The Validity of the Theory of Planned Behaviour for Understanding People’s Beliefs and Intentions toward Reusing Medicines



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Overview of the Common Health-Related Behavioural Change Theories
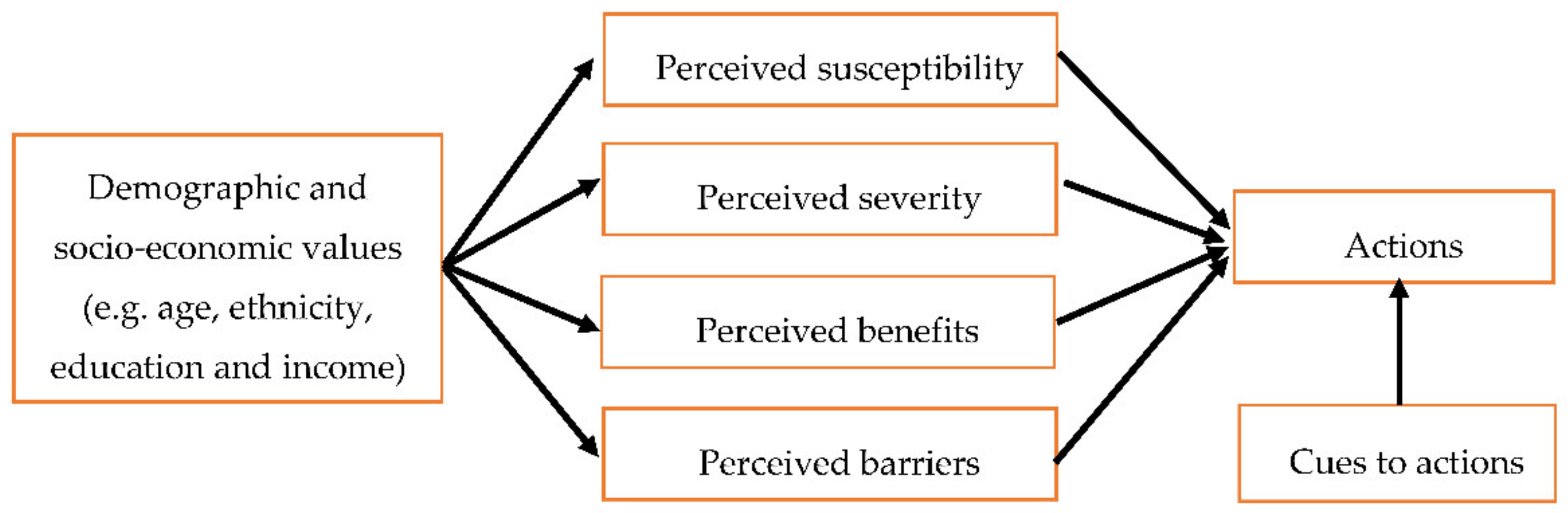
2.1. Health Belief Model (HBM)
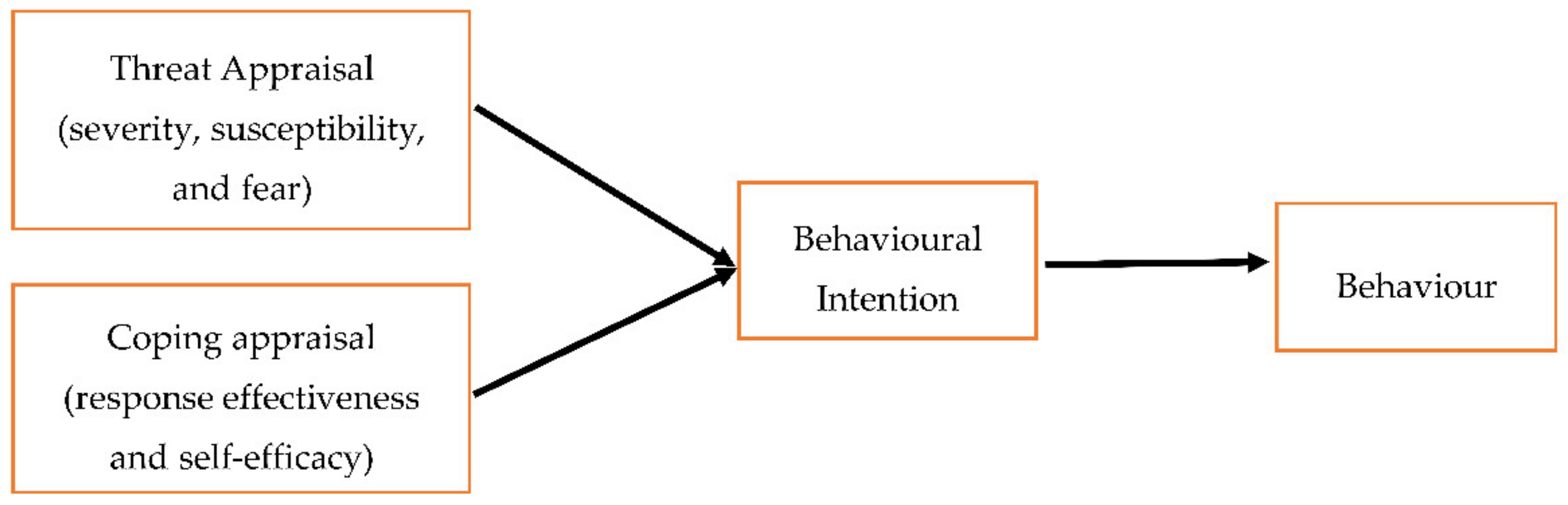
2.2. Protection Motivation Theory (PMT)
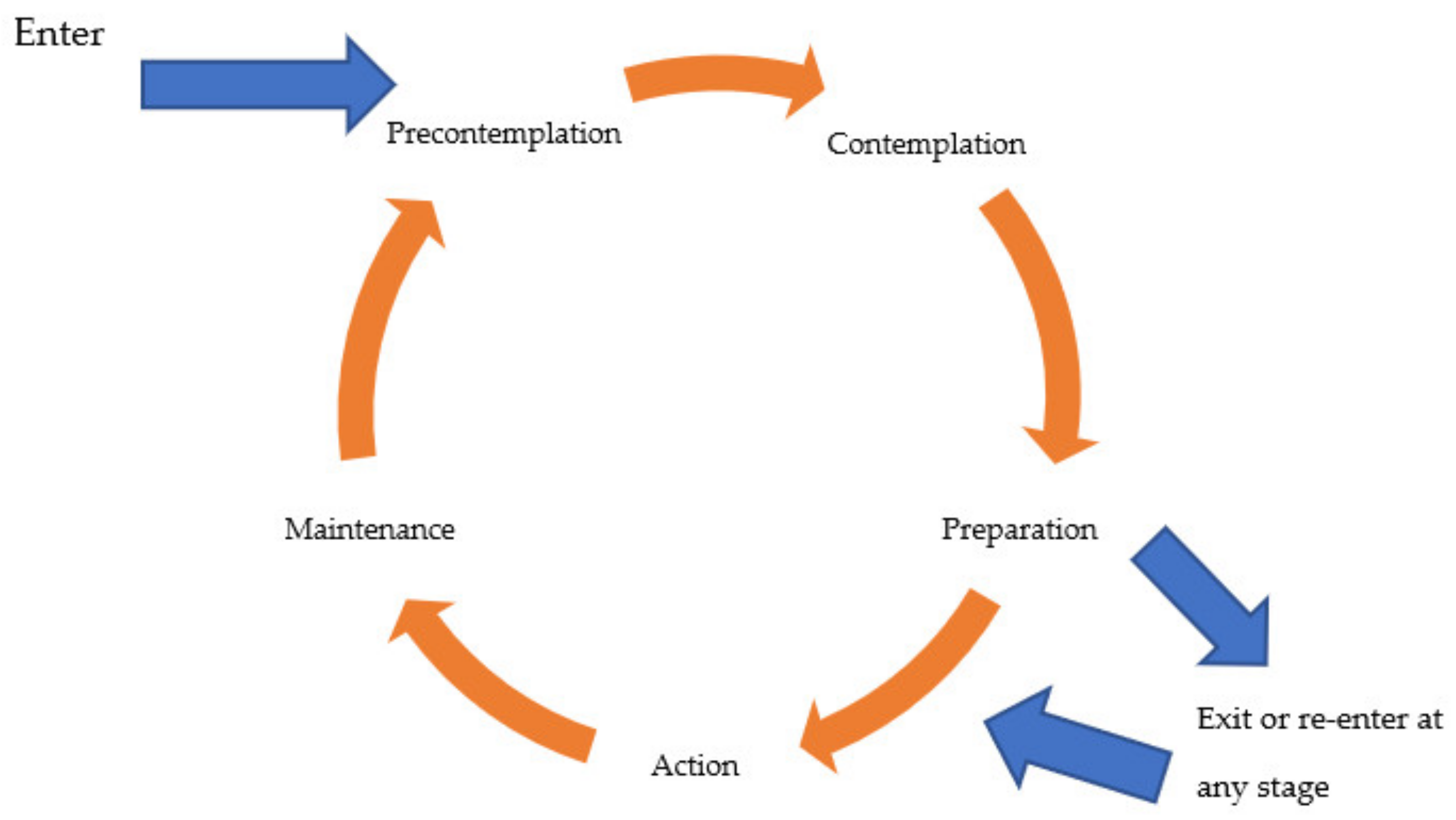
2.3. Trans-Theoretical Model of Behaviour Change or Stages of Change (TTM/SoC)
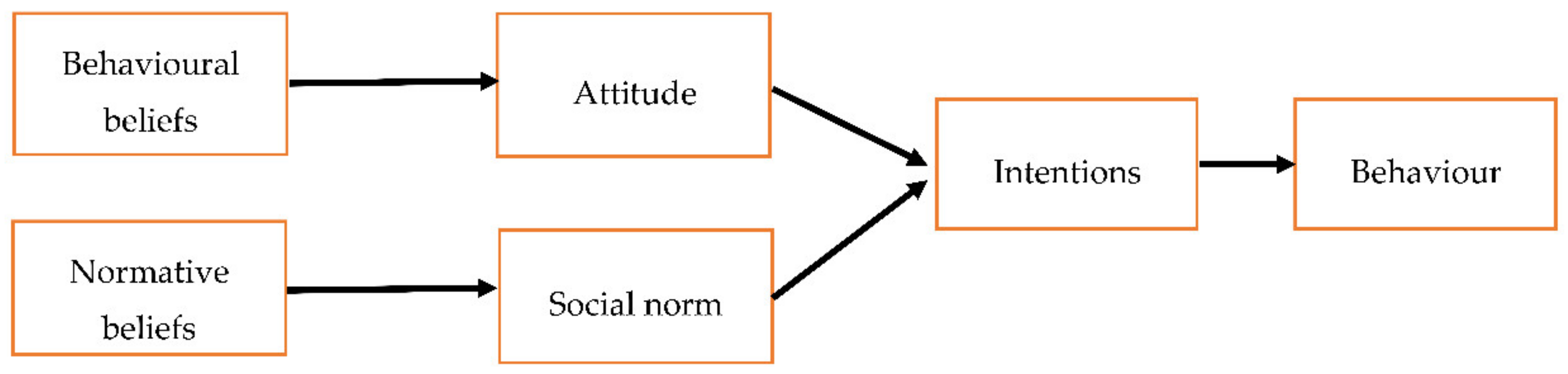
2.4. The Theory of Reasoned Action (TRA) and the Theory of Planned Behaviour (TPB)
3. Discussion
3.1. The TPB Compared to the TRA, HBM, PMT, and TTM/SoC
3.2. Support for the Application of TPB to Predicts People’s Behaviour and Intention towards Reusing Medicines
3.3. Steps to Manage the Development of a TPB Medication Reuse Questionnaire (MRQ) to Explore People’s Beliefs and Intention toward Reusing Medicines
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alhamad, H.; Patel, N.; Donyai, P. Towards Medicines Reuse: A Narrative Review of the Different Therapeutic Classes and Dosage Forms of Medication Waste in Different Countries. Pharmacy 2020, 8, 230. [Google Scholar] [CrossRef]
- Hui, T.K.L.; Mohammed, B.; Donyai, P.; McCrindle, R.; Sherratt, R.S. Enhancing pharmaceutical packaging through a technology ecosystem to facilitate the reuse of medicines and reduce medicinal waste. Pharmacy 2020, 8, 58. [Google Scholar] [CrossRef]
