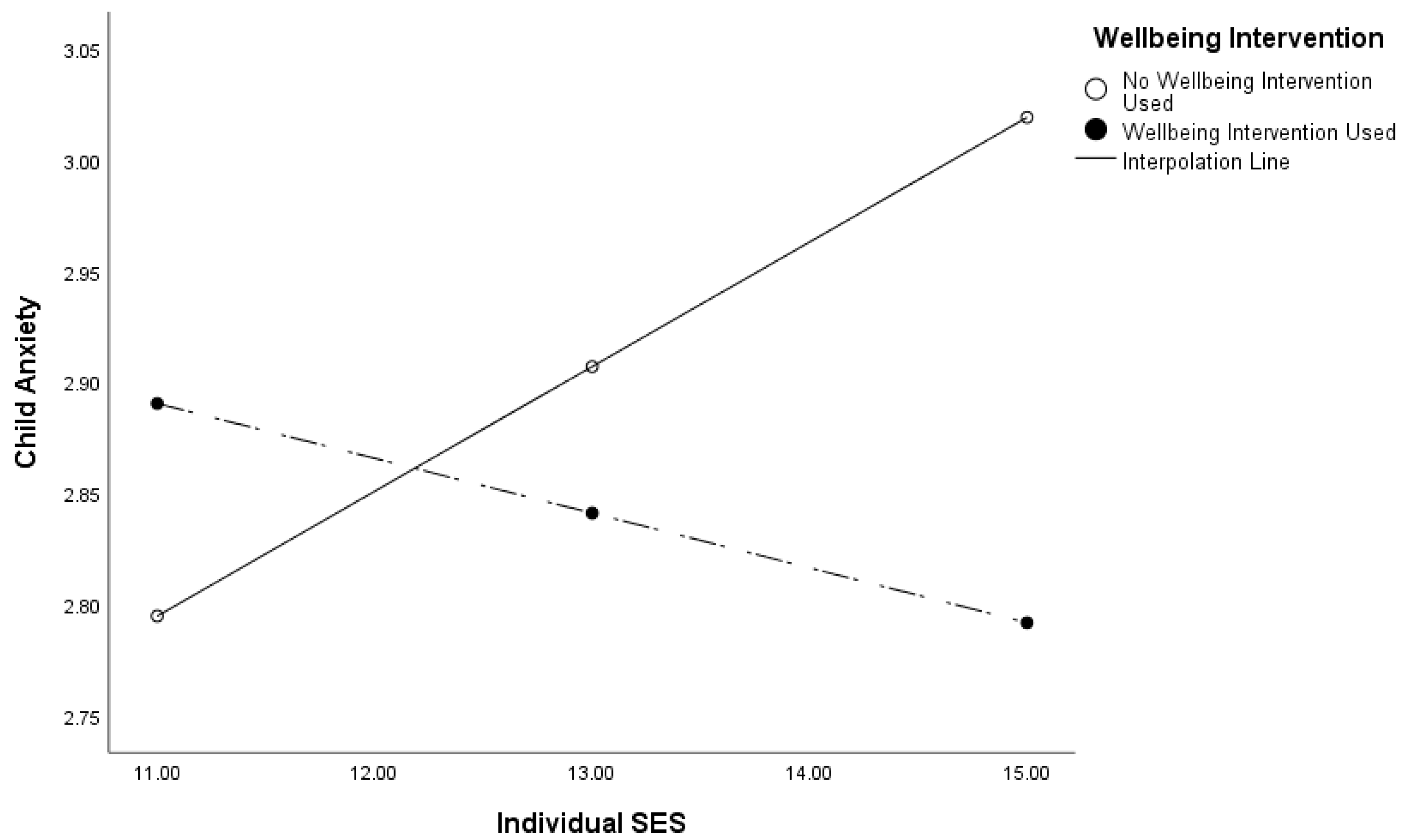
3.4. Moderation Analysis Three
4. Discussion
4.1. Anxiety Development and SES
4.2. Anxiety Development, Gender, and Wellbeing Interventions
4.3. Anxiety Development, SES, and Wellbeing Interventions
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nelemans, S.A.; Hale, W.W.; Branje, S.J.T.; Meeus, W.H.J.; Rudolph, K.D. Individual differences in anxiety trajectories from Grades 2 to 8: Impact of the middle school transition. Dev. Psychopathol. 2018, 30, 1487–1501. [Google Scholar] [CrossRef] [PubMed]
- Dooley, B.; O’Connor, C.; Fitzgerald, A.; O’Reilly, A. My World Survey 2: The National Study of Youth Mental Health in Ireland; University College Dublin School of Psychology/Jigsaw, the National Centre for Youth Mental Health: Dublin, Ireland, 2019. [Google Scholar]
- Foa, E.B.; Franklin, M.; McClean, C.; McNally, R.J.; Pine, D. Defining anxiety disorders. In Treating and Preventing Adult Mental Health Disorders: What We Know and What We Don’t Know, 2nd ed.; Evans, D.L., Foa, E.B., Gur, R.E., Hendin, H., O’Brien, C.P., Seligman, M.E.P., Walsh, B.T., Eds.; Oxford University Press: Oxford, UK, 2005; pp. 189–222. [Google Scholar]
- Collishaw, S.; Sellers, R. Trends in child and adolescent mental health prevalence, outcomes, and inequalities. In Mental Health and Illness of Children and Adolescents; Taylor, E., Verhulst, F., Wong, J.C.M., Yoshida, K., Eds.; Springer: Singapore, 2020; pp. 63–73. [Google Scholar] [CrossRef]
- Barrett, P. FRIENDS for Life: Group Leaders’ Manual for Children; Barrett Research Resources Pty Ltd.: Brisbane, Australia, 2005. [Google Scholar]
- Ruttledge, R.; Devitt, E.; Greend, G.; Mullany, M.; Charles, E.; Frehill, J.; Moriarty, M. A randomised controlled trial of the FRIENDS for Life emotional resilience programme delivered by teachers in Irish primary schools. Educ. Child Psychol. 2016, 33, 69–89. Available online: https://www.ucl.ac.uk/educational-psychology/resources/Ruttledge_et_al_2016.pdf (accessed on 3 February 2022). [CrossRef]
