1. Introduction
1.1. Background
People with severe intellectual disabilities and visual impairment are often withdrawn and sedentary and lag behind in their developmental process [
1,
2,
3,
4]. In essence, this (marginality and passivity) condition may be connected to their problems in critical areas, such as activity engagement, orientation and mobility, communication, and motivation [
5,
6,
7,
8,
9,
10]. For example, activity engagement requires appropriate object use and motivation to perform the actions (object use responses) involved in the activity [
11,
12]. Yet, many of these people may have a limited ability to discriminate and handle objects and no specific interest in using those objects for completing a specific activity/task [
11,
12,
13,
14,
15]. Orientation and mobility may be prerequisites to gather objects for the activities and to practice basic physical exercise essential for wellbeing [
10,
12,
13,
14]. Yet, many of these people tend to have difficulties orienting and moving even in small indoor areas and, thus, tend to remain sedentary rather than exploring their context [
12,
16,
17,
18,
19].
The complexity of this situation and the need to alleviate the negative consequences associated with it have prompted the development of a variety of intervention programs aimed at promoting people’s general progress and wellbeing [
5,
6,
12,
18]. In particular, efforts were made to develop programs assisted by technology that would provide the types of support necessary for the participants to advance in specific areas of their rehabilitation process [
18,
19,
20,
21]. For example, programs were developed in which technology was adopted to enable the participants to use simple motor actions to make clear requests that would lead to satisfactory (reinforcing) consequences from the environment (consequences that would foster the participants’ motivation to repeat their requests) [
22,
23,
24]. Programs were developed to enable the participants to carry out basic physical exercise independent of staff or caregivers’ direct supervision [
25,
26,
27,
28]. Those programs typically involved the use of technology devices to monitor the participants’ exercise responses and possibly (a) provide the participants with encouragements to emit those responses and (b) follow those responses with brief stimulation events that were expected to motivate the participants to maintain/strengthen the responses.
1.2. Related Work
Programs were also developed to enable participants to orient within a work room and carry out simple activities within such a room. For example, Lancioni et al. [
29] designed a program that involved a smartphone with an Android system, which was fitted with Amazon Alexa, MacroDroid, and Philips Hue applications, as well as indoor motion sensors and mini speakers. The technology was to help seven participants to collect objects from three different areas of the room and bring those objects to a central desk located in the same room through the provision of spatial cues, verbal instructions, and positive stimulation. At the start of a session, the participants were called to one of the three areas of the room from which they had to take objects. The calls served as encouragements as well as spatial cues that would help the participants to orient to that area and reach it and were emitted by the mini speaker available in that area. As they reached that area (i.e., were detected by the motion sensor available there), they received praise and the instruction to take an object. The instruction was then followed by the activation of the mini speaker available at the central desk, which called the participants to the desk. As they reached the desk (i.e., were detected by the motion sensor available there), the speaker on that desk delivered praise, the instruction to put away the object transported, and 15 s of preferred stimulation.
At the end of the stimulation, the mini speaker of the next area to be reached started calling the participants. The process was repeated for each of the other objects to be collected and transported, and a session lasted until all the objects available (i.e., 18 in total) had been transported to the central desk or a 30 min period had elapsed, whichever came first. The results showed that the participants were able to transport and put away between 13 and 18 objects per session during the intervention sessions. Their mean frequency was zero or near zero before the intervention.
Lancioni et al. [
30] designed a program that involved the use of a barcode reader, a series of barcodes, a smartphone fitted with a special application, and a mini speaker or headphones. The technology served to enable seven participants to find different room entrances distributed along the two sides of a corridor and deliver objects at those rooms. Each session included seven different trials. At each trial, the participants were to walk to a specific room and enter the room with the object they had to deliver, and then they would receive 20 s of preferred stimulation. A trial started with the research assistants guiding the participants to a specific position of the corridor, providing them with an object that they were to transport to one of the rooms, and typing the number of the destination room into the smartphone. The room entrances were marked with barcodes reproduced on sheets of paper. Those barcodes could be decoded by a small barcode reader that the participants wore at their ankle or waist. Based on the barcodes decoded, the smartphone provided the participants with different verbal messages, which were delivered via the mini speaker or the headphones the participants had. The message would invite the participants to walk forward (when the barcode detected indicated that the entrance did not correspond to the destination where the object was to be delivered) or stop and enter the room (when the barcode detected indicated that the entrance was that of the destination room). The results showed that the mean frequency of trials correctly completed (with the participants entering the right room) per session varied from about six to nearly seven during the intervention with the technology, while it was between zero and two before the intervention.
1.3. Objectives
The aim of the present study was to extend the scope of Lancioni et al.’s intervention programs [
29,
30], which are summarized above in several ways. First, this study aimed to enable participants to collect boxes containing different sets of objects from a storage room and transport them to five different destination rooms, thus expanding the activity context used by Lancioni et al. [
29]. Second, the boxes were to be transported to the pertinent destination rooms, that is, to the rooms that were connected to the objects the boxes contained. For example, a box containing soap and grooming items was to be transported to a washroom, whereas a box with food and drink items was to be transported to the room used as a snack area. This new activity arrangement (supplying different rooms with different/appropriate types of material) was thought to have practical and vocational relevance [
2,
8,
21]). Third, the technology system used during the study, which included tags with radio frequency identification codes, a tag reader, a smartphone, and mini speakers, was set to guide the participants to the different pertinent rooms automatically throughout the entire activity session (i.e., without any need for research assistants’ inputs, such as those scheduled by Lancioni et al. [
30]). These three new aspects were thought to make the intervention program set up in the present study more relevant from a rehabilitation standpoint and more functional and convenient from a technological standpoint than previous programs. The study included seven participants with intellectual disabilities and blindness and relied on a single-case research methodology.
