



Speckle Plethysmograph-Based Blood Pressure Assessment
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
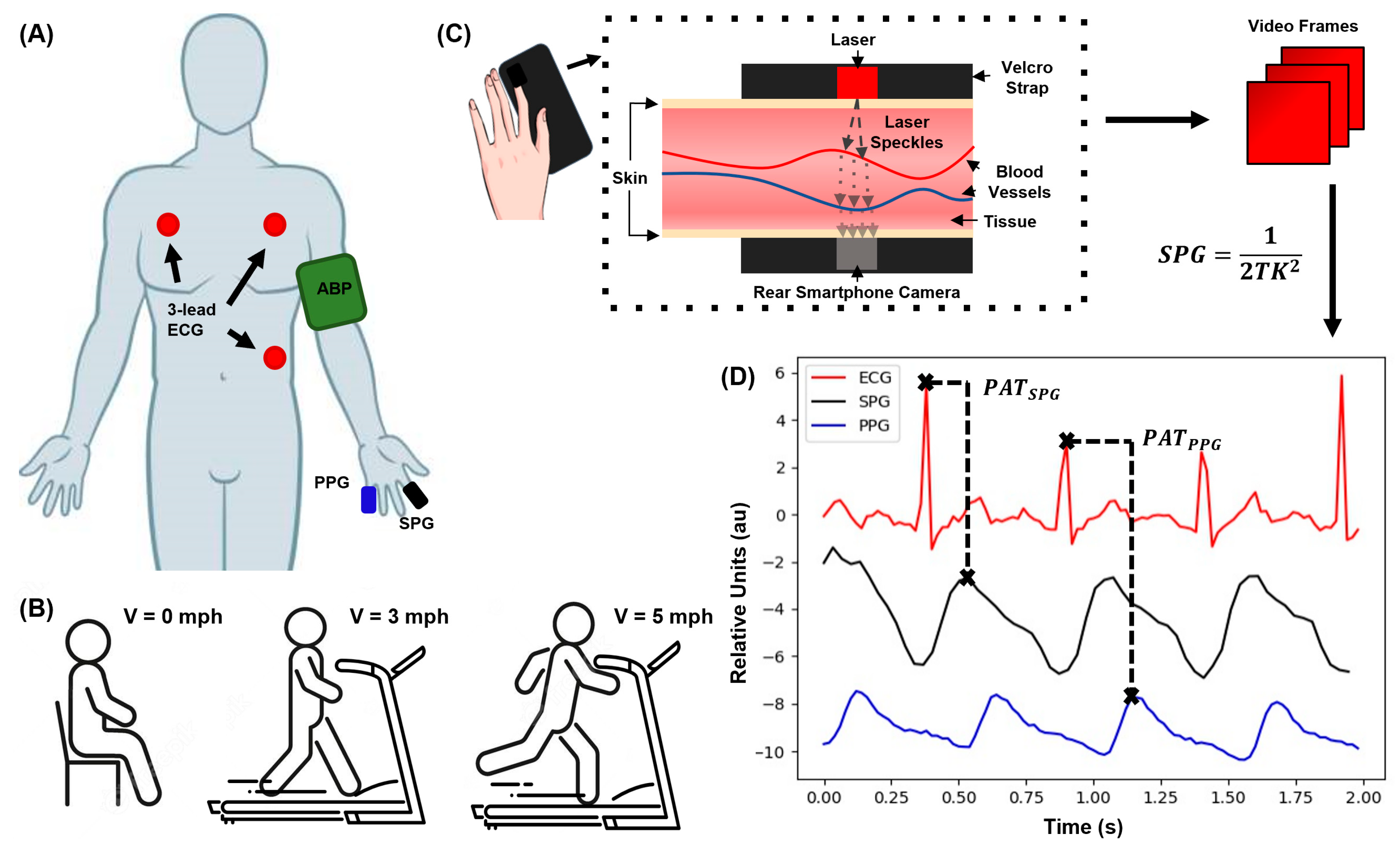
2.1. Experimental Procedure
2.2. Data Processing and Models
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IEEE Standard for Wearable Cuffless Blood Pressure Measuring Devices.; IEEE Standard 1708 IEEE Engineering in Medicine and Biology Society: New York, NY, USA, 2014.