- Schoneveld, E.A.; Lichtwarck-Aschoff, A.; Granic, I. Preventing childhood anxiety disorders: Is an applied game as effective as a cognitive behavioral therapy-based program? Prev. Sci. 2017, 19, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Zwaanswijk, M.; van der Ende, J.; Verhaak, P.F.; Bensing, J.M.; Verhulst, F.C. Help-seeking for child psychopathology: Pathways to informal and professional services in the Netherlands. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Liber, J.M.; Van Widenfelt, B.M.; Utens, E.M.; Ferdinand, R.F.; Van der Leeden, A.J.; Van Gastel, W.; Treffers, P.D. No differences between group versus individual treatment of childhood anxiety disorders in a randomised clinical trial. J. Child Psychol. Psychiatry Allied Discip. 2008, 49, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.D.; Oberle, E.; Durlak, J.E.; Weissberg, R.P. Promoting positive youth development through school-based social and emotional learning interventions: A meta-analysis of follow-up effects. Child Dev. 2017, 88, 1156–1171. [Google Scholar] [CrossRef]
- Rooksbya, M.; Elouafkaoui, P.; Humphris, G.; Clarksona, J.; Freeman, R. Internet-assisted delivery of cognitive behavioural therapy (CBT) for childhood anxiety: Systematic review and meta-analysis. J. Anxiety Disord. 2015, 29, 83–92. [Google Scholar] [CrossRef]
- Utens, E.; Ferdinand, R. VRIENDEN voor het Leven: Werkboek voor Kinderen. Rotterdam, the Netherlands: Afdeling Kinder-en Jeugdpsychiatrie, Erasmus Medisch Centrum-Sophia Kinderziekenhuis; Afdeling Kinder—en Jeugdpsychiatrie, Erasmus Medisch Centrum—Sophia Kinderziekenhuis: Rotterdam, The Netherlands, 2006. [Google Scholar]
- Shortt, A.L.; Barrett, P.M.; Fox, T.L. Evaluating the FRIENDS program: A cognitive-behavioral group treatment for anxious children and their parents. J. Clin. Child Psychol. 2001, 30, 525–535. [Google Scholar] [CrossRef]
- Stallard, P.; Simpson, N.; Anderson, S.; Goddard, M. The FRIENDS emotional health prevention programme: 12 month follow-up of a universal UK school based trial. Eur. Child Adolesc. Psychiatry 2008, 17, 283–289. [Google Scholar] [CrossRef]
- World Health Organization (WHO). International Classification of Diseases for Mortality and Morbidity Statistics, 11th ed.; WHO: Geneva, Switzerland, 2018; Available online: https://icd.who.int/browse11/l-m/en (accessed on 19 February 2022).
