1. Introduction
In COVID-19 times, the healthcare system needs more financial and other resources for covering all necessary medical products and services. On the other hand, we have observed pressure on the effectiveness and optimisation of resources in hospitals and healthcare facilities. All resources should be optimized—employees, medical products, medical services, rooms, capacities. For such optimisation and decision-making, the managers need suitable data resources and well-structured data inputs. Therefore, digitalisation in hospitals can represent an important source of information for management.
Several studies have recently focused on the importance of digitalisation for modern management. Regarding general studies,
Hofmann (
2021) underlines that digitalisation enables new, previously unimagined, innovative business models. Companies can be faster and more flexible in developing new business ideas and new products, thanks to more direct and faster contacts and a larger amount of data. This development also leads to increasing customer demands and ever shorter reaction times.
Another study (
Hoerlsberger 2019) focuses on the impact of digitisation in the industries. Based on the results, existing business models are disrupted through new technology. Thus, the author indicates that businesses today have to open up their minds to innovation and continuous learning. In the modern world, there is a definite shift towards individualised products and services as well as a unique customer experience.
Based on
Gigauri (
2020), management strategies need resilience, flexibility, and adaptability in digitalisation time. In the quality management (QM) area, many future digitalised solutions for improving internal work will require collaboration between functions. In this respect, the explorative-internal role of digitalisation for QM practitioners includes planning, designing, and reviewing with internal stakeholders to provide solutions that create better opportunities for the provider to offer value for the customer (
Rojas et al. 2021).
Ageron et al. (
2020) focused in more detail on the issues related to the digitalisation of SME supply chains and indicated that public supply chains, such as public hospitals supply chains, are under-studied.
Regarding the impacts of digitalisation on healthcare services,
Iadanza and Luschi (
2020) support innovative approaches in healthcare institutions. Innovation, together with digitalisation and development in health technology, contribute significantly to the quality of health care provided by various health facilities (
Austin et al. 2018). Moreover, it represents new challenges for both management and staff of health care services. Health care professionals need to understand the forces that add value to the cost-effectiveness and efficiency of health care delivery systems. Based on the study performed by
Blythe et al. (
2019), technology and health care equipment play a significant role in health care services. It is necessary to understand the role of technology management to communicate effectively about it to health planners (
Cucciniello et al. 2016). The COVID-19 situation in particular represents a big challenge for health care management and innovative approaches.
The aspects of patient safety and integration of digitalisation into the professional context necessitate an assessment of healthcare professionals’ competencies in digitalisation (
Basu 2020). The key competencies from a healthcare perspective include encompassing knowledge of digital technology and the digital skills required to provide good patient care, including associated social and communication skills, and ethical considerations of digitalisation in patient care (
Konttila et al. 2019).
Moreover, financial benefits are linked to the use of electronic documents (
Geier and Smith 2019). A good drug inventory planning system is important for efficient budgeting, procurement, and cost control of drugs. When quantities of stagnant drugs in the inventory are too much, wastage due to expired and spoiled drugs could occur. This not only causes loss of income but could also jeopardize healthcare service delivery (
Dewi et al. 2020).
Pouloudi and Whitley (
1997) focused on drug use management information systems help to manage information on patients. Moreover, these systems can be used on drugs and their costs to monitor and evaluate the effectiveness of drug use policies (
Pouloudi and Whitley 1997).
Chan et al. (
