Abstract
Undergraduate interprofessional courses aim to enhance health and social care students’ knowledge and skills for working life. Employing a pre-posttest design, this mixed methods study explored the impact of a new interprofessional course on content learning with the aid of mind maps. Questionnaires were used to assess the course’s effect on learning activities (including strategies for cognitive processing and regulation) and appraisals of group work. The students represented six health and social care disciplines. The results indicate that students’ content learning at the concept level was significantly improved. While participants’ cognitive, critical processing was clearly enhanced and group work appraisals became more positive, more than one in four post-course mind maps overlooked an essential concept related to interprofessional work. The more sophisticated mind maps were linked to a stepwise cognitive processing strategy and a sense of the cognitive benefits of group learning. This relatively short course did not impact regulation strategies. The study discusses the implications of these findings for effective techniques to support interprofessional learning in higher education.
1. Introduction
In the health and social care sector, students must acquire the requisite skills for interprofessional collaborative practice. In recent decades, an increasing emphasis has been placed on joint learning and collaboration with colleagues from other professional fields, and this approach is considered central to improving patient care [1,2]. Interprofessional education (IPE) provides opportunities for students and practitioners to build collective knowledge and refine collaborative skills [3,4]. By bringing different disciplines together in a shared learning environment, IPE enables students to experience interprofessional collaboration before entering the professional domain [5]. To support interactive, high-quality interprofessional learning (IPL) [6], there is clearly a need to develop effective IPE in higher education, especially as healthcare professionals and educators face increasing challenges that include an aging population, more complex health issues, and the effects of pandemics such as COVID-19. This study contributes to a better understanding of health and social care students’ interprofessional content learning during IPE and the effect on learning activities and appraisals of group work.
The available evidence confirms the positive effect of IPE on learning outcomes [5,7], but questions remain about how IPE can be optimized. The reviews of interprofessional collaborative education and practice [8,9] illustrate that many strategies such as using checklists or interprofessional team activities, which were thought to enhance interprofessional collaboration, were often unsuccessful or lacked the evidence on their effectiveness. Additionally, interprofessional collaboration may be hindered by tunnel vision if students are focused primarily on their own professional roles or if there are insufficient opportunities to interact with other professionals [10]. Mistrust, negative attitudes, and communication difficulties are among the other known barriers to interprofessional collaboration [11]. Langlois et al. [12] and Treve [13] noted that the COVID-19 pandemic increased the use of distance learning and online platforms, offering an opportunity to reflect on and enhance pedagogical strategies and innovation in higher education learning environments, including IPE. Situations where IPE educators need to “stop and think” offer beneficial insights of creating new and envisioning how learning environments could be optimized for the needs of collaborative education and practice.
The aim of the present study is to assess how a new interprofessional course and interdisciplinary learning environment impacts the content knowledge of interprofessional work of health and social care students, including learning activities such as cognitive processing, regulation strategies, and group work appraisals. We targeted less widely studied areas of IPL, such as the development of interprofessional content learning and learning activities, since they underpin the effectiveness and quality of learning in higher education.
1.1. Interprofessional Content Learning in Health and Social Care
In IPE group learning settings, ‘two or more professions learn with, from and about each other to improve collaboration and the quality of care’ [2,14]. Earlier studies of IPE have reported multiple benefits for students, including better preparation for collaborative work [15], an understanding of the value of other professions [5], and opportunities to view the patient’s situations through the eyes of another profession [16]. Students who participate in IPE subsequently display a more sophisticated understanding of interprofessional activities, issues, and contributing elements [17]. Previous IPE intervention studies have reported knowledge outcomes for topics that include professional roles, collaborative approaches, and patient safety [18]. However, more is known about IPE experiences and satisfaction than about knowledge-level changes [6], and fewer studies have explored interprofessional content knowledge in health and social care contexts. For present purposes, the term content learning is used to refer to the comprehension of key concepts and areas of interprofessional work.
One challenge for research in this area concerns the evaluation of perceived knowledge gain. In their review of IPE initiatives, Reeves et al. [7] found that evaluations of knowledge or skill changes typically rely on tools such as self-report questionnaires, and they called for more robust measures. For teachers, an understanding of the student’s conceptual and knowledge base is critical for pedagogical planning and supports for knowledge construction. Without fundamental concepts and knowledge, students cannot be expected to achieve the intended learning outcomes [19].
1.2. Effective Learning Environments
Interprofessional collaboration and learning also depend heavily on contextual factors. Reeves et al. [7] and Berger-Estilita, Fuchs, Hahn, Chiang, and Greif [20] have highlighted how the effectiveness of IPE is impacted by complex individual factors that include expectations, knowledge, insights, experiences, and attitudes. While previous studies suggest that authentic, dynamic, hybrid model learning environments with problem-based real-life scenarios [15,21,22] can be useful and improve IPL, there remains a need to clarify how effective IPE can be created and delivered [5,7,23]. It seems likely that complex and dynamic interprofessional learning environments must support deep-level learning processes and cognitive regulation. The latter contributes to metacognition, which is known to play an important role in improving thinking and learning [24,25,26,27] and in learning processes such as communication, attention, memory, problem solving, and critical thinking [28,29]. In the field of health and social care, metacognitive regulation can help to prevent medical errors through awareness of one’s own thought processes and critical reflection on thoughts and actions [29]. In this study, regulation refers to metacognitive regulation activities and regulation strategies as defined by Vermunt [27].
