
Indoor Environmental Monitoring and Chronic Respiratory Diseases: A Systematic Review

 ,
,  , and
, and 
Abstract

1. Introduction
- (a)
- The lack of methodological standardization in studies.
- (b)
- The need for long-term longitudinal trials that consider the spatial variability, individualized measures of exposure to pollutants, and the heterogeneity in demographic and health characteristics of patients.
- (c)
- The need for linking monitored air quality measurements with respiratory health markers collected from sensors, mobile applications, and the patient’s medical history.
- (d)
- The limited research studies focused on how the combination of indoor pollutants and the confounding factors beyond the isolated effects of each pollutant separately affect respiratory health, thus contributing to pro-inflammatory states and genetic and epigenetic alterations.
- (e)
- The lack of personalized early warning and recommendations systems that combine environmental monitoring with artificial intelligence techniques.
- (a)
- To determine peer-reviewed scientific studies that have been conducted on IAQ monitoring and its effect on the health of patients with asthma or COPD, and to create a synopsis of the empirical knowledge on this field to date.
- (b)
- To provide a focused understanding of the possibilities of monitoring IAQ to predict exacerbations in asthma and COPD and improve respiratory environmental health.
- (c)
- Identify action gaps in indoor monitoring air quality studies and possible actions to mitigate them.
2. Methods
2.1. Search Strategy and Inclusion and Exclusion Criteria
2.2. Data Extraction and Quality Assessment
2.3. Risk-of-Bias Assessment
3. Results
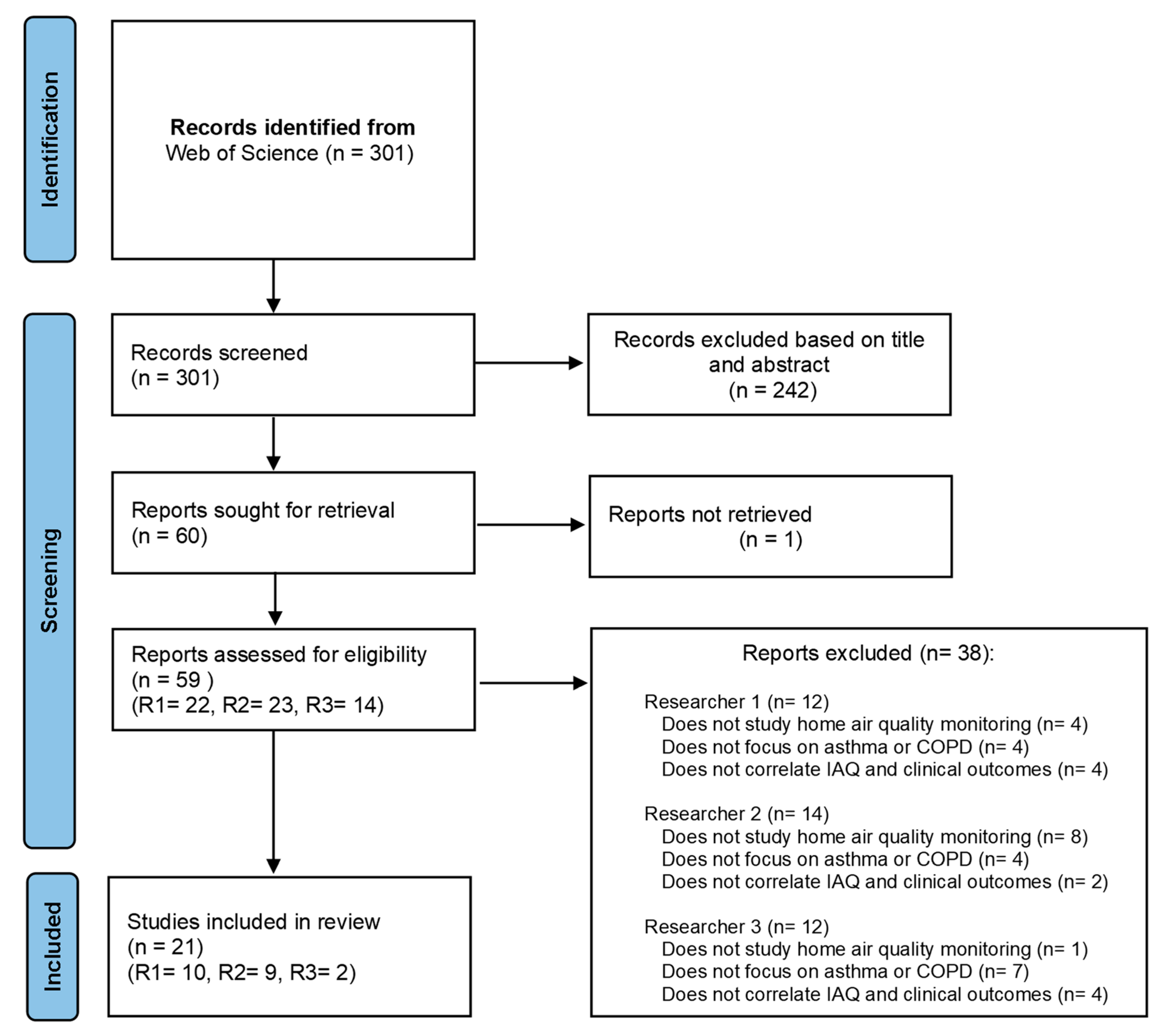
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Publication and Study Design Type

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Authors | Country | Disease | Study Design | Study Population | Objective |
|---|---|---|---|---|---|---|
| 2023 | J. Kang et al. [29] | South Korea | COPD | RCT | Adults | To assess the effectiveness of a behavioral intervention in reducing PM2.5 exposure and to improve clinical outcomes in patients with COPD. |
| 2023 | N. N. Hansel et al. [30] | USA | COPD | RCT | Adults | To determine whether placement of active portable HEPA cleaners can improve respiratory morbidity in former smokers. |
| 2023 | A. McCarron et al. [33]. | UK | Asthma | OCS | Adults | To investigate the acute effects of personal exposure to PM2.5 on self-reported asthma-related health. |
| 2023 | I. Kang et al. [35] | USA | Asthma | OCS | Adults | To examine the joint impacts of exposures to residential indoor and outdoor air pollutants and housing risk factors on asthma-related health outcomes. |
| 2022 | G. P. Bălă et al. [28] | Romania | COPD | OCS | Adults | To assess the degree of microparticulate pollution in the houses of COPD patients and to determine whether the values recorded correlate to COPD exacerbations. |
| 2022 | B. J. John et al. [22] | Germany | COPD | OCS | Adults | To identify the affected surroundings to take early steps to reduce the risk of COPD and other respiratory illnesses by introducing an AQI real-time device. |
| 2022 | U. Rabbani et al. [18] | Pakistan | Asthma | OCS | Adults | To assess the association of formaldehyde, CO, and PM2.5 with respiratory symptoms, asthma, and post-bronchodilator reversibility. |
| 2022 | J. Woo et al. [37] | South Korea | Asthma | RCT | Pediatric | To predict PEFR with a deep learning algorithm through RNNs and DNNs trained using 4 months of linked data of IAQ and PEFR. |
| 2022 | L. Nurhussien et al. [32] | USA | COPD | NRCT | Adults | To study how daily pollutant exposures impact lung function in COPD, considering the influence of eosinophil levels as indicators of airway inflammation and pollution susceptibility. |
| 2021 | H. Kim et al. [11] | South Korea | COPD | OCS | Adults | To assess if indoor particulate matter concentration is affected by a life behavior pattern, and if it can be reduced with appropriate lifestyle modification. |