2020) proposed to optimize medical expenditure by focusing on the common diagnosis segment, as this segment of individuals is one of the largest groups that drive medical claims. This analysis helps to better understand the employees’ medical claims and to have an overview of the current employee health population.
Choi et al. (
2013) analysed the economic effects of an electronic medical record system in hospitals that used a cost-benefit analysis based on the differential costs of managerial accounting. The benefits included cost reductions after system adoption and additional revenues both from the remodelling of paper chart storage areas and medical transcriptionists’ contributions.
The digitalisation of hospitals can improve financial management (
Dasgupta and Narendran 2021). Moreover, it can identify how many beds are occupied and what is the expected revenue (
Kawale et al. 2020). Adopting electronic documents can save organizations money by decreasing costs associated with paper records (e.g., storage, purchasing paper, printing) and by reducing duplicate testing and other redundant interventions (
Geier and Smith 2019).
Besides the economic impact of COVID-19, both public and private expenditures connected with healthcare systems are increasing for a number of reasons.
Carbonaro et al. (
2018) examined the links between various variables influencing economic impacts, such as population ageing, demographic development, local economic development prospects, and financial implications. Population ageing and demographic development tend to increase the demand for health services.
Burian et al. (
2018) compared the consumption expenditures of households of employees with households of pensioners and identified a group of significantly higher consumption expenditures of households of pensioners. Within this group, the most significant are the health expenditures of pensioners, including expenditures on medical products, medical services, dental services, paramedical services, and hospital services.
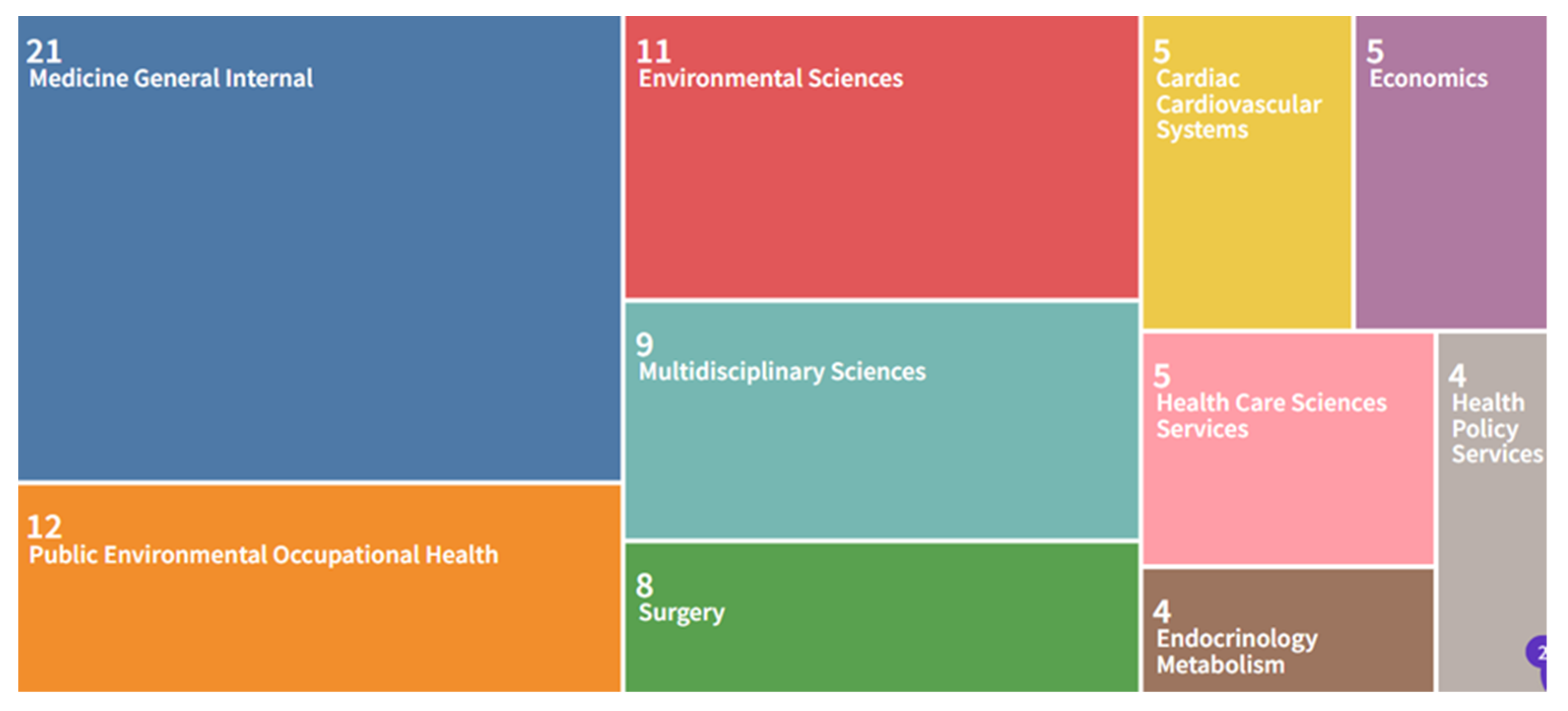
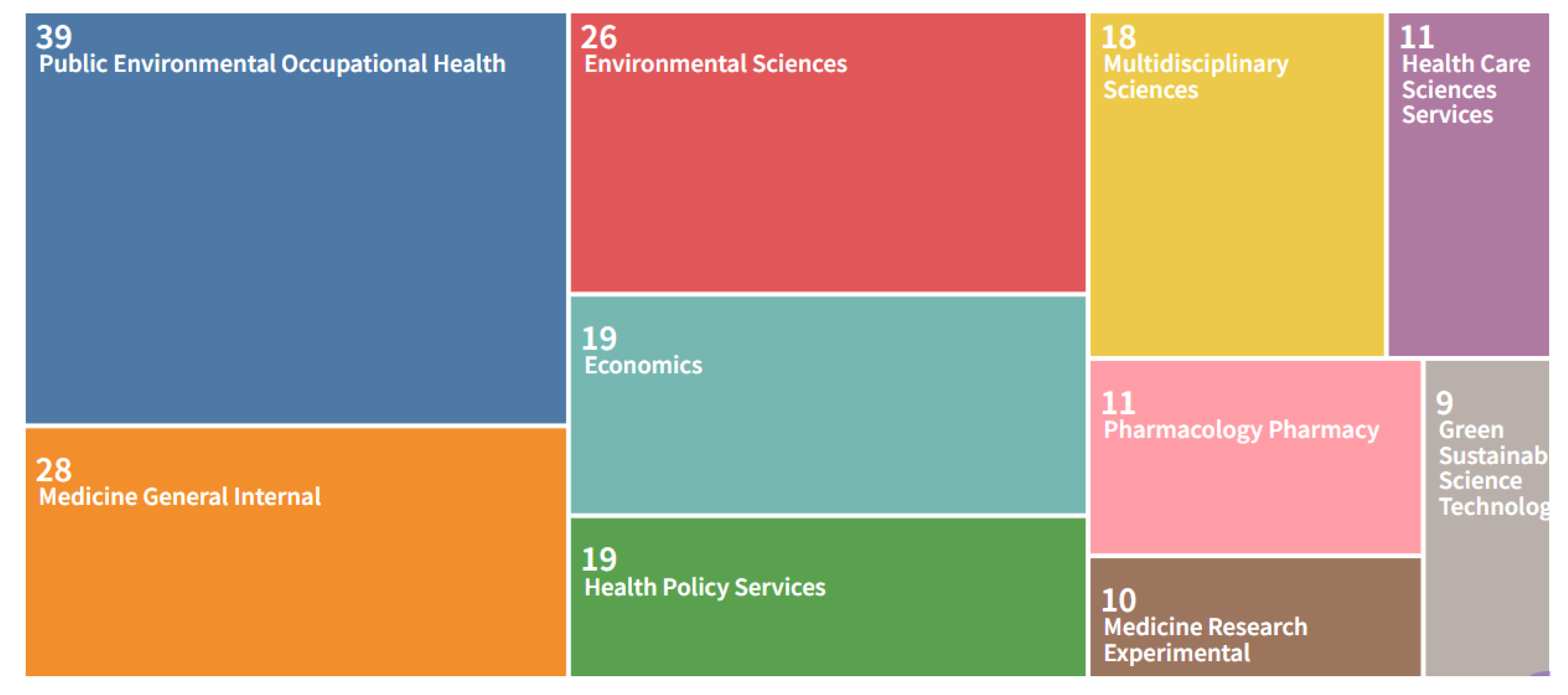
Searching for scientific studies focused simultaneously on COVID-19, healthcare institutions, and economic impact, we found 312 studies in total, published in the period 2020–2021 in scientific journals indexed on the Web of Science database (
WoS 2021). Using the WoS tool Treemap (
Wilkinson 2021) shows 10 results for scientific disciplines most connected with the keywords COVID-19, healthcare, and economy (
Figure 1).
There are fewer studies focusing in more detail on the impact of COVID-19 on hospitals and their economic situation specifically. Using the keywords COVID-19, hospital, and economy, we found 124 relevant scientific studies (
Figure 2). Regarding economic scientific studies, most of them are case studies, such as case studies from the United Kingdom (
Mitha 2020), United States (
Chen et al. 2020), Italy (
Barbieri and Bonini 2021), France (
Sainsaulieu 2021), and a complex study that presented an economic analysis for 94 countries (
Vera-Valdés 2021).
Looking for synergies between these scientific studies, there is one common link—hospital bed/beds. Such equipment is an important indicator for management and planning in hospitals. Moreover, it is a suitable indicator for the analysis of efficiency and economic approach. For example, healthcare and hospital beds are analysed in the study performed by
Barbieri and Bonini (
2021), while hospital beds and staff (permanent staff, administration staff, management) are focused on by
Sainsaulieu (
2021) and hospital beds per 1000 inhabitants are a statistically significant factor in reducing the number of deaths (
Vera-Valdés 2021). Hospital bed capacity is discussed in
Chen et al. (
2020). The authors considered a case where HRRs share hospital beds among the neighbouring HRRs during a surge in demand beyond the available beds and the impact it has in controlling additional deaths.
Based on these studies, “use of hospital beds” was selected as an important indicator for the correlation and regression analysis also in our study.
The paper is divided as follows: key scientific studies are described in
Section 1 “Introduction”,
Section 2 will focus on “Methodology”, the key findings will be presented in
Section 3, and
Section 4 of the results within the broader context of answering the research questions will follow. Finally,
Section 5 underline the key findings and formulate the recommendations.