Vermunt [30] studied effective learning environments in order to identify the elements that influence learning quality, which include learning activities such as strategies for cognitive processing and regulation. According to Vermunt [27] (p. 26), “cognitive processing refers to content learning activities related to the acquisition of ‘knowledge, understanding and skill”. Critical processing, looking for relations and creating examples of the subject matter are examples of cognitive processing. Regulation strategies, such as planning and monitoring the learning process, govern both cognitive and affective activities. The use of these learning activities can determine the quality of achieved learning outcomes [27,30]. In higher education, where solving complex tasks depends on high-level learning, regulation can improve the quality of learning outcomes. In interprofessional learning environments, students encounter diverse views, thoughts, and perspectives on knowledge from different disciplines and professions. As this may challenge cognitive processing and make greater demands on metacognitive regulation [31,32], effective teaching and learning should acknowledge and support regulation skills, especially in online learning situations [33].
1.3. Interprofessional Collaborative Learning
Fostering collaborative learning is arguably the core requirement for IPE [5]. During the collaborative process, the key activity is learning together to address the assignment or problem at hand [34]. Interprofessional collaborative learning provides an opportunity to build content knowledge while also learning about each other’s professional roles [35,36]. However, it would be wrong to assume that collaborative activities automatically produce high-quality learning or intended outcomes. For example, attitudes to interprofessional collaboration can affect the benefits of participation in IPE [37]. In particular, as a negative attitude can hinder collaborative learning, especially in IPL contexts, it is important to help students to see others as a potential resource [10] and to address any negative assumptions or stereotypical thinking about other professions [38].
Previous research suggests that students are usually willing and ready to participate in IPE and exhibit positive attitudes [7,20,38,39]. Dallaghan, Hultquist, Nickol, Collier, and Geske [40] and Tervaskanto-Mäentausta [41] reported that positive attitudes persist over the long term, but there is mixed evidence regarding the effects of IPE on attitudes. In their review, Berger-Estilita et al. [20] reported no change in attitude in 9 of 23 IPE interventions, and in one case, negativity increased. Hammick et al. [15] reported that while attitudes to collaborative learning were positive, perceptions of other professionals in the team remained unchanged or even declined following IPE.
1.4. Research Questions
As research in this area has devoted relatively little attention to content learning during IPL, the present study sought to clarify how the Monelle course Interprofessional Competence in Care and Rehabilitation affects students’ concept-level learning about the core themes of interprofessional work. The goal was to assess the acquisition of core content during the course rather than merely assuming that this occurs. We were also interested in how the diversity of disciplines in this new course would affect student learning activities, as the role of cognitive processing or regulation strategies in IPL, and how the learning environment impacts students’ appraisals of group work and links to content learning. To that end, we addressed the following research questions.
- How do the core concepts of interprofessional work develop during the Monelle course?
- How do students’ cognitive processing strategies, regulation strategies, and group work appraisals change during the Monelle course?
- Are cognitive processing strategies, regulation strategies, and group work appraisals linked to the development of core content?
2. Materials and Methods
To analyze changes in knowledge building during the Monelle course, we employed a mixed methods design that enabled us to gather versatile data with pre- and post-measurement points. Using multiple methods that included content and statistical analyses, we sought to develop a more comprehensive understanding of the new learning environment and its effects on student learning and appraisals.
2.1. Research Setting
The Monelle course was a joint effort involving two universities and one university of applied sciences in a city in southern Finland. The 2.5-month-long course was both interdisciplinary and interprofessional, with health and social care undergraduates studying medicine, occupational therapy, physiotherapy, psychology, social science/services, and speech therapy. We characterize the course as interprofessional because participants will enter one of the social or health professions following graduation [42]. The main goal for students attending the course was to learn about interprofessional collaboration and the essentials of interprofessional work. The course learning outcomes included enhanced competencies in recognizing, evaluating, and addressing interdisciplinary health problems and patient/customer needs; familiarization with the roles and duties of those involved in interprofessional patient care; and enhanced consultation and interaction skills.
This optional course was offered to undergraduate students who had been studying for at least two years. Teaching methods included face-to-face interaction, online small-group learning, and seminars to discuss the online assignment with teachers. The course opened with lectures that addressed topics such as interprofessional collaboration, interaction in client work, service structure, and health and social services legislation. Participants then completed a four-week online group assignment based on a patient case in small groups of 6 or 7 people. To ensure an interprofessional dimension, majority of the groups included students from each of the participating disciplines. The online assignment was designed to foster IPL, enabling students to benefit from the knowledge and skills of the other professions by collaborating like a real interprofessional team. The groups also practiced consultative work, enhancing their ability to listen to the views of others, reflect on their own expertise, and develop new perspectives through dialog and group discussion. A named teacher was assigned to each group for support and experts to consult in each of the professional disciplines. Case assignments were subsequently presented and discussed in the course seminars. Course outcomes were assessed on a binary scale of pass/fail.
2.2. Participants and Data Collection
All participants in the Monelle course were offered an opportunity to participate in this study at the beginning of the first lecture. Of the 57 students on the course, 52 (91%) consented to participate in the present study, and this defined the sample size. All data (mind maps and self-report questionnaires) were received at the beginning and end of the course from 43 participants, with the exception of the ILS questionnaire data, which were collected from 40 participants. The sample included 38 females and 5 males; a majority (44%) reported their age as 25–30 years.