| 2021 | C.T. Wu et al. [21] | Taiwan | COPD | OCS | Adults | To develop a prediction system using lifestyle data, environmental factors, and patient symptoms for the early detection of acute exacerbations of COPD in the upcoming 7 days. |
| 2021 | W.D. Bae et al. [17] | South Korea | Asthma | OCS | Adults | To compare ten machine-learning techniques, using imbalanced sampling to improve nine of them in predicting how IAQ affects patients’ PEFR. |
| 2021 | C.I. Prasasti et al. [34] | Indonesia | Asthma | OCS | Pediatric | To study how VOCs, PM2.5, and household environmental exposure relate to respiratory allergic symptoms in children in Surabaya, Indonesia. |
| 2021 | A.Y. Lim et al. [42] | South Korea | Asthma | OCS | Adults + Pediatric | To evaluate the IAQ level and daily health symptoms of adults and children living in EEHs compared to conventional buildings over one year. |
| 2020 | SE. Guo et al. [31] | Taiwan | COPD | NRCT | Adults | The study explored how educating patients with COPD about particulate matter (PM) affects their knowledge of air pollution prevention, self-care, symptom management, and indoor PM levels. |
| 2020 | E.N. Schachter et al. [36] | USA | Asthma | OCS | Pediatric | To study how indoor pollutants and their seasonal changes affect asthma exacerbations in children with moderate to severe asthma. |
| 2020 | R. J. Khusial et al. [38] | Netherlands, UK, Greece, and Germany | Asthma | RCT + OCS | Adults | To assess the clinical effectiveness and technology acceptance of myAirCoach-supported self-management on top of usual care in patients with asthma using inhalation medication. |
| 2020 | G. H. Lee et al. [39] | South Korea | Asthma | RCT | Pediatric | To study air purifiers’ impact on indoor air pollutant levels and asthma control in children, using HEPA filters. |
| 2020 | S. Kim et al. [40] | South Korea | Asthma | RCT | Pediatric | To evaluate the effects of indoor PM2.5 on children’s PEFR, with a daily intervention of air purifiers with filter on, compared with groups with filter off. |
| 2019 | R. Chi et al. [12] | China | COPD | OCS | Adults | To compare the effects of outdoor- and indoor-originated PM2.5 on cardiopulmonary function in COPD patients and healthy elderly adults. |
| 2019 | S. Hussain et al. [41] | UK | Asthma | OCS | Adults | To assess if overnight particulate matter exposure affects daily symptoms, lung function, and inflammation in asthmatic patients sensitive to dust mites. |
3.2.2. Subjects, Study Sample and Follow-Up Months
| Ref. | Clinical Data Gathered During the Study | Follow-Up | Study Sample (Subjects) | Results | MMAT Score |
|---|---|---|---|---|---|
| [29] | Questionnaires (SGRQ, CAT), exacerbations | 9 months | 106 | Good adherence to the intervention led to improved CAT scores and lower PM2.5 levels compared to poor adherence in the control group. Checking air quality forecasts regularly reduced CAT scores across all activities. | 100% |
| [30] | Questionnaires (SGRQ, CAT), scales (mMRC, BCSS), exacerbations, functional capacity (6 min walk test distance) | 6 months | 116 | The active filter group showed better SGRQ symptom scores, fewer respiratory symptoms, and lower rates of exacerbations and rescue medication use than the sham group. In the active group, a 30–40% reduction in NO2 and more than 40% in PM2.5 was observed. | 100% |
| [33] | Self-reported asthma symptoms, medication use | 12 months | 28 | PM2.5 levels varied by location. Higher PM2.5 exposure increased asthma symptom likelihood, but it did not affect reliever inhaler use. | 75% |
| [35] | Questionnaires (ACT, HRQoL SF-12), scale (PSS), hospitalizations and emergency department visits | 19 months | 53 | In both cross-sectional and longitudinal analyses, lower ACT scores correlated with higher indoor NO2 levels, indoor temperature, PM1, PM2.5, and PM10. Emergency department visits were linked to poorer asthma control, physical health, and mental health, as well as higher indoor NO2 ratios and temperatures. | 100% |
| [28] | Clinical data extracted from medical records, exacerbations | 8 months | 79 | Average PM1, PM2.5, and PM10 values were lower in the group of infrequently exacerbating patients than in the group of frequently exacerbating patients. | 100% |