2. Materials and Methods
2.1. Participants
Table 1 lists the seven participants by using their pseudonyms and reports their chronological ages and their age equivalents for daily living skills (personal subdomain), which were computed via the second edition of the Vineland Adaptive Behavior Scales [
31,
32]. Their chronological age ranged from 25 to 45 years. Their Vineland age equivalents ranged from 2 years and 8 months to 4 years. All the participants were diagnosed with congenital encephalopathy associated with intellectual disability and blindness. The seventh participant (Edgar) also presented with ambulation difficulties. Specifically, he walked when he had some form of physical support. For example, he could walk and transport objects by using a shopping cart (see below). No Intelligence Quotient scores were available for the participants, but the psychological services of the rehabilitation and care contexts that they attended considered their intellectual disability level to fall within the moderate-to-severe range (Eloise) or the severe range (all the others).
The participants represented a convenience sample, in that they were recruited from rehabilitation and care centers belonging to a single organization [
33]. Their recruitment, however, was carried out based on a number of conditions, which had been verified through preliminary observations and interviews. First, they were adults who needed to increase their levels of mobility and occupational engagement (the functional use of objects). Second, they had difficulties orienting and traveling in indoor contexts and were totally dependent when in outdoor contexts. Third, they were able to orient to sound cues (i.e., voices or other types of sounds) and could reach the sound source and the destination it represented within relatively small indoor contexts. Fourth, they could respond to simple verbal instructions concerning the use of objects such as “take” and “put away” the object. Fifth, they were interested in various forms of environmental stimulation (e.g., music and songs), so such stimulation was considered important to motivate their activity engagement (e.g., collecting and transporting boxes with objects). Sixth, staff personnel considered the use of technology support to promote mobility and occupational engagement a valuable objective and thus endorsed the study.
2.2. Ethical Considerations
The participants’ regular staff viewed the study as a positive opportunity for the participants. In fact, the study was deemed to offer the participants the chance to increase their mobility and occupational engagement, as well as their access to preferred stimulation. This access was expected to motivate their involvement and make it enjoyable for them. Given their condition, they could not provide a clear/reliable response as to their interest in the study or read and sign a consent form for it. In view of that, the participants’ legal representatives read and signed the consent form on their behalf. This study complied with the 1964 Helsinki Declaration and its later amendments and was approved by an institutional Ethics Committee.
2.3. Setting, Responses, Sessions, Instruction Cues, Research Assistants, and Stimuli
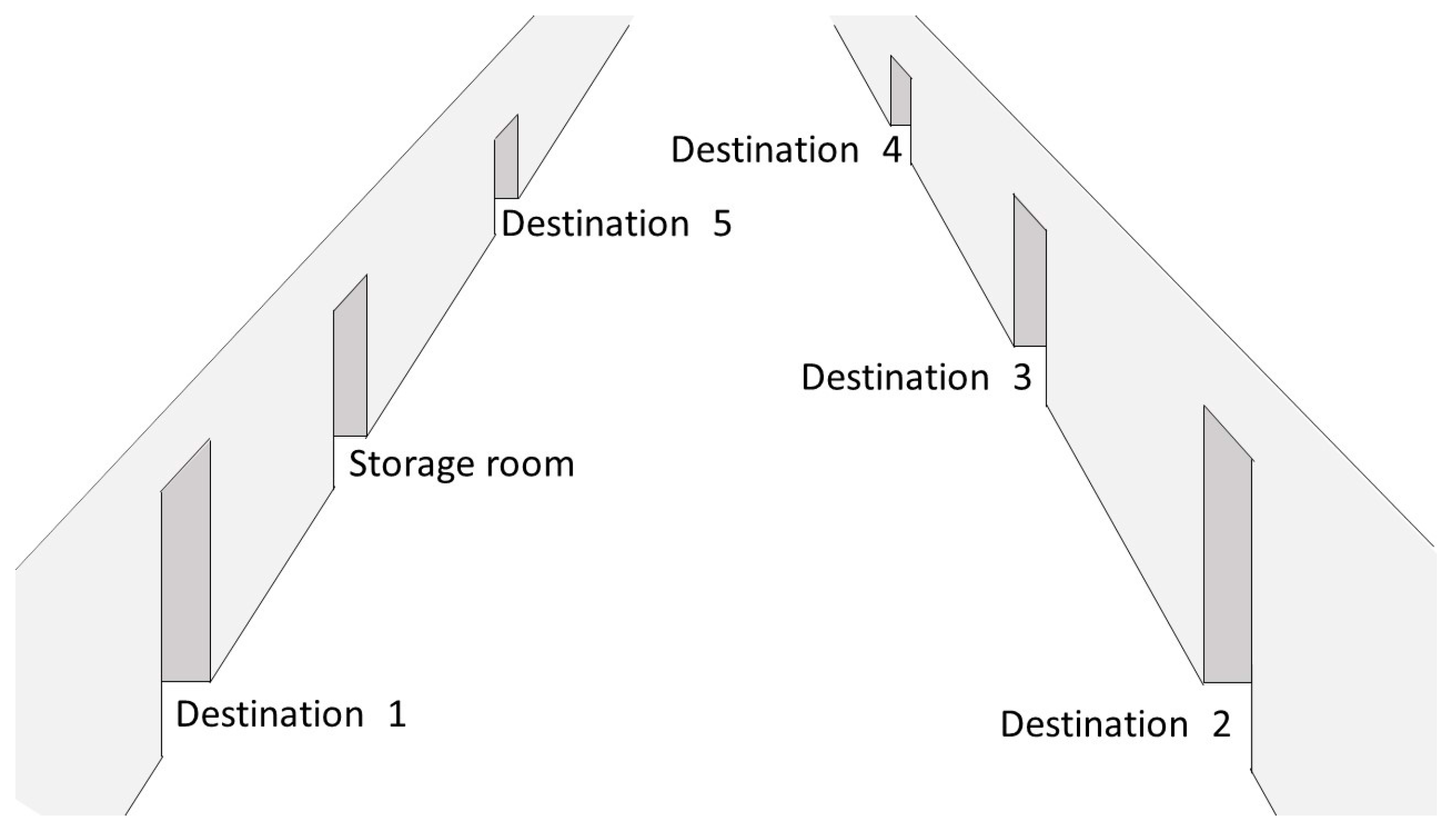
The setting was an area of the centers that the participants attended, which involved a corridor with room entrances on both sides. In total, six rooms were included: one serving as storage room and the others as destination rooms (see
Figure 1). The storage room contained a desk with 15 different boxes of 25 × 19 × 17 cm. Each box contained specific objects (e.g., toilet, food, or cleaning items). Each of the destination rooms had a large carton (placed on a chair) right after its entrance. A response consisted of taking one of the boxes from the storage room, transporting the box to the pertinent destination room, and depositing the box in the carton displayed in that room. For example, boxes containing grooming items were to be transported to a washroom and deposited in the carton available there, while boxes containing leisure items were to be transported to a room used as leisure area and deposited in the carton of that room (see the Introduction). A session lasted until the participants had transported all the 15 boxes available on the desk of the storage room, a 20 min period had elapsed, or several instances of research assistants’ guidance had occurred (see the Baseline for the First Six Participants Section). The participants typically had one session per day, 3 to 6 days a week.
