Design of a Pharmacy Curriculum on Patient Centered Communication Skills


 ,
,
Abstract
1. Introduction
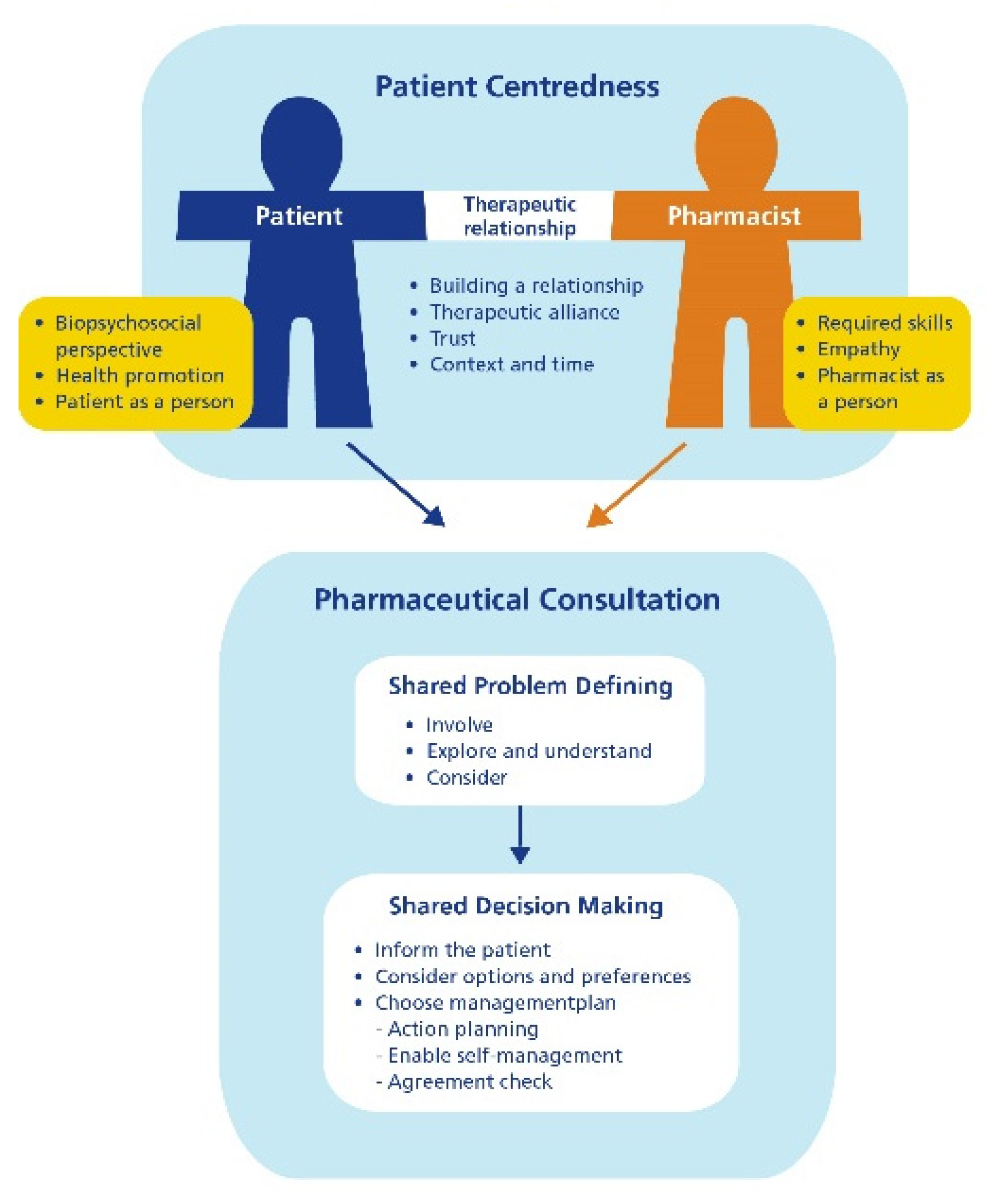
2. Patient Centered Communication
- The pharmacist considers the patient as a unique person, with unique problems which require tailored solutions
- The focus of the pharmacist is more on the patient than the product, the pharmacist is respectful and empathic
- The pharmacist strives for mutual understanding and agreement, both pharmacist and patient participate: two-way communication
- The pharmacist shares control and responsibility with the patient as much as possible, respecting the patient’s right on information
- The pharmacist stimulates the patient to be self-reliant
- The pharmacist adapts their communication style to the individual patient
- The pharmacist views being competent in communication as an important part of their profession
3. General Educational Principles for Our Curriculum Design
- Systematic and explicit attention to the development of academic and personal skills and values. Patient centered communication is repeatedly trained and practiced in courses in year 1 and 3 of our master program, increasing the complexity of the specific skills or consultations over time.