| [22] | Questionnaire (RQ), lung function from medical records | 8 days | 196 | High daily PM2.5 levels, especially in smokers, significantly affected COPD patients’ health. Indoor PM2.5 levels were closely correlated with health conditions, emphasizing the impact of particulate exposure. | 50% |
| [18] | Questionnaire (ATS-DLD-78A), spirometry (FVC, FEV1) | 6 months | 1629 | Formaldehyde and CO levels were associated with cough, phlegm, and wheezing. PM2.5 levels were linked to shortness of breath and overall respiratory symptoms and were associated with a lower risk of cough, phlegm, and bronchitis. | 100% |
| [37] | PEFR | 4 months | 26 | The 10 min RNN model accurately predicted PEFR with an RMSE of 42.5 and MAPE of 14.0, showing how indoor PM2.5 levels impacted PEFR over time. | 75% |
| [32] | Questionnaire, spirometry (FVC, FEV1) | 4 months | 30 | Higher personal NO2 exposure was associated with lower FEV1 (11.3 mL) and lower forced vital capacity (18.0 mL). PM2.5 and NO2 exposure at personal and community levels were also linked to lower FEV1 in participants with higher eosinophil levels. | 100% |
| [11] | Questionnaire (inhaler use), exacerbations | 3 months | 104 | Indoor PM2.5 levels were influenced by lifestyle and economic status in COPD patients and were significantly linked to acute COPD exacerbations. | 75% |
| [21] | Questionnaire (CAT), scale (mMRC), physiological data, exacerbations | 4 months | 67 | The AECOPD predictive model achieved 92% accuracy, 94% sensitivity, and 90% specificity for 7-day predictions, with an AUC above 0.9. Results show lifestyle and environmental data are highly correlated with health conditions. | 100% |
| [17] | PEFR | 6 months | 25 | Transfer machine learning with imbalanced sampling effectively predicted changes in PEFR linked to IAQ, including PM2.5 and carbon dioxide concentrations. | 75% |
| [34] | Questionnaire | 3 months | 80 | The periodic monitoring of IAQ was found to be an effective measure to prevent respiratory allergies among children in an indoor environment. | 75% |
| [42] | Questionnaire, scale | 12 months | 25 adults + 25 children | Indoor PM10, PM2.5, CO2, and VOCs concentrations were lower in EEH. Seasonal adjustments showed consistent indoor temperature and humidity levels in EEH. | 75% |
| [31] | Questionnaire (CAT), scale (mMRC) | 6 months | 63 | PM education led to improved knowledge in the first and third months but not by the sixth month. The experimental group had greater gains initially, with better physical health in the first month, and better psychological health in the sixth month. | 50% |
| [36] | Questionnaire, medication use, unscheduled clinic, emergency department visits, hospitalizations, spirometry (FVC, FEV1) | 2 weeks | 36 | NO2 and PM2.5 elements like Ca, Si, Ni, and Cl were linked to worsened asthma symptoms and increased use of rescue medication in inner-city children with moderate to severe asthma. | 100% |
| [38] | Questionnaires (ACQ, m-AQLQ, EQ-5D-5L), exacerbations, PEFR (FEV1), FeNO, inhaler use and technique score. | Study 1: 3–6 months Study 2: 3 months | Study 1: 30 Study 2: 12 | In study 1, the intervention improved asthma control (ACQ difference 0.70) and reduced exacerbations (HR 0.31). Asthma-related quality of life also improved (mini AQLQ difference 0.53) but forced expiratory volume in 1 s did not change. In study 2, asthma control improved by 0.86 compared to baseline. | 100% |
| [39] | Questionnaire (based on TRACK), PEFR, FeNO | 2 months | 30 | Medication use decreased from 6.9 to 7.12 when using air purifiers, suggesting less medication was needed. Bacterial diversity, measured by the Chao 1 index, was lower with the air purifier on compared to off. | 75% |
| [40] | PEFR, FeNO | 1 month, 3 weeks | 26 | The use of in-home air filtration could be considered as an intervention strategy for IAQ control in asthmatic children’s homes. | 100% |
| [12] | Blood pressure, PEFR, FEV1 | 7 months | 43 | During the heating season, COPD patients had a reduction in forced expiratory volume in the first second (FEV1) associated with PM2.5 | 100% |
| [41] | Questionnaires (ACQ, AQLQ), PEFR, FeNO, spirometry | 3 months | 28 | No significant associations were observed between overnight particulate matter exposure and clinical outcomes measured daily or at study visits. | 100% |