2.2.1. Mind Maps
The development of content learning during the course was tracked using mind maps, which visualize associations between ideas from different topics [43]. The aim was to comprehend the links between participants’ ideas about interprofessional work at a conceptual level. Novak [44] (p. 550) defines concepts as “perceived regularities in events or objects … designated by a label (usually a word)”. As a pedagogical tool, concept maps are used to promote quality learning through critical thinking, reflection, and linking theory and practice. Mind maps can also be used as a tool for learning assessment in higher education settings [45]. One advantage of the mind map is that it encourages the user to record anything that seems connected to the main topic, which means it is less strict than concept mapping [43,46,47]. The present study used a mixed-mode or ‘hybrid format’ mind map [46] that incorporates concepts but provides clear and simple guidelines.
Mind map data were collected from each student in a natural setting at the beginning of the first lecture and again later, before the first seminars—an interval of eight weeks. To guide their responses, the mind map posed a focus question [48]: “In your opinion, what are the elements of interprofessional work? Map these core elements and their connections. You can use arrows to describe the connections”. Three general models of mind maps were shown briefly to the participating students to acquaint them with the approach. The guidelines were deliberately kept to a minimum, and to avoid influencing participants’ ideas about the central topic (interprofessional work), no predefined concepts were provided. Participants were allowed 10 min to draw their maps. The same procedure was used in the post-assignment follow-up (without mentioning the three mind map models).
2.2.2. Self-Report Questionnaires
In addition to the mind maps, we collected data from two self-report questionnaires. The first questionnaire—Part A, Study Activities from the Inventory of Learning Styles (ILS) [49]—was chosen for its relevance to the study context. It measures two domains of student learning: processing strategies (Deep processing, Stepwise processing, and Concrete processing scales) and regulation strategies (Self-regulation, External regulation, and Lack of regulation scales). Participants were asked to respond to the questionnaire’s 55 statements on a five-point Likert scale (1 = I do this seldom or never; 2 = I do this sometimes; 3 = I do this regularly; 4 = I do this often; 5 = I do this almost always). The second questionnaire was a contextualized version of Volet’s [50] Students’ Appraisals of Group Assignments (SAGA). This instrument was used to capture participants’ appraisals of a specific group work assignment and to clarify their thoughts, skills, and willingness to engage in group work. SAGA comprises six scales: Cognitive benefits, Motivational influence, Group assessment, Affect, Management, and Interpersonal. Students responded to the questionnaire’s 30 statements on a four-point Likert scale (1 = strongly disagree; 2 = disagree; 3 = agree; 4 = strongly agree).
Both questionnaires were translated from English to Finnish by the researcher (the first author of the present article) with the help of the university’s language center. The translations’ validity and reliability were verified by a group of educational and medical experts, who read the questions and noted any issues regarding clarity. The transcribed questionnaires were then converted to the Webropol electronic survey format, and the survey link was emailed to course participants who had agreed to participate in the study. The data from both questionnaires were gathered during the first days of the course (pre-test) and again at the end of the course (post-test). In statistical reliability tests, most of the relevant ILS and SAGA scales achieved acceptable Cronbach’s alpha values ranging from 0.60 to 0.90. The exception was the SAGA Interpersonal scale, which failed to reach the cutoff value and was therefore excluded.
2.3. Data Analysis
2.3.1. Mind Map Content Analysis and Categorization
In this mixed methods study, both qualitative and quantitative methods were used to analyze the data. The concepts used in mind maps were first analyzed and categorized using content analysis [51] (Stemler, 2001). To focus on participants’ content learning, we developed a categorization scheme for the mind maps that reflected the three essential conceptual themes of interprofessional work: (1) who (referring to the different professions involved); (2) to whom (referring to patients/customers/rehabilitants); and (3) how (referring to interactions between professionals—for example, consulting, information sharing, and collaboration). These three themes were defined as core concepts based on a theoretical definition of interprofessional collaborative practice [2] and were, therefore, expected to appear in the mind maps. The three themes were also embedded in the Monelle course’s learning outcomes. The categories were developed in consultation with two local university experts, both being coordinators and teachers in the field of IPE. The mind map data were co-coded with one of them. The co-coding with the main author reached inter-rater reliability estimation of 88% agreement. In cases where the coders’ categorizations did not agree, a final agreement was reached through discussion.
After the development of categorization scheme the mind maps were further analyzed. There were four distinct categories of mind map (see Table 1): category 1 (incorporating only one core concept); category 2 (incorporating two core concepts); category 3 (incorporating all three core concepts); and category 4 (incorporating all three core concepts plus additional concepts). As all of the analyzed maps included at least one core concept, there was no category 0. The maps were further classified as adequate or inadequate for the purposes of categorization and for the later use of statistical analyses. The “adequate” maps included one or more core concepts of each essential theme (1 “who”, 2 “to whom, 3 “how”). Any map that lacked even one of the core concepts was classified as “inadequate”, and this distinction facilitated statistical comparison.

Table 1.
Categories of content learning based on core mind map concepts.
To make the analysis more explicit, the mind maps were further categorized. The main categories (1–3) were classified by the number of additional clarifying concepts (0 = none, 1 = one clarification, 2 = two clarifications, 3 = three or more clarifications). The number of clarifications were seen to reflect a more refined or sophisticated knowledge of a particular concept. The concepts in categories were subsequently quantified using mean scores based on the total of clarifying concepts, with a maximum point of 9 (for three or more clarifications of all three core concept categories). For example, when mind map included the core concept “who” 3 times, “to whom” 0 times, and “how” 2 times, the total score of the map was 5 and mean score 0.56. Finally, the scores of pre- and post-maps were combined and compared to the self-reported questionnaire data.