The instruction cues consisted of single words or combinations of two or three words presented by the technology system during the intervention sessions. Specifically, the cues included expressions such as the following: (a) “Come here” and “Take a box”, which were presented from the desk with the boxes at intervals of about 5–7 s every time the participants were to go to such desk and collect a box; (b) “NAME plus walk”, or “Over here”, which was presented from the room where the box that the participants had collected was to be transported; and (c) “Box down” or “Box in carton”, which was presented when the participants were to deposit the transported box into the carton.
Four research assistants (two women and two men) were employed to implement the sessions and record the data. They held a university degree in psychology and were familiar with different data recording procedures and the technology systems/solutions employed with people with different types of disabilities.
The stimuli provided to the participants in connection with their depositing a box in a carton included music and song segments combined with verbal approval. The music and song stimuli were selected through a stimulus preference screening procedure. The procedure involved the presentation of two or three 10 s clips of each song or music piece included in the preference evaluation for a minimum of 10 non-consecutive times distributed over different evaluation periods. Stimuli were selected for use during the intervention phase of the study if the research assistants involved in the screening agreed that they had elicited the participants’ positive reactions (e.g., alerting and smiling) in at least 50% of their presentations.
2.4. Technology System for the First Six Participants
The technology system used for the first six participants (i.e., Dean, Ryan, Ruth, Eloise, Graham, and George) included (a) tags with radio frequency identification codes suitable for NFC; (b) a tag reader; (c) an Android smartphone with a light sensor, which was equipped with the Talking Hands application [
34] and the MacroDroid application; and (d) six mini speakers. The smartphone was fixed at the participants’ waist. The mini speakers were displayed in the storage room and the five destination rooms (one speaker per room).
The tags (5.4 × 8.5 × 0.1 cm; NFC MIFARE RFID, 1 K 13.56 MHz) were fixed onto the sides of the boxes that the participants were to transport and deposit in the cartons available in the destination rooms. All the tags attached to a specific box had the same code, which could be easily identified by the tag reader.
The tag reader consisted of two watch-like devices linked to one another. During the intervention (i.e., when the technology system was used), one of the devices (4.5 × 4.5 × 0.9 cm) was strapped to the palm of the participants’ right hand (see
Figure 2) and contained an NFC module which was designed to identify the tags attached to the different boxes with objects. The other device (6.5 × 4 × 1.5 cm) was strapped to the participants’ right wrist and contained an electronic circuit that was designed to send the smartphone Bluetooth signals about the tags identified.
At the start of each session, the participants were called to take a box by the mini speaker of the storage room (see
Figure 3). When the participants collected a box, their tag reader identified the box’s tags and sent a Bluetooth signal to the smartphone. The smartphone decoded the Bluetooth signal through the Talking Hands application. Decoding a Bluetooth signal (recognizing the tags’ code for the box being collected) led to the activation of the MacroDroid application, which (a) triggered the mini speaker of the room to which the box was to be transported and (b) ensured that the mini speaker presented the participants with the instructions to reach that room. The instructions (i.e., verbal encouragements to reach the room that were repeated every 5–7 s; see
Section 2.3 also provided orientation and spatial guidance for the participants traveling to the room.
Once the participants entered the room and approached the carton where the box was to be deposited, the smartphone’s light sensor detected a light change (i.e., a reduction in light intensity caused by the smartphone’s proximity to the carton; see
Figure 4). Based on this change, the MacroDroid caused the mini speaker available in the area to deliver (a) the instruction to deposit the box in the carton and (b) (3–4 s thereafter) 20 s of preferred music stimulation. Once the stimulation was over, the MacroDroid triggered the mini speaker of the storage room to present the instructions to reach the desk and take a box (see
Section 2.3). The box was then to be transported to the pertinent destination room following the procedure described above. The same procedure was applied to each box to be collected, transported, and deposited during the session.
2.5. Technology System for the Seventh Participant
The technology system used for the seventh participant (i.e., Edgar) included the same components as the system used for the first six participants. Yet, the position and functioning of some of those components differed as Edgar walked with the support of a shopping cart and used the cart for transporting the boxes (see the Participants Section). The cart was adapted so that (a) only a small sector of it (i.e., the one close to the handle) was open and accessible for placing the boxes (see
Figure 5) and (b) the tag reader and the smartphone were fixed at the bottom of that sector (see
Figure 5).
As soon as Edgar placed a box in the cart, the tag reader would identify the tags attached to the box and send a signal to the smartphone. The smartphone decoded the signal and activated (via the MacroDroid) the mini speaker of the destination room where the box was to be transported and deposited. The mini speaker presented encouragement (orientation) messages, as it had done for the other participants. Once in the room, he was to take the box from the cart, causing a change for the smartphone’s light sensor. This change led the MacroDroid to trigger the emission of the instruction to put the box in the carton. About 5 s after this instruction, a 20 s presentation of preferred music started. The end of the music led to the instructions to reach the storage room and take a box. The same process was followed for the other boxes to be used during the session.