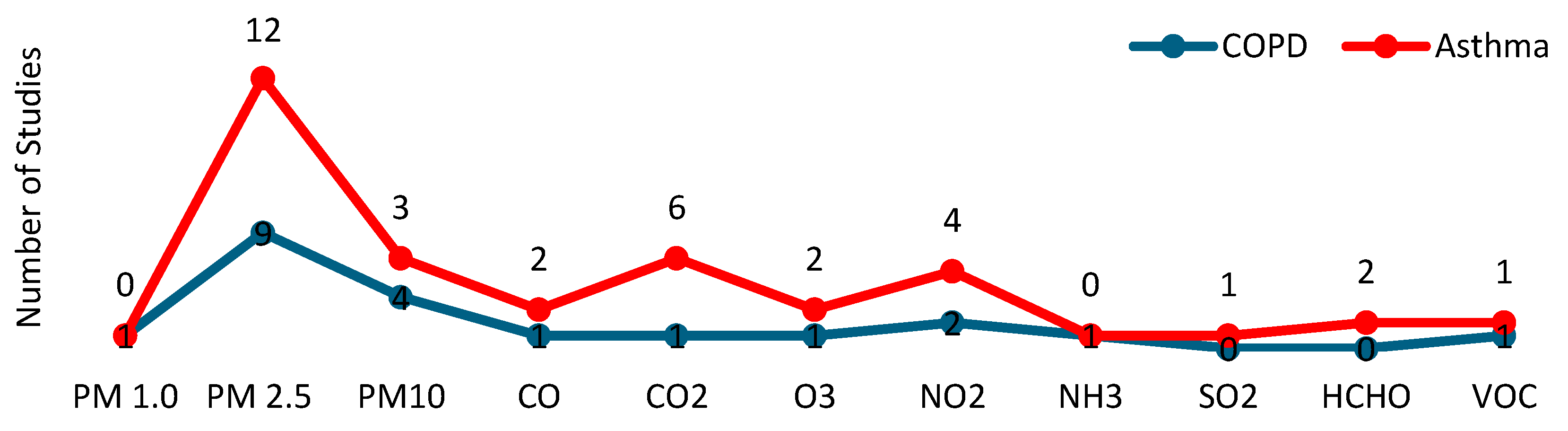
3.2.3. Pollutants
| Ref. | Pollutants | Sensors | Sensor Location | Calibration | Communications | Sampling | Time Series Processing | Predictive Model | Machine Learning |
|---|---|---|---|---|---|---|---|---|---|
| [29] | PM2.5 | Particle Sensor | Participants’ main area of activity | - | IoT | 1 sample/2 min | Mean ± standard deviation | Yes | No |
| [30] | PM2.5, PM10, NO2, airborne nicotine (VOC) | Particle Sensor, Gas Sensor | Participants’ main area of activity | - | Local Storage | 1 week in three periods: at months 0, 3, and 6. | - | No | No |
| [33] | PM2.5 | Air Quality Monitor | Backpack | Median values for calibration | Local Storage | 1 sample/2 min | Min, max, and mean values | Yes | No |
| [35] | HCHO, CO, CO2, NO2, O3, PM2.5 | Particle Sensor | Participants’ main area of activity | Quarterly colocation calibration | IoT | 1 sample/min | Mean ± standard deviation | No | No |
| [28] | PM1, PM2.5, and PM10 | Air Quality Monitor | Participants’ main area of activity | - | Wi-Fi | 1 sample/min | Min, max, and mean values | Yes | No |
| [22] | PM2.5, CO, CO2, NH3 | Particle Sensor, Gas Sensor, Air Quality Monitor | Participants’ main area of activity | - | Wi-Fi | 1 sample/2 min | Mean values | No | ✘ |
| [18] | HCHO, CO, NO2, PM2.5 | Air Quality Monitor, Particle Sensor | Living room, bedroom, and kitchen | - | Local Storage | 1 sample/5 min | Median values | No | ✘ |
| [37] | PM2.5, CO2 | Particle sensor, Gas Sensor | Bedrooms/living rooms | With a reference device | Local Storage | 1 sample/2 min | Mean values | Yes | Yes |
| [32] | PM2.5, NO2, O3 | Particle Sensor, Gas Sensor | Living room, bedroom, and kitchen | With a reference device | Local Storage | 3 samples/min | Mean ± standard deviation | No | No |
| [11] | PM2.5 | Particle Sensor | Center of the participants’ houses | - | IoT | 1 sample/2 min | Mean ± standard deviation | No | No |
| [21] | PM2.5 | Air Quality Monitor | Participants’ main area of activity | - | IoT | 1 sample/15 min | Mean values | Yes | Yes |
| [17] | PM2.5, CO2 | Particle Sensor, Gas Sensor | Outside, front door, living room, bedroom, and kitchen | - | Local Storage | 1 sample/2 min | Mean values | Yes | Yes |
| [34] | PM2.5 | Dust Sensor | Bedroom | Airflow calibrator | Local Storage | - | Min, max, and mean values | Yes | No |
| [42] | PM10, PM2.5, CO2, VOCs | Air Quality Monitor | Living room | - | IoT | 1 sample/5 min | Mean values | Yes | No |
| [31] | PM10, PM2.5, | Dust Sensor | Outside, front door, living room, bedroom, and kitchen | - | Local Storage | 3 samples/min | Mean ± standard deviation | Yes | No |
| [36] | PM10, PM2.5, NO2, SO2, O3 | Dust Sensor, Gas Sensor | Participants’ main area of activity | - | Local Storage | 3 samples/min | Odds ratios | No | No |
| [38] | NO2, SO2, PM2.5, PM10 | Air Quality Monitor | Bedrooms | - | Bluetooth | 1 sample/2 min | Mean ± standard deviation and median values | No | No |
| [39] | PM2.5, CO2 | Particle Sensor | Living room | - | IoT | 1 sample/2 min | Mean ± standard deviation | No | No |
| [40] | PM2.5, CO2 | Air Quality Monitor, Particle Sensor | Living room | Laboratory test | IoT | 1 sample/2 min | Median values | No | No |
| [12] | PM2.5 | Dust Sensor | Participants’ main area of activity | - | Local Storage | 3 samples/min | Mean ± standard deviation and median values | No | No |
| [41] | PM10, PM2.5 | Air Quality Monitor | Bedroom | - | Wireless | 1 sample/min | Mean values | No | No |
3.3. Quality Assessment
3.4. Clinical Data
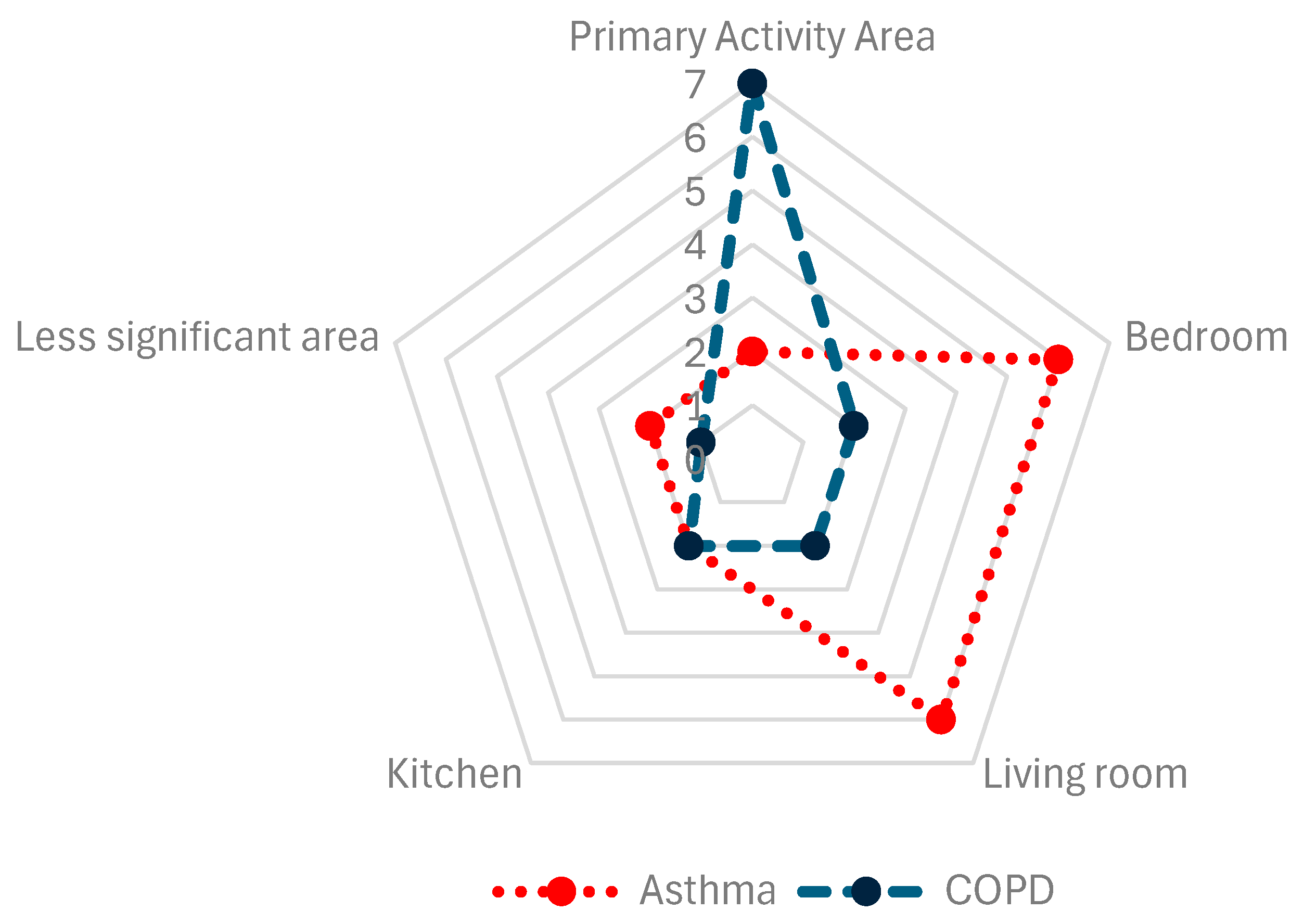
3.5. Air Quality Sensors
3.6. Sensors Calibration
3.7. Data Processing
3.8. Predictive Models and Machine Learning
3.9. Disease Progression and Pollutants
3.9.1. Particulate Matter
3.9.2. Gaseous Pollutants
4. Discussion
4.1. IAQ, Asthma, and COPD
4.2. Sensors for IAQ Monitoring
4.3. Disease Progression and Pollutants
4.3.1. Particulate Matter
4.3.2. Gaseous Pollutants
4.4. Predictive Models and AI
4.5. Methodological Considerations
4.6. Opportunities and Challenges
- (a)
- the lack of methodological standardization in studies.
