Technology-Supported Group Activity to Promote Communication in Dementia: A Protocol for a Within-Participants Study †


Abstract
1. Introduction
1.1. Information and Communication Technologies (ICTs)
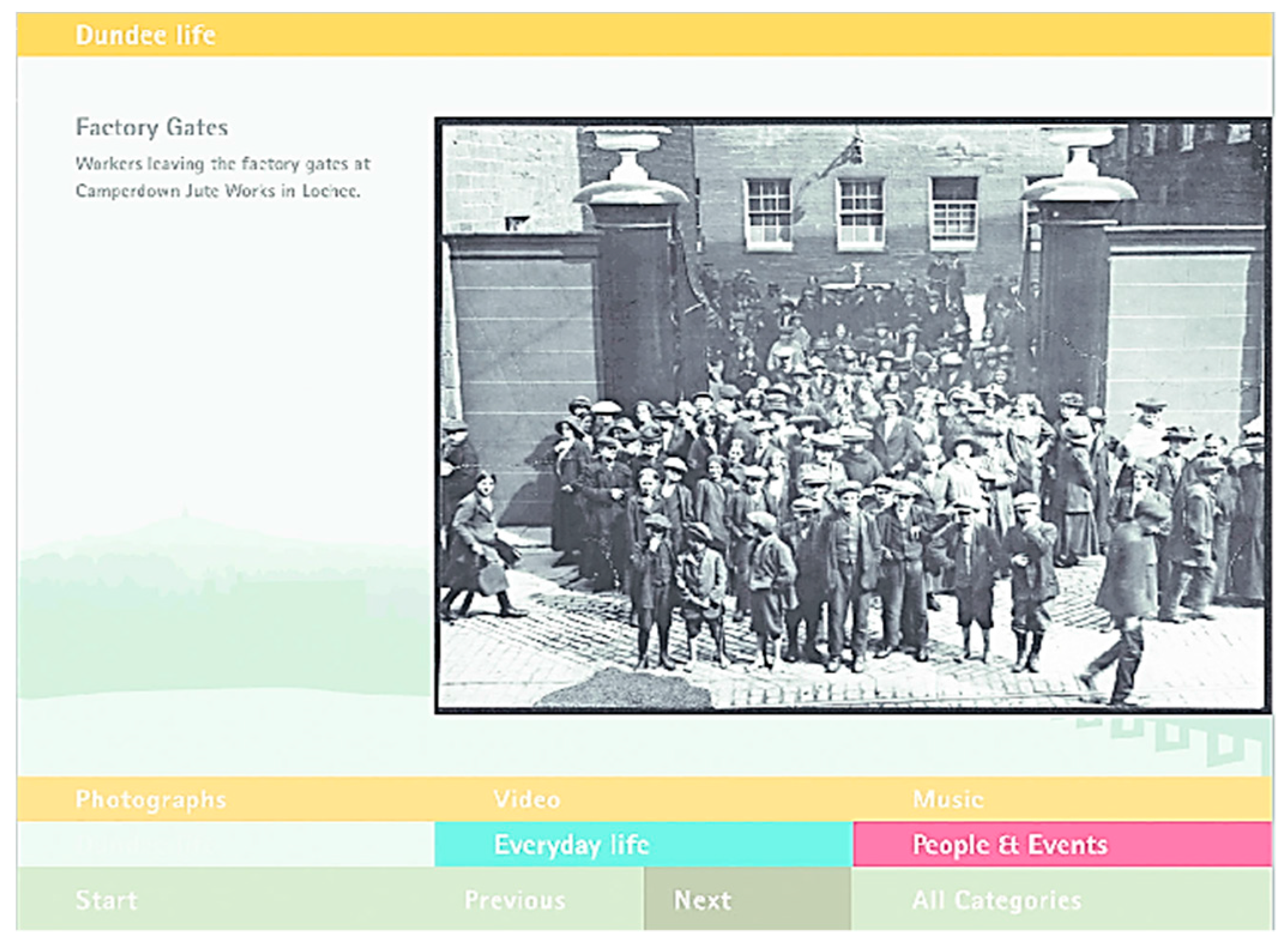
1.2. Computer Interactive Reminiscence and Conversation Aid (CIRCA)
1.3. Current Study
2. Methods
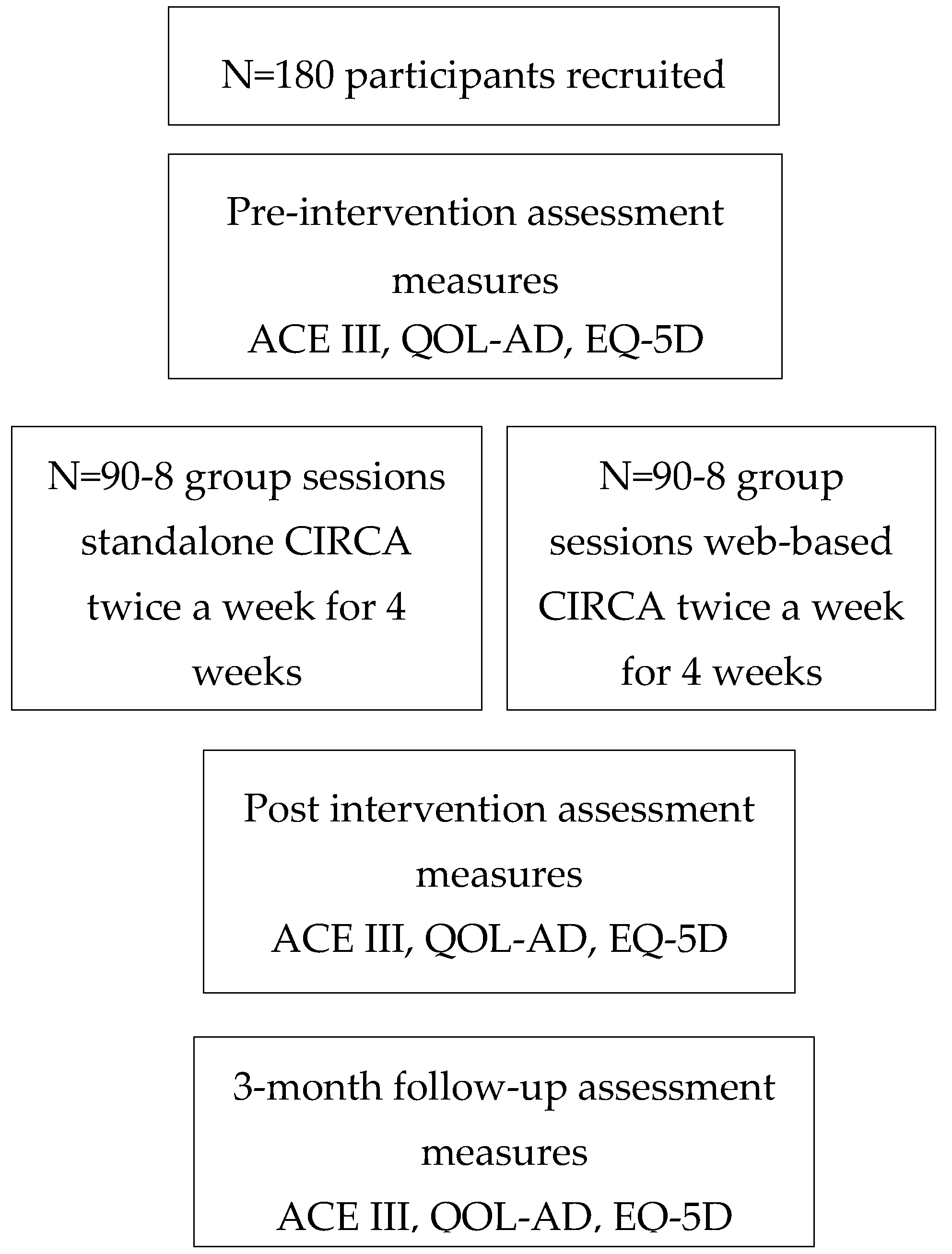
2.1. Design
2.2. Sample Size
2.3. Ethics
2.4. Participants
2.5. Recruitment Strategy
3. Materials
3.1. Assessment Measures
3.2. Cognition
3.3. Quality of Life
3.4. Health Status
4. Procedure
4.1. CIRCA Group Activity
4.2. Analysis
5. Discussion
6. Trial Status
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Prince, M.; Albanese, M.; Guerchet, E.; Prina, M. World Alzheimer Report; Alzheimer’s Disease International: London, UK, 2014. [Google Scholar]
- Alzheimer’s Association. 2017 Alzheimer’s Disease Facts and Figures; Alzheimer’s Association: Chicago, IL, USA, 2017. [Google Scholar]
- Egan, K.; Macleod, M. Two decades testing interventions in transgenic mouse models of Alzheimer’s disease: Designing and interpreting studies for clinical trial success. Clin. Investig. 2014, 4, 693–704. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Baddeley, A.; Logie, R.; Bressi, S.; della Sala, S.; Spinnler, H. Dementia and Working Memory. Q. J. Exp. Psychol. Sect. A 1986, 38, 603–618. [Google Scholar] [CrossRef]
- Gold, C.A. Memory loss in Alzheimer’s disease: Implications for development of therapeutics. Expert Rev. Neurother. 2009, 8, 1879–1891. [Google Scholar] [CrossRef] [PubMed]
- Astell, A.J.; Ellis, M.P.; Bernardi, L.; Alm, N.; Dye, R.; Gowans, G.; Campbell, J. Using a touch screen computer to support relationships between people with dementia and caregivers. Interact. Comput. 2010, 22, 267–275. [Google Scholar] [CrossRef]
- Alm, N.; Dye, R.; Gowans, G.; Campbell, J.; Astell, A.; Ellis, M. A communication support system for older people with dementia. Computer 2007, 40, 35–41. [Google Scholar] [CrossRef]