2.6. Data Recording
Data recording concerned (a) the number of boxes correctly handled (i.e., collected, transported, and placed in the carton of the right destination room, independently of any research assistants’ guidance), (b) the research assistants’ guidance instances, and (c) the length of the sessions. The measures were recorded by the research assistants implementing the sessions. Inter-rater agreement was assessed in more than 23% of the sessions of the single participants, with a reliability observer watching those sessions and scoring the measures. The percentage of agreement (computed by dividing the number of sessions in which both the research assistants and the reliability observer had the same scores for the boxes being correctly handled and for the research assistants’ guidance, with differences of less than 1.5 min for the session lengths, by the total number of sessions carried out with the reliability observer and then multiplying by 100%) was above 93% for all the participants.
2.7. Experimental Conditions and Data Analysis
The first six participants (Dean, Ryan, Ruth, Eloise, Graham, and George) were exposed to the study according to a non-concurrent multiple baseline design across participants [
35]. During the initial phase of the study, they received baseline sessions in which the technology system was not in use. The number of baseline sessions differed across them, as required by the design. The baseline phase was followed by an intervention phase, during which the technology system was available (see below). For the seventh participant (Edgar), the study was carried out according to an ABAB design [
35], in which A represented baseline conditions (without the system), and B represented intervention conditions (with the system).
The research assistants were in charge of the baseline and intervention sessions of all the participants. To ensure that the sessions were implemented accurately (i.e., to ensure a high level of procedural fidelity [
36]), the research assistants were provided with (a) three or four preliminary practice sessions to familiarize them with the baseline and intervention conditions and (b) feedback on whether or not they had been procedurally accurate after regular sessions. Feedback was provided by a study supervisor who had access to videos of the sessions.
The participants’ frequency of boxes correctly handled during the baseline and intervention sessions was summarized in graphic form. The difference between the baseline and the intervention frequency levels was assessed through the Percentage of Nonoverlapping Data (PND) method [
37]. This method, which is a practical tool for the evaluation of single-case research data, allowed us to verify for each participant the percentage of intervention sessions in which the frequency of boxes correctly handled was higher than the highest baseline value.
2.7.1. Baseline for the First Six Participants
The baseline phase included 5 to 10 sessions during which the system was not available. Familiar objects were attached to the boxes to be transported and to the doorframes of the rooms to which those boxes were to be transported. For example, a toothpaste tube would be attached to the boxes that were to be transported to the washroom as well as to the doorframe of that room. At the start of a session, the participants were guided to touch the objects on the doorframes. Then, they were instructed to (a) take a box, (b) touch the object attached to the box (e.g., a cup), and (c) find (enter) the room with the cup.
If the participants transported the box to the correct room destination and deposited that in the carton available there, the research assistants provided verbal praise, guided the participants to the desk with the boxes, and instructed them to take a box. If the participants failed to make any progress toward the destination for 30–60 s or entered a wrong destination room, the research assistants provided verbal and physical guidance to help them find the correct room and deposit the box in the carton available there. Depositing the box in the carton led to verbal praise even when the response was carried out with the research assistants’ guidance. The session lasted until the participants had transported all the 15 boxes available, a 20 min time period had elapsed, or research assistants’ guidance had occurred on four consecutive boxes, whichever came first.
2.7.2. Intervention for the First Six Participants
The intervention included 59 to 78 sessions, with differences in the number of sessions being largely due to the participants’ availability. The technology system was in use and worked as described in the Technology System Section and summarized in
Figure 3. The research assistants provided guidance only if the participants failed to make progress for over 60 s. The intervention sessions were preceded by four to seven familiarization (practice) sessions, during which the research assistants’ guidance was available to help the participants respond to the system instructions without hesitation or breaks and experience the system praise and music.
2.7.3. Baseline for the Seventh Participant
Each of the two baseline (A) phases available for Edgar included six sessions. The conditions were as those described for the first six participants, except that he was to place the boxes in the cart and walk with the cart to the destinations.
2.7.4. Intervention for the Seventh Participant
The two intervention (B) phases available included 29 and 51 sessions, respectively. During those sessions, Edgar was provided with the technology system that worked as described in the technology system section concerning him. The first intervention phase was preceded by eight familiarization (practice) sessions, which were similar to those described for the first six participants.
3. Results
The six graphs of
Figure 6 report the baseline and intervention data for the first six participants. Each data point represents the mean frequency of boxes correctly handled per session over a block of two sessions. Blocks of three sessions (at the end of the baseline or intervention phases) are marked with an arrow. The graphs do not report the introduction (practice) sessions preceding the start of the intervention phase.
Figure 7 reports the baseline and intervention data for Edgar, which are plotted as in
Figure 6.
Figure 6 shows that only two of the first six participants, namely Eloise and George, managed to handle some of the boxes correctly (i.e., totals of 2 and 4, respectively) during the baseline sessions. Given the participants’ difficulties, research assistants’ guidance was regularly required, and all the participants’ baseline sessions were interrupted following four consecutive instances of research assistants’ guidance. The length of those sessions was below 10 min.
During the intervention phase, all the participants showed a clear performance improvement. Eloise, Graham, and George were able to correctly handle nearly all the boxes available in the sessions (i.e., their mean frequency of boxes correctly handled per session was about or above 14.5). Their mean session length was about 16.5, close to 20, and 18 min, respectively. Ruth’s mean frequency of boxes correctly handled per session was about 13.5. In some sessions, she managed to handle all 15 boxes correctly within the 20 min allowed. In most of the sessions, however, she would handle between 12 and 14 boxes. Ryan and Dean’s mean frequency of boxes correctly handled per session was about 9 and 12, respectively. Their sessions always ended after the 20 min time limit had elapsed. Research assistants’ guidance was virtually absent or very sporadic for all six participants. In fact, the discrepancies in their data reflected their differences in performance speed and dexterity more than their level of independence, which was high for all of them. The PND method showed indices of 1 for all the participants, given that their frequency of boxes correctly handled during the intervention sessions was always higher than their baseline best performance.
Edgar did not manage to handle any box correctly during the baseline phases (see
Figure 7), and the sessions were interrupted after four consecutive instances of research assistants’ guidance. During the first intervention phase, his mean frequency of boxes handled correctly was about 7 per session. During the second intervention phase, the mean frequency was about 8.5 per session. The sessions were always ended after the 20 min limit had elapsed. Research assistants’ guidance occurred on a few occasions during the initial sessions of the first intervention phase and then became highly sporadic and virtually absent. His relatively low frequency of boxes handled correctly was largely due to the fact that he was rather slow in taking and putting away boxes and also in his walking with the shopping cart. The PND index for him was 1 as it was for the previous participants.