2.3.2. Statistical Analyses
The questionnaire data were analyzed using IBM SPSS Statistics 24. The first research question (How do the core concepts of interprofessional work develop during the Monelle course?) was addressed by means of content analysis. The second and third questions (How do students’ cognitive processing strategies, regulation strategies, and group work appraisals change during the Monelle course? and Are cognitive processing strategies, regulation strategies, and group work appraisals linked to the development of core content?) were addressed using t-tests and logistic regression. For pre- and post- measurement points on the ILS and SAGA scales and subscales, t-tests were performed to identify any changes in self-reported evaluations of cognitive and regulative strategies and group work appraisals. Mean mind map scores were also subjected to t-tests. In the case of the third research question, logistic regressions were performed to assess any links between the development of content learning and self-evaluation of learning activities (cognitive processing strategies and regulation strategies) and group work appraisals, again based on mean mind map scores.
3. Results
3.1. Interprofessional Content Learning
The first objective was to explore how the interprofessional learning environment affects interprofessional content learning at the concept level. The pre- and post-test comparison of mind maps at the beginning and end of the course revealed statistically significant changes in participants’ content learning (pre-test: M = 0.60, SD = 0.24; post-test: M = 0.68, SD = 0.23; t (43) −2.30, p = 0.04). Looking in detail at each core concept (see Figure 1), we found that concept 1 (who) was mentioned frequently in most (93%) of the pre-maps (n = 40) and post-maps (95%) (n = 41). The most common defect was the omission of concept 2 (to whom), which was mentioned in 74% (n = 32) of pre-maps and in 79% (n = 34) of post-maps. Concept 3 (interaction) showed the greatest increase: from 84% of pre-maps (n = 36) to 98% of post-maps (n = 42). All three concepts were present in 51% (n = 22) of pre-maps and in 72% (n = 31) of post-maps; in other words, at least one core concept was missing in 28% of the students’ mind maps (n = 12) at the end of the course.
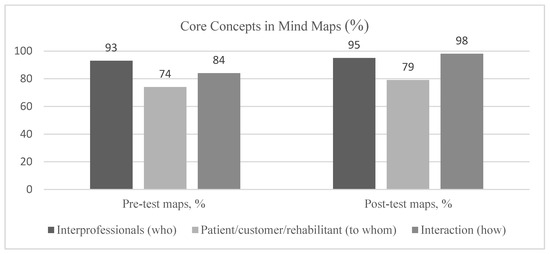
Figure 1.
Incidence of core concepts in pre- and post-test maps (%): main categories.
In summary, the Monelle interprofessional learning environment helped students to develop a more sophisticated understanding of the key content at a conceptual level, but there is a need to strengthen awareness of the core element of patient/customer/rehabilitant.
3.2. The Change in Students’ Learning Activities and Group Work Appraisals
A second objective of the current study was to investigate how the interprofessional learning environment affected learning activities as measured by ILS, including cognitive processing and regulation strategies. Comparing pre- and post-test data, t-tests revealed significant development in the domain of cognitive processing on the Critical processing subscale of Deep processing (pre-test: M = 2.12, SD = 0.76; post-test: M = 3.14, SD = 0.88; t (39) −12.017, p = 0.00). Participant self-evaluations indicate that interprofessional studies enhanced this capability, but no other statistically significant changes in cognitive processing or regulation strategies were observed between pre- and post-test.
Individual Appraisals of Group Work
t-tests to assess participants’ willingness and ability to participate in assigned interprofessional group work on the SAGA scales found that group assessment and management were significantly enhanced during the Monelle course. After the course, students were more satisfied with group assessments than before (pre-test: M = 3.27, SD = 0.49; post-test: M = 3.45, SD = 0.44; t (42) −2.50, p = 0.017). Group assessment was considered suitable for this assignment, and the management of small-group learning was seen to be easier than anticipated (pre-test: M = 2.79, SD = 0.38; post-test: M = 2.94, SD = 0.51; t (42) −2.29, p = 0.027). Management included reaching a consensus and ensuring effective coordination during the group assignment. The results indicate that the course enhanced attitudes to mutual learning appraisals, but there were no significant post-test changes in scores on the other three SAGA scales (Cognitive benefits, Motivational influence, and Affect).
3.3. The Link between Content Learning, Learning Activities, and Group Work Appraisals
Combining ILS and SAGA data with the results for adequate and inadequate mind maps, logistic regressions confirmed that stepwise processing (ILS) and cognitive benefits (SAGA) were linked to more sophisticated (adequate) mind maps at the end of the course. The stepwise processing results indicate improved learning quality based on strategies that include memorizing, rehearsing, and analyzing: B = 2.841, p = 0.029, OR = 17.139, (1.333, 220.358). Cognitive benefits include knowledge enrichment and opportunities to consider different views and to rethink one’s own ideas while learning with others. Opportunities to learn with peers were seen as a versatile cognitive advantage: B = −3.779, p = 0.045, OR = 0.023, (0.001, 0.926).
4. Discussion
The present study explored how an interprofessional learning environment affected content learning among health and social care students in terms of concept-level development. The study also investigated learning activities that included cognitive processing and regulation strategies and group work appraisals.