- Hui, T.K.L.; Donyai, P.; McCrindle, R.; Sherratt, R.S. Enabling Medicine Reuse Using a Digital Time Temperature Humidity Sensor in an Internet of Pharmaceutical Things Concept. Sensors 2020, 20, 3080. [Google Scholar] [CrossRef]
- Michie, S.; Johnston, M.; Abraham, C.; Lawton, R.; Parker, D.; Walker, A. Making psychological theory useful for implementing evidence based practice: A consensus approach. BMJ Qual. Saf. 2005, 14, 26–33. [Google Scholar] [CrossRef]
- Godin, G.; Bélanger-Gravel, A.; Eccles, M.; Grimshaw, J. Healthcare professionals’ intentions and behaviours: A systematic review of studies based on social cognitive theories. Implement. Sci. 2008, 3, 36. [Google Scholar] [CrossRef] [PubMed]
- Armitage, C.J.; Conner, M. Efficacy of the theory of planned behaviour: A meta-analytic review. Br. J. Soc. Psychol. 2001, 40, 471–499. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.; Bury, M.; Campling, N.; Carter, S.; Garfied, S.; Newbould, J.; Rennie, T. A Review of the Use of the Health Belief Model (HBM), the Theory of Reasoned Action (TRA), the Theory of Planned Behaviour (TPB) and the Trans-Theoretical Model (TTM) to Study and Predict Health Related Behaviour Change; The National Institute for Health and Clinical Excellence: London, UK, 2006; pp. 1–215. [Google Scholar]
- Ogden, J. Health Psychology: A Textbook: A textbook; McGraw-Hill Education: London, UK, 2012. [Google Scholar]