- Werner-Seidler, A.; Perry, Y.; Calear, A.L.; Newby, J.M.; Christensen, H. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 51, 30–47. [Google Scholar] [CrossRef]
- Dowling, K.; Simpkin, A.J.; Barry, M.M. A cluster randomized-controlled trial of the MindOut social and emotional learning program for disadvantaged post-primary school students. J. Youth Adolesc. 2019, 48, 1245–1263. [Google Scholar] [CrossRef]
- World Health Organization. Prevention of Mental Disorders: Effective Interventions and Policy Options: Summary Report; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Carr, A. The Handbook of Child and Adolescent Clinical Psychology: A Contextual Approach; Routledge: London, UK, 2016. [Google Scholar]
- Bittner, A.; Egger, H.L.; Erkanli, A.; Costello, E.J.; Foey, D.L.; Angold, A. What do childhood anxiety disorders predict? J. Child Psychol. Psychiatry 2007, 48, 1174–1183. [Google Scholar] [CrossRef] [PubMed]
- Mifsud, C.; Rapee, R.M. Early intervention for childhood anxiety in a school setting. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Kerns, K.A.; Brumariu, L.E. Attachment in middle childhood. In Handbook of Attachment: Theory, Research and Clinical Applications, 3rd ed.; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 366–382. [Google Scholar]
- Muris, P. The pathogenesis of childhood anxiety disorders: Considerations from a developmental psychopathology perspective. Int. J. Behav. Dev. 2006, 30, 5–11. [Google Scholar] [CrossRef]
- Lijster, J.M.; Dierckx, B.; Utens, E.M.; Verhulst, F.C.; Zieldorff, C.; Dieleman, G.C.; Legerstee, J.S. The Age of Onset of Anxiety Disorders. Can. J. Psychiatry. Rev. Can. Psychiatr. 2017, 62, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Poleshuck, E.L.; Green, C.R. Socioeconomic disadvantage and pain. Pain 2008, 136, 235–238. [Google Scholar] [CrossRef]
- American Psychological Association (APA). Socioeconomic Status; American Psychological Association. 2021. Available online: https://www.apa.org/topics/socioeconomic-status (accessed on 3 March 2022).
- Farrell, A.; Kagan, S.L.; Tisdall, E.K.M. The SAGE Handbook of Early Childhood Research; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Farrell, L.; Sijbenga, A.; Barrett, P. An examination of childhood anxiety, depression and self-esteem across socioeconomic groups: A comparison study between high and low socio-economic status school communities. Adv. Sch. Ment. Health Promot. 2009, 2, 5–18. [Google Scholar] [CrossRef]
- Spencer, R.; Walsh, J.; Liang, B.; Mousseau, A.M.D.; Lund, T.J. Having it all? A qualitative examination of affluent adolescent girls’ perceptions of stress and their quests for success. J. Adolesc. Res. 2018, 33, 3–33. [Google Scholar] [CrossRef]
- Haase, T.; Pratschke, J. The 2016 Pobal HP Deprivation Index. 2017. Available online: www.trutzhaase.eu (accessed on 19 January 2023).