4. Discussion
The results show that the seven participants succeeded in correctly collecting, transporting, and depositing boxes with objects within an activity context that included six different rooms (i.e., a storage room and five destination rooms). These data expand upon previous evidence in this area, in that the participants managed to carry out their activity engagement (a) using a relatively large and articulated activity context, (b) delivering the material (boxes) by transporting it to the pertinent destination rooms [
20,
29,
30], and (c) relying on a technology system that did not require research assistants’ input throughout the sessions [
30]. In light of the new evidence/findings, several considerations may be in order.
First, enabling people to transport boxes with different objects to the pertinent destination rooms might be seen as an important achievement that could have practical and vocational implications. In fact, one might envisage the use of activities such as supplying different rooms with different/appropriate types of material as viable within domestic and vocational (supported employment) contexts [
38,
39,
40]. The possibility of being successfully involved in those forms of activity independently of staff could thus represent a new perspective for people’s futures with expectedly positive consequences for their developmental and social progress and for their quality of life [
6,
41,
42,
43,
44,
45].
Second, the technology system used in the study was accurate in discriminating the boxes with the different objects and activating the encouragement and orientation cues of the rooms where those objects were to be transported and deposited. This role of the technology can be considered crucial to support the performance of people with intellectual and visual disabilities who are unlikely to discriminate many of the objects to be transported and to find the appropriate rooms for them [
46,
47,
48]. In practice, the technology may be seen as a necessary instrument (a prosthetic means) to help people progress from simply transporting objects to some general destination to distributing them accurately across different (pertinent) destination areas. Using such a prosthetic means in daily contexts would appear to be a realistic prospect.
Third, fixing tags onto the boxes ensured that there was no need to manipulate (attach tags to) the single objects to be transported. This approach was viewed as (a) a practical solution, given that not all objects could be easily fitted with tags (e.g., it could be rather difficult to fit a toothpaste tube or a toothbrush with a tag given the shape and dimensions of the tags), and (b) a time-saving strategy, given that fitting all objects with tags would require a considerable time investment in addition to interfering with the normal use of the objects within the context. Using the boxes was convenient because they allowed the participants to transport several objects at a time. Moreover, the boxes could be recovered after their use and employed across sessions without any additional preparation work or any waste of the tags that were pasted on them.
Fourth, the tag reader used in this study was divided into two sections that were designed to be relatively small so that the participants could wear them without a negative impact on their handling of the boxes [
47,
48,
49]. A wearable tag reader that automatically proceeds to the identification of the boxes’ tags and thus automatically triggers the presentation of instructions and orientation cues may be considered essential for a successful outcome with people like the participants of this study (i.e., people who could have omissions and failures if required to bring a tag reader in contact with the boxes right after collecting them [
46,
48,
50,
51].
Fifth, the participants of this study did not have problems wearing the tag reader’s components inside their hand and on their wrist. For people who would have problems in doing so, one could find a different position for the tag reader. For example, one could fix it onto the participant’s chest. This position would allow the boxes being collected to touch or come close to the tag reader, thus allowing it to identify their tags and consequently activate the presentation of instructions and orientation cues. To ensure the reliable contact (or near contact) of the boxes with the tag reader, one might use boxes larger than those included in this study.
Sixth, while the technology system employed in this study is not a commercially available package, several of its components, such as the smartphone, the mini speakers, and the MacroDroid, are easily accessible and inexpensive, so anyone can purchase them. With regard to the tag reader, it is important to clarify that (a) one of its sections concerns an NFC module that can be readily acquired commercially, and (b) the other section concerns an electronic unit, the design of which can be freely obtained from the authors.
Limitations and Future Research
The main limitations of the study concern the lack of maintenance and generalization data and the lack of assessment of participants’ satisfaction and social validation. To counter the first limitation, new studies will have to include follow-up checks to determine performance maintenance over time and also extend the evaluation of the system impact to new settings so as to verify generalization effects (i.e., ascertain whether the system can support the participants’ performance within settings not directly involved in the intervention) [
52,
53,
54].
To counter the second limitation, new studies will need to include an evaluation of participants’ satisfaction as part of the assessment process. One of the possible ways to check participants’ satisfaction with the sessions could involve the measurement of their indices of happiness (e.g., smiles and other facial or bodily expressions typically associated with happiness) during the sessions with the system and during other (daily) occupational situations [
55,
56]. A difference in the favor of the sessions would suggest that the participants may have a higher level of satisfaction within those sessions than within conventional occupational situations. A second way to check participants’ satisfaction with the sessions may involve the presentation of choice situations in which one of the options is a session with the system and the other option is a daily activity [
57,
58]. Preference for the session could be taken to suggest that the participants find the sessions more satisfactory than daily activities.
To counter the third limitation, one could apply a social validation procedure in which staff personnel are first asked to watch videos reporting clips of the sessions with the system and then interviewed as to the effectiveness, friendliness, and applicability of the system and the practical/vocational relevance of the participants’ performance [
59,
60]. The interview could also include the use of a conventional questionnaire, such as The System Usability Scale [
61,
62].
The small number of participants involved might be considered another limitation of this study. In relation to this point, one could make two statements. First, the single-subject research designs used for evaluating the impact of the system appear adequate to support the internal validity of the data reported [
63,
64]. Second, to determine the external validity of such data, one could rely on single-case replication studies, as well as studies involving both treatment and control groups [
65,
66].
5. Conclusions
In conclusion, the results show that participants with moderate-to-severe or severe intellectual disabilities and blindness managed to use the technology system to correctly collect, transport, and deposit boxes with objects within an activity context that included six different rooms (i.e., a storage room and five destination rooms). These results, which expand upon previous evidence in the area, appear very encouraging as to the possibility of offering people with significant intellectual disabilities and blindness new occupational opportunities with the potential of being vocationally relevant. Even so, caution is required in drawing conclusions about the robustness and general implications of the findings given the limitations of the study that new research needs to address. New research may also aim to upgrade the technology system so as to make it more easily usable across people and settings.