- Michie, S. Designing and implementing behaviour change interventions to improve population health. J. Health Serv. Res. Policy 2008, 13 (Suppl. S3), 64–69. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef]
- Alhamad, H.; Patel, N.; Donyai, P. How do people conceptualise the reuse of medicines? An interview study. Int. J. Pharm. Pract. 2018, 26, 232–241. [Google Scholar] [CrossRef]
- Alhamad, H.; Donyai, P. Intentions to “Reuse” Medication in the Future Modelled and Measured Using the Theory of Planned Behavior. Pharmacy 2020, 8, 213. [Google Scholar] [CrossRef] [PubMed]
- Donyai, P. Social and Cognitive Pharmacy: Theory and Case Studies; Pharmaceutical Press: London, UK, 2012. [Google Scholar]
- Armitage, C.J.; Conner, M. Social cognition models and health behaviour: A structured review. Psychol. Health 2000, 15, 173–189. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Conner, M. Cognitive determinants of health behavior. In Handbook of Behavioral Medicine; Springer: Berlin/Heidelberg, Germany, 2010; pp. 19–30. [Google Scholar]
- Munro, S.; Lewin, S.; Swart, T.; Volmink, J. A review of health behaviour theories: How useful are these for developing interventions to promote long-term medication adherence for TB and HIV/AIDS? BMC Public Health 2007, 7, 104. [Google Scholar] [CrossRef]
- Janmaimool, P. Application of protection motivation theory to investigate sustainable waste management behaviors. Sustainability 2017, 9, 1079. [Google Scholar] [CrossRef]
- Norman, P.; Boer, H.; Seydel, E.R. Protection motivation theory. Predict. Health Behav. 2005, 81, 126. [Google Scholar]