3. Results
3.1. Temporal Changes in Equipment/Facilities Use
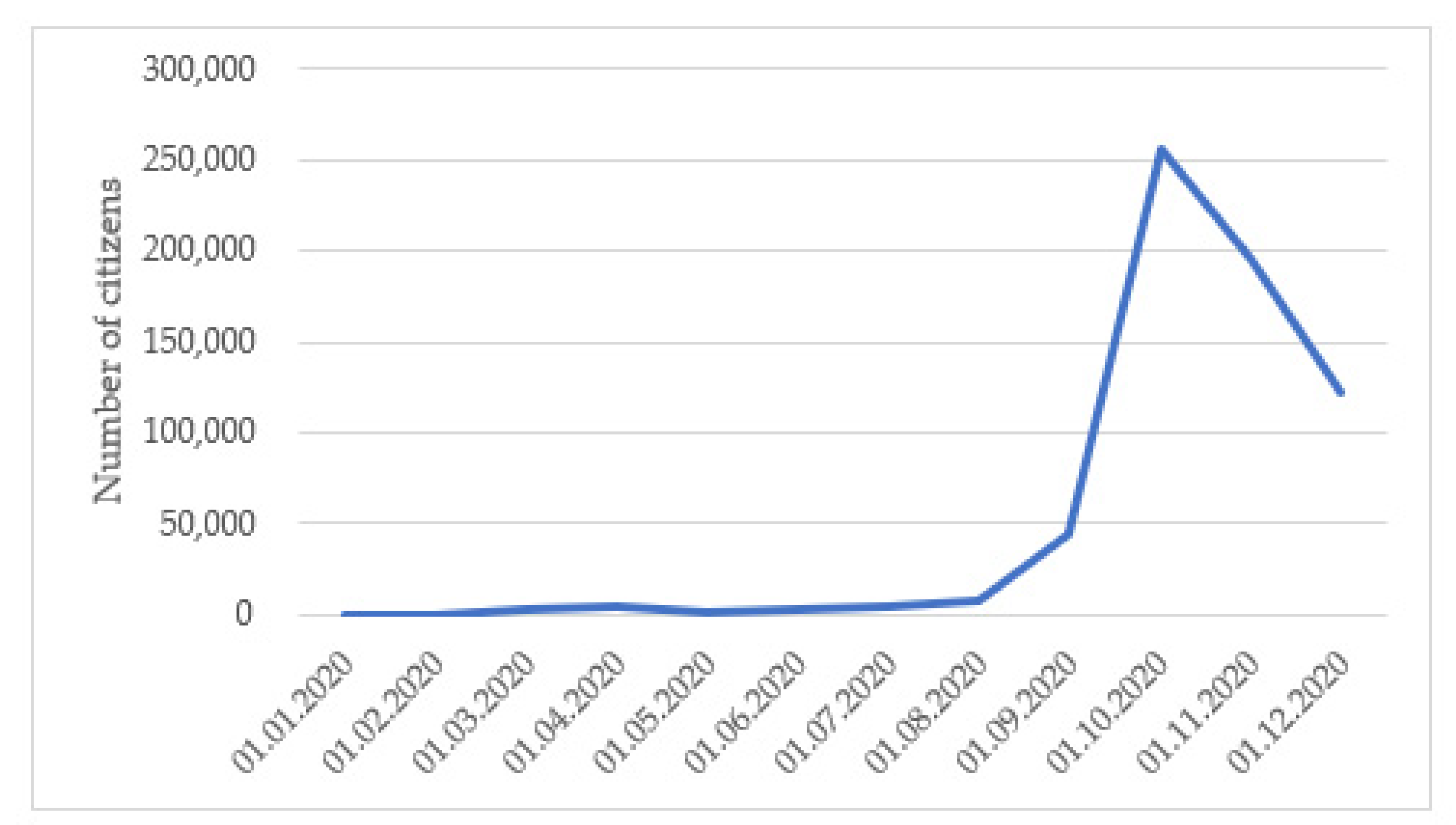
The first area of focus was on the development of COVID-19 positive citizens in the Czech Republic in 2020 (
Figure 3).
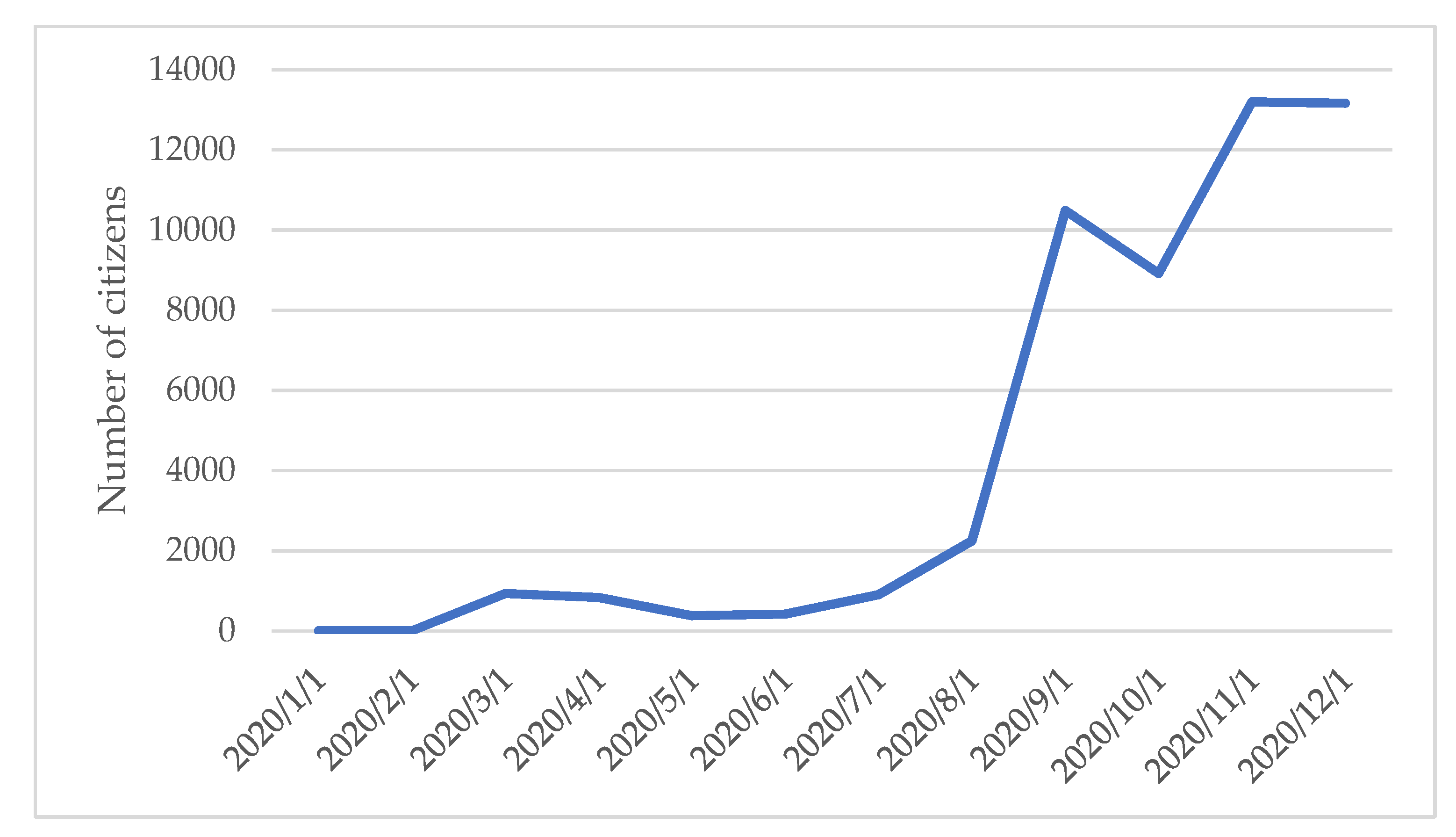
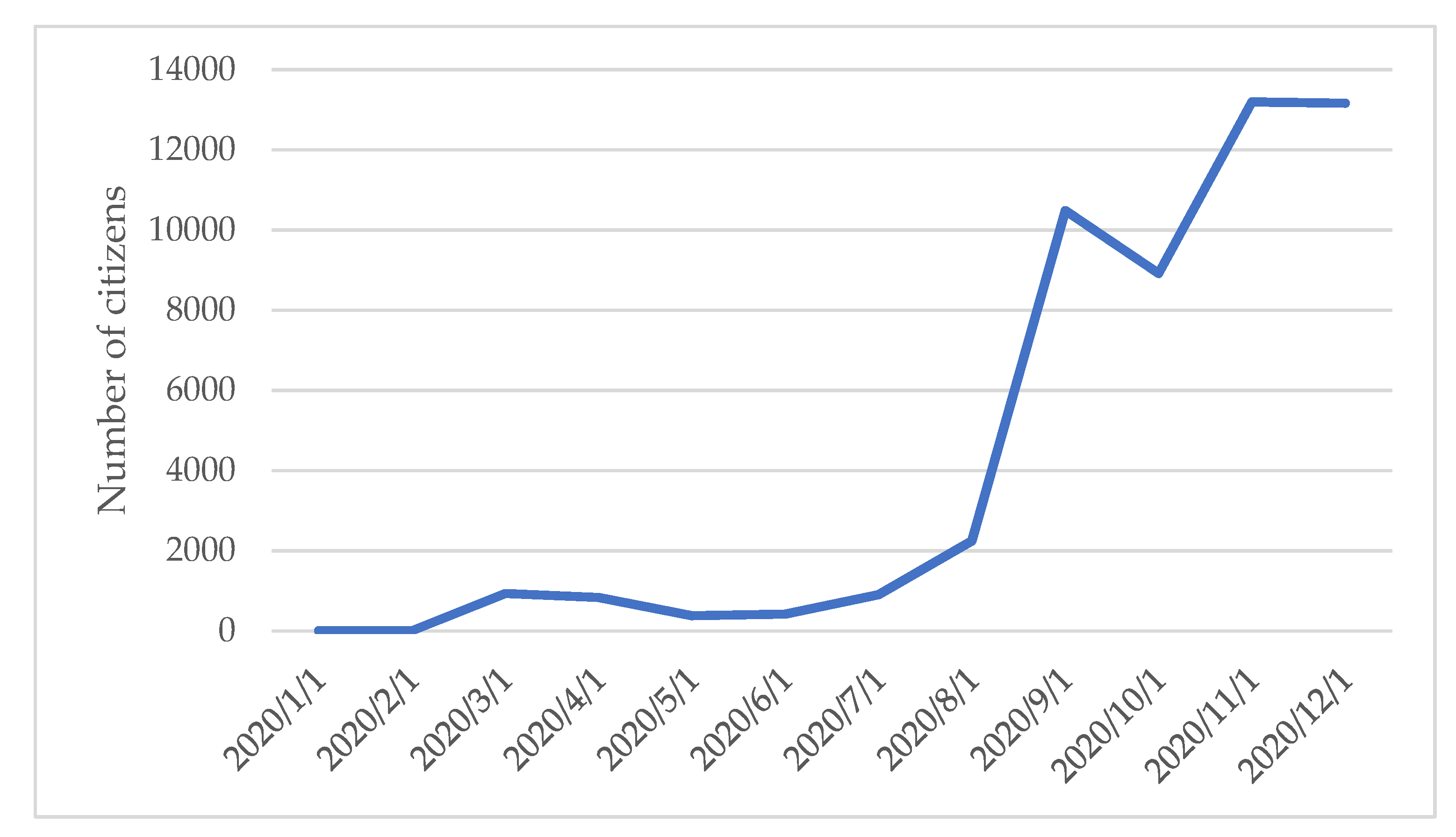