- (b)
- the need for long-term longitudinal trials that consider the spatial variability, individualized measures of exposure to pollutants, and the heterogeneity in demographic and health characteristics of patients.
- (c)
- the key to connecting monitored air quality measurements with respiratory health markers.
- (d)
- the lack of personalized early warning and recommendations systems that combine environmental monitoring with artificial intelligence techniques.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACQ | Asthma Control Questionnaire |
| ACT | Asthma Control Test |
| AECOPD | Acute Exacerbation of Chronic Obstructive Pulmonary Disease |
| AQ | Air Quality |
| AQI | Air Quality Index |
| AQLQ | Asthma Quality of Life Questionnaire |
| ATS-DLD-78A | American Thoracic Society Division of Lung Diseases Questionnaire for Detecting Respiratory Symptoms in Welders |
| AUC | Area Under the Receive Operating Characteristic Curve |
| BCSS | Breathlessness, Cough and Sputum Scale |
| CAT | COPD Assessment Test |
| CO | Carbon Monoxide |
| CO2 | Carbon Dioxide |
| COPD | Chronic Obstructive Pulmonary Disease |
| CRD | Chronic Respiratory Diseases |
| DNN | Deep Neural Networks |
| EEH | Energy-efficient homes |
| FeNO | Fractional Exhaled Nitric Oxide |
| FEV1 | Forced Expiratory Volume during the first second |
| FVC | Forced Vital Capacity |
| HCHO | Formaldehyde |
| HEPA | High-Efficiency Particulate Air |
| HRQoL | Health-Related Quality of Life |
| IAQ | Indoor Air Quality |
| IoT | Internet of Things |
| MAPE | Mean Absolute Percentage Error |
| mMRC | Modified Medical Research Council Dyspnea Scale |
| NH3 | Ammonia |
| NO2 | Nitrogen Dioxide |
| NRCT | Non-randomized Control Trial |
| O3 | Ozone |
| OCS | Observational Cohort Study |
| PEFR | Peak Expiratory Flow Rate |
| PM | Particulate Matter |
| RCT | Randomized Control Trial |
| RH | Relative Humidity |
| RMSE | Root Mean Square Error |
| RNN | Recurrent Neural Networks |
| RQ | Respiratory Questionnaire |
| SGRQ | St. George’s Respiratory Questionnaire |
| SO2 | Sulfur Dioxide |
| T | Temperature |
| VOCs | Volatile Organic Compounds |
References
- World Health Organization. Chronic Respiratory Diseases. Available online: https://www.who.int/health-topics/chronic-respiratory-diseases#tab=tab_1 (accessed on 16 July 2024).
- Labaki, W.W.; Han, M.K. Chronic respiratory diseases: A global view. Lancet Respir. Med. 2020, 8, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Boers, E.; Barrett, M.; Su, J.G.; Benjafield, A.V.; Sinha, S.; Kaye, L.; Zar, H.J.; Vuong, V.; Tellez, D.; Gondalia, R.; et al. Global Burden of Chronic Obstructive Pulmonary Disease Through 2050. JAMA Netw. Open 2023, 6, e2346598. [Google Scholar] [CrossRef] [PubMed]
- Mattila, T.; Vasankari, T.; Herse, F.; Leskelä, R.-L.; Erhola, M.; Avellan-Hietanen, H.; Toppila-Salmi, S.; Haahtela, T. Contrasting healthcare costs of COPD and asthma in elderly. Respir. Med. 2023, 220, 107477. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.; Khanam, R.; Kabir, E.; Jürges, H. The Healthcare Cost Burden of Asthma in Children: A Longitudinal Population-Based Study. Value Health 2023, 26, 1201–1209. [Google Scholar] [CrossRef]
- Wedzicha, J.A. Impact of Chronic Obstructive Pulmonary Disease Exacerbations on Patients and Payers. Proc. Am. Thorac. Soc. 2006, 3, 218–221. [Google Scholar] [CrossRef]
- Halpin, D.M.; Miravitlles, M.; Metzdorf, N.; Celli, B. Impact and prevention of severe exacerbations of COPD: A review of the evidence. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2891–2908. [Google Scholar] [CrossRef]
- Graham, L.M.; Eid, N. The impact of asthma exacerbations and preventive strategies. Curr. Med. Res. Opin. 2015, 31, 825–835. [Google Scholar] [CrossRef]
- Loftus, P.A.; Wise, S.K. Epidemiology and economic burden of asthma. Int. Forum Allergy Rhinol. 2015, 5, S7–S10. [Google Scholar] [CrossRef]
- Kim, H.; Na, G.; Park, S.; Ra, S.W.; Kang, S.-Y.; Kim, H.-C.; Lee, S.W. The impact of life behavior and environment on particulate matter in chronic obstructive pulmonary disease. Environ. Res. 2021, 198, 111265. [Google Scholar] [CrossRef]
- Chi, R.; Chen, C.; Li, H.; Pan, L.; Zhao, B.; Deng, F.; Guo, X. Different health effects of indoor- and outdoor-originated PM 2.5 on cardiopulmonary function in COPD patients and healthy elderly adults. Indoor Air 2019, 29, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wang, J.; Lu, W. Exposure to nitrogen dioxide and chronic obstructive pulmonary disease (COPD) in adults: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2018, 25, 15133–15145. [Google Scholar] [CrossRef] [PubMed]
- Ghozikali, M.G.; Heibati, B.; Naddafi, K.; Kloog, I.; Conti, G.O.; Polosa, R.; Ferrante, M. Evaluation of Chronic Obstructive Pulmonary Disease (COPD) attributed to atmospheric O3, NO2, and SO2 using Air Q Model (2011–2012 year). Environ. Res. 2016, 144, 99–105. [Google Scholar] [CrossRef]
