Abstract
The pressure pain threshold (PPT) is a useful tool for evaluating mechanical sensitivity in individuals suffering from various musculoskeletal disorders. The aim of this study is to investigate PPT at the heel area in order to assist in the design of orthotic shoes for sufferers of heel pain due to a calcaneal spur. The size and location of the calcaneal spur was determined by x-ray images, with PPT data measured around the spur at five points by using algometer FDIX 25. The pain test experiment was conducted by pressing each point to obtain the pain minimum compressive pressure (PMCP) and its location. The information of shoe size, spur location and dimensions, and the PMCP location for each individual is used to obtain the exact point location for applying a softer material to the shoe in-sole, in order to reduce heel pain. The results are significant as it can be used by designers to design appropriate shoe in-soles for individuals suffering from heel pain.
1. Introduction
A calcaneal/heel spur is a small bone that grows on the inferior side of the heel bone and can be seen with an x-ray examination [1]. Calcaneal spurs, as a cause of plantar fasciitis (PF), are currently debatable [2], however, it has a strong correlation with PF [3,4]. The disease can cause pain in the heel and tenderness beneath which is typically severe in the morning and improves only after a routine daily weight bearing activity [5]. Obese people who have to stand or walk for a long time, and people with diabetes are most vulnerable to this disease [6]. The most common treatments for individuals with heel spur syndrome are the intake of a nonsteroidal anti-inflammatory drugs or corticosteroid injections, however, these treatments should not be administered continuously for a long duration time due to their side effects on the kidney, and liver, and they may also lead to high blood pressure, and stroke [7]. Another treatment that has relatively little effect to the human body is to reduce pressure on the heel through the use of orthotic shoes [8,9].
The sole of the human foot, particularly, at the heel area, carries a weight of about 69% of the body weight (BW) when standing [10], whilst when walking or running, the heel strike phase ranges from 2.0–5.4 BW [11]. This large amount of load on the heel may cause heel pain and plantar fasciitis, especially if there is a spur present on the heel bone. Orthotic shoes are designed to reduce pressure in the heel area, and its design requires knowledge of the location and dimensions of the spur, as well as the pressure threshold that can cause pain. Previous studies have reported that plantar heel pain caused by heel spurs generally increases in intensity with the age and weight of the person. In some research, spurs have been classified into three categories: small (1–2 mm), medium (3–5 mm) and large (≥6 mm), to determine the relationship between the spur’s dimension and pain intensity. However, the level of pain experienced by each individual has been estimated by a telephone survey, and hence, definitely subjective and qualitative [12]. To obtain a quantitative level of pain, an algometer may be used, which needs to be applied to the tissues via a small rubber tip. The measurement may be taken by pressing each region using the algometer probe (Algomed, Medoc Ltd., Ramat Yishai, Israel), with the minimum pressure that is causing pain (in kg/cm2), or the pressure pain threshold (PPT) being recorded.
The use of an algometer has been widely used by researchers to study trochanteric pain [13], musculoskeletal pain [14], neck pain [15], myofascial pain [16], low back pain [17], and knee osteoarthritis [18]. An algometer has been used to determine PPT value on the heel of individuals experiencing plantar heel pain syndrome [19]. To measure PPT, the heel regions has been divided into five regions: (1) the medial posterior, (2) the medial anterior, (3) the lateral posterior, (4) the lateral anterior, and (5) central site.
In this paper, a study has been performed to investigate PPT measurements at the heel area to assist in the design of proper orthotic shoes in order to reduce pain pressure for individuals with calcaneal spur. These orthotic shoes cannot be mass produced [8] as the location and dimensions of the spur, and the shoe sizes of each individual may be different. Hence, each orthotic shoe must be specially tailored to each individual. The pain minimum compressive pressure (PMCP), and its location on a particular individual, are used as a basis for determining the material hardness of the shoe in-sole at the smallest PPT location as measured using an algometer [20,21]. Previous research has shown that reducing pressure in the heel area can be achieved by raising the heel height of the shoe, whereby shoes with heel height of 2 cm and 3 cm for men and women, respectively, have been shown to be sufficient to decrease calcaneal pain [21]. Combining the shoe insole material with the appropriate hardness and increasing the heel height of the shoe greatly reduces the pressure in the heel area.