- Morris, J.; Marzano, M.; Dandy, N.; O’Brien, L. Theories and Models of Behaviour and Behaviour Change; Forest Research: Surrey, UK, 2012; pp. 1–27. [Google Scholar]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- West, R. Time for a change: Putting the Transtheoretical (Stages of Change) Model to rest. Addiction 2005, 100, 1036–1039. [Google Scholar]
- Friman, M.; Huck, J.; Olsson, L.E. Transtheoretical model of change during travel behavior interventions: An integrative review. Int. J. Environ. Res. Public Health 2017, 14, 581. [Google Scholar] [CrossRef]
- Fishbein, M. Leek Ajzen (1975), Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading; Addison-Wesley: Boston, MA, USA, 1981. [Google Scholar]
- Ajzen, I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior 1. J. Appl. Soc. Psychol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Steinmetz, H.; Knappstein, M.; Ajzen, I.; Schmidt, P.; Kabst, R. How effective are behavior change interventions based on the theory of planned behavior? Zeitschrift fürPsychol. 2016, 224, 216–233. [Google Scholar] [CrossRef]
- Francis, J.; Eccles, M.P.; Johnston, M.; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers; Centre for Health Services Research, University of Newcastle upon Tyne: Newcastle upon Tyne, UK, 2004. [Google Scholar]
- TPB with Background Factors. Available online: https://people.umass.edu/aizen/tpb.background.html (accessed on 4 December 2020).