- Huang, W.; Wu, J.; Lin, X. Ozone Exposure and Asthma Attack in Children. Front. Pediatr. 2022, 10, 830897. [Google Scholar] [CrossRef]
- Agache, I.; Canelo-Aybar, C.; Annesi-Maesano, I.; Cecchi, L.; Rigau, D.; Rodríguez-Tanta, L.Y.; Nieto-Gutierrez, W.; Song, Y.; Cantero-Fortiz, Y.; Roqué, M.; et al. The impact of outdoor pollution and extreme temperatures on asthma-related outcomes: A systematic review for the EAACI guidelines on environmental science for allergic diseases and asthma. Allergy 2024, 79, 1725–1760. [Google Scholar] [CrossRef]
- Bae, W.D.; Kim, S.; Park, C.-S.; Alkobaisi, S.; Lee, J.; Seo, W.; Park, J.S.; Park, S.; Lee, S.; Lee, J.W. Performance improvement of machine learning techniques predicting the association of exacerbation of peak expiratory flow ratio with short term exposure level to indoor air quality using adult asthmatics clustered data. PLoS ONE 2021, 16, e0244233. [Google Scholar] [CrossRef]
- Rabbani, U.F.; Razzaq, S.F.; Irfan, M.F.; Semple, S.; Nafees, A.A.F. Indoor Air Pollution and Respiratory Health in a Metropolitan City of Pakistan. J. Occup. Environ. Med. 2022, 64, 761–765. [Google Scholar] [CrossRef]
- Bhat, G.S.; Shankar, N.; Kim, D.; Song, D.J.; Seo, S.; Panahi, I.M.S.; Tamil, L. Machine Learning-Based Asthma Risk Prediction Using IoT and Smartphone Applications. IEEE Access 2021, 9, 118708–118715. [Google Scholar] [CrossRef]
- Dong, Q.; Li, B.; Downen, R.S.; Tran, N.; Chorvinsky, E.; Pillai, D.K.; Zaghloul, M.E.; Li, Z. A Cloud-Connected NO2 and Ozone Sensor System for Personalized Pediatric Asthma Research and Management. IEEE Sens. J. 2020, 20, 15143–15153. [Google Scholar] [CrossRef]
- Wu, C.-T.; Li, G.-H.; Huang, C.-T.; Cheng, Y.-C.; Chen, C.-H.; Chien, J.-Y.; Kuo, P.-H.; Kuo, L.-C.; Lai, F. Acute Exacerbation of a Chronic Obstructive Pulmonary Disease Prediction System Using Wearable Device Data, Machine Learning, and Deep Learning: Development and Cohort Study. JMIR Mhealth Uhealth 2021, 9, e22591. [Google Scholar] [CrossRef]
- John, B.J.; Harish, C.; Lawrence, C.C.; Krishnakumar, S.; Divakaran, S.; Premkumar, J.; Kanmani, P.G.; Sabarivani, A.; Jagadeesan, A.K. Monitoring indoor air quality using smart integrated gas sensor module (IGSM) for improving health in COPD patients. Environ. Sci. Pollut. Res. Int. 2023, 30, 28889–28902. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Morillo, D.; A Fernandez-Granero, M.; Leon-Jimenez, A. Use of predictive algorithms in-home monitoring of chronic obstructive pulmonary disease and asthma: A systematic review. Chronic Respir. Dis. 2016, 13, 264–283. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme; Peninsula Medical School: Lancaster, UK, 2006. [Google Scholar]
- Egger, M.; Zellweger-Zähner, T.; Schneider, M.; Junker, C.; Lengeler, C.; Antes, G. Language bias in randomised controlled trials published in English and German. Lancet 1997, 350, 326–329. [Google Scholar] [CrossRef]
- Bălă, G.-P.; Timar, B.; Gorun, F.; Motisan, R.; Pescaru, C.; Tudorache, E.; Marc, M.; Manolescu, D.; Citu, C.; Oancea, C. The Impact of Air Pollution on Frequent Exacerbations among COPD Patients: An Observational Study on the Population of Western Romania. J. Clin. Med. 2022, 11, 4352. [Google Scholar] [CrossRef]
- Kang, J.; Kim, H.-C.; Jang, Y.; Lee, J.B.; Lee, J.S.; Oh, Y.-M.; Ji, H.W.; Jung, J.Y.; Lee, S.W. Randomised controlled trial of a behavioural intervention to reduce exposure to PM2.5 in patients with COPD. Environ. Int. 2023, 181, 108286. [Google Scholar] [CrossRef]
- Hansel, N.N.; Putcha, N.; Woo, H.; Peng, R.; Diette, G.B.; Fawzy, A.; Wise, R.A.; Romero, K.; Davis, M.F.; Rule, A.M.; et al. Randomized Clinical Trial of Air Cleaners to Improve Indoor Air Quality and Chronic Obstructive Pulmonary Disease Health: Results of the CLEAN AIR Study. Am. J. Respir. Crit. Care Med. 2022, 205, 421–430. [Google Scholar] [CrossRef]
- Guo, S.-E.; Chi, M.-C.; Hwang, S.-L.; Lin, C.-M.; Lin, Y.-C. Effects of Particulate Matter Education on Self-Care Knowledge Regarding Air Pollution, Symptom Changes, and Indoor Air Quality among Patients with Chronic Obstructive Pulmonary Disease. Int. J. Environ. Res. Public Health 2020, 17, 4103. [Google Scholar] [CrossRef]
- Nurhussien, L.; Kang, C.-M.; Koutrakis, P.; Coull, B.A.; Rice, M.B. Air Pollution Exposure and Daily Lung Function in Chronic Obstructive Pulmonary Disease: Effect Modification by Eosinophil Level. Ann. Am. Thorac. Soc. 2022, 19, 728–736. [Google Scholar] [CrossRef]
- McCarron, A.; Semple, S.; Braban, C.F.; Gillespie, C.; Swanson, V.; Price, H.D. Personal exposure to fine particulate matter (PM2.5) and self-reported asthma-related health. Soc. Sci. Med. 2023, 337, 116293. [Google Scholar] [CrossRef] [PubMed]
- Prasasti, C.I.; Haryanto, B.; Latif, M.T. Association of VOCs, PM2.5 and household environmental exposure with children’s respiratory allergies. Air Qual. Atmos. Health 2021, 14, 1279–1287. [Google Scholar] [CrossRef]