Author Contributions
Conceptualization, G.E.L.; data curation, G.E.L., G.A., and F.A.; formal analysis, G.E.L., F.P., N.N.S., M.F.O., and J.S.; investigation, G.E.L., G.A., and F.A.; methodology, G.E.L., G.A., F.P., F.A., N.N.S., M.F.O., and J.S.; software, F.P.; validation, G.E.L., G.A., N.N.S., M.F.O., and J.S.; writing—original draft, G.E.L.; writing—review and editing, G.A., F.P., F.A., N.N.S., M.F.O., and J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Ethics Committee of the Lega F. D’Oro, Osimo (AN), Italy (P090220244). All the procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Given their intellectual and visual disabilities, the participants could not provide a clear/reliable response as to their interest in the study or read and sign a consent form for it. In view of that, the participants’ legal representatives provided written informed consent on their behalf.
Data Availability Statement
The original data contributions presented in the study are reproduced in the graphs of
Figure 6 and
Figure 7. Datasets are available from the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest. The third author, who developed the tag reader used in this study, makes the design of the reader’s electronic circuit available at no cost.
Abbreviations
The following abbreviations are used in this manuscript:
| NFC | Near Field Communication |
| PND | Percentage of Nonoverlapping Data |
References
- Chang, Y.J.; Wang, T.Y. Indoor wayfinding based on wireless sensor networks for individuals with multiple special needs. Cybern. Syst. 2010, 41, 317–333. [Google Scholar] [CrossRef]
- Dijkhuizen, A.; Hilgenkamp, T.I.; Krijnen, W.P.; van der Schans, C.P.; Waninge, A. The impact of visual impairment on the ability to perform activities of daily living for persons with severe/profound intellectual disability. Res. Dev. Disabil. 2016, 48, 35–42. [Google Scholar] [CrossRef]
- Fellinger, J. Intellectual disability and sensory impairment. In Textbook of Psychiatry for Intellectual Disability and Autism Spectrum Disorder; Bertelli, M.O., Deb, S., Munir, K., Hassiotis, A., Salvador-Carulla, L., Eds.; Springer: New York, NY, USA, 2022; pp. 849–867. [Google Scholar] [CrossRef]
- Jarjoura, W. Disorientation and loss of wayfinding in individuals with congenital blindness and other affecting comorbidities. Brit. J. Vis. Impair. 2019, 37, 240–247. [Google Scholar] [CrossRef]
- Cuturi, L.F.; Aggius-Vella, E.; Campus, C.; Parmiggiani, A.; Gori, M. From science to technology: Orientation and mobility in blind children and adults. Neurosci. Biobehav. Rev. 2016, 71, 240–251. [Google Scholar] [CrossRef]
- Enkelaar, L.; Oosterom-Calo, R.; Zhou, D.; Nijhof, N.; Barakova, E.; Sterkenburg, P. The LEDs move pilot study: The Light Curtain and physical activity and well-being among people with visual and intellectual disabilities. J. Intellect. Disabil. Res. 2021, 65, 971–988. [Google Scholar] [CrossRef]
- Hanzen, G.; Waninge, A.; Vlaskamp, C.; van Nispen, R.M.; van der Putten, A.A. Participation of adults with visual and severe or profound intellectual disabilities: Analysis of individual support plans. Res. Dev. Disabil. 2018, 83, 132–141. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Campodonico, F.; Zimbaro, C.; Alberti, G.; Trubia, G.; Zagaria, T. Helping people with multiple disabilities manage an assembly task and mobility via technology-regulated sequence cues and contingent stimulation. Life Span. Disabil. 2018, 21, 143–163. [Google Scholar]
- Nair, V.; Olmschenk, G.; Seiple, W.H.; Zhu, Z. ASSIST: Evaluating the usability and performance of an indoor navigation assistant for blind and visually impaired people. Assist. Technol. 2022, 34, 289–299. [Google Scholar] [CrossRef]
- Parker, A. Considering a practical orientation and mobility framework to design communication interventions for people with visual impairments, deafblindness, and multiple disabilities. Perspect. ASHA Spec. Interest. Groups. 2017, 2, 89. [Google Scholar] [CrossRef]
- Desideri, L.; Lancioni, G.; Malavasi, M.; Gherardini, A.; Cesario, L. Step-instruction technology to help people with intellectual and other disabilities perform multistep tasks: A literature review. J. Dev. Phys. Disabil. 2021, 33, 857–886. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Alberti, G.; Filippini, C.; Fiore, A.; Simonetti, C.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J. Interactive technology to help people with multiple disabilities practice relevant physical responses within an occupational task. OBM Neurobiol. 2024, 8, 1–15. [Google Scholar] [CrossRef]
- Brock, M.E.; Schaefer, J.M.; Seaman, R.L. Self-determination and agency for all: Supporting students with severe disabilities. Theory Pract. 2020, 59, 162–171. [Google Scholar] [CrossRef]
- Gkora, V.; Karabatzaki, Z. Motivation in learning disabilities and the impact of ICTs. TechHub J. 2023, 3, 14–26. Available online: https://techhubresearch.com/index.php/journal/article/view/79 (accessed on 15 December 2024).