- Valderrama, A.L.; Gillespie, C.; King, S.C.; George, M.G.; Hong, Y.; Gregg, E. Vital signs: Awareness and treatment of uncontrolled hypertension among adults–United States, 2003–2010. MMWR. Morb. Mortal. Weekly Rep. 2012, 61, 703–709. [Google Scholar]
- Carós, J.M.S.I. Continuous Non-Invasive Blood Pressure Estimation; ETH: Zürich, Switzerland, 2011. [Google Scholar]
- Delgado-Gonzalo, S.J.A.R. The Handbook of Cuffless Blood Pressure Monitoring: A Practical Guide for Clinicians, Researchers, and Engineers; Spinger: New York, NY, USA, 2019. [Google Scholar]
- Perloff, D.; Grim, C.; Flack, J.; Frohlich, E.D.; Hill, M.; McDonald, M.; Morgenstern, B.Z. Human blood pressure determination by sphygmomanometry. Circulation 1993, 88, 2460–2470. [Google Scholar] [CrossRef] [PubMed]
- El-Hajj, C.; Kyriacou, P.A. A review of machine learning techniques in photoplethysmography for the non-invasive cuff-less measurement of blood pressure. Biomed. Signal Process. Control 2020, 58, 101870. [Google Scholar] [CrossRef]
- Bartels, K.; Esper, S.A.; Thiele, R.H. Blood pressure monitoring for the anesthesiologist: A practical review. Anesth. Analg. 2016, 122, 1866–1879. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Barbosa, K.; Ho, V.; Griggs, D.; Ghirmai, T.; Krishnan, S.K.; Hsiai, T.K.; Chiao, J.-C.; Cao, H. Cuff-less and Continuous Blood Pressure Monitoring: A Methodological Review. Technologies 2017, 5, 21. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Goldberger, Z.D.; Shvilkin, A. Clinical Electrocardiography: A Simplified Approach E-Book; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Elgendi, M.; Fletcher, R.; Liang, Y.; Howard, N.; Lovell, N.H.; Abbott, D.; Lim, K.; Ward, R. The Use of Photoplethysmography for Assessing Hypertension. NPJ Digit. Med. 2019, 2, 60. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Atef, M.; Lian, Y. Towards a continuous non-invasive cuffless blood pressure monitoring system using PPG: Systems and circuits review. IEEE Circuits Syst. Mag. 2018, 18, 6–26. [Google Scholar] [CrossRef]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuffless Blood Pressure Estimation Algorithms for Continuous Health-Care Monitoring. IEEE Trans. Biomed. Eng. 2016, 64, 859–869. [Google Scholar] [CrossRef]
- Chen, S.; Ji, Z.; Wu, H.; Xu, Y. A Non-Invasive Continuous Blood Pressure Estimation Approach Based on Machine Learning. Sensors 2019, 19, 2585. [Google Scholar] [CrossRef]
- Liu, Z.; Zhou, B.; Li, Y.; Tang, M.; Miao, F. Continuous Blood Pressure Estimation From Electrocardiogram and Photoplethysmogram during Arrhythmias. Front. Physiol. 2020, 11, 575407. [Google Scholar] [CrossRef]
- Olazábal, J.H.; Wieringa, F.; Hermeling, E.; Van Hoof, C. Beat-to-beat intervals of speckle amp; intensity-based optical plethysmograms compared to electrocardiogram. In 2021 Computing in Cardiology; IEEE: New York, NY, USA, 2021. [Google Scholar]
- Dunn, C.E.; Lertsakdadet, B.; Crouzet, C.; Bahani, A.; Choi, B. Comparison of speckleplethysmographic (spg) and photoplethysmographic (ppg) imaging by monte carlo simulations and in vivo measurements. Biomed. Opt. Express 2018, 9, 4306–4316. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.B.; Yang, B.; White, S. Effect of skin optical absorption on speckleplethysmographic (spg) signals. Biomed. Opt. Express 2020, 11, 5352–5361. [Google Scholar] [CrossRef] [PubMed]
- Bi, R.; Du, Y.; Singh, G.; Ho, J.-H.; Zhang, S.; Attia, A.B.E.; Li, X.; Olivo, M.C. Fast pulsatile blood flow measurement in deep tissue through a multimode detection fiber. J. Biomed. Opt. 2020, 25, 055003. [Google Scholar] [CrossRef] [PubMed]
- Dunn, C.E.; Monroe, D.C.; Crouzet, C.; Hicks, J.W.; Choi, B. Speckleplethysmographic (SPG) estimation of heart rate variability during an orthostatic challenge. Sci. Rep. 2019, 9, 14079. [Google Scholar] [CrossRef]