2. Materials and Methods
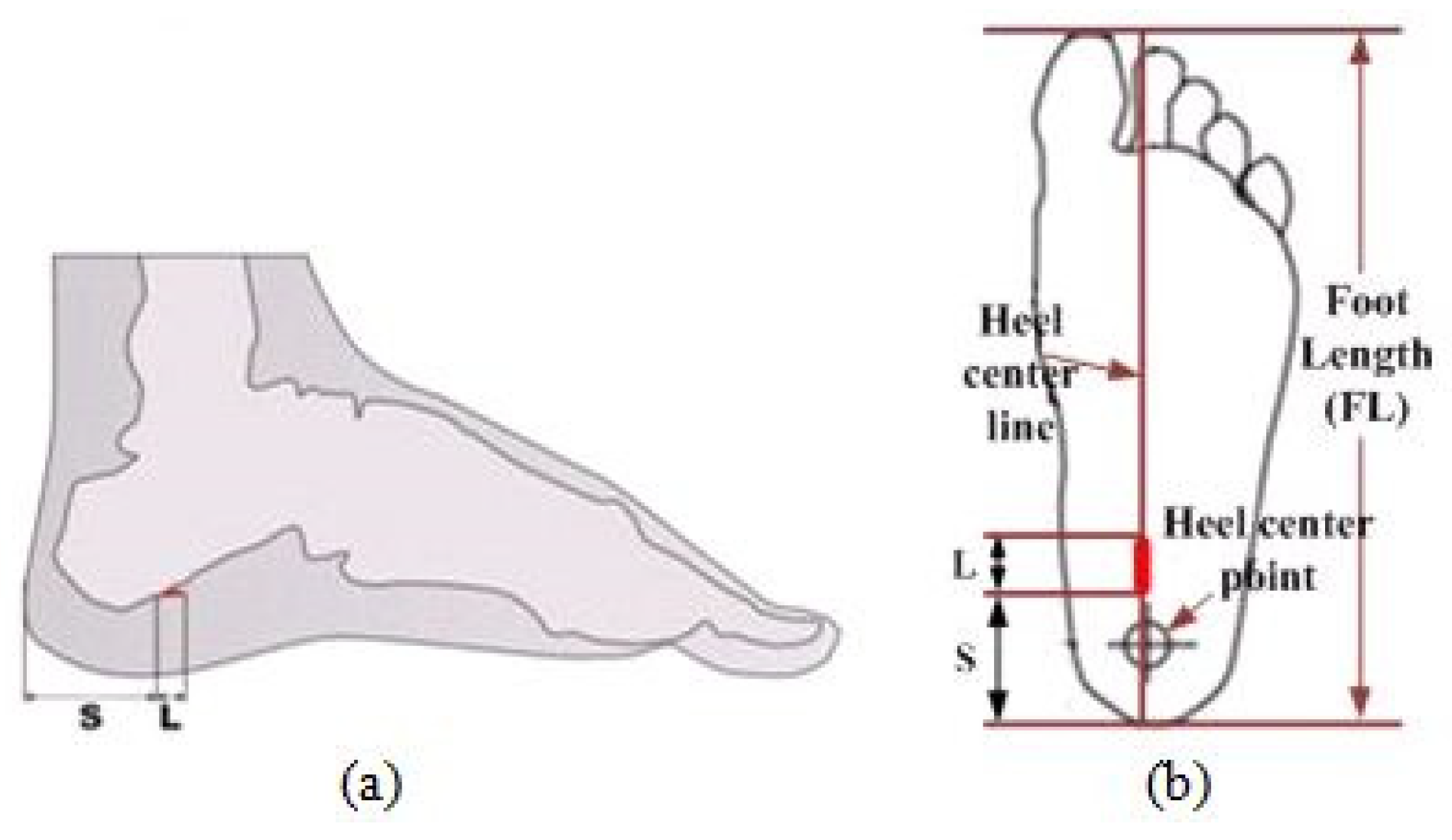
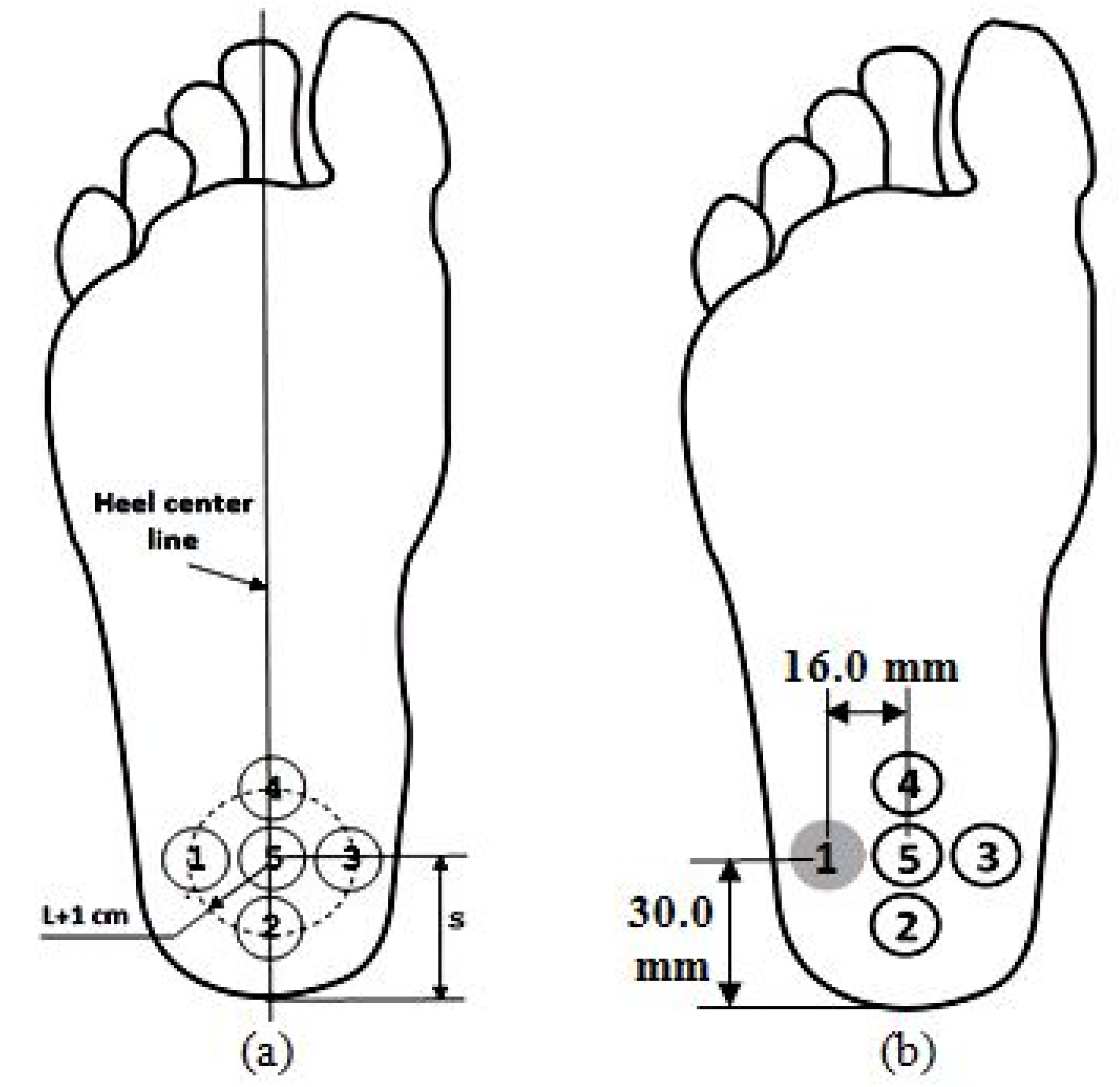
Thirteen volunteers, who suffer from calcaneal spur and had been carefully selected by an orthopedic specialist at RSUD, a local public hospital in Tugurejo Semarang, were involved in this study. Each of the individuals had signed a consent form related to the study of calcaneal spurs. The location and dimension of the calcaneal spur of each individual was determined using an X-Ray, with S and L denoting the distance from the tip of the heel to the base of the spur growth, and the length of spur, respectively, as shown in Figure 1a. To observe the location and dimension of the spur in plantar view, the X-Ray image was plotted by using digital footprint, which also displays foot length (FL), foot width (FW), shoe size, and foot type [21,22]. In this study, the base of spur is assumed to be located in the heel center line, which is a line drawn from the center of the heel to the tip of the second toe, as shown in Figure 1b [21,22]. Table 1 shows the spur location and dimension for the 13 volunteers with their details.