- Searson, R.; Hendry, A.M.; Ramachandran, R.; Burns, A.; Purandare, N. Activities enjoyed by patients with dementia together with their spouses and psychological morbidity in carers. Aging Ment. Health 2008, 12, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Dementia: A State of the Nation Report on Dementia Care and Support in England; Department of Health: London, UK, 2013.
- Spector, A.; Thorgrimsen, L.; Woods, B.; Royan, L.; Davies, S.; Butterworth, M.; Orrell, M. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: Randomised controlled trial. Br. J. Psychiatry 2003, 183, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Spector, A.; Orrell, M.; Davies, S.; Woods, B. Can reality orientation be rehabilitated? Development and piloting of an evidence-based programme of cognition-based therapies for people with dementia. Neuropsychol. Rehabil. 2001, 11, 377–397. [Google Scholar] [CrossRef]
- Department of Health. The Dementia Challenge: Driving Improvements in Health; Department of Health: London, UK, 2015.
- Burstein, A.A.; DaDalt, O.; Kramer, B.; D’Ambrosio, L.A.; Coughlin, J.F. Dementia caregivers and technology acceptance: Interest outstrips awareness. Gerontechnology 2015, 14, 45–56. [Google Scholar] [CrossRef]
- Astell, A.J. Technology and personhood in dementia care. Qual. Ageing 2006, 7, 15–25. [Google Scholar] [CrossRef]
- Gilliard, J. Dementia care in England and the social model of disability: Lessons and issues. Dementia 2005, 4, 571–586. [Google Scholar] [CrossRef]
- Innes, A. Dementia Studies: A Social Science Perspective; SAGE Publications Ltd.: Thousand Oaks, CA, USA; London, UK, 2009. [Google Scholar]
- The National Institute for Health and Care Excellence. Dementia: Supporting People with Dementia and Their Carers in Health and Social Care; The National Institute for Health and Care Excellence: London, UK, 2006. [Google Scholar]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Buckingham, UK, 1997. [Google Scholar]