4.1. Interprofessional Content Learning
Regarding the first research question, the Monelle interprofessional learning environment supported content learning of interprofessional work. Specifically, the course helped students to learn about interprofessional interaction (i.e., the how of consulting, information sharing, delegating, etc.), which was one of the intended learning outcomes. However, another central concept, to whom (i.e., patient/customer/rehabilitator), was most frequently omitted in both pre- and post-test mind maps; despite the lectures and patient case assignments, this learning outcome was not fully achieved. As patients are at the center of every healthcare system and are increasingly seen as partners and an integral part of the interprofessional team [1], this study finding represents an alarming gap in the participants’ thinking. Previous studies have shown that IPE learners’ are motivated to focus on the patient and their experience [52]. Still, interprofessional discussions could lack a patient-centered perspective, indicating a strong focus on interprofessional interactions rather than on the patient [53]. In the present case, this suggests the possibility of tunnel vision or an undue focus on professional roles [10], which is typical of novice thinking.
To support comprehensive knowledge construction, educators should consider using techniques such as concept mapping or mind maps (as in the present study) to disclose teachers’ and students’ cognitive processes and gaps in understanding [45,54,55]. These techniques can help to build a fuller understanding of interprofessional work.
4.2. Changes in Students’ Cognitive Processing and Regulation Strategies and Group Work Appraisals
The present study also sought to explore how a diverse interprofessional learning environment would affect learning activities and group work appraisals, both of which are important factors in the quality of learning processes. The observed development of a critical approach to the course subject matter reflects a clear shift in cognitive strategy and enhanced deep-level learning. Specifically, this strategy involves asking questions, forming personal opinions, and drawing one’s own conclusions [27,30]. The interprofessional learning environment and consultative approach encouraged critical processing (i.e., comparing knowledge and drawing one’s own conclusions). A heterogeneous mix of learners and a non-threatening atmosphere [42] can create a learning environment that accommodates different views and interpretations, which students must then process. Intriguingly, none of the participants’ other self-evaluations of learning activities changed notably in the present case.
The ability to ask questions and to analyze and solve problems are among the critical thinking skills currently considered crucial in higher education [56]. Regulation skills also play an important role, especially in IPL settings, where students must cope with demanding cognitive tasks and dynamic interactions. In practice, facilitating a questioning approach is likely to support both high-level content processing and regulation of learning during collaborative work [57]. In addition, learning methods such as concept mapping enable teachers to support students’ cognitive and metacognitive learning processes [55], allowing them to take control of their own learning [58].
Along with regulation of learning, attitudes play a key role in successful collaborative learning [59]. Our findings indicate that, despite the level of participant diversity and enhanced critical processing, perceptions of group work were more positive at the end of the course, especially in the areas of management and assessment. This aligns with earlier reports of improved evaluations of IPE [7,60]. These findings suggest that learning together in interprofessional small groups is successful in many ways and supports the development of interaction skills as a key learning outcome.
4.3. The Role of Learning Activities and Appraisals in Core Content Learning
Regarding the third research question, the present findings indicate a clear association between core content learning and more sophisticated mind maps. The first scale measured a cognitive learning activity known as stepwise processing within the domain of processing strategies. This form of learning involves thorough analytical processing of separate elements of the subject matter [27]. The participating students who said they study in this stepwise way produced more adequate mind maps at the end of the course.
More sophisticated mind maps were also linked to the perceived cognitive benefits of group learning. In other words, students produced more adequate maps if they viewed group work as an opportunity to enrich their knowledge, rethink their ideas, learn from others, and receive feedback. These findings align with Raidal and Volet [59], who reported a positive correlation between the perceived cognitive benefits of social learning and a constructivist conception of learning. Similarly, Mebert et al. [22] reported that students found other disciplinary perspectives particularly rewarding and improving their learning experiences. From an instructional point of view, these findings confirm the importance of making students explicitly aware of the benefits of learning together. This deeper understanding can enhance learning and attitudes; for example, Clinton and Kelly [61] found that students who were given a rationale for collaborative discussion changed their attitude and developed an enhanced awareness of the utility and relevance of group discussion as compared to a control group.
During this interprofessional course, students achieved many (but not all) of the key learning outcomes. The interprofessional learning environment served to enhance students’ knowledge of interprofessional work and their experience of interacting with students from different disciplines. However, it also seems clear that the intense focus on interprofessional interactions may have distracted from the issue of patient and customer needs, which should be of central concern to health and social care professionals. This has an obvious practical implication for future instructional design: the need to emphasize the essential role of the patient or customer. Our findings suggest that health and social care students can benefit from teaching practices that offer tools for assessing new and existing knowledge. This interprofessional learning environment successfully enabled interprofessional interaction and promoted a positive learning experience, which Wei et al. [11] identified as a key element of functional professional communication and practice.
4.4. Limitations
The present study has some limitations. The use of self-report measures can be seen as a limitation, as these rely entirely on participants’ own evaluations and may not correspond to their actual behavior. Although the co-coders achieved an acceptable level of inter-rater reliability, the analysis of the mind maps inevitably entails an element of interpretation, and researchers may diverge from the respondent’s intended meaning. As a related issue, the categorization scheme may not have allowed sufficient scope to capture the extent of content improvement among higher-achieving students. Overall, the generalizability of our results is weakened by the small sample size and the case study approach, which failed to address the sustainability of any changes in knowledge (concepts), learning activities, or appraisals. This is a common weakness in IPE research [1,18], especially in the case of outcomes at the undergraduate level [7]. Therefore, longitudinal follow-up studies are the only way of determining how IPE interventions alter practice [20]. Nevertheless, the study has some strengths, including the use of mixed methods, the involvement of multiple disciplines, and the generation of new insights for supporting quality IPL and future IPE initiatives. As Reeves et al. [9] noted, there is a need for further research on IPE and associated collaborative practices, using rigorous mixed-methods to explore individual and group-level interactions.