- Ajzen, I. The theory of planned behavior: Frequently asked questions. Hum. Behav. Emerg. Technol. 2020, 2, 314–324. [Google Scholar] [CrossRef]
- Armitage, C.J.; Christian, J. From attitudes to behaviour: Basic and applied research on the theory of planned behaviour. Curr. Psychol. 2003, 22, 187–195. [Google Scholar] [CrossRef]
- Noar, S.M.; Zimmerman, R.S. Health behavior theory and cumulative knowledge regarding health behaviors: Are we moving in the right direction? Health Educ. Res. 2005, 20, 275–290. [Google Scholar] [CrossRef]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an effective health interventions design: An extension of the health belief model. Online J. Public Health Inf. 2012, 4. [Google Scholar] [CrossRef] [PubMed]
- Davis, G.; Morgan, A. Using the Theory of Planned Behaviour to Determine Recycling and Waste Minimisation Behaviours: A Case Study of Bristol City, UK. Aust. Community Psychol. 2008, 20, 105–117. [Google Scholar]
- Topa, G.; Moriano, J.A. Theory of planned behavior and smoking: Meta-analysis and SEM model. Subst. Abus. Rehabil. 2010, 1, 23. [Google Scholar] [CrossRef] [PubMed]
- Chase, K.; Reicks, M.; Jones, J.M. Applying the theory of planned behavior to promotion of whole-grain foods by dietitians. J. Am. Diet. Assoc. 2003, 103, 1639–1642. Available online: https://pubmed.ncbi.nlm.nih.gov/14647092/ (accessed on 5 December 2020). [CrossRef]
- Milton, A.C.; Mullan, B.A. An application of the theory of planned behavior—A randomized controlled food safety pilot intervention for young adults. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2012, 31, 250–259. [Google Scholar] [CrossRef]
- Hagger, M.S.; Chatzisarantis, N.L.D.; Biddle, S.J.H. A meta-analytic review of the theories of reasoned action and planned behavior in physical activity: Predictive validity and the contribution of additional variables. J. Sport Exerc. Psychol. 2002, 24, 3–32. [Google Scholar] [CrossRef]
- McConnon, Á.; Raats, M.; Astrup, A.; Bajzova, M.; Handjieva-Darlenska, T.; Lindroos, A.K.; Martínez, J.A.; Larson, T.M.; Papadaki, A.; Pfeiffer, A.F.H.; et al. Application of the Theory of Planned Behaviour to weight control in an overweight cohort. Results from a pan-European dietary intervention trial (DiOGenes). Appetite 2012, 58, 313–318. [Google Scholar] [CrossRef]
- Armitage, C.J.; Talibudeen, L. Test of a brief theory of planned behaviour-based intervention to promote adolescent safe sex intentions. Br. J. Psychol. 2010, 101, 155–172. [Google Scholar] [CrossRef]
- Quine, L.; Rutter, D.R.; Arnold, L. Persuading school-age cyclists to use safety helmets: Effectiveness of an intervention based on the Theory of Planned Behaviour. Br. J. Health Psychol. 2001, 6, 327–345. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.A.; Armitage, C.J. Promoting drivers’ compliance with speed limits: Testing an intervention based on the theory of planned behaviour. Br. J. Psychol. 2009, 100, 111–132. [Google Scholar] [CrossRef]
- de Leeuw, A.; Valois, P.; Schmidt, P.; Ajzen, I. Using the theory of planned behavior to identify key beliefs underlying pro-environmental behavior in high-school students: Implications for educational interventions. Artic. J. Environ. Psychol. 2015, 42, 128–138. [Google Scholar] [CrossRef]
- Pakpour, A.H.; Zeidi, I.M.; Emamjomeh, M.M.; Asefzadeh, S.; Pearson, H. Household waste behaviours among a community sample in Iran: An application of the theory of planned behaviour. Waste Manag. 2014, 34, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Kok, G. The theory of planned behavior: A review of its applications to health-related behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef]
- Bledsoe, L.K. Smoking cessation: An application of theory of planned behavior to understanding progress through stages of change. Addict. Behav. 2006, 31, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, M.A.; Williamson, G.M.; Lance, C.E.; Mulloy, L.L. Predicting adherence to immunosuppressant therapy: A prospective analysis of the theory of planned behaviour. Nephrol. Dial. Transplant. 2007, 22, 2339–2348. [Google Scholar] [CrossRef] [PubMed]