- Banerjee, S. Living well with dementia—Development of the national dementia strategy for England. Int. J. Geriatr. Psychiatry 2010, 25, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Vernooij-dassen, M.J.; Moniz-Cook, E.D.; Woods, R.T.; De Lepeleire, J.; Leuschner, A.; Zanetti, O.; de Rotrou, J.; Kenny, G.; Franco, M.; Peters, V.; et al. Factors affecting timely recognition and diagnosis of dementia—From awareness to stigma 2005. Int. J. Geriatr. Psychiatry 2005, 20, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Wells, D.L.; Dawson, P. Description of retained abilities in older persons with dementia. Res. Nurs. Health 2000, 23, 158–166. [Google Scholar] [CrossRef]
- Brody, H.; Kleban, E.; Lawton, M.; Silverman, P. Excess Disabilities of Mentally Impaired Aged: Impact of Individualized Treatment. Gerontologist 1971, 11, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Astell, A.J. Supporting a good life with dementia. In Ageing and the Digital Life Course; Prendergast, D., Garattini, C., Eds.; Berghan Books: Oxford, UK, 2015. [Google Scholar]
- Smith, S.K.; Mountain, G.A. New forms of information and communication technology (ICT) and the potential to facilitate social and leisure activity for people living with dementia. Int. J. Comput. Healthc. 2012, 1, 332–345. [Google Scholar] [CrossRef]
- Meiland, F.; Innes, A.; Mountain, G.; Robinson, L.; van der Roest, H.; García-Casal, J.A.; Gove, D.; Thyrian, J.R.; Evans, S.; Dröes, R.M.; et al. Technologies to Support Community-Dwelling Persons with Dementia: A Position Paper on Issues Regarding Development, Usability, Effectiveness and Cost-Effectiveness, Deployment, and Ethics. JMIR Rehabil. Assist. Technol. 2017, 4, e1. [Google Scholar] [CrossRef] [PubMed]
- Nygard, L. The meaning of everyday technology as experienced by people with dementia who live alone. Dementia 2008, 7, 481–502. [Google Scholar] [CrossRef]