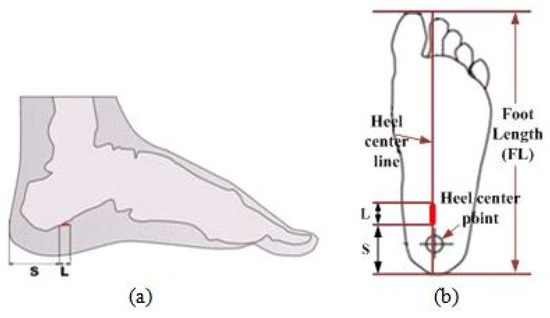
Figure 1.
Determination of spur location and dimension in plantar view.

Table 1.
Subject characteristics.
The volunteers consist of five males and eight females, with a mean age of 56.5 years. Three of the volunteers are public servants, whose activities require them to stand and walk for a long duration of time during the day. The other volunteers consist of four factory workers, three unemployed persons and three housewives, all of whom are required to stand often. These volunteers have been suffering from heel pain due to calcaneal spur since, on average, 1.5 years ago, and have been prescribed nonsteroidal anti-inflammatory drug and/or corticosteroid injections, for treatment. The surgical procedure was never done in the last 10 years because the individual previously complained that their foot could not be used to walk after the surgery and that an infection occurred due to the individuals’ living environment not being clean.
Research ethics committee guidelines, relating to volunteers of RSUD Tugurejo for research purposes, were duly followed. Pain in the heel area of each volunteer was inspected, giving emphasis around the area of the spur growth. All subjects had experienced no pain in the foot other than calcaneal spur. Pain test was done by pressing certain points on the heel area by using a rigid stick with diameter of 1.0 cm or more, and prior to the test being done, the volunteers were instructed not to consume any anti-inflammatory drug. The purpose of inspection is to determine the pain minimum compressive pressure (PMCP) and its associated location in the heel area, with pain known from the volunteer’s facial expression (qualitatively rated on a scale of 0 to 10) [23].
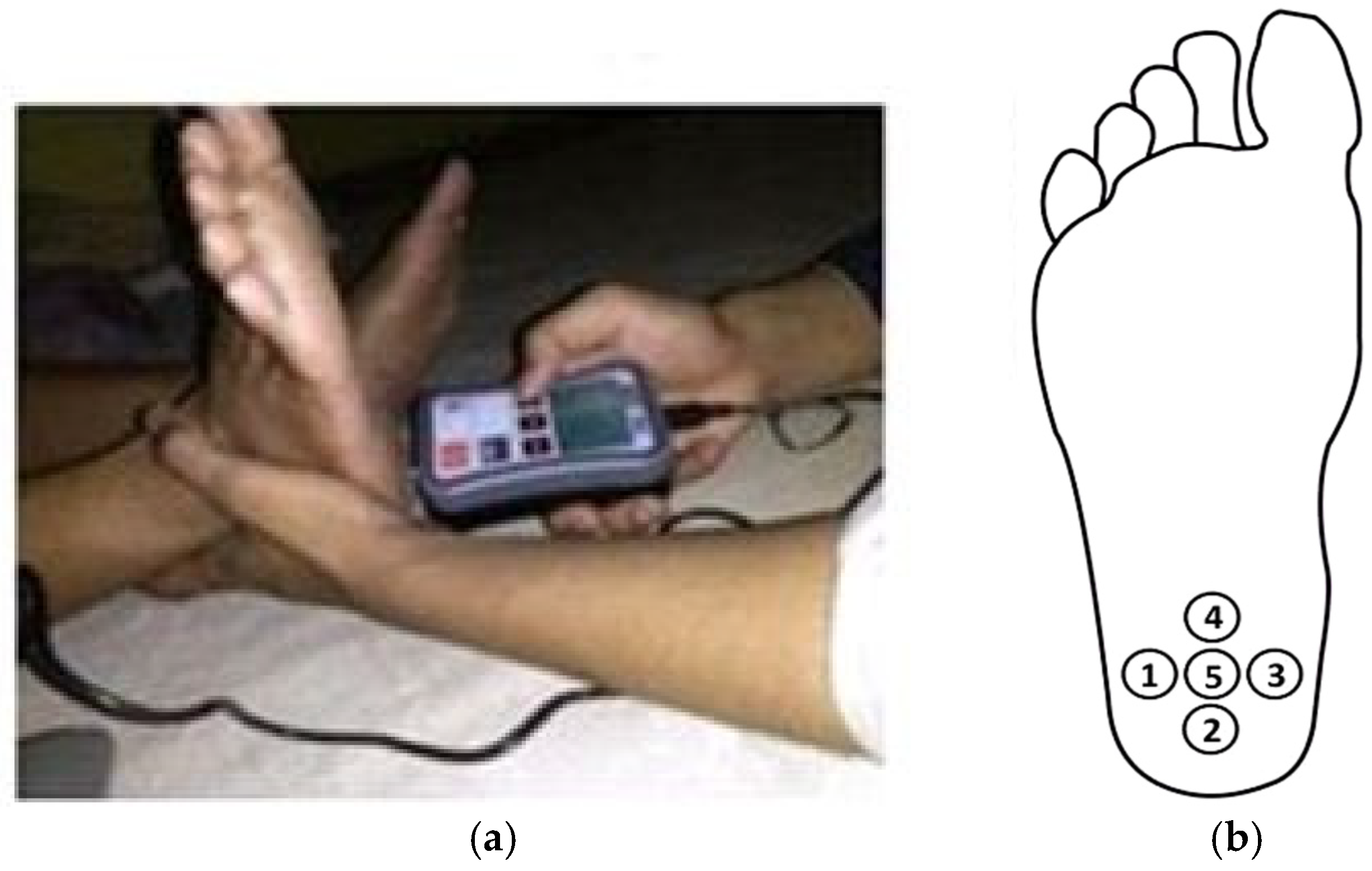
The pain test has been conducted using algometer FDIX 25 (Wagner Instruments, Greenwich, CT, USA), as shown in Figure 2a [24]. This device consists of a flat rubber tip probe of 1.0 cm in diameter, which is applied perpendicular to the skin, with the pressure transmitted to a load cell to produce a voltage output. The signal is transduced and amplified, and subsequently, the output is displayed in newton or kilogram (pressure is equal to force divided by the probe area).
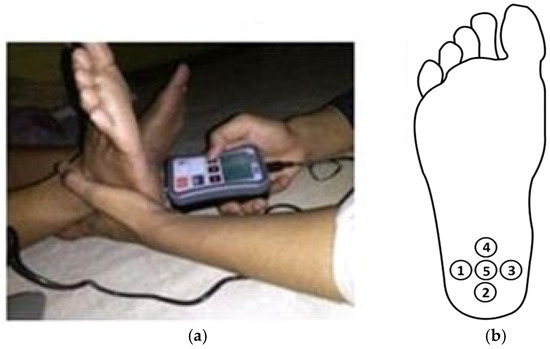
Figure 2.
(a) Pain test in the heel region using algometer FDIX 25; (b) Five pain compressive points.