- The principle of constructive alignment: a curriculum in which the teaching activities are based on the desired learning outcomes, which are assessed in such a way that the desired study behavior of students will be evoked [21]. Consequently, it is important to describe the learning objectives carefully. As a source of inspiration, we used Bachmann’s description of learning objectives for a core communication curriculum for health care professions [22]. This description is based on literature and expert knowledge.
- Learning in context: knowledge and skills are taught in a context relevant for the future profession. Therefore, it is important to integrate communication competence with pharmaceutical expertise in educational activities and not provide it as a single course only focusing on communication skills. By incorporating communication skills training in different courses, a wide variety of contexts is offered. Some of our courses use the method of experiential learning. This means that learning activities at the university run parallel with students’ internships at the pharmacy. It aims to enhance the integration of theoretical understanding and practical experience and to promote transfer of learning. During internships students can practice what they have learned and get feedback from their internship supervisors, which is an effective way of learning [13].
- The Self-Determination Theory (SDT) poses that people will be motivated when three psychological needs are fulfilled, namely feeling competent, feeling connected with others and being able to make autonomous decisions [23]. Therefore, the program should stimulate active study behavior, it should be challenging and varied and should enable students to follow individual interests, thus motivating students for learning.The courses in our curriculum in which communication skills training is integrated are all compulsory, so students do not have the freedom to opt out. Nevertheless, we stimulate, activate and motivate students to participate as active learners in different ways. Firstly, we offer students e-learning modules that they can use to prepare for the training session. This gives them the freedom to choose when to do these modules. Secondly, some learning activities (regarding clinical medication reviews) are optional. Thirdly, students can choose their own learning goals for the training sessions. Finally, students have multiple opportunities to pass the assessment. In time, they will be able to succeed and feel competent.
- Using a well-balanced system of mentoring and assessment. We try to create such a balanced system by using different types of assessment (self-reflection assignments, peer feedback, assessment of consultations), as well as both formative (focused on development) as summative assessment (focused on meeting the defined standards). We also pay attention to reflection through a system of mentoring by qualified teachers.
- Self-directed learning: the direction of the learning process is gradually shifted from teacher to student, from more traditional forms of teaching to methods that stimulate students to take responsibility for their own learning process [24]. At the beginning of year 1, we strongly guide our students in the educational activities followed by a summative assessment. Later in year 1 and 3 students have more responsibility for their own learning process. Then, the assessment is more often formative and the portfolio with personal reflections is even more important for their learning process.
4. Teaching Methods for Communication Skills
4.1. Preparatory E-Modules
- Theory: texts and knowledge clips
- Videoclips of (effective and not effective) consultations with reflection assignments
- Assignments to self-test both pharmaceutical knowledge as well as insight in consultations and communication
- Interactive simulation with a virtual patient
- Assignments to formulate personal learning goals and questions
4.2. Small Group Training (including Roleplay)
4.2.1. Importance of a Safe Learning Environment
4.2.2. Working with Simulation Patients
4.3. Assessment of Communication Competence
5. Major Topics on Patient Centered Communication in Our Curriculum
5.1. Pharmaceutical Consultations on Prescription Medicines
5.2. Pharmaceutical Consultations on Self-Care Medication