5. Conclusions
The results of the present study reinforce the importance of ensuring that health and social care students can access IPE during their undergraduate studies. It can be challenging to create an effective interprofessional learning environment because of its complex and dynamic nature. Crucially, such environments should simulate real-world problem-solving situations involving students and experts from all relevant disciplines. Interactive and effective IPL also depends on teaching tools that support comprehensive knowledge construction and deep-level learning strategies and highlight the benefits of collaborative learning to enable students to build essential interprofessional skills. As well as devising ways of helping students to focus more on the patient, the processes of knowledge co-construction and metacognitive regulation that contribute to the success of IPL must be studied in greater depth.
Author Contributions
Conceptualization, E.Ö., T.I., O.K.-S. and M.M.; methodology, E.Ö., T.I. and M.M.; validation, E.Ö., T.I., M.-K.W. and M.M.; formal analysis, E.Ö.; investigation, E.Ö.; resources, E.Ö.; data curation, E.Ö.; writing—original draft preparation, E.Ö.; writing—review and editing, E.Ö., T.I., M.-K.W., O.K.-S. and M.M.; visualization, E.Ö.; supervision, T.I., O.K.-S. and M.M.; project administration, E.Ö.; funding acquisition, E.Ö. All authors have read and agreed to the published version of the manuscript.
Funding
The author Erika Österholm acknowledge receipt of financial support for the research, writing, and/or publication of this article from The Finnish Medical Society Duodecim (Grant 11/2017), Turku University Foundation (Grant 4/2021).
Institutional Review Board Statement
The study was conducted according to the ethical regulation and with ethical approval of the Ethics Committee for Human Sciences at University of Turku (Archive 46/2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
The authors wish to acknowledge the help of Eero Laakkonen with statistical matters and the advice in analysis of Miia Tuominen at University of Turku and the support of all the teachers of Monelle.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Institute of Medicine. Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes; The National Academic Press: Washington, DC, USA, 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK338360/ (accessed on 21 May 2020).
- World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice; WHO: Geneva, Switzerland, 2010; Available online: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice (accessed on 11 November 2021).
- Bridges, D.R.; Davidson, R.A.; Odegard, P.S.; Maki, I.V.; Tomkowiak, J. Interprofessional collaboration: Three best practice models of interprofessional education. Med. Educ. Online 2011, 16, 6035. [Google Scholar] [CrossRef] [PubMed]
- Hammick, M.; Olckers, L.; Campion-Smith, C. Learning in interprofessional teams: AMEE guide no 38. Med. Teach. 2009, 31, 1–12. [Google Scholar] [CrossRef]
- Guraya, S.Y.; Barr, H. The effectiveness of interprofessional education in healthcare: A systematic review and meta-analysis. Kaohsiung J. Med. Sci. 2018, 34, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Thistlethwaite, J. Interprofessional education: A review of context, learning and the research agenda. Med. Educ. 2012, 46, 58–70. [Google Scholar] [CrossRef] [PubMed]
- Reeves, S.; Fletcher, S.; Barr, H.; Birch, I.; Boet, S.; Davies, N.; McFadyen, A.; Rivera, J.; Kitto, S. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med. Teach. 2016, 38, 656–668. [Google Scholar] [CrossRef]
- Brandt, B.; Lutfiyya, M.N.; King, J.; Chioreso, C. A scoping review of interprofessional collaborative practice and education using the lens of the Triple Aim. J. Interprof. Care 2014, 28, 393–399. [Google Scholar] [CrossRef]
- Reeves, S.; Pelone, F.; Harrison, R.; Goldman, J.; Zwarenstein, M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2017, 6, CD000072. [Google Scholar] [CrossRef]
- Tran, C.; Kaila, P.; Salminen, H. Conditions for interprofessional education for students in primary healthcare: A qualitative study. BMC Med. Educ. 2018, 18, 122. [Google Scholar] [CrossRef]
- Wei, H.; Horns, P.; Sears, S.F.; Huang, K.; Smith, C.M.; Wei, T.L. A systematic meta-review of systematic reviews about interprofessional collaboration: Facilitators, barriers, and outcomes. J. Interprof. Care 2022, 36, 735–749. [Google Scholar] [CrossRef]
- Langlois, S.; Xyrichis, A.; Daulton, B.J.; Gilbert, J.; Lackie, K.; Lising, D.; MacMillan, K.; Najjar, G.; Pfeifle, A.L.; Khalili, H. The COVID-19 crisis silver lining: Interprofessional education to guide future innovation. J. Interprof. Care 2020, 34, 587–592. [Google Scholar] [CrossRef]
- Treve, M. What COVID-19 has introduced into education: Challenges facing higher education institutions (HEIs). High. Educ. Pedagog. 2021, 6, 212–227. [Google Scholar] [CrossRef]
- CAIPE. Interprofessional Education—A Definition; CAIPE: London, UK, 2002; Available online: https://www.caipe.org.uk (accessed on 5 February 2020).
- Hammick, M.; Freeth, D.; Koppel, I.; Reeves, S.; Barr, H. A best evidence systematic review of interprofessional education: BEME guide no. 9. Med. Teach. 2007, 29, 735–751. [Google Scholar] [CrossRef] [PubMed]
- Clark, P.G. What would a theory of interprofessional education look like? Some suggestions for developing a theoretical framework for teamwork training. J. Interprof. Care 2006, 20, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Pollard, K.; Rickaby, C.; Miers, M. Evaluating Student Learning in an Interprofessional Curriculum: The Relevance of Pre-Qualifying Inter-Professional Education for Future Professional Practice. Project Report, Higher Education Academy, Health Sciences and Practice. 2008. Available online: https://www.caipe.org/topic/resources/publications (accessed on 25 March 2020).