There are five pain compressive points specified in this study. The fifth point is set at the base of the spur, the fourth point is set at the end of the spur add 1.0 cm, and another three points are set around the spur with the radius equal to spur length added with 1.0 cm, as presented in Figure 2b [22]. The procedure of pain test are as follows: (1) mark the five pressure points around the spur growth with a marker, (2) press the skin at fifth point, (3) increase the pressure gradually and stop until the volunteer screams “ouch”, (4) take a note on the pressure value, (5) apply the same pressuring procedure at point 4, point 3, point 2 and point 1. From the record of quantitative data of the pain test, the PMCP and its associated point location on the heel of each individual can be determined. This PPT measurement procedure is represented as a flowchart, in Figure 3.
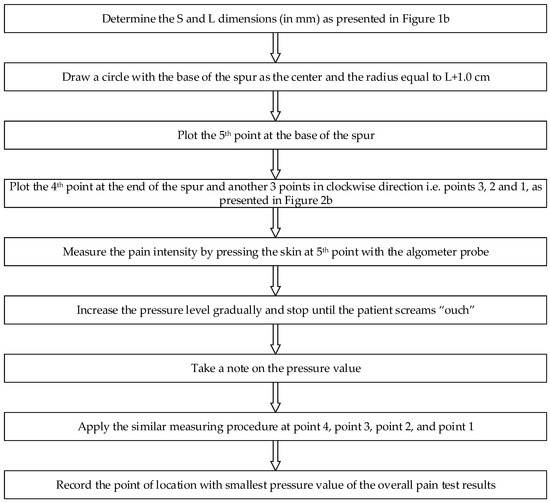
Figure 3.
The PPT measurement procedure.
3. Results
From the 13 volunteers, seven volunteers suffer calcaneal spur on both feet, as shown in Table 1. Testing pressure of pain on these volunteers was done on both their right and left foot, such that a total of 20 sets of testing were performed. Only the smallest recorded pressure pain from the volunteers, who suffer calcaneal spur on both feet, was used as the basis for the evaluation of pain, and only the longest spur was recorded. Table 2 shows PMCP test results sorted by the volunteers’ occupation. Body mass index (BMI) can be calculated by dividing the body weight (in kg) to the squared height (in m2) and was used to classify the volunteers into three groups: normal weight with BMI value between 18.5–24.9 kg/m2, overweight with BMI value between 25.0–29.9 kg/m2, and obese with BMI ≥ 30 kg/m2 [25]. Consequently, eight volunteers had been as normal weight, four volunteers as overweight, and one volunteer as obese.
Table 2.
PMCP test results.
The average length of spur of all volunteers is 4.5 mm. There are two volunteers whose spur lengths are classified as small, seven volunteers as medium, and four volunteers as large. PMCPs for the volunteers vary between 1.17 to 2.95 kg/cm2, with an average of 1.89 kg/cm2. The average PMCP of adults (age between 18–50 years old), and elderly (age between 51–75 years old), are 1.93 kg/cm2, and 1.83 kg/cm2, respectively, whilst the average PMCP of males and females are 1.99 kg/cm2 and 1.75 kg/cm2, respectively. Averages for occupational groups are 2.64 kg/cm2, 2.18 kg/cm2, and 1.58 kg/cm2, for housewife, unemployed, and working volunteers, respectively. For different points on the heel, the average PMCP at point 1 is 1.82 kg/cm2 (4 subjects), point 2 is 1.17 kg/cm2 (1 subject), point 4 is 2.01 kg/cm2 (6 subjects), and point 5 is 2.06 kg/cm2 (2 subjects). No PMCP point has been identified at point 3.