- Topo, P. Technology Studies to Meet the Needs of People with Dementia and Their Caregivers: A Literature Review. J. Appl. Gerontol. 2008, 28, 5–37. [Google Scholar] [CrossRef]
- Cutler, C.; Hicks, B.; Innes, A. Technology, fun and games. J. Dement. Care 2014, 22, 12–13. [Google Scholar]
- Leng, F.Y.; Yeo, D.; George, S.; Barr, C. Comparison of iPad applications with traditional activities using person-centred care approach: Impact on well-being for persons with dementia. Dementia 2014, 13, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Lazar, A.; Demiris, G.; Thompson, H.J. Involving family members in the implementation and evaluation of technologies for dementia: A dyad case study. J. Gerontol. Nurs. 2015, 41, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.K. Exploring the Potential of Touch-Screen Computer Technology in Promoting Enjoyable Activities for People Living with Dementia: A Visual Ethnography Sarah Kate Smith a Thesis Submitted to the University of Sheffield in Partial Fulfilment of the Requiremen; University of Sheffield: Sheffield, UK, 2015. [Google Scholar]
- Robinson, L.; Brittain, K.; Lindsay, S.; Jackson, D.; Olivier, P. Keeping in Touch Everyday (KITE) project: Developing assistive technologies with people with dementia and their carers to promote independence. Int. Psychogeriatr. 2009, 21, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Alm, N.; Astell, A.; Ellis, M.; Dye, R.; Gowans, G.; Campbell, J. A cognitive prosthesis and communication support for people with dementia. Neuropsychol. Rehabil. 2004, 14, 117–134. [Google Scholar] [CrossRef][Green Version]
- Astell, A. Facilitating communication in dementia with multimedia technology. Brain Lang. 2004, 91, 80–81. [Google Scholar] [CrossRef]
- Astell, A.J.; Purves, B.; Phinney, A. “Story of My Life?” The Contents and Functions of Reminiscing. Available online: http://www.cs.cornell.edu/~danco/remchiwork/papers/astell-Stimulating-reminiscing-BP-AJA.pdf (accessed on 7 December 2017).