- Kang, I.; McCreery, A.; Azimi, P.; Gramigna, A.; Baca, G.; Hayes, W.; Crowder, T.; Scheu, R.; Evens, A.; Stephens, B. Impacts of residential indoor air quality and environmental risk factors on adult asthma-related health outcomes in Chicago, IL. J. Expo. Sci. Environ. Epidemiol. 2023, 33, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Schachter, E.N.; Rohr, A.; Habre, R.; Koutrakis, P.; Moshier, E.; Nath, A.; Coull, B.; Grunin, A.; Kattan, M. Indoor air pollution and respiratory health effects in inner city children with moderate to severe asthma. Air Qual. Atmos. Health 2020, 13, 247–257. [Google Scholar] [CrossRef]
- Woo, J.; Lee, J.-H.; Kim, Y.; Rudasingwa, G.; Lim, D.H.; Kim, S. Forecasting the Effects of Real-Time Indoor PM2.5 on Peak Expiratory Flow Rates (PEFR) of Asthmatic Children in Korea: A Deep Learning Approach. IEEE Access 2022, 10, 19391–19400. [Google Scholar] [CrossRef]
- Khusial, R.J.; Honkoop, P.J.; Usmani, O.; Soares, M.; Simpson, A.; Biddiscombe, M.; Meah, S.; Bonini, M.; Lalas, A.; Polychronidou, E.; et al. Effectiveness of myAirCoach: A mHealth Self-Management System in Asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 1972–1979.e8. [Google Scholar] [CrossRef]
- Lee, G.H.; Kim, J.H.; Kim, S.; Lee, S.; Lim, D.H. Effects of Indoor Air Purifiers on Children with Asthma. Yonsei Med. J. 2020, 61, 310–316. [Google Scholar] [CrossRef]
- Kim, S.; Lee, J.; Park, S.; Rudasingwa, G.; Lee, S.; Yu, S.; Lim, D.H. Association between Peak Expiratory Flow Rate and Exposure Level to Indoor PM2.5 in Asthmatic Children, Using Data from the Escort Intervention Study. Int. J. Environ. Res. Public Health 2020, 17, 7667. [Google Scholar] [CrossRef]
- Hussain, S.; Parker, S.; Edwards, K.; Finch, J.; Jeanjean, A.; Leigh, R.; Gonem, S. Effects of indoor particulate matter exposure on daily asthma control. Ann. Allergy Asthma Immunol. 2019, 123, 375–380.e3. [Google Scholar] [CrossRef]
- Lim, A.-Y.; Yoon, M.; Kim, E.-H.; Kim, H.-A.; Lee, M.J.; Cheong, H.-K. Effects of mechanical ventilation on indoor air quality and occupant health status in energy-efficient homes: A longitudinal field study. Sci. Total Environ. 2021, 785, 147324. [Google Scholar] [CrossRef]
- Raju, S.; Siddharthan, T.; McCormack, M.C. Indoor Air Pollution and Respiratory Health. Clin. Chest Med. 2020, 41, 825–843. [Google Scholar] [CrossRef] [PubMed]
- Eguiluz-Gracia, I.; Mathioudakis, A.G.; Bartel, S.; Vijverberg, S.J.H.; Fuertes, E.; Comberiati, P.; Cai, Y.S.; Tomazic, P.V.; Diamant, Z.; Vestbo, J.; et al. The need for clean air: The way air pollution and climate change affect allergic rhinitis and asthma. Allergy 2020, 75, 2170–2184. [Google Scholar] [CrossRef] [PubMed]
- Bruce, N.; Perez-Padilla, R.; Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 2000, 78, 1078–1092. [Google Scholar] [PubMed]
- Kurmi, O.P.; Semple, S.; Simkhada, P.; Smith, W.C.S.; Ayres, J.G. COPD and chronic bronchitis risk of indoor air pollution from solid fuel: A systematic review and meta-analysis. Thorax 2010, 65, 221–228. [Google Scholar] [CrossRef]
- Raju, S.; Woo, H.; Koehler, K.; Fawzy, A.; Liu, C.; Putcha, N.; Balasubramanian, A.; Peng, R.D.; Lin, C.T.; Lemoine, C.; et al. Indoor Air Pollution and Impaired Cardiac Autonomic Function in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2023, 207, 721–730. [Google Scholar] [CrossRef]
- Spinelle, L.; Gerboles, M.; Villani, M.G.; Aleixandre, M.; Bonavitacola, F. Field calibration of a cluster of low-cost commercially available sensors for air quality monitoring. Part B: NO, CO and CO2. Sens. Actuators B Chem. 2017, 238, 706–715. [Google Scholar] [CrossRef]
- Karagulian, F.; Barbiere, M.; Kotsev, A.; Spinelle, L.; Gerboles, M.; Lagler, F.; Redon, N.; Crunaire, S.; Borowiak, A. Review of the Performance of Low-Cost Sensors for Air Quality Monitoring. Atmosphere 2019, 10, 506. [Google Scholar] [CrossRef]
- De Vito, S.; Esposito, E.; Salvato, M.; Popoola, O.; Formisano, F.; Jones, R.; Di Francia, G. Calibrating chemical multisensory devices for real world applications: An in-depth comparison of quantitative machine learning approaches. Sens. Actuators B Chem. 2017, 255, 1191–1210. [Google Scholar] [CrossRef]
- Barot, V.; Kapadia, V. Air Quality Monitoring Systems using IoT: A Review. In Proceedings of the 2020 International Conference on Computational Performance Evaluation (ComPE), Shillong, India, 2–4 July 2020; pp. 226–231. [Google Scholar] [CrossRef]
- Ullo, S.L.; Sinha, G.R. Advances in Smart Environment Monitoring Systems Using IoT and Sensors. Sensors 2020, 20, 3113. [Google Scholar] [CrossRef]
- Kumar, A.; Dhawan, S.; Bhatt, S.; Saxena, A.; Khare, M.; Dubey, S.K.; Mehta, D.S. Ambient particulate matter monitoring using bright field imaging-based sensor. Mater. Today Proc. 2024. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, B. Review of relationship between indoor and outdoor particles: I/O ratio, infiltration factor and penetration factor. Atmos. Environ. 2011, 45, 275–288. [Google Scholar] [CrossRef]