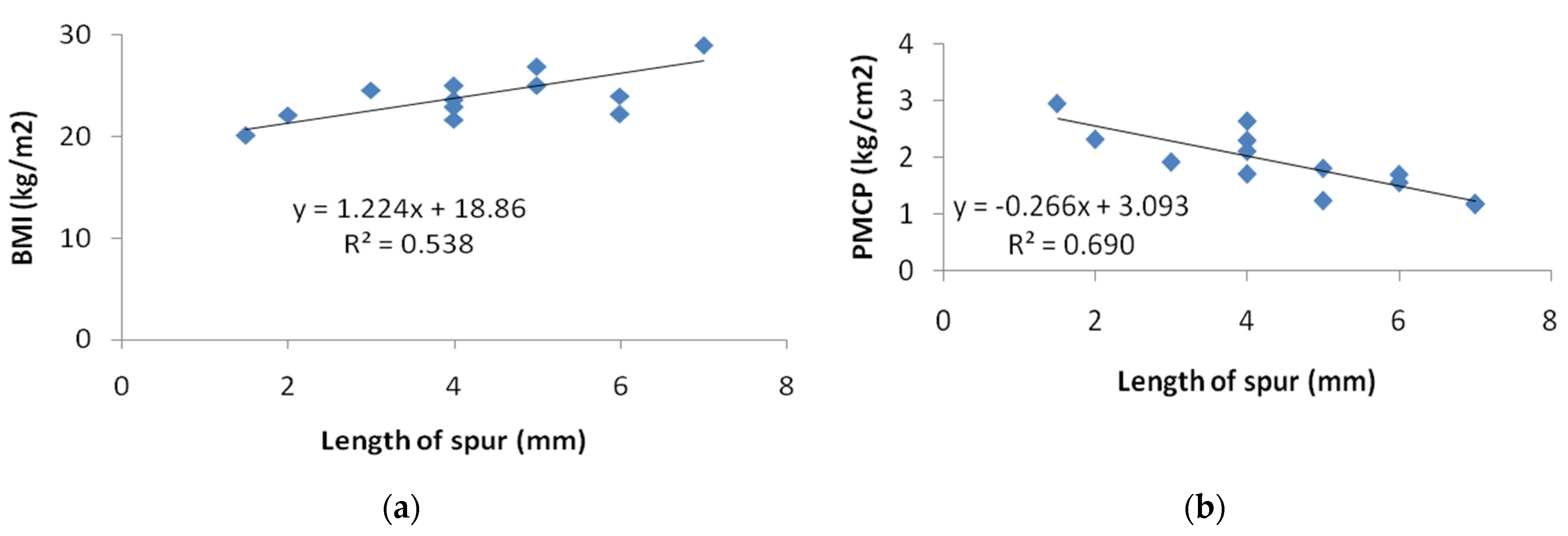
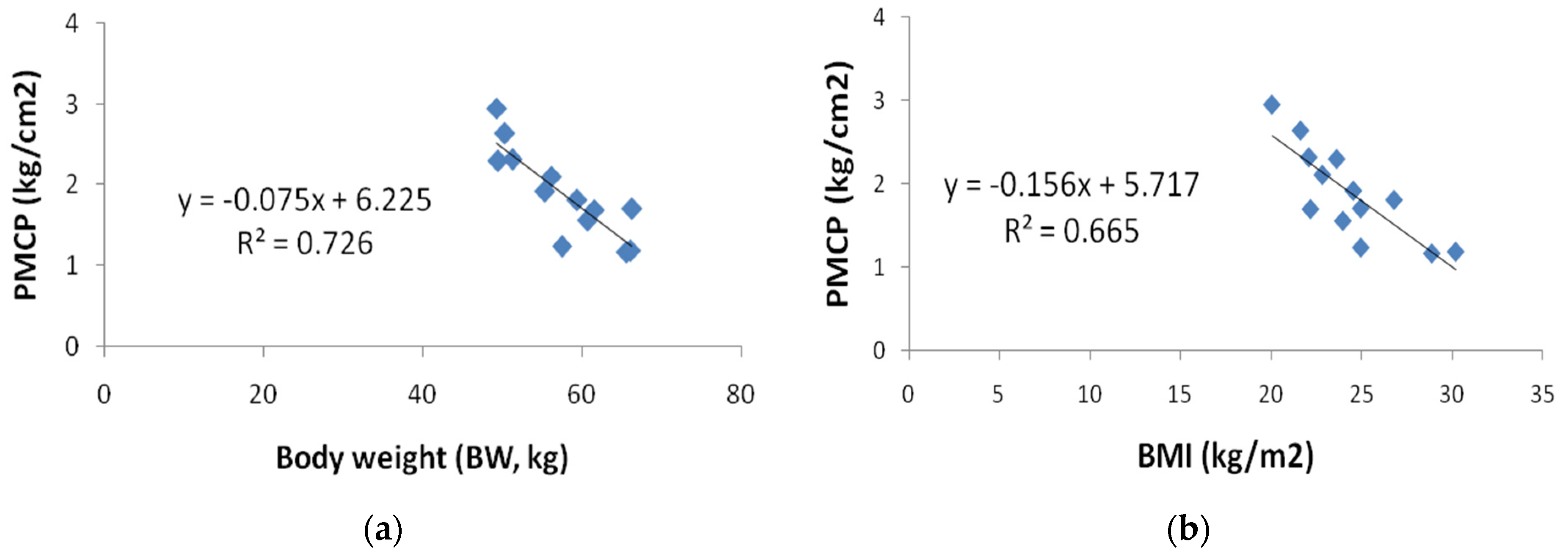
The correlations between length of spur and BMI; and between length of spur and PMCP, can be presented as linear regressions with correlation coefficients of 0.73 and 0.83, as shown in Figure 4a,b, respectively. Figure 5 shows the correlation between BW and PMCP; and between BMI and PMCP, which can also be presented with linear regressions with correlation coefficients of 0.85 and 0.82, as shown in Figure 5a,b, respectively. The relation between age and PMCP shows an inverse relationship but is very insignificant as shown by the correlation coefficient of only 0.14.