- Jakovels, D.; Saknite, I.; Krievina, G.; Zaharans, J.; Spigulis, J. Mobile phone based laser speckle contrast imager for assessment of skin blood flow. In Proceedings of the Eighth International Conference on Advanced Optical Materials and Devices (AOMD-8), Riga, Latvia, 25–27 August 2014; SPIE: Bellingham, WA, USA, 2014. [Google Scholar] [CrossRef]
- Ghijsen, M.; Rice, T.B.; Yang, B.; White, S.M.; Tromberg, B.J. Wearable speckleplethysmography (spg) for characterizing microvascular flow and resistance. Biomed. Opt. Express 2018, 9, 3937–3952. [Google Scholar] [CrossRef]
- Stojanova, A.; Koceski, S.; Koceska, N. Continuous blood pressure monitoring as a basis for ambient assisted living (AAL)–review of methodologies and devices. J. Med. Syst. 2019, 43, 24. [Google Scholar] [CrossRef] [PubMed]
- Bard, D.M.; Joseph, J.I.; van Helmond, N. Cuff-less methods for blood pressure telemonitoring. Front. Cardiovasc. Med. 2019, 6, 40. [Google Scholar] [CrossRef]
- Mukkamala, R.; Hahn, J.-O.; Inan, O.T.; Mestha, L.K.; Kim, C.-S.; Toreyin, H.; Kyal, S. Toward ubiquitous blood pressure monitoring via Pulse Transit Time: Theory and Practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef]
- Olazabal, J.H.; Lorato, I.; Kling, J.; Verhoeven, M.; Wieringa, F.; Van Hoof, C.; Verkruijsse, W.; Hermeling, E. Comparison between Speckle Plethysmography and Photoplethysmography during Cold Pressor Test Referenced to Finger Arterial Pressure. Sensors 2023, 23, 5016. [Google Scholar] [CrossRef]
- Olazábal, J.H.; Wieringa, F.; Hermeling, E.; Van Hoof, C. Camera-Derived Photoplethysmography (rPPG) and Speckle Plethysmography (rSPG): Comparing Reflective and Transmissive Mode at Various Integration Times Using LEDs and Lasers. Sensors 2022, 22, 6059. [Google Scholar] [CrossRef]
- Ellington, F.T. Elucidation of Speckleplethysmography as an Alternative to Photoplethysmography for Deriving Blood Pressure; UC Irvine, eScholarship: Irvine, CA, USA, 2022. [Google Scholar]
- Xu, H.; Caramanis, C.; Mannor, S. Robustness and Regularization of Support Vector Machines. J. Mach. Learn. Res. 2009, 10, 1485–1510. [Google Scholar]
- Leiva, R.G.; Anta, A.F.; Mancuso, V.; Casari, P. A Novel Hyperparameter-Free Approach to Decision Tree Construction That Avoids Overfitting by Design. IEEE Access 2019, 7, 99978–99987. [Google Scholar] [CrossRef]
- Zhang, G.; Gao, M.; Xu, D.; Olivier, N.B.; Mukkamala, R. Pulse arrival time is not an adequate surrogate for pulse transit time as a marker of blood pressure. J. Appl. Physiol. 2011, 111, 1681–1686. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| RSME (± mmHg) | SV (1 Feat.) | SV (2 Feat.) | DT (1 Feat.) | DT (2 Feat.) |
|---|---|---|---|---|
| SPG Rest | 12.4 | 3.7 | 3.9 | 2.8 |
| PPG Rest | 13.7 | 3.7 | 22.5 | 1.9 |
| SPG LE | 16.1 | 15.9 | 20.1 | 2.2 |
| PPG LE | 15.3 | 15.9 | 14.1 | 3.7 |
| SPG HE | 20 | 19.3 | 22.7 | 25.9 |
| PPG HE | 21 | 19.3 | 11.9 | 17.2 |
| MAPE (%) | SV (1 Feat.) | SV (2 Feat.) | DT (1 Feat.) | DT (2 Feat.) |
|---|---|---|---|---|
| SPG Rest | 8 | 3 | 3 | 2 |
| PPG Rest | 9 | 3 | 15 | 1 |
| SPG LE | 11 | 10 | 14 | 2 |
| PPG LE | 10 | 10 | 9 | 3 |
| SPG HE | 10 | 11 | 11 | 14 |
| PPG HE | 11 | 11 | 7 | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ellington, F.T.; Nguyen, A.; Huang, M.-H.; Le, T.; Choi, B.; Cao, H. Speckle Plethysmograph-Based Blood Pressure Assessment. Technologies 2024, 12, 70. https://doi.org/10.3390/technologies12050070
Ellington FT, Nguyen A, Huang M-H, Le T, Choi B, Cao H. Speckle Plethysmograph-Based Blood Pressure Assessment. Technologies. 2024; 12(5):70. https://doi.org/10.3390/technologies12050070
Chicago/Turabian StyleEllington, Floranne T., Anh Nguyen, Mao-Hsiang Huang, Tai Le, Bernard Choi, and Hung Cao. 2024. "Speckle Plethysmograph-Based Blood Pressure Assessment" Technologies 12, no. 5: 70. https://doi.org/10.3390/technologies12050070
APA StyleEllington, F. T., Nguyen, A., Huang, M.-H., Le, T., Choi, B., & Cao, H. (2024). Speckle Plethysmograph-Based Blood Pressure Assessment. Technologies, 12(5), 70. https://doi.org/10.3390/technologies12050070