- Momtazmanesh, S.; Moghaddam, S.S.; Ghamari, S.-H.; Rad, E.M.; Rezaei, N.; Shobeiri, P.; Aali, A.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abdelmasseh, M.; et al. Global burden of chronic respiratory diseases and risk factors, 1990–2019: An update from the Global Burden of Disease Study 2019. eClinicalMedicine 2023, 59, 101936. [Google Scholar] [CrossRef]
- Zeng, S.; Arjomandi, M.; Tong, Y.; Liao, Z.C.; Luo, G. Developing a Machine Learning Model to Predict Severe Chronic Obstructive Pulmonary Disease Exacerbations: Retrospective Cohort Study. J. Med. Internet Res. 2022, 24, e28953. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, C.; Jabbar, M.S.M.; Zaïane, O.; Osornio-Vargas, A. A systematic review of data mining and machine learning for air pollution epidemiology. BMC Public Health 2017, 17, 907. [Google Scholar] [CrossRef] [PubMed]
- YoussefAgha, A.H.; Jayawardene, W.P.; Lohrmann, D.K.; El Afandi, G.S. Air pollution indicators predict outbreaks of asthma exacerbations among elementary school children: Integration of daily environmental and school health surveillance systems in Pennsylvania. J. Environ. Monit. 2012, 14, 3202–3210. [Google Scholar] [CrossRef]
- Ratcliff, G.E.; Matheny, M.E.; Brown, J.R.; Sullivan, I.; Richmond, B.W.; Paulin, L.M.; Conger, A.K.; Davis, S.E. Integrating Clinical and Air Quality Data to Improve Prediction of COPD Exacerbations. AMIA Annu. Symp. Proc. 2024, 2023, 1209–1217. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC10785856 (accessed on 14 February 2025).
- Hansel, N.N.; McCormack, M.C.; Belli, A.J.; Matsui, E.C.; Peng, R.D.; Aloe, C.; Paulin, L.; Williams, D.L.; Diette, G.B.; Breysse, P.N. In-Home Air Pollution Is Linked to Respiratory Morbidity in Former Smokers with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2013, 187, 1085–1090. [Google Scholar] [CrossRef]
- Klepeis, N.E.; Nelson, W.C.; Ott, W.R.; Robinson, J.P.; Tsang, A.M.; Switzer, P.; Behar, J.V.; Hern, S.C.; Engelmann, W.H. The National Human Activity Pattern Survey (NHAPS): A resource for assessing exposure to environmental pollutants. J. Expo. Sci. Environ. Epidemiol. 2001, 11, 231–252. [Google Scholar] [CrossRef]
- Winquist, A.; Kirrane, E.; Klein, M.; Strickland, M.; Darrow, L.A.; Sarnat, S.E.; Gass, K.; Mulholland, J.; Russell, A.; Tolbert, P. Joint Effects of Ambient Air Pollutants on Pediatric Asthma Emergency Department Visits in Atlanta, 1998–2004. Epidemiology 2014, 25, 666–673. [Google Scholar] [CrossRef]
- Perera, P.N.; Armstrong, E.P.; Sherrill, D.L.; Skrepnek, G.H. Acute Exacerbations of COPD in the United States: Inpatient Burden and Predictors of Costs and Mortality. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 131–141. [Google Scholar] [CrossRef]
- Rennard, S.I.; Farmer, S.G. Exacerbations and Progression of Disease in Asthma and Chronic Obstructive Pulmonary Disease. Proc. Am. Thorac. Soc. 2004, 1, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Chen, W.; Jia, X.; Jia, Y.; Liu, C. Machine learning for prediction of asthma exacerbations among asthmatic patients: A systematic review and meta-analysis. BMC Pulm. Med. 2023, 23, 278. [Google Scholar] [CrossRef]
- Xydi, I.; Saharidis, G.; Kalantzis, G.; Pantazopoulos, I.; Gourgoulianis, K.I.; Kotsiou, O.S. Assessing the Impact of Spatial and Temporal Variability in Fine Particulate Matter Pollution on Respiratory Health Outcomes in Asthma and COPD Patients. J. Pers. Med. 2024, 14, 833. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Managi, S. Spatial Variability of the Relationship between Air Pollution and Well-being. Sustain. Cities Soc. 2022, 76, 103447. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camacho-Magriñán, P.; Sales-Lerida, D.; León-Jiménez, A.; Sanchez-Morillo, D. Indoor Environmental Monitoring and Chronic Respiratory Diseases: A Systematic Review. Technologies 2025, 13, 122. https://doi.org/10.3390/technologies13030122
Camacho-Magriñán P, Sales-Lerida D, León-Jiménez A, Sanchez-Morillo D. Indoor Environmental Monitoring and Chronic Respiratory Diseases: A Systematic Review. Technologies. 2025; 13(3):122. https://doi.org/10.3390/technologies13030122
Chicago/Turabian StyleCamacho-Magriñán, Patricia, Diego Sales-Lerida, Antonio León-Jiménez, and Daniel Sanchez-Morillo. 2025. "Indoor Environmental Monitoring and Chronic Respiratory Diseases: A Systematic Review" Technologies 13, no. 3: 122. https://doi.org/10.3390/technologies13030122
APA StyleCamacho-Magriñán, P., Sales-Lerida, D., León-Jiménez, A., & Sanchez-Morillo, D. (2025). Indoor Environmental Monitoring and Chronic Respiratory Diseases: A Systematic Review. Technologies, 13(3), 122. https://doi.org/10.3390/technologies13030122