- Smyth, E.; McCoy, S. School experiences and post-school pathways in the Republic of Ireland. In Young Adult Development at the School-to-Work Transition: International Pathways and Processes; Marshall, E.A., Symonds, J.E., Eds.; Oxford University Press: Oxford, UK, 2021. [Google Scholar] [CrossRef]
- Symonds, J.E.; Sloan, S.; Kearns, M.; Devine, D.; Sugrue, C.; Suryanaryan, S.; Capistrano, D.; Samonova, E. Developing a social evolutionary measure of child and adolescent hedonic and eudaimonic wellbeing in rural Sierra Leone. J. Happiness Stud. 2021, 23, 1433–1467. [Google Scholar] [CrossRef]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef]
- Wanless, S.B.; Domitrovich, S.E. Readiness to implement school-based social-emotional learning interventions: Using research on factors related to implementation to maximize quality. Prev. Sci. 2015, 16, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U.; Evans, G.W. Developmental science in the 21st century: Emerging questions, theoretical models, research designs and empirical findings. Soc. Dev. 2000, 9, 115–125. [Google Scholar] [CrossRef]
- Bronfenbrenner, U.; Morris, P.A. The Bioecological Model of Human Development. Volume 1: Theoretical Models of Human Development; John Wiley and Sons Inc.: Hoboken, NJ, USA, 2007. [Google Scholar] [CrossRef]
- Rosa, E.M.; Tudge, J. Urie Bronfenbrenner’s theory of human development: Its evolution from ecology to bioecology. J. Fam. Theory Rev. 2013, 5, 243–258. [Google Scholar] [CrossRef]
- Eme, R. Developmental psychopathology: A primer for clinical paediatrics. World J. Psychiatry 2017, 7, 159–162. [Google Scholar] [CrossRef]
- Rowe, H.L.; Trickett, E.J. Student diversity representation and reporting in universal school-based social and emotional learning programs: Implications for generalizability. Educ. Psychol. Rev. 2018, 30, 559–583. [Google Scholar] [CrossRef]
- Devine, D.; Symonds, J.; Sloan, S. Children’s School Lives: Annual Report, Report No. 1; University College Dublin: Dublin, Ireland, 2019. [Google Scholar]
- Memon, M.A.; Cheahb, J.H.; Ramayah, T.; Ting, H.; Chuah, F.; Cham, T.H. Moderation analysis: Issues and guidelines. J. Appl. Struct. Equ. Model. 2019, 3, i–xi. [Google Scholar] [CrossRef]
- Hinshaw, S.; Beauchaine, S. The developmental perspective on externalizing behavior dimensions and externalizing disorders. In Oxford Handbook of Externalizing Spectrum Disorders; Beauchaine, T., Hinshaw, S., Eds.; Oxford University Press: Oxford, UK, 2016; pp. 90–104. [Google Scholar]
- Hoff, E.; Laursen, B.; Tardiff, T. Socioeconomic status and parenting. In Handbook of Parenting Volume 2: Biology and Ecology of Parenting; Bornstein, M.H., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2002; pp. 231–252. [Google Scholar]
- Bender, P.K.; Reinholdt-Dunne, M.L.; Esbjørn, B.H.; Pons, F. Emotion dysregulation and anxiety in children and adolescents: Gender differences. Personal. Individ. Differ. 2012, 53, 284–288. [Google Scholar] [CrossRef]
- Garner, P.W.; Mahatmya, D.; Brown, E.L.; Vesely, C.K. Promoting desirable outcomes among culturally and ethnically diverse children in social emotional learning programs: A multilevel heuristic model. Educ. Psychol. Rev. 2014, 26, 165–189. [Google Scholar] [CrossRef]
- Hacker, A.H.; Hayes, A. Within and beyond: Some implications of developmental contexts for reframing school psychology. Psychol. Sch. 2017, 54, 1252–1259. [Google Scholar] [CrossRef]
- Ramirez, T.; Brush, K.; Raisch, N.; Bailey, R.; Jones, S.M. Equity in social emotional learning programs: A content analysis of equitable practices in preK-5 SEL programs. Front. Educ. 2021, 6, 679467. [Google Scholar] [CrossRef]
- McCallops, K.; Barnes, T.N.; Jones, I.; Nelson, M.; Fenniman, J.; Berte, I. Incorporating culturally responsive pedagogy within social-emotional learning interventions in urban schools: An international systematic review. Int. J. Educ. Res. 2019, 94, 11–28. [Google Scholar] [CrossRef]
- Travers, J.; Balfe, T.; Butler, C.; Daly, T.; Dupont, M.; McDaid, R.; O’Donnell, M.; Prunty, A. Addressing the Challenges and Barriers to Inclusion in Irish Schools; Special Education Department, St. Patrick’s College Dublin: Dublin, Ireland, 2010; Available online: https://core.ac.uk/download/pdf/195384332.pdf (accessed on 29 March 2022).