- Abu-Rish, E.; Kim, S.; Choe, L.; Varpio, L.; Malik, E.; White, A.A.; Craddick, K.; Blondon, K.; Robins, L.; Nagasawa, P.; et al. Current trends in interprofessional education of health sciences students: A literature review. J. Interprof. Care 2012, 26, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, P.; Sweller, J.; Clark, R.E. Why minimal guidance during instruction does not work: An analysis of the failure of constructivist, discovery, problem-based, experiential, and inquiry-based teaching. Educ. Psychol. 2006, 41, 75–86. [Google Scholar] [CrossRef]
- Berger-Estilita, J.; Fuchs, A.; Hahn, M.; Chiang, H.; Greif, R. Attitudes towards interprofessional education in the medical curriculum: A systematic review of the literature. BMC Med. Educ. 2020, 20, 254. [Google Scholar] [CrossRef]
- Inoa, R.; Sullivan, K.; Giordano, K.; Wynarczuk, K. The process of developing a hybrid interprofessional education initiative for graduate students. High. Educ. Pedagog. 2022, 7, 179–200. [Google Scholar] [CrossRef]
- Mebert, L.; Barnes, R.; Dalley, J.; Gawarecki, L.; Ghazi-Nezami, F.; Shafer, G.; Slater, J.; Yezbick, E. Fostering student engagement through a real-world, collaborative project across disciplines and institutions. High. Educ. Pedagog. 2020, 5, 30–51. [Google Scholar] [CrossRef]
- Lindvig, K.; Ulriksen, L. Different, difficult and local: A review of interdisciplinary teaching activities. Rev. High. Educ. 2019, 43, 697–725. [Google Scholar] [CrossRef]
- Flavell, J.H. Speculations about the nature and development of metacognition. In Metacognition, Motivation, and Understanding; Weinert, F.E., Kluwe, R., Eds.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1987; pp. 21–29. [Google Scholar]
- Schraw, G. Promoting general metacognitive awareness. Instr. Sci. 1998, 26, 113–125. [Google Scholar] [CrossRef]
- Schraw, G.; Moshman, D. Metacognitive theories. Educ. Psychol. Rev. 1995, 7, 351–371. [Google Scholar] [CrossRef]
- Vermunt, J.D. Metacognitive, cognitive and affective aspects of learning styles and strategies: A phenomenographic analysis. High. Educ. 1996, 31, 25–50. [Google Scholar] [CrossRef]
- Flavell, J.H. Metacognition and cognitive monitoring: A new area of cognitive–developmental inquiry. Am. Psychol. 1979, 34, 906–911. [Google Scholar] [CrossRef]
- Medina, M.S.; Castleberry, A.N.; Persky, A.M. Strategies for improving learner metacognition in health professional education. Am. J. Pharm. Educ. 2017, 81, 78. [Google Scholar] [CrossRef] [PubMed]
- Vermunt, J.D. The power of teaching-learning environments to influence student learning. In Student Learning and University Teaching; Entwistle, N.J., Thomlinson, P., Eds.; British Psychological Society: London, UK, 2007; pp. 73–90. [Google Scholar]
- Järvelä, S.; Kirschner, P.A.; Panadero, E.; Malmberg, J.; Phielix, C.; Jaspers, J.; Koivuniemi, M.; Järvenoja, H. Enhancing socially shared regulation in collaborative learning groups: Designing for CSCL regulation tools. Educ. Technol. Res. Dev. 2015, 63, 125–142. [Google Scholar] [CrossRef]
- Raes, A.; Schellens, T.; De Wever, B.; Benoit, D.F. Promoting metacognitive regulation through collaborative problem solving on the web: When scripting does not work. Comput. Hum. Behav. 2016, 58, 325–342. [Google Scholar] [CrossRef]
- Sánchez-Martí, A.; Ciraso-Calí, A.; Fernández-Sequi, H.; Pineda-Herrero, P. The school-life balance effect on acquiring cross-disciplinary competences in VET: Disruption or continuity during COVID-19? Vocat. Learn. 2023, 16, 207–226. [Google Scholar] [CrossRef]
- Teasley, S.D.; Roschelle, J. Constructing a joint problem space: The computer as a tool for sharing knowledge. In Computers as Cognitive Tools; Lajoie, S., Deny, S., Eds.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1993; pp. 229–258. [Google Scholar]
- Barr, H.; Koppel, I.; Reeves, S.; Hammick, M.; Freeth, D. Effective Interprofessional Education—Argument, Assumption and Evidence; Blackwell: Oxford, UK, 2005. [Google Scholar]
- Ciani, G.J.; Grimaldi, G.; Macalintal, M.; Orner, D. The Impact of Interprofessional Education on Health Profession Students’ Professional Identity. Educ. Sci. 2023, 13, 494. [Google Scholar] [CrossRef]
- Coster, S.; Norman, I.; Murrells, T.; Kitchen, S.; Meerabeau, E.; Sooboodoo, E.; d’Avray, L. Interprofessional attitudes amongst undergraduate students in the health professions: A longitudinal questionnaire survey. Int. J. Nurs. Stud. 2008, 45, 1667–1681. [Google Scholar] [CrossRef]
- Williams, B.; McCook, F.; Brown, T.; Palmero, C.; McKenna, L.; Boyle, M.; Scholes, R.; French, J.; McCall, L. Are undergraduate health care students “ready” for interprofessional learning? A cross-sectional attitudinal study. Internet J. Allied Health Sci. Pract. 2012, 10, 4. [Google Scholar] [CrossRef]
- Wang, Z.; Feng, F.; Gao, S.; Yang, J. A systematic meta-analysis of the effect of interprofessional education on health professions students’ attitudes. J. Dent. Educ. 2019, 83, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Dallaghan, B.; Hultquist, T.B.; Nickol, D.; Collier, D.; Geske, J. Attitudes toward interprofessional education improve over time. J. Interprof. Educ. Pract. 2018, 13, 24–26. [Google Scholar] [CrossRef]
- Tervaskanto-Mäentausta, T. Interprofessional Education during Undergraduate Medical and Health Care Studies. Ph.D. Thesis, University of Oulu, Oulu, Finland, 2018. Available online: http://jultika.oulu.fi/files/isbn9789526218571.pdf (accessed on 15 November 2019).