Regarding the situation in Prague in 2020, the development of COVID-19 positive citizens was slightly different from the whole Czech Republic, as is visible in
Figure 4,
Figure 5 and
Figure 6.
The increase in the number of COVID-19 positive people started earlier in Prague in 2020 than in the whole Czech Republic. Moreover, we can say that the development of time series and their peaks differ from the whole Czech Republic.
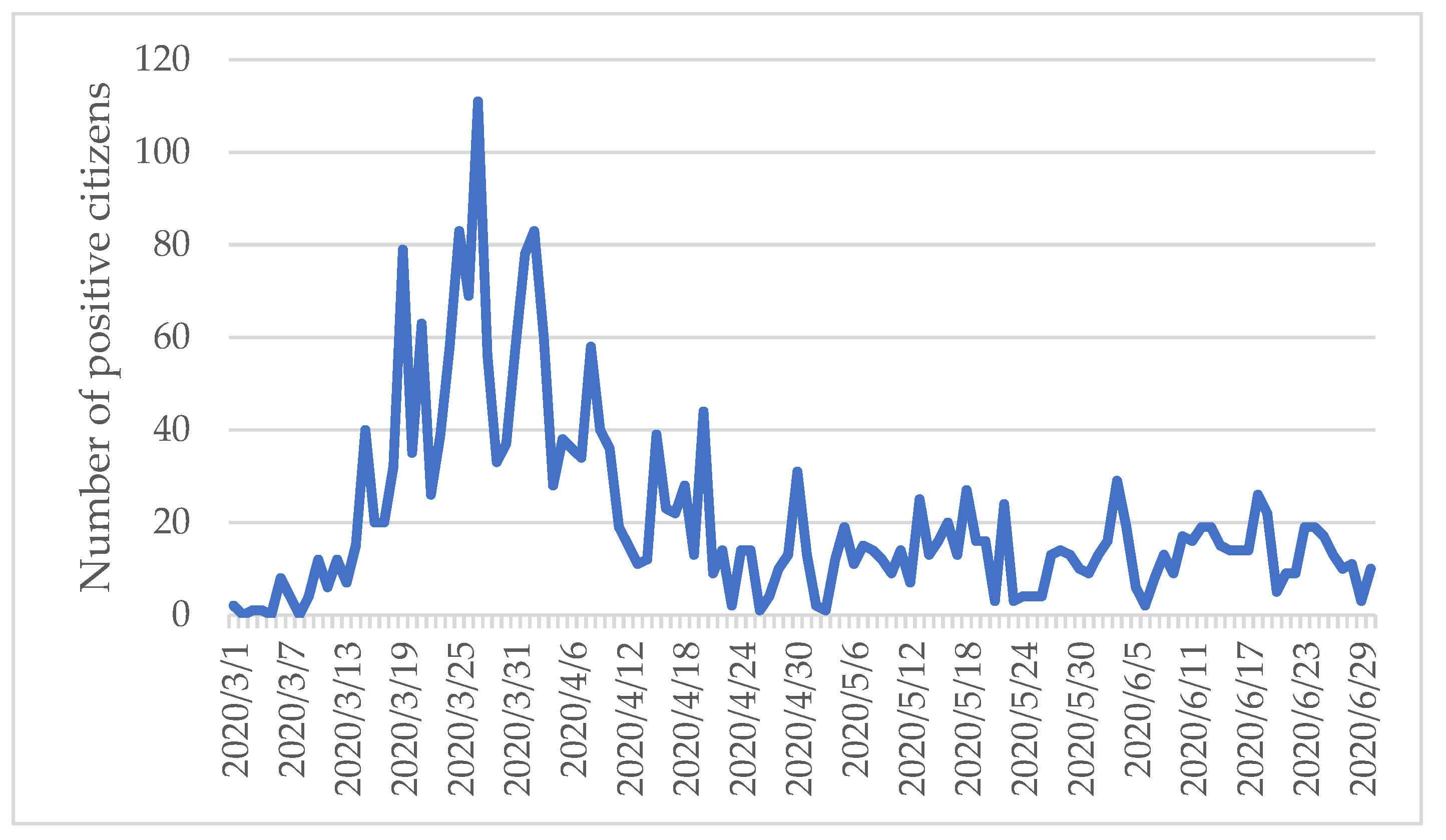
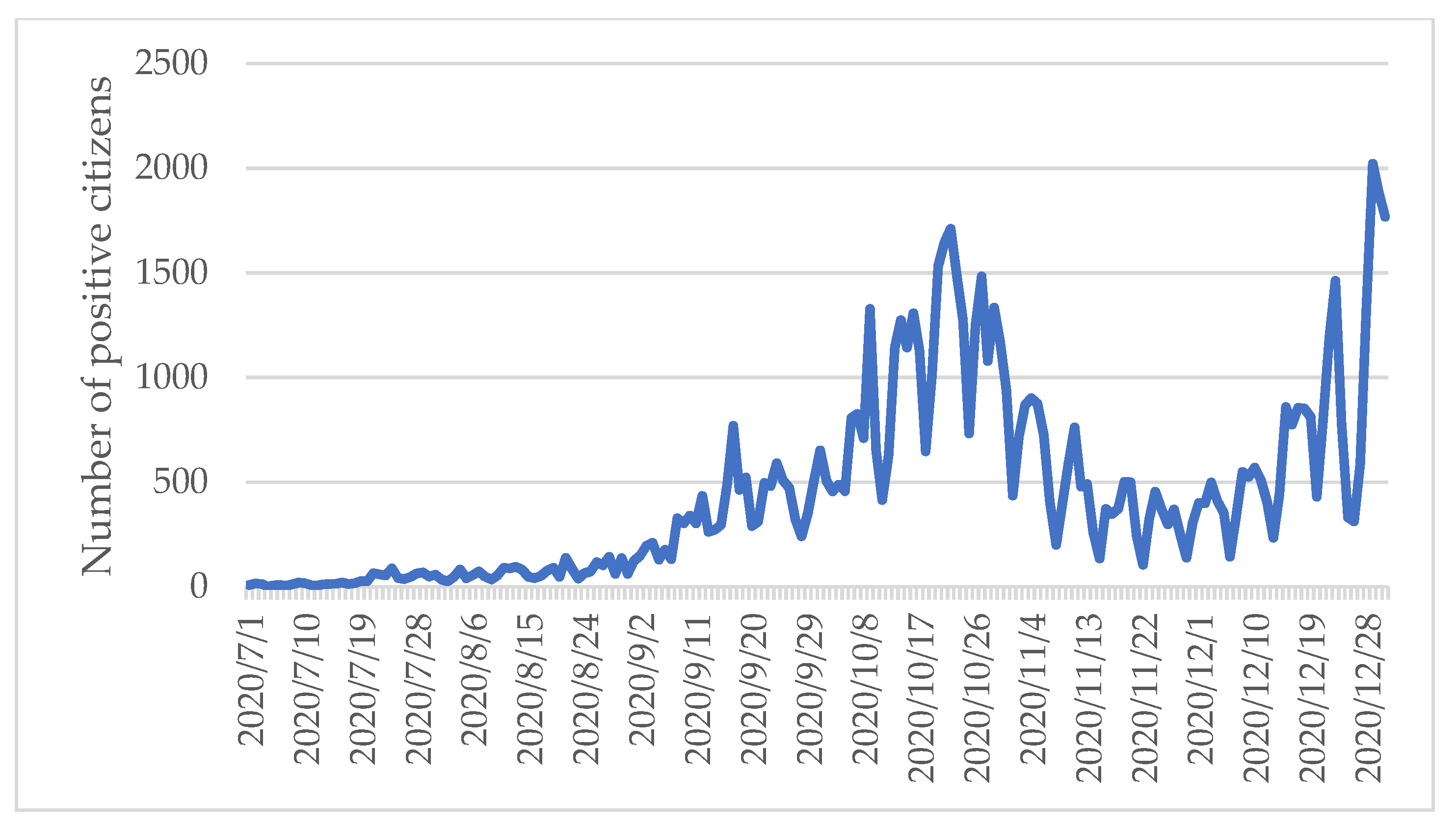
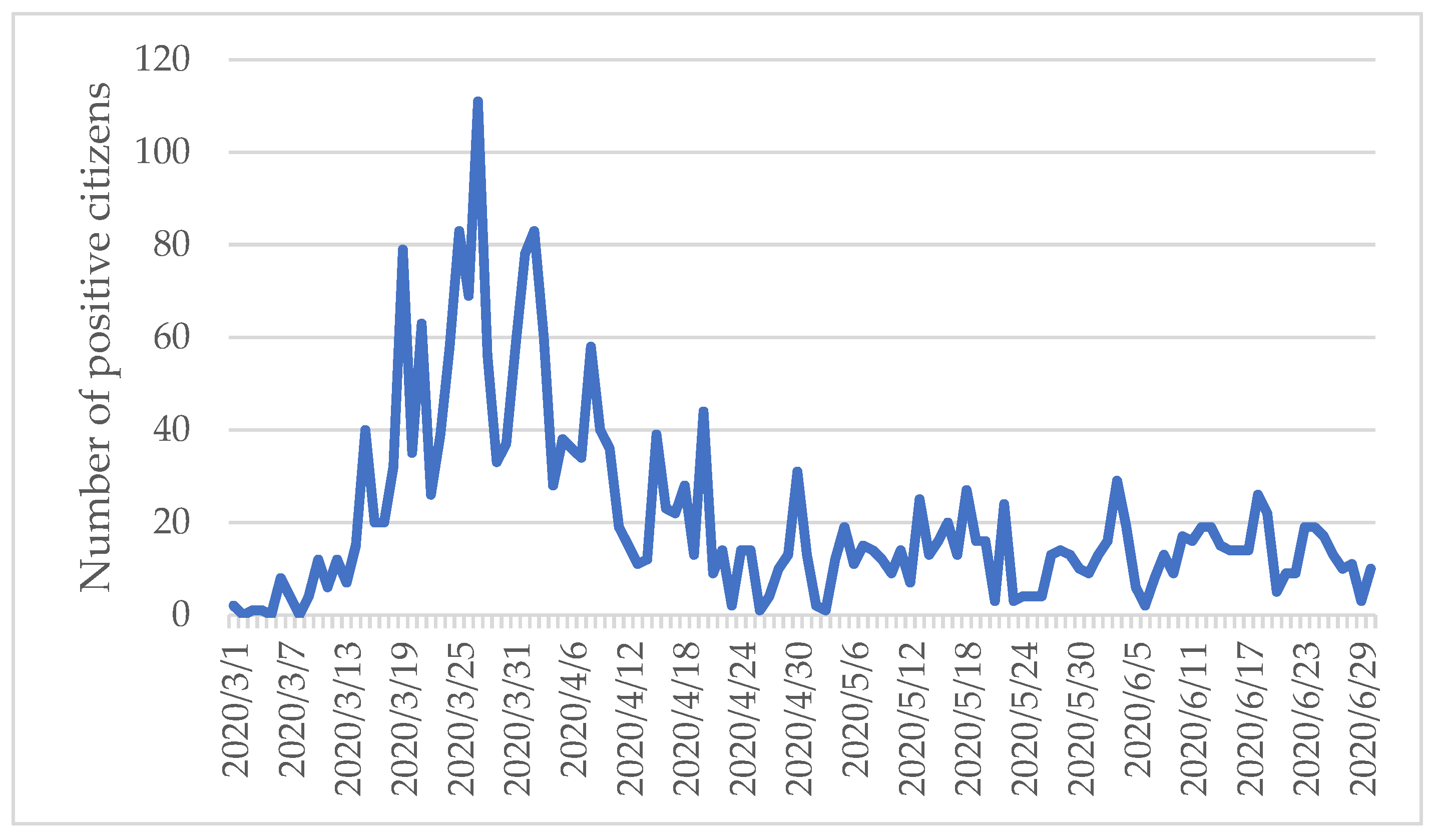
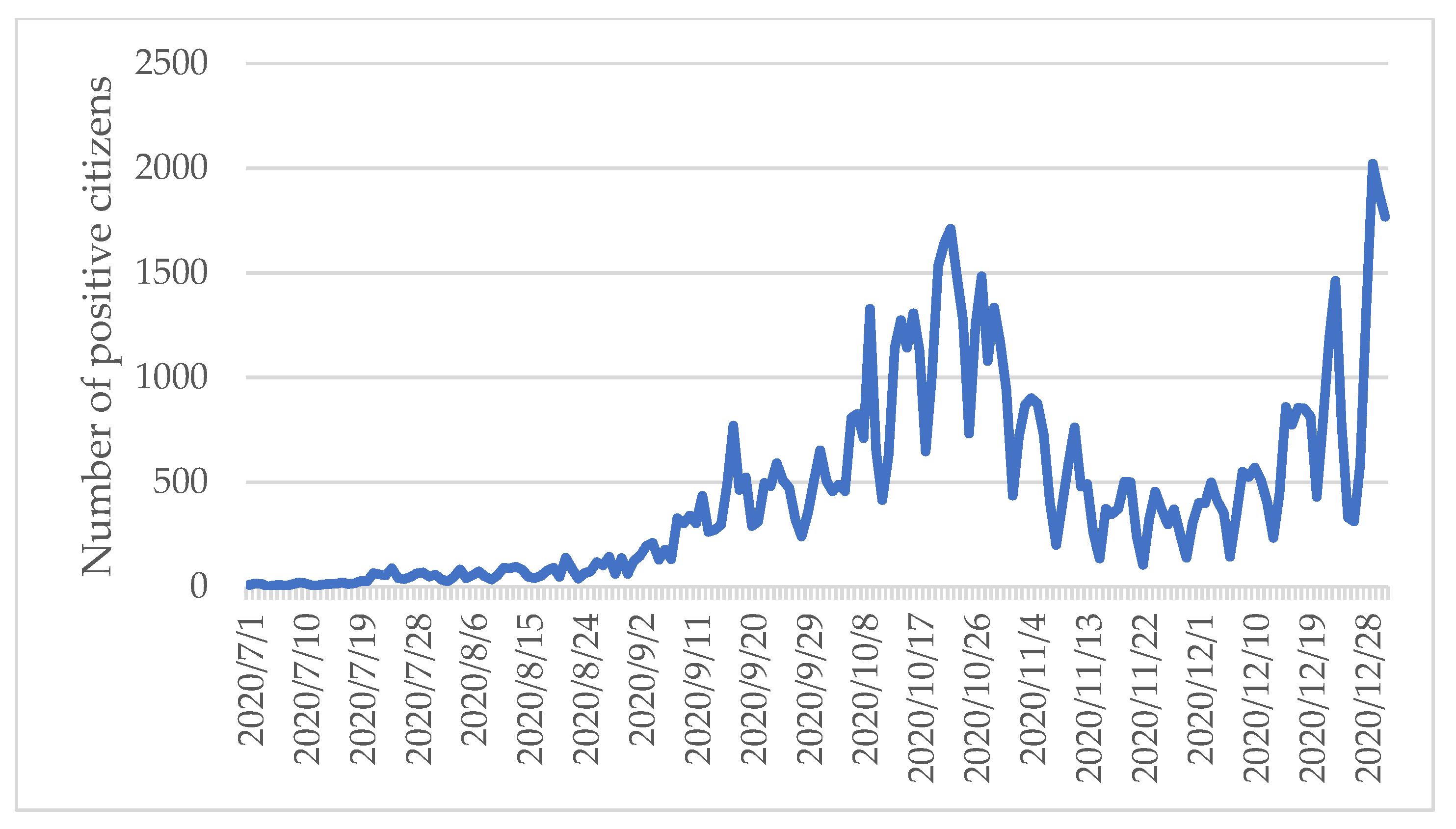
Therefore, for the case study of the selected hospital in Prague, the time series of COVID-19 positive citizens in Prague should be more significant and valuable. Concerning daily data connected with the situation in Prague in 2020,
Figure 5 shows the period March–June 2020, and
Figure 6 shows the development over the period July–December 2020.