- Hutzler, Y.; Korsensky, O. Motivational correlates of physical activity in persons with an intellectual disability: A systematic literature review. J. Intellect. Disabil. Res. 2010, 54, 767–786. [Google Scholar] [CrossRef]
- Sahoo, S.; Choudhury, B. Exploring the use of computer vision in assistive technologies for individuals with disabilities: A review. J. Future Sustain. 2024, 4, 133–148. [Google Scholar] [CrossRef]
- Fernandes, H.; Costa, P.; Filipe, V.; Paredes, H.; Barroso, J. A review of assistive spatial orientation and navigation technologies for the visually impaired. Univ. Access Inf. Soc. 2019, 18, 155–168. [Google Scholar] [CrossRef]
- Kuriakose, B.; Shrestha, R.; Sandnes, F.E. Tools and technologies for blind and visually impaired navigation support: A review. IETE Tech. Rev. 2020, 39, 3–18. [Google Scholar] [CrossRef]
- Deverell, L.; Bhowmik, J.; Lau, B.T.; Al Mahmud, A.; Sukunesan, S.; Islam, F.M.A.; McCarthy, C.; Meyer, D. Use of technology by orientation and mobility professionals in Australia and Malaysia before COVID-19. Disabil. Rehabil. Assist. Technol. 2020, 17, 260–267. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Alberti, G.; Chiariello, V.; Abbatantuono, C.; Taurisano, P.; Desideri, L. Fostering functional occupation and mobility in people with intellectual disability and visual impairment through technology-aided support. Adv. Neurodev. Disord. 2023, 7, 392–402. [Google Scholar] [CrossRef]
- Manzoor, M.; Vimarlund, V. Digital technologies for social inclusion of individuals with disabilities. Health Technol. 2018, 8, 377–390. [Google Scholar] [CrossRef]
- Chavers, T.N.; Schlosser, R.W.; Cheng, C.; Koul, R. Effects of interventions involving speech output technologies on communication outcomes for individuals with developmental disabilities: A scoping review. Am. J. Speech-Lang. Pathol. 2022, 31, 2248–2267. [Google Scholar] [CrossRef] [PubMed]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Alberti, G.; Troccoli, O.; Orlando, I.; Ricci, C. Enabling people with intellectual and other disabilities to make verbal requests using cardboard chips with mini objects or pictures and a smartphone. Front. Rehabil. Sci. 2023, 4, 1257493. [Google Scholar] [CrossRef]
- Ripat, J.; Verdonck, M.; Gacek, C.; McNicol, S. A qualitative metasynthesis of the meaning of speech-generating devices for people with complex communication needs. Augment. Altern. Comm. 2018, 35, 69–79. [Google Scholar] [CrossRef]
- Burns, J.; Carter, A.; Draper, S.; Foad, A. Engaging and sustaining people with intellectual disabilities in physical activity: A narrative review of existing evidence. Int. J. Dev. Disabil. 2022, 70, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Hassan, N.M.; Landorf, K.B.; Shields, N.; Munteanu, S.E. Effectiveness of interventions to increase physical activity in individuals with intellectual disabilities: A systematic review of randomised controlled trials. J. Intellec. Disabil. Res. 2019, 63, 168–191. [Google Scholar] [CrossRef]
- Rotta, K.; Raaymakers, A.; Poling, A. Using positive reinforcement to increase the physical activity of individuals with developmental disabilities: A review. J. Dev. Phys. Disabil. 2023, 35, 551–575. [Google Scholar] [CrossRef]
- Savage, M.N.; Clark, T.A.; Baffoe, E.; Candelaria, A.E.; Aneke, L.; Gonzalez, R.; Al Enizi, A.; Anguita-Otero, M.; Edwards-Adams, K.; Grandberry, L.; et al. Technology-based physical health interventions for adults with intellectual disability: A scoping review. J. Dev. Phys. Disabil. 2024, 36, 757–792. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Alberti, G.; Chiariello, V.; Campodonico, F.; Desideri, L. Technology-aided spatial cues, instructions, and preferred stimulation for supporting people with intellectual and visual disabilities in their occupational engagement and mobility: Usability study. JMIR Rehabil. Assist. Technol. 2021, 8, e33481. [Google Scholar] [CrossRef]
- Lancioni, G.E.; Alberti, G.; Filippini, C.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Orlando, I.; Desideri, L. A technology system to help people with intellectual disability and blindness find room destinations during indoor traveling: Case series study. JMIR Rehabil. Assist. Technol. 2024, 11, e65680. [Google Scholar] [CrossRef]
- Balboni, G.; Belacchi, C.; Bonichini, S.; Coscarelli, A. Vineland Adaptive Behavior Scales, 2nd ed.; Vineland-II; Standardizzazione Italiana: Florence, Italy, 2016. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland Adaptive Behavior Scales, 2nd ed.; Vineland II; Pearson: New York, NY, USA, 2005. [Google Scholar]
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of convenience sampling and purposive sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef]
- Pezzuoli, F.; Corona, D.; Corradini, M.L. Improvements in a wearable device for sign language translation. In Advances in Human Factors in Wearable Technologies and Game Design; Ahram, T., Ed.; Advances in Intelligent Systems and Computing; Springer International Publishing: Champaign, IL, USA, 2020; Volume 973, pp. 70–81. [Google Scholar] [CrossRef]
- Ledford, J.R.; Gast, D.L. Single Case Research Methodology: Applications in Special Education and Behavioral Sciences, 3rd ed.; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Strain, P.; Fox, L.; Barton, E.E. On expanding the definition and use of procedural fidelity. Res. Pract. Pract. Pers. Sev. Disabil. 2021, 46, 173–183. [Google Scholar] [CrossRef]
- Parker, R.I.; Vannest, K.J.; Davis, J.L. Effect size in single-case research: A review of nine nonoverlap techniques. Behav. Modif. 2011, 35, 303–322. [Google Scholar] [CrossRef]
- Ashley, D.; Fossey, E.; Bigby, C. The home environments and occupational engagement of people with intellectual disabilities in supported living. Br. J. Occup. Ther. 2019, 82, 698–709. [Google Scholar] [CrossRef]
- Cannella-Malone, H.I.; Schaefer, J.M. A review of research on teaching people with significant disabilities vocational skills. Career Dev. Transit. Except. Individ. 2017, 40, 67–78. [Google Scholar] [CrossRef]