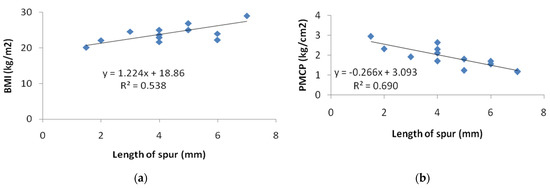
Figure 4.
The correlation between lengths of spur with: (a) Body mass index (BMI); and (b) Pain minimum compressive pressure (PMCP).
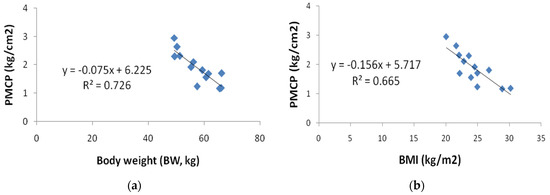
Figure 5.
(a) The correlation between body weight (BW) with pain minimum compressive pressure (PMCP); (b) The correlation between body mass index (BMI) with pain minimum compressive pressure (PMCP).
Figure 6 shows the correlation between the classifications of gender, age, occupation, and spur location, and the average PMCPs. Low PMCP value indicates that light/low pressure has caused the volunteer to scream in pain. From the results, it can be concluded that generally female felt more pain than male, elderly felt more pain than adult, and volunteers who worked felt more pain than those who did not work and housewife. Furthermore, the average PMCP at point 1 is lower than in points 4 and 5.

Figure 6.
The correlation between the classification of gender, age, occupation, and spur location to the average pain minimum compressive pressure (PMCP).
4. Discussion
Figure 4b shows that the longer the spur, the more painful it is. This is consistent with reality, whereby the longer the spur, the greater the bending moment occurring at the base of the spur, and consequently, the more painful it is. The pain at the spur and the length of the spur, are also related to BW. It can be seen from Figure 4a and Figure 5a, that the weight of the volunteers not only significantly increases the length of the spur but also heel pain [6,7,8]. In addition, obese volunteers generally experience more pain than volunteers with normal BMI, as can be seen in Figure 5b [6].
Figure 6 show that PMCP of elderly is less than adult. It indicates that elderly patients felt more pain than adult patients. Therefore, calcaneal spurs as form of foot disorder can negatively influence elderly people. Another researcher reported that foot disorders can negatively influence elderly people, thus affecting their condition of frailty [26]. This is in contrast to the conclusions reached from another research work based on telephone survey in relation to daily weight-bearing activity, which concluded that adults felt more pain than the elderly [12]. These differences may be due to the differences in the methods of inspection of pain. In reference [12], qualitative and subjective method of measuring pain was used, without giving detail relationship between pain levels and their daily activities. On the other hand, the level of pain was obtained from the pain test using algometer in this study, and hence, it is quantitative in nature. Figure 6 also demonstrates that volunteers who actively engage in work feel more pain than those who do not work [5]. This is because pain in the heel would need to be withstand whilst working, causing the heel conditions to deteriorate even further, and consequently, making the pain threshold to be even lower. The condition is different on volunteers who do not work; they can sit or lie down to rest their heel, when they feel the pain. Figure 6 also shows that females with plantar heel pain syndrome demonstrate significantly lower PPTs than males [5].
The results of pain pressure tests on the 13 volunteers demonstrates that a large portion of the volunteers (46%) experience pain on the tip of the spur (point 4). 31% and 15% of the volunteers’ experience pain on the lateral side (point 1), and central or base of the spur (point 5), respectively. However, the average PMCP on the lateral side (point 1) is relatively lower than on points 4 and 5. This result is consistent with the reality that the compressive force on the end of spur produces the lowest PPT. Another group of researchers has also reported that PPT levels at medial and central sites are lower than at sites lateral, from subjects with plantar heel pain syndrome, who are not specifically due to calcaneal spurs [19]. In this study, the locations of the probe of the algometer on the calcaneal spur sufferers, have been placed strategically around the spur growth, and results have indicated that areas around the spur end give lower PMCP value as compared to the spur base.
Pain suffered by calcaneal spur volunteers whilst standing or walking is generally caused by the improper distribution of large pressure in the calcaneus region. This is consistent with the measurement obtained using a foot plantar measurement system [10,11]. To correct the distribution, orthotic shoes with increased heel height can be used [21]. However, this may be impractical for the subject populations, especially male volunteers who work as public servants. Alternatively, a flat heel height shoe but with a softer material in the heel area of the in-sole, as shown in Figure 7 [27] may be used. Similar shoe-insoles in the form of inserts have been sold in the market, but they are not effective in reducing pain in volunteers with calcaneal spur, as the insertion area, which is made of soft silicone rubber, does not properly support the area with the smallest PPT.

Figure 7.
Soft shoe in-sole insert material in the heel for people with calcaneal spur.