- Rosenman, R.; Tennekoon, V.; Hill, L.G. Measuring bias in self-reported data. Int. J. Behav. Healthc. Resour. 2011, 2, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.G.; Phillips, M.R. Secondary analysis of existing data: Opportunities and implementation. Shanghai Arch. Psychiatry 2014, 26, 371–375. [Google Scholar] [CrossRef]
- Biau, D.J.; Kernéis, S.; Porcher, R. Statistics in brief: The importance of sample size in the planning and interpretation of medical research. Clin. Orthop. Relat. Res. 2008, 466, 2282–2288. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable Names | Score | N | % | ||
|---|---|---|---|---|---|
| 1 | Gender | 2279 | 100 | ||
| Boys | 1 | 1140 | 51 | ||
| Girls | 2 | 1139 | 49 | ||
| 2 | Low-income schooling | 2294 | 100 | ||
| Children in low-income schools | 1 | 1537 | 67 | ||
| Children not in low-income schools | 2 | 757 | 33 | ||
| Min–Max | N | M | SD | ||
| 3 | Child SES | 6–16 | 1947 | 12.85 | 1.91 |
| 4 | Anxiety W1 | 1–5 | 1863 | 2.64 | 1.05 |
| 5 | Anxiety W3 | 1–5 | 1978 | 2.88 | 1.01 |
| 6 | Wellbeing intervention | 0–1 | 1548 | 0.51 | 0.50 |
| 1 | 2 | 3 | 4 | 5 | ||
|---|---|---|---|---|---|---|
| 1 | Gender (Girl) | 1 | ||||
| 2 | Low-income schooling | −0.15 ** | 1 | |||
| 3 | Child SES | −0.01 | −0.16 ** | 1 | ||
| 4 | Anxiety W1 | 0.06 * | 0.02 | −0.06 * | 1 | |
| 5 | Anxiety W3 | 0.12 ** | 0.04 | 0.02 | 0.29 ** | 1 |
| 6 | Wellbeing intervention | −0.02 | 0.10 ** | 0.01 | −0.02 | −0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Halloran, T.; Symonds, J.; Bhreathnach, L.L.; Sloan, S.; Devine, D.; Martinez Sainz, G.; Davies, A. How School-Based Wellbeing Interventions, Socioeconomic Status, and Gender Impact Anxiety Development in Middle Childhood. Educ. Sci. 2023, 13, 994. https://doi.org/10.3390/educsci13100994
O’Halloran T, Symonds J, Bhreathnach LL, Sloan S, Devine D, Martinez Sainz G, Davies A. How School-Based Wellbeing Interventions, Socioeconomic Status, and Gender Impact Anxiety Development in Middle Childhood. Education Sciences. 2023; 13(10):994. https://doi.org/10.3390/educsci13100994
Chicago/Turabian StyleO’Halloran, Tracy, Jennifer Symonds, Linda L. Bhreathnach, Seaneen Sloan, Dympna Devine, Gabriela Martinez Sainz, and Aisling Davies. 2023. "How School-Based Wellbeing Interventions, Socioeconomic Status, and Gender Impact Anxiety Development in Middle Childhood" Education Sciences 13, no. 10: 994. https://doi.org/10.3390/educsci13100994
APA StyleO’Halloran, T., Symonds, J., Bhreathnach, L. L., Sloan, S., Devine, D., Martinez Sainz, G., & Davies, A. (2023). How School-Based Wellbeing Interventions, Socioeconomic Status, and Gender Impact Anxiety Development in Middle Childhood. Education Sciences, 13(10), 994. https://doi.org/10.3390/educsci13100994