- Oandasan, I.; Reeves, S. Key elements for interprofessional education. Part 1: The learner, the educator and the learning context. J. Interprof. Care 2005, 1, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Davies, M. Concept mapping, mind mapping and argument mapping: What are the differences and do they matter? High. Educ. 2011, 62, 279–301. [Google Scholar] [CrossRef]
- Novak, J.D. Meaningful learning: The essential factor for conceptual change in limited or inappropriate propositional hierarchies leading to empowerment of learners. Sci. Educ. 2002, 86, 548–571. [Google Scholar] [CrossRef]
- Machado, C.T.; Carvalho, A.A. Concept mapping: Benefits and challenges in higher education. J. Contin. High. Educ. 2020, 68, 38–53. [Google Scholar] [CrossRef]
- Eppler, M. A comparison between concept maps, mind maps, conceptual diagrams, and visual metaphors as complementary tools for knowledge construction and sharing. Inf. Vis. 2006, 5, 202–210. [Google Scholar] [CrossRef]
- Murtonen, M. University students’ understanding of the concepts empirical, theoretical, qualitative and quantitative research. Teach. High. Educ. 2015, 20, 684–698. [Google Scholar] [CrossRef]
- Novak, J.D.; Cañas, A.J. The Theory Underlying Concept Maps and How to Construct and Use Them, (Technical Report IHMC CmapTools 2006-01 Rev 01-2008). Florida Institute for Human and Machine Cognition. 2008. Available online: http://cmap.ihmc.us/publications/ (accessed on 2 September 2021).
- Vermunt, J.D. Inventory of Learning Styles in Higher Education: Scoring Key; Department of Educational Psychology, Tilburg University: Tilburg, The Netherlands, 1994. [Google Scholar]
- Volet, S.E. Significance of cultural and motivational variables on students’ appraisals of group work. In Student Motivation: The Culture and Context of Learning; Salili, F., Chiu, C.Y., Hong, Y.Y., Eds.; Plenum: New York, NY, USA, 2001; pp. 309–334. [Google Scholar]
- Stemler, S. An overview of content analysis. Pract. Assess. Res. Eval. 2001, 7, 17. [Google Scholar] [CrossRef]
- Lieneck, C.; Wang, T.; Gibbs, D.; Russian, C.; Ramamonjiarivelo, Z.; Ari, A. Interprofessional Education and Research in the Health Professions: A Systematic Review and Supplementary Topic Modeling. Educ. Sci. 2022, 12, 850. [Google Scholar] [CrossRef]
- Aase, I.; Hansen, B.; Aase, K.; Reeves, S. Interprofessional training for nursing and medical students in Norway: Exploring different professional perspectives. J. Interprof. Care 2016, 30, 109–115. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Entwistle, N. Student Learning and Academic Understanding: A Research Perspective with Implications for Teaching; Academic Press: London, UK, 2018. [Google Scholar]
- Khosa, D.; Volet, S.; Bolton, J.R. Making clinical case-based learning in veterinary medicine visible: Analysis of collaborative concept-mapping processes and reflections. J. Vet. Med. Educ. 2014, 41, 406–417. [Google Scholar] [CrossRef]
- Davies, M.; Barnett, R. The Palgrave Handbook of Critical Thinking in Higher Education; Palgrave Macmillan: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Volet, S.; Summers, M.; Thurman, J. High-level co-regulation in collaborative learning: How does it emerge and how is it sustained? Learn. Instr. 2009, 19, 128–143. [Google Scholar] [CrossRef]
- Kallio, H.; Kallio, M.; Virta, K.; Iiskala, T.; Hotulainen, R. Teachers’ support for learners’ metacognitive awareness. Scand. J. Educ. Res. 2021, 65, 802–818. [Google Scholar] [CrossRef]
- Raidal, S.L.; Volet, S.E. Preclinical students’ predispositions towards social forms of instruction and self-directed learning: A challenge for the development of autonomous and collaborative learners. High. Educ. 2009, 57, 577–596. [Google Scholar] [CrossRef]
- Kenaszchuk, C.; Rykhoff, M.; Collins, L.; McPhail, S.; van Soeren, M. Positive and null effects of interprofessional education on attitudes toward interprofessional learning and collaboration. Adv. Health Sci. Educ. 2012, 17, 651–669. [Google Scholar] [CrossRef]
- Clinton, V.; Kelly, A.E. Student attitudes toward group discussions. Act. Learn. High. Educ. 2020, 21, 154–164. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).