Foot pain can be minimized by redistributing pressure from the affected area for example using shoe in-sole [28]. Accurate foot pressure distribution measurements can be obtained using foot scanner [29], however this method is in many ways less practical. PMCP measurement using an algometer offers a simpler technique for detecting heel pain. So that appropriate treatment for each patient can be given, therefore no large patient samples are needed. Another example of foot pain measurement based on visual analogic scale is presented in [30].
In this study, PMCP measurement method using an algometer intends to guide and assist orthotic shoe designer by placing a softer material in the heel area where the PMCP of patient is the smallest. As the exact location is person specific, large samples are not necessarily needed. Details of each individual, including age, gender, occupation, shoe size, the distance from the tip of the heel to the base of the spur (S); length of spur (L); and PMCP location of left and/or right foot, need to be recorded. Age, gender, and occupation are required to determine the appropriate type and model of shoes, whilst shoe size, the distance from the tip of the heel to the base of the spur (S); length of spur (L), and the PMCP location, are required to design a proper shoe in-sole material with a certain hardness [20].
Figure 8 illustrates an example of a shoe in-insole with a softer material in the heel area, of the right foot of volunteer #9. The location of PMCP is at point 1, with the distance from the heel tip equal to S = 30 mm and from the heel center line the length of spur, L = 6 mm plus the diameter of the algometer tip probe 10 mm. Putting a softer material in the right location and slightly raising the heel height of the shoe (especially for female volunteers) or alternatively, slightly enlarging the contour area in the heel region of the shoe in-sole [21], significantly reduce the pressure in that area.
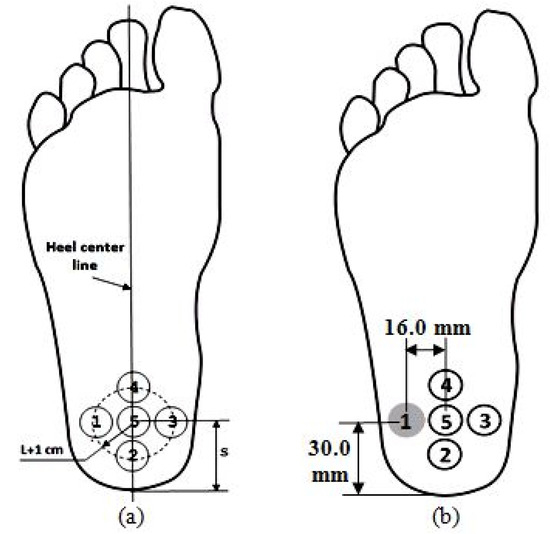
Figure 8.
Soft shoe in-sole insert material in the heel area for volunteer #9: (a) Definition and notation; (b) The dimensions of the distances for soft material laying.
5. Conclusions
Pressure algometry can be used to objectively and quantitatively determine the best heel location, such that optimal improvement towards the relief of pain can be achieved using orthotic shoe. The information on shoe size, spur location and dimensions, and the PMCP location of each individual are essential to obtain the exact point location, in order to apply a softer material in the heel area of the shoe in-sole. Putting a softer material in the right location plus slightly raising the heel height of the shoe, especially for female, significantly reduces the pressure in that area. It has also been shown that the level of pain increases with increasing weight; another incentive for individual to reduce body weight, in order to reduce pain in the heel area. An alternative method to detect the presence or absence of calcanea spurs on the heel using algometer is presented. An algometer is able to show quantitatively the amount of pressure applied. The magnitude of the pressure and the response of the sample to pain can be used to determine PMCP. Therefore, the small number of samples in our opinion is sufficient to obtain the PMCP value.
Future work: the results of this research will be used to design shoe in-sole according to PMCP measurement data and the effectiveness of these shoe in-sole in minimizing pain in the sample.
Author Contributions
Conceptualization, D.B.W.; methodology, D.B.W. and A.S.; software, W.C.; validation, D.B.W.; A.S.; and W.C.; formal analysis, W.C.; investigation, R.H.; resources, A.S.; data curation, R.H.; writing—original draft preparation, D.B.W.; writing—review and editing, W.C., A.G. and P.E.A.; visualization, A.S.; supervision, R.H.; project administration, D.B.W. funding acquisition, A.G., R.T. and E.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Barrett, S.J.; O’Malley, R. Plantar fasciitis and other causes of heel pain. Am. Fam. Physician 1999, 59, 2200–2206. [Google Scholar]
- Zhou, B.; Zhou, Y.; Tao, X.; Yuan, C.; Tang, K. Classification of Calcaneal Spurs and Their Relationship with Plantar Fasciitis. J. Foot Ankle Surg. 2015, 54, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Johal, K.S.; Milner, S.A. Plantar fasciitis and the calcaneal spur: Fact or fiction? Foot Ankle Surg. 2012, 18, 39–41. [Google Scholar] [CrossRef]
- Kuyucu, E.; Koçyiğit, F.; Erdil, M. The association of calcaneal spur length and clinical and functional parameters in plantar fasciitis. Int. J. Surg. 2015, 21, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Malay, D.S. Plantar fasciitis and heel spur syndrome: A retrospective analysis. In Reconstructive Surgery of the Foot and Leg: Update ’96; Vickers, N.S., Ed.; Podiatry Institute Publishing: Tucker, GA, USA, 1996; pp. 39–43. [Google Scholar]
- Bartold, S.J. The plantar fascia as a source of pain—Biomechanics, presentation and treatment. J. Bodyw. Mov. Ther. 2004, 8, 214–226. [Google Scholar] [CrossRef]