5.3. Clinical Medication Reviews

6. Final Remarks
6.1. The Importance of Support by Management
6.2. Strive for Quality and Effectiveness
6.3. The Importance of Supportive and Qualified Staff
6.3.1. Using the Experience and Expertise of Others
6.3.2. A Curriculum Is Never Finished
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Droege, M. The role of reflective practice in pharmacy. Educ. Health Chang. Learn. Pract. 2003, 16, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Hosp. Pharm. 1990, 47, 533–543. [Google Scholar] [CrossRef] [PubMed]
- International Pharmaceutical Federation. Strategic Plan 2019 to 2024; FIP: The Hague, The Netherlands, 2019; pp. 1–9. [Google Scholar]
- De Oliveira, D.R.; Shoemaker, S.J. Achieving patient centeredness in pharmacy practice: Openness and the pharmacist’s natural attitude. J. Am. Pharm. Assoc. 2006, 46, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, A.M. Teaching patient-centered care to pharmacy students. Int. J. Clin. Pharm. 2011, 33, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Ilardo, M.L.; Speciale, A. The community pharmacist: Perceived barriers and patient-centered care communication. Int. J. Environ. Res. Public Heal. 2020, 17, 536. [Google Scholar] [CrossRef]
- Illingworth, R. What does ‘patient-centred’ mean in relation to the consultation? Clin. Teach. 2010, 7, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Koster, A.S.; Mantel-Teeuwisse, A.; Woerdenbag, H.J.; Mulder, W.; Wilffert, B.; Schalekamp, T.; Buurma, H.; Wilting, I.; Westein, M. Alignment of CanMEDS-based undergraduate and postgraduate pharmacy curricula in The Netherlands. Pharmacy 2020, 8, 117. [Google Scholar] [CrossRef]
- Wolfe, A. Institute of Medicine Report: Crossing the quality chasm: A new health care system for the 21st century. Policypoliti-Nurs. Pract. 2001, 2, 233–235. [Google Scholar] [CrossRef]
- Mead, N.; Bower, P. Patient-centred consultations and outcomes in primary care: A review of the literature. Patient Educ. Couns. 2002, 48, 51–61. [Google Scholar] [CrossRef]
- Stewart, M.; Brown, J.; Weston, W.; Mcwhinney, I.; McWilliam, C.; Freeman, T. (Eds.) Patient-Centered Medicine: Transforming the Clinical Method, 2nd ed.; Radcliffe Medical Press: Abingdon, UK, 2003. [Google Scholar]
- Wolters, M.; Van Hulten, R.; Blom, L.; Bouvy, M.L. Exploring the concept of patient centred communication for the pharmacy practice. Int. J. Clin. Pharm. 2017, 39, 1145–1156. [Google Scholar] [CrossRef]
- Hyvärinen, M.-L.; Tanskanen, P.; Katajavuori, N.; Isotalus, P. A method for teaching communication in pharmacy in authentic work situations. Commun. Educ. 2010, 59, 124–145. [Google Scholar] [CrossRef]
- Makoul, G. Essential elements of communication in medical encounters: The Kalamazoo consensus statement. Acad. Med. 2001, 76, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Hargie, O.; Morrow, N.C.; Woodman, C. Pharmacists’ evaluation of key communication skills in practice. Patient Educ. Couns. 2000, 39, 61–70. [Google Scholar] [CrossRef]
- Brown, R.F.; Bylund, C.L. Communication skills training: Describing a new conceptual model. Acad. Med. 2008, 83, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Cegala, D.J.; Broz, S.L. Physician communication skills training: A review of theoretical backgrounds, objectives and skills. Med Educ. 2002, 36, 1004–1016. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Silverman, J.D. The Calgary-Cambridge Referenced Observation Guides: An aid to defining the curriculum and organizing the teaching in communication training programmes. Med. Educ. 1996, 30, 83–89. [Google Scholar] [CrossRef]
- Blind, C.S.; Daemen, B.J.G.; Faber, A. Mulder-Wildemors LGM, Meijvis VAM. In KNMP-Richtlijn Consultvoering; KNMP: The Hague, The Netherlands, forthcoming.
- Koster, A.S.; Schalekamp, T.; Meijerman, I. Implementation of Competency-Based Pharmacy Education (CBPE). Pharmacy 2017, 5, 10. [Google Scholar] [CrossRef]
- Biggs, J. Enhancing teaching through constructive alignment. High. Educ. 1996, 32, 347–364. [Google Scholar] [CrossRef]