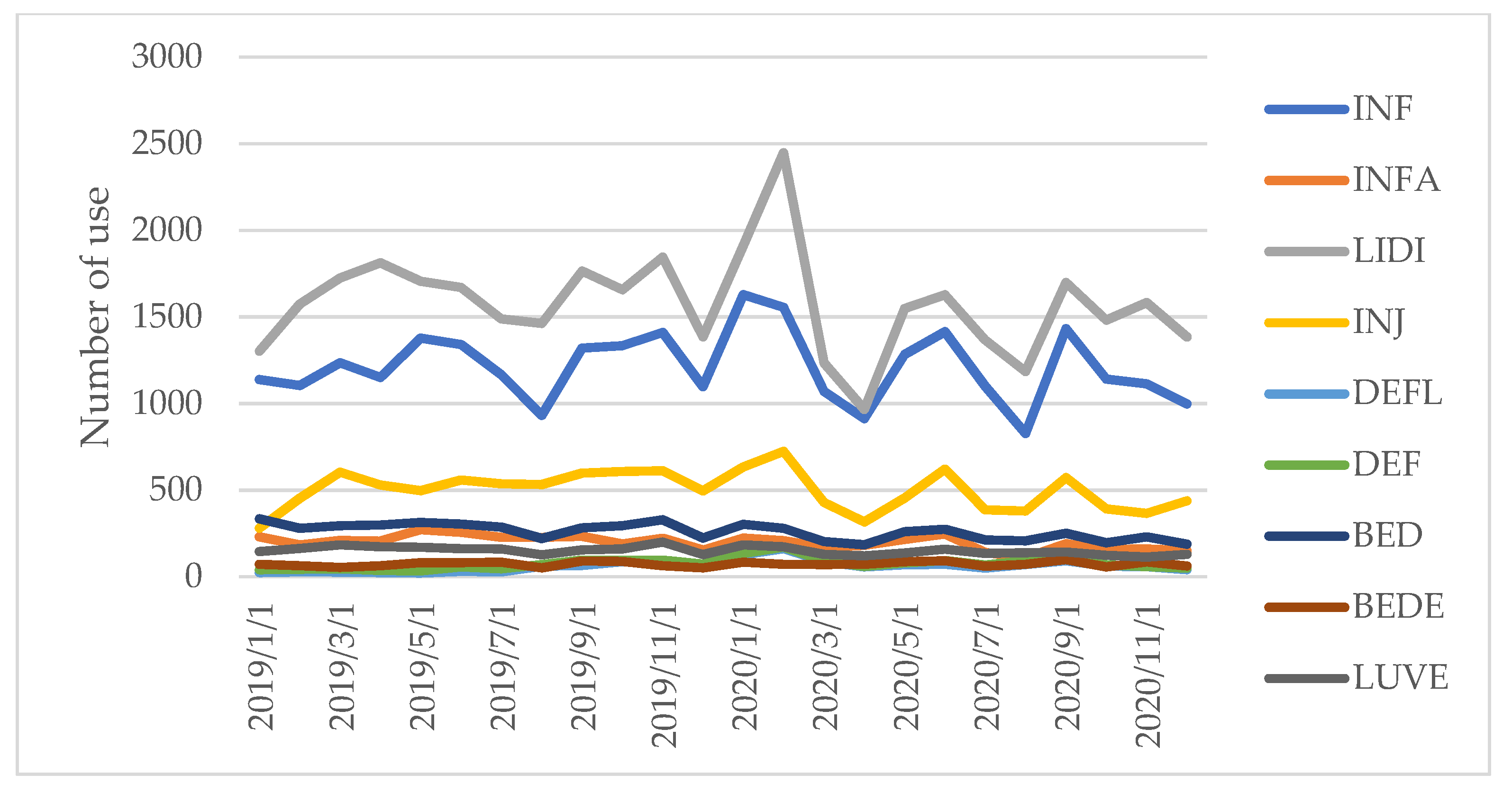
The next focus was on the aspects of the digitalisation of medical devices in the selected hospital in Prague. As was mentioned before, the new software EFAS was implemented in 2018 (the pilot year). The statistically valuable data are available for years 2019 and 2020.
Figure 7 shows the development of selected equipment/facilities use in the years 2019–2020.
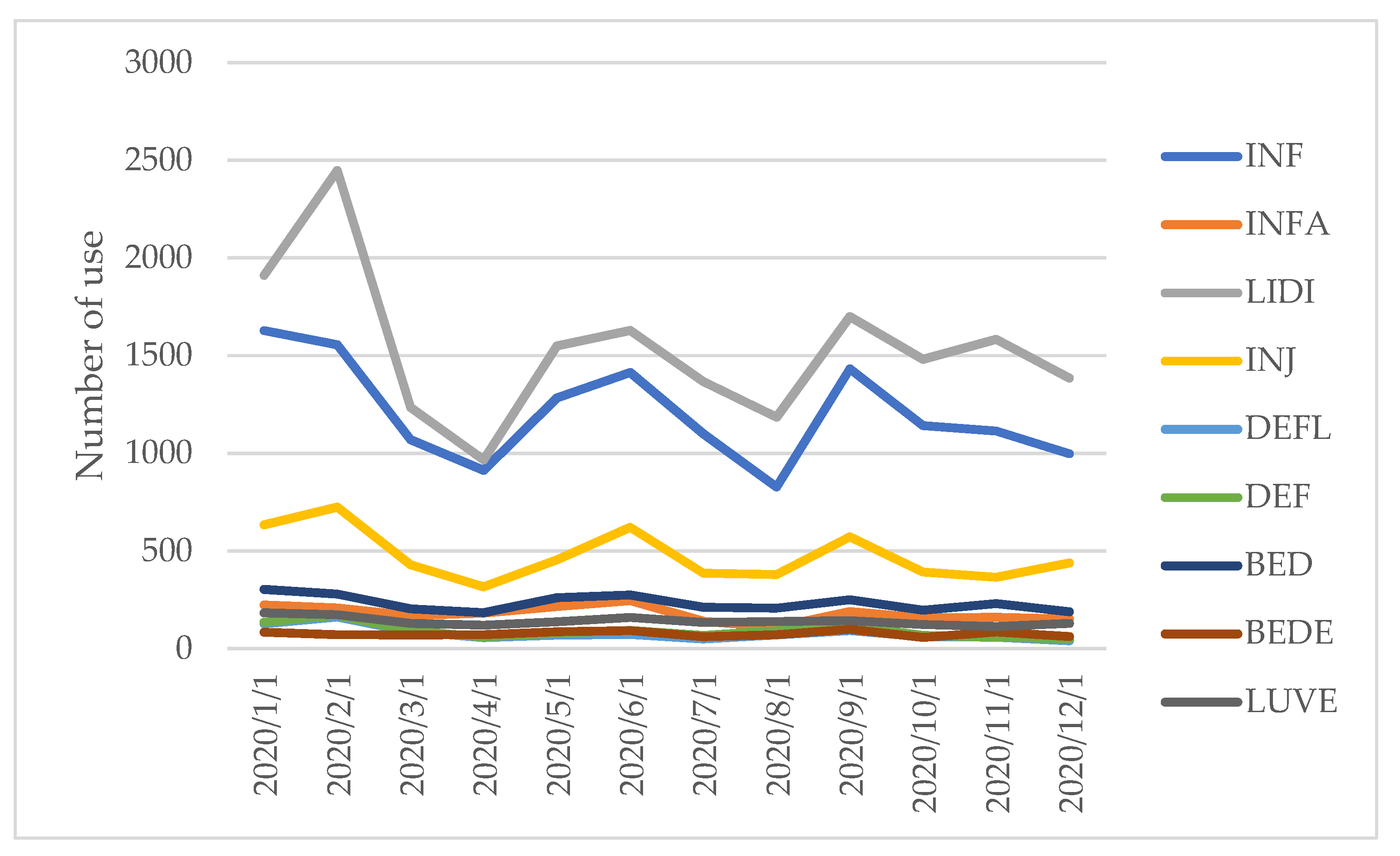
For COVID-19 period evaluation,
Figure 6 shows equipment/facilities use in 2020 in more detail.
Observing
Figure 4,
Figure 5,
Figure 6 and
Figure 8, an increase in COVID-19 positive people seems to relate to a decrease in the equipment/facilities use in the hospital. It shows a change in the distribution of resources, a decrease in the use of some equipment/facilities, and the equipment/facilities move between the departments, hospitals, and/or healthcare organizations. It can also show a change in equipment/facilities use and selected equipment move to COVID-19 departments. We will use more sophisticated tools for analysing the equipment/facilities use in the hospital in Prague, such as correlation, and regression analysis, gradually.
3.2. Correlation and Regression Analysis
For the correlation analysis, variables connected with selected equipment/facilities use in the hospital in Prague and COVID-19 positive people in Prague were used.