- Brinks, A.; Koes, B.W.; Volkers, A.C.W.; Verhaar, J.A.N.; Bierma-Zeintra, S.M.A. Adverse effects of extra-articular corticosteroid injections: A systematic review. BMC Musculoskelet. Disord. 2010, 11, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turlik, M.; Donatelli, T.; Veremis, M. A comparison of shoe inserts in relieving mechanical heel pain. Foot 1999, 9, 84–87. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.L.; Christensen, J.C.; Kravitz, S.R.; Mendicino, R.W.; Schuberth, J.M.; Vanore, J.V.; Weil, L.S., Sr.; Zlotoff, H.J.; Bouché, R.; Baker, J.; et al. The Diagnosis and Treatment of Heel Pain: A Clinical Practice Guideline—Revision 2010. J. Foot Ankle Surg. 2010, 40, 329–340. [Google Scholar] [CrossRef]
- Jason Chia, K.K.; Suresh, S.; Kuah, A.; Ong, J.L.; Phua, J.M.; Seah, A.L. Comparative trial of the foot pressure patterns between corrective orthotics, formthotics, bone spur and flat insoles in patients with chronic plantar fasciitis. Ann. Acad. Med. Singap. 2009, 38, 869–875. [Google Scholar] [PubMed]
- Giddings, V.L.; Beaupré, G.S.; Whalen, R.T.; Carter, D.R. Calcaneal loading during walking and running. Med. Sci. Sports Exerc. 2000, 32, 627–634. [Google Scholar] [CrossRef]
- Özdemır, H.; Söyüncü, Y.; Özgörgen, M.; Dabak, K. Effects of Changes in Heel Fat Pad Thickness and Elasticity on Heel Pain. J. Am. Podiatr. Med. Assoc. 2004, 94, 47–52. [Google Scholar] [CrossRef]
- Sayed-Noor, A.S.; Englund, E.; Wretenberg, P.; Sjoden, G.O. Pressure-Pain Threshold Algometric Measurement in Patients with Greater Trochanteric Pain After Total Hip Arthroplasty. Clin. J. Pain 2008, 24, 232–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, G.-N.; Lars, A.-N. Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat. Rev. Rheumatol. 2010, 6, 599–606. [Google Scholar] [CrossRef]
- Walton, D.; MacDermid, J.; Nielson, W.; Teasell, R.; Nailer, T.; Maheu, P. A Descriptive Study of Pressure Pain Threshold at 2 Standardized Sites in People with Acute or Subacute Neck Pain. J. Orthop. Sports Phys. Ther. 2011, 41, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Park, G.; Kim, C.W.; Park, S.B.; Kim, M.J.; Jang, S.H. Reliability and Usefulness of the Pressure Pain Threshold Measurement in Patients with Myofascial Pain. Ann. Rehabil. Med. 2011, 35, 412–417. [Google Scholar] [CrossRef] [Green Version]
- Özdolap, N.; Sarikaya, S.; Kokturk, F. Evaluation of Pain Pressure Threshold and Widespread Pain in Chronic Low Back Pain. FTR-Turk. Fiz. Tip ve Rehabil. Derg. 2014, 60, 32–36. [Google Scholar] [CrossRef]
- Mutlu, E.K.; Ozdincler, A.R. Reliability and responsiveness of algometry for measuring pressure pain threshold in patients with knee osteoarthritis. J. Phys. Ther. Sci. 2015, 27, 1961–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saban, B.; Masharawi, Y. Pain Threshold Tests in Patients with Heel Pain Syndrome. Foot Ankle Int. 2016, 37, 730–736. [Google Scholar] [CrossRef]
- Sandro, R.; Pergine, V. Insole Foe Sports Shoes, Particularly for Golf. U.S. Patent 2008.0086909, 17 April 2008. [Google Scholar]
- Wibowo, D.B.; Harahap, R.; Widodo, A.; Haryadi, G.D.; Ariyanto, M. The effectiveness of raising the heel height of shoes to reduce heel pain in patients with calcaneal spurs. J. Phys. Ther. Sci. 2017, 29, 2068–2074. [Google Scholar] [CrossRef] [Green Version]
- Haryadi, G.D.; Wibowo, D.B.; Ariyanto, M.; Suprihanto, A. Digital Scanning Method for Evaluation of Dimensional Parameters and Identification of Foot Type. Indonesian Patent No. IDS000002253, 2 April 2019. [Google Scholar]
- Holy Redeemer. Pain Level Chart. Available online: http://www.holyredeemer.com/Uploads/Public/Documents/2011%20Pain%20Level%20Chart.pdf (accessed on 23 October 2020).
- Wagner Instruments. Wagner FPTX Series Economy Manual Pain Threshold Testers. Pain TestTM Algometer, USA. Available online: http://www.wagnerinstruments.com/products/PAIN-TEST-Algometers (accessed on 20 June 2021).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Navarro-Flores, E.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C.; Losa-Iglesias, M.E.; Palomo-López, P.; Mazoteras-Pardo, V.; Romero-Morales, C.; López-López, D. Influence of foot pain on frailty symptoms in an elderly population: A case-control study. Sao Paulo Med. J. 2021, 139, 319–324. [Google Scholar] [CrossRef]
- Kennedy, S. Stepping Out—Designing Foot Orthotics. The O&P Edge. 2003. Available online: www.oandp.com/edge (accessed on 20 July 2021).
- Wibowo, D.B.; Suprihanto, A.; Caesarendra, W.; Khoeron, S.; Glowacz, A.; Irfan, M. A Simple Foot Plantar Pressure Measurement Platform System Using Force-Sensing Resistors. Appl. Syst. Innov. 2020, 3, 33. [Google Scholar] [CrossRef]
- Wibowo, D.B.; Widodo, A.; Haryadi, G.D.; Caesarendra, W.; Harahap, R. Effect of in-shoe foot orthosis contours on heel pain due to calcanea spur. Appl. Sci. 2019, 9, 493. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Flores, E.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; López-López, D.; Rodríguez-Sanz, D.; Palomo-López, P.; Calvo-Lobo, C. Translation and Test–Retest of the Spanish Podiatry Health Questionnaire (PHQ-S). Int. J. Environ. Res. Public Health 2018, 15, 2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).