- Fivush, E.; Haden, R.; Reese, C. Remembering, recounting and reminiscing: The development of autobiographical memory in social context. In Rembereing Our Past: Studies in Autobiographical Memory; Rubin, D.C., Ed.; Cambridge University Press: Cambridge, UK, 1995. [Google Scholar]
- Fels, D.I.; Astell, A.J. Storytelling as a model of conversation for people with dementia and caregivers. Am. J. Alzheimers Dis. Other Dement. 2011, 26, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, E.; Bruce, P. Remembering Yesterday, Caring Today: Reminiscence in Dementia Care—A Guide to Good Practice UK; Jessica Kingsley: London, UK, 2008. [Google Scholar]
- Gowans, G.; Dye, R.; Alm, N.; Vaughan, P.; Astell, A.; Ellis, M. Designing the interface between dementia patients, caregivers and computer-based intervention. Des. J. 2007, 10, 12–23. [Google Scholar] [CrossRef]
- Astell, P.; Alm, A.J.; Gowans, N.; Ellis, G.; Dye, M.; Campbell, R.; Vaughan, J. The CIRCA: A communication prosthesis for dementia. Technol. Aging 2008, 105, 64–69. [Google Scholar]
- Astell, M.S.; Parsons, A. CIRCA: Technology to prompt reminiscing and conversation between residents in care homes and care staff. Gerontechnology 2010, 9, 68–69. [Google Scholar] [CrossRef]
- Breuil, V.; de Rotrou, J.; Forette, F.; Tortrat, D.; Ganansia-Ganem, A.; Frambourt, A.; Moulin, F.; Boller, F. Cognitive stimulation of patients with dementia: Preliminary results. Int. J. Geriatr. Psychiatry 1994, 9, 211–217. [Google Scholar] [CrossRef]
- Knapp, M.; Thorgrimsen, L.; Patel, A.; Spector, A.; Hallam, A.; Woods, B.; Orrell, M. Cognitive stimulation therapy for people with dementia: Cost-effectiveness analysis. Br. J. Psychiatry 2006, 188, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.; Schubert, S.; Hoon, C.; Mioshi, E.; Hodges, J.R. Validation of the Addenbrooke’s Cognitive Examination III in Frontotemporal Dementia and Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2013, 36, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Giebel, C.M.; Challis, D. Sensitivity of the Mini-Mental State Examination, Montreal Cognitive Assessment and the Addenbrooke’s Cognitive Examination III to everyday activity impairments in dementia: An exploratory study. Int. J. Geriatr. Psychiatry 2017, 32, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, R.G.; Gibbons, L.E.; McCurry, S.M.; Teri, L. Assessing Quality of Life in Older Adults with Cognitive Impairment. Psychosom. Med. 2002, 64, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Moniz-Cook, E.; Vernooij-Dassen, M.; Woods, R.; Verhey, F.; Chattat, R.; De Vugt, M.; Mountain, G.; O’Connell, M.; Harrison, J.; Vasse, E.; et al. A European consensus on outcome measures for psychosocial intervention research in dementia care. Aging Ment. Health 2008, 12, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Euroqol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Hounsome, N.; Orrell, M.; Edwards, R.T. EQ-5D as a quality of life measure in people with dementia and their carers: Evidence and key issues. Value Health 2011, 14, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Wolfs, C.A.G.; Kessels, A.; Dirksen, C.D.; Severens, J.L.; Verhey, F.R.J. Integrated multidisciplinary diagnostic approach for dementia care: Randomised controlled trial. Br. J. Psychiatry 2008, 192, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Bjorneby, S. Ethical Considerations in the ENABLE Project. Dementia 2004, 3, 297–312. [Google Scholar] [CrossRef]
- Dewing, J. Participatory research A method for process consent with persons who have dementia. Dementia 2007, 6, 11–25. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Diagnosis of dementia according to the Diagnostic & Statistical Manual of Mental Disorders(DSM-5) | Requires consultee involvement |
| Ability to verbally communicate | Sensory impairment that will negatively impact technology participation |
| Secondary long term conditions that could affect group participation | |
| Behavioural challenges that could negatively affect group activities |
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, S.K.; Astell, A.J. Technology-Supported Group Activity to Promote Communication in Dementia: A Protocol for a Within-Participants Study. Technologies 2018, 6, 33. https://doi.org/10.3390/technologies6010033
Smith SK, Astell AJ. Technology-Supported Group Activity to Promote Communication in Dementia: A Protocol for a Within-Participants Study. Technologies. 2018; 6(1):33. https://doi.org/10.3390/technologies6010033
Chicago/Turabian StyleSmith, Sarah K., and Arlene J. Astell. 2018. "Technology-Supported Group Activity to Promote Communication in Dementia: A Protocol for a Within-Participants Study" Technologies 6, no. 1: 33. https://doi.org/10.3390/technologies6010033
APA StyleSmith, S. K., & Astell, A. J. (2018). Technology-Supported Group Activity to Promote Communication in Dementia: A Protocol for a Within-Participants Study. Technologies, 6(1), 33. https://doi.org/10.3390/technologies6010033