- Perkins, M.B.; Jensen, P.S.; Jaccard, J.; Gollwitzer, P.; Oettingen, G.; Pappadopulos, E.; Hoagwood, K.E. Applying theory-driven approaches to understanding and modifying clinicians’ behavior: What do we know? Psychiatr. Serv. 2007, 58, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Hagger, M.S.; Lonsdale, A.; Chatzisarantis, N.L.D. A theory-based intervention to reduce alcohol drinking in excess of guideline limits among undergraduate students. Br. J. Health Psychol. 2012, 17, 18–43. [Google Scholar] [CrossRef]
- Armitage, C.J.; Rowe, R.; Arden, M.A.; Harris, P.R. A brief psychological intervention that reduces adolescent alcohol consumption. J. Consult. Clin. Psychol. 2014, 82, 546. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Clift, S.; Grabowski, P. Cognitive predictors of adherence to malaria prophylaxis regimens on return from a malarious region: A prospective study. Soc. Sci. Med. 1999, 48, 1641–1654. [Google Scholar] [CrossRef]
- Yardley, L.; Miller, S.; Schlotz, W.; Little, P. Evaluation of a Web-based intervention to promote hand hygiene: Exploratory randomized controlled trial. J. Med. Internet Res. 2011, 13, e107. [Google Scholar] [CrossRef]
- Schifter, D.E.; Ajzen, I. Intention, perceived control, and weight loss: An application of the theory of planned behavior. J. Pers. Soc. Psychol. 1985, 49, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.R.; Norman, P.; Goyder, E.; Harris, P.R.; Campbell, M.J. Pilot study of a brief intervention based on the theory of planned behaviour and self-identity to increase chlamydia testing among young people living in deprived areas. Br. J. Health Psychol. 2014, 19, 636–651. [Google Scholar] [CrossRef]
- Asare, M. Using The Theory of Planned Behavior to Determine the Condom Use Behavior Among College Students. Am. J. Health Stud. 2015, 30, 43–50. [Google Scholar]
- Sheeran, P.; Silverman, M. Evaluation of three interventions to promote workplace health and safety: Evidence for the utility of implementation intentions. Soc. Sci. Med. 2003, 56, 2153–2163. [Google Scholar] [CrossRef]
- Understanding Individuals’ Environmentally Significant Behavior|Environmental Law Reporter. Available online: https://elr.info/news-analysis/35/10785/understanding-individuals-environmentally-significant-behavior (accessed on 5 December 2020).
- Koger, S.M. The Psychology of Environmental Problems; Psychology Press: East Sussex, UK, 2011; Available online: http://www.copyright.com/ (accessed on 5 December 2020).
- Sumaedi, S.; Yarmen, M.; Bakti, I.G.M.Y.; Rakhmawati, T.; Astrini, N.J.; Widianti, T. The integrated model of theory planned behavior, value, and image for explaining public transport passengers’ intention to reuse. Manag. Environ. Qual. 2016, 27, 124–135. [Google Scholar] [CrossRef]
- van der Linden, S. Charitable Intent: A Moral or Social Construct? A Revised Theory of Planned Behavior Model. Curr. Psychol. 2011, 30, 355–374. Available online: https://link.springer.com/article/10.1007/s12144-011-9122-1 (accessed on 5 December 2020). [CrossRef]
- Ham, M.; Jeger, M.; Frajman Ivković, A. The role of subjective norms in forming the intention to purchase green food. Econ. Res. Istraživanja 2015, 28, 738–748. [Google Scholar] [CrossRef]
- Heuckmann, B.; Hammann, M.; Asshoff, R. Advantages and disadvantages of modeling beliefs by single item and scale models in the context of the theory of planned behavior. Educ. Sci. 2019, 9, 268. [Google Scholar] [CrossRef]
- Ajzen, I. TPB Questionnaire Construction 1. Constructing a Theory of Planned Behavior Questionnaire. Available online: https://people.umass.edu/aizen/pdf/tpb.measurement.pdf (accessed on 19 February 2021).





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhamad, H.; Donyai, P. The Validity of the Theory of Planned Behaviour for Understanding People’s Beliefs and Intentions toward Reusing Medicines. Pharmacy 2021, 9, 58. https://doi.org/10.3390/pharmacy9010058
Alhamad H, Donyai P. The Validity of the Theory of Planned Behaviour for Understanding People’s Beliefs and Intentions toward Reusing Medicines. Pharmacy. 2021; 9(1):58. https://doi.org/10.3390/pharmacy9010058
Chicago/Turabian StyleAlhamad, Hamza, and Parastou Donyai. 2021. "The Validity of the Theory of Planned Behaviour for Understanding People’s Beliefs and Intentions toward Reusing Medicines" Pharmacy 9, no. 1: 58. https://doi.org/10.3390/pharmacy9010058
APA StyleAlhamad, H., & Donyai, P. (2021). The Validity of the Theory of Planned Behaviour for Understanding People’s Beliefs and Intentions toward Reusing Medicines. Pharmacy, 9(1), 58. https://doi.org/10.3390/pharmacy9010058