- Luthra, R. Young adults with intellectual disability who are not in employment, education, or daily activities: Family situation and its relation to occupational status. Cogent Soc. Sci. 2019, 5, 1622484. [Google Scholar] [CrossRef]
- Beadle-Brown, J.; Leigh, J.; Whelton, B.; Richardson, L.; Beecham, J.; Baumker, T.; Bradshaw, J. Quality of life and quality of support for people with severe intellectual disability and complex needs. J. Appl. Res. Intellect. Disabil. 2016, 29, 409–421. [Google Scholar] [CrossRef]
- Hobeika, L.; Ghilain, M.; Schiaratura, L.; Lesafre, M.; HuventGrelle, D.; Puisieux, F.; Samson, S. Socio-emotional and motor engagement during musical activities in older adults with major neurocognitive impairment. Sci. Rep. 2021, 11, 15291. [Google Scholar] [CrossRef]
- Kocman, A.; Weber, G. Job satisfaction, quality of work life and work motivation in employees with intellectual disability: A systematic review. J. Appl. Res. Intellect. Disabil. 2018, 31, 1–22. [Google Scholar] [CrossRef]
- Mumbard-Adam, C.; Vicente, E.; Balboni, G. Self-determination and quality of life of people with intellectual and developmental disabilities: Past, present, and future of close research paths. J. Policy Pract. Intellect. Disabil. 2024, 21, e12460. [Google Scholar] [CrossRef]
- Wehmeyer, M.L. The importance of self-determination to the quality of life of people with intellectual disability: A perspective. Int. J. Environ. Res. Public. Health. 2020, 17, 7121. [Google Scholar] [CrossRef]
- Evmenova, A.S.; Graff, H.J.; Genaro Motti, V.; Giwa-Lawal, K.; Zheng, H. Designing a wearable technology intervention to support young adults with intellectual and developmental disabilities in inclusive postsecondary academic environments. J. Spec. Educ. Technol. 2019, 34, 92–105. [Google Scholar] [CrossRef]
- Filippini, C.; Lancioni, G.E.; Alberti, G.; Pezzuoli, F.; Ceccarani, P. A technology aid to help people with blindness and moderate intellectual disability retrieve common objects from storage units: A proof-of-concept study. Sensors 2024, 24, 4453. [Google Scholar] [CrossRef] [PubMed]
- Abdi, S.; Kitsara, I.; Hawley, M.S.; de Witte, L.P. Emerging technologies and their potential for generating new assistive technologies. Assist. Technol. 2021, 33 (Suppl. S1), 17–26. [Google Scholar] [CrossRef]
- Nelson, E.C.; Sools, A.M.; Vollenbroek-Hutten, M.M.R.; Verhagen, T.; Noordzij, M.L. Embodiment of wearable technology: Qualitative longitudinal study. JMIR Mhealth Uhealth 2020, 8, e16973. [Google Scholar] [CrossRef]
- Johnson, K.R.; Blaskowitz, M.G.; Mahoney, W.J. Technology for adults with intellectual disability: Secondary analysis of a scoping review. Can. J. Occup. Ther. 2023, 90, 395–404. [Google Scholar] [CrossRef]
- Mishra, S.; Laplante-Lévesque, A.; Barbareschi, G.; Witte, L.D.; Abdi, S.; Spann, A.; Khasnabis, C.; Allen, M. Assistive technology needs, access and coverage, and related barriers and facilitators in the WHO European region: A scoping review. Disabil. Rehabil. Assist. Technol. 2024, 19, 474–485. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.O.; Heron, T.E.; Heward, W.L. Applied Behavior Analysis, 3rd ed.; Pearson: New York, NY, USA, 2019. [Google Scholar]
- Pennington, B.; Simacek, J.; McComas, J.; McMaster, K.; Elmquist, M. Maintenance and generalization in functional behavior assessment/behavior intervention plan literature. J. Behav. Educ. 2019, 28, 27–53. [Google Scholar] [CrossRef]
- Pierce, W.D.; Cheney, C.D. Behavior Analysis and Learning, 6th ed.; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Holyfield, C.; Lorah, E. Effects of high-tech versus low-tech AAC on indices of happiness for school-aged children with multiple disabilities. J. Dev. Phys. Disabil. 2022, 35, 209–225. [Google Scholar] [CrossRef]
- Ramey, D.; Healy, O.; McEnaney, E. Defining and measuring indices of happiness and unhappiness in children diagnosed with autism spectrum disorder. Behav. Anal. Pract. 2023, 16, 194–209. [Google Scholar] [CrossRef]
- Frounfelker, S.A.; Bartone, A. The importance of dignity and choice for people assessed as having intellectual disabilities. J. Intellect. Disabil. 2021, 25, 490–506. [Google Scholar] [CrossRef]
- Stancliffe, R.J.; Wehmeyer, M.L.; Shogren, K.A.; Abery, B.H. Choice, Preference, and Disability; Springer: New York, NY, USA, 2020. [Google Scholar]
- Stasolla, F.; Caffò, A.O.; Perilli, V.; Boccasini, A.; Damiani, R.; D’Amico, F. Assistive technology for promoting adaptive skills of children with cerebral palsy: Ten cases evaluation. Disabil. Rehabil. Assist. Technol. 2019, 14, 489–502. [Google Scholar] [CrossRef] [PubMed]
- Worthen, D.; Luiselli, J.K. Comparative effects and social validation of support strategies to promote mindfulness practices among high school students. Child. Fam. Behav. Ther. 2019, 41, 221–236. [Google Scholar] [CrossRef]
- Lewis, J.R. The System Usability Scale: Past, preset, and future. Int. J. Hum-Comp. Inter. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Borsci, S.; Federici, S.; Lauriola, M. On the dimensionality of the System Usability Scale: A test of alternative measurement models. Cogn. Process. 2009, 10, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Kazdin, A.E. Single-Case Research Designs: Methods for Clinical and Applied Settings, 3rd ed.; Oxford University Press: New York, NY, USA, 2020. [Google Scholar]
- Walker, S.G.; Carr, J.E. Generality of findings from single-case designs: It’s not all about the “N”. Behav. Anal. Pract. 2021, 14, 991–995. [Google Scholar] [CrossRef]
- Coiera, E.; Tong, H.L. Replication studies in the clinical decision support literature–frequency, fidelity, and impact. J. Am. Med. Inform. Assoc. 2021, 28, 1815–1825. [Google Scholar] [CrossRef]
- Tanious, R.; Manolov, R.; Onghena, P.; Vlaeyen, J.W.S. Single-case experimental designs: The importance of randomization and replication. Nat. Rev. Methods Primers 2024, 34, 100511. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}