Table 4 shows the results of the correlation analysis.
With exception of elegance bed (BEDE), we can observe a negative correlation between COVID-19 positive people in Prague and equipment/facilities use in the hospital in Prague. Regarding statistical significance, there is a statistically significant correlation coefficient between COVID-19 positive people in Prague (COVP) and infusion pump ARGUS (INFA, −0.46), bed (BED, −0.49), and lung ventilator (LUVE, −0.51).
In the next step, we focused on regression analysis using variables INFA, BED, and LUVE as dependent variables and COVID-19 positive people in Prague as an independent variable. To be sure not to omit any important results, we created more regression models for all variables presented in
Table 3, working with both single and multiply regression models. However, only the variables INFA, BED, and LUVE showed statistically significant results in single regression models. Such results are presented in
Table 5 and
Table 6.
Based on all regression models and equations, we can say that an increase in the number of COVID-19 positive people influenced a change/decrease in equipment/facilities use, such as infusion pump ARGUS, bed, and lung ventilator.
3.3. Cost-Benefit Analysis of Digitalisation of Medical Devices in Hospitals
It is not easy to identify, moreover to calculate, possible benefits and costs of digitalisation of medical devices in hospitals. In the previous chapter, the results of correlation and regression analysis show us that COVID-19 influenced the distribution of processes and equipment/facilities use in the hospital in Prague. It is connected both with the economic and financial aspects of management. However, COVID-19 is only one example of possible changes in hospital processes and facility management. It is necessary for all managers to have updated information for their decision-making.
It should be underlined that cost-benefit analysis of digitalisation of medical devices in hospitals is connected with various periods. We should distinguish between short-time and long-time costs and benefits.
Regarding the phase of implementation of digitalisation and new software in hospitals, it is clear that there are costs connected with system infrastructure, systems applications, office administration, scanning of paper documents, technical support, and training of management and employees. The overview of such costs is described in
Table 7.
Most of these costs occur in a short time period. On the other hand, a long time period is connected more with possible benefits. These benefits are represented by various kinds of costs reductions and also with additional income. The overview of possible cost reduction is described in
Table 8.
Generally, reduction in costs is connected with various processes and materials in the hospital, such as paper documentation, storage space, management, time management, employees, materials, orders to the departments, and services.
Besides cost reductions, digitalisation also helps to improve the income side of hospitals. The overview of possible additional income is described in
Table 9.
Free storage space (both regular and occasional) can be modified and adapted to other rooms. Moreover, hospitals can rent these rooms. Based on our case study, the hospital rented additional free rooms to providers of services connected with healthcare, such as massage salons, beauty salons, and/or nutritional counselling.
Focusing on the impact of digitalisation of medical devices in hospitals in time, based on our research, we can say that the costs occur mostly in a short time period and the benefits in a long time period.
4. Discussion
Digitalisation is one of the key tools of modern management. All its aspects now face the challenges of the post-COVID-19 period, and the process of digitalisation is very important in this development. Customization, flexibility, acceleration of all processes, and pressure to constantly streamline HR management are some of the features of modern management (
Sternad Zabukovšek et al. 2021). Digitalisation permeates all spheres of business and should be an integral part of the component (active tool) of healthcare management. Generally, digital transformation relates to various fields of economic entities, including hospitals and health care facilities.
Regarding the first research question (RQ1)—“Is the impact of the COVID-19 pandemic on the distribution of resources and facility management in hospitals significant?”, based on our research the answer is “rather yes”. Concerning the literature review and case study data, COVID-19 caused a great acceleration in the use of technology, digitalisation of processes, and new forms of working. Moreover, COVID-19 represents a huge impetus for innovation in many sectors, including healthcare. As
Fabiano (
2020) highlighted: “Like a rocket blasting off for the moon, the global pandemic accelerated 20 years of pent-up innovation for the healthcare industry into 8 months.” We agree with
Ageron et al. (
2020) and
Tortorella et al. (
2021) that this period is characterised by a complex and dynamic environment in hospitals, where digitalisation affects several aspects of life, such as internal logistics distribution and facility management.
A new system of distribution and connected facility management relates to financial issues. On the one side, the healthcare system needs more financial and other resources for covering all necessary medical products and services. On the other side, there is pressure on the effectiveness and optimisation of resources in hospitals and healthcare facilities. All resources are optimized—employees, medical products, medical services, rooms, and capacities. Economic optimisation represents the challenge for digitalisation and the new management approach.
Dealing with the second research question (RQ2)—“Is the digitalisation of medical devices beneficial for the selected hospital in Prague?”, based on our research the answer is not so clear. Focusing on the impact of digitalisation of medical devices in hospitals in time, based on our research, we can say that the costs occur mostly in a short time period and the benefits over a long-time period. However, it is not easy to identify all possible savings, as some of them only have a non-financial expression. Therefore, the answer is “rather yes”, but only over a long-time period.
Our results correspond with the study performed by
Choi et al. (
2013). The authors analysed the economic effects of an electronic medical record system in hospitals that used cost-benefit analysis based on the differential costs of managerial accounting. The benefits included both cost reductions and additional revenues.
As
Dasgupta and Narendran (
2021) underline, modern hospitals should be technologically sophisticated healthcare facilities with technologically specialised personnel. On the other hand, healthcare is a multidisciplinary sector and various professionals from different fields should cooperate. New solutions and ideas can emerge in interdisciplinary teams, using disruptive and out-of-box thinking.
Regarding this point, we agree with
Ageron et al. (
2020) that researchers should focus in more detail on the issues related to the digitalisation of public supply chains, such as public hospitals supply chains, which are under-studied. Innovations and developments in health technology can contribute significantly to the quality of health care provided by various health facilities, but have also brought new challenges in the management of health care services. Health service planners, hospital administrators, physicians, and other health care professionals need to understand the forces that add value to the cost-effectiveness and efficiency of health care delivery systems.
Concerning further research, firstly, 2021 should be examined. This “second COVID-19 year” has specific characteristics, such as vaccination, new tools in hospitals, and a new managerial approach. Simultaneously, the economic impacts of COVID-19 are increasing. Secondly, qualitative research can help to add the personal view of employees and managers. The presented analysis is based on a dataset extracted from system EFAS. Expert interviews with managers can represent valuable input to the overall picture of the hospital.
5. Conclusions
Generally, COVID-19 has been a huge accelerator for R&D, innovation, optimization, and new ideas. Technology and health care equipment/facilities play a significant role in health care services. Therefore, effective facility management can contribute to the improvement of healthcare.
The main aim of our research was the identification of the benefits of digitalisation of medical devices in hospitals in COVID-19 times, focusing on a case study in the Czech Republic. Our methodological approach included a literature review, data analysis, correlation analysis, and regression analysis. The case study presented the changes of the equipment/facilities use in 2019 and 2020 in a selected hospital in Prague and the impact of COVID-19 on the use of these resources. Management and financial issues were discussed. Based on the results, COVID-19 influenced both the distribution of resources and facility management in hospitals. Economic benefits are represented mainly by various kinds of savings and optimization of both processes and employees.
It is clear that digitalisation represents an important source of information for management in hospitals. Based on the presented research, we can recommend digitalisation as a suitable tool for managers and headquarters in hospitals. They can easily observe all processes and persons and optimize the healthcare services provided.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}