- Bachmann, C.; Abramovitch, H.; Barbu, C.G.; Cavaco, A.M.; Elorza, R.D.; Haak, R.; Loureiro, E.; Ratajska, A.; Silverman, J.; Winterburn, S.; et al. A European consensus on learning objectives for a core communication curriculum in health care professions. Patient Educ. Couns. 2013, 93, 18–26. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Robinson, J.D.; Persky, A.M. Developing self-directed learners. Am. J. Pharm. Educ. 2020, 84, 847512. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, R.S. Communication skills development in colleges of pharmacy. Am. J. Pharm. Educ. 2001, 65, 307. [Google Scholar]
- Svensberg, K.; Björnsdottir, I.; Wallman, A.; Sporrong, S.K. Nordic pharmacy schools’ experience in communication skills training. Am. J. Pharm. Educ. 2017, 81, 6005. [Google Scholar] [CrossRef] [PubMed]
- Wallman, A.; Vaudan, C.; Sporrong, S.K. Communications training in pharmacy education, 1995–2010. Am. J. Pharm. Educ. 2013, 77, 36. [Google Scholar] [CrossRef] [PubMed]
- Emmanuelle, S.; Chung, E.; Sakharkar, P.; Law, A.V. Instruction and assessment of student communication skills in US and Canadian pharmacy curricula. Curr. Pharm. Teach. Learn. 2013, 5, 508–517. [Google Scholar] [CrossRef]
- Miller, G.E. The assessment of clinical skills/competence/performance. Acad. Med. 1990, 65, S63–S67. [Google Scholar] [CrossRef]
- Cruess, R.L.; Cruess, S.R.; Steinert, Y. Amending Miller’s pyramid to include professional identity formation. Acad. Med. 2016, 91, 180–185. [Google Scholar] [CrossRef]
- Bell, C.; Paterson, J.; Murison, P.; Warman, S.M. How do we learn? InPractice 2014, 36, 153–154. [Google Scholar] [CrossRef]
- Berkhof, M.; van Rijssen, H.J.; Schellart, A.J.; Anema, J.R.; van der Beek Allard, J. Effective training strategies for teaching communication skills to physicians: An overview of systematic reviews. Patient Educ. Couns. 2011, 84, 152–162. [Google Scholar] [CrossRef]
- Van Dalen, J.; Bartholomeus, P.; Kerkhofs, E.; Lulofs, R.; Van Thiel, J.; Rethans, J.J.; Scherpbier, A.J.; Van Der Vleuten, C.P. Teaching and assessing communication skills in Maastricht: The first twenty years. Med. Teach. 2001, 23, 245–251. [Google Scholar] [CrossRef]
- Taylor, P.J.; Russ-Eft, D.F.; Chan, D.W.L. A meta-analytic review of behavior modeling training. J. Appl. Psychol. 2005, 90, 692–709. [Google Scholar] [CrossRef] [PubMed]
- Latham, G.P.; Saari, L.M. Application of social-learning theory to training supervisors through behavioral modeling. J. Appl. Psychol. 1979, 64, 239. [Google Scholar] [CrossRef]
- Schönrock-Adema, J. De Ontwikkeling En Evaluatie Van Een Zelfinstructieprogramma Voor Een Training In Basisgespreksvaar-Digheden. Ph.D. Thesis, Rijksuniversiteit Groningen, Groningen, The Netherlands, 2002. [Google Scholar]
- Jin, H.K.; Choi, J.H.; Kang, J.E.; Rhie, S.J. The effect of communication skills training on patient-pharmacist communication in pharmacy education: A meta-analysis. Adv. Health Sci. Educ. 2018, 23, 633–652. [Google Scholar] [CrossRef]
- Jin, H.K.; Park, S.H.; Kang, J.E.; Choi, K.S.; Kim, H.A.; Jeon, M.S.; Rhie, S.J. The influence of a patient counseling training session on pharmacy students’ self-perceived communication skills, confidence levels, and attitudes about communication skills training. BMC Med. Educ. 2019, 19, 172. [Google Scholar] [CrossRef] [PubMed]
- Kubota, R.; Shibuya, K.; Tanaka, Y.; Aoki, M.; Shiomi, M.; Ando, W.; Otori, K.; Komiyama, T. Clinical pharmacy education in Japan: Using simulated patients in laboratory-based communication-skills training before clinical practice. Pharmacy 2018, 6, 49. [Google Scholar] [CrossRef]
- Rao, D. Skills development using role-play in a first-year pharmacy practice course. Am. J. Pharm. Educ. 2011, 75, 84. [Google Scholar] [CrossRef]
- Blom, L.; Wolters, M.; Hoor-Suykerbuyk, M.T.; Van Paassen, J.; Van Oyen, A. Pharmaceutical education in patient counseling: 20h spread over 6 years? Patient Educ. Couns. 2011, 83, 465–471. [Google Scholar] [CrossRef]
- Gartmeier, M.; Bauer, J.; Fischer, M.R.; Hoppe-Seyler, T.; Karsten, G.; Kiessling, C.; Möller, G.E.; Wiesbeck, A.; Prenzel, M. Fostering professional communication skills of future physicians and teachers: Effects of e-learning with video cases and role-play. Instr. Sci. 2015, 43, 443–462. [Google Scholar] [CrossRef]
- Hess, R.; Hagemeier, N.E.; Blackwelder, R.; Rose, D.; Ansari, N.; Branham, T. Teaching communication skills to medical and pharmacy students through a blended learning course. Am. J. Pharm. Educ. 2016, 80, 64. [Google Scholar] [CrossRef]
- Wolters, M.; Van Paassen, J.G. Pharmacy students appreciate e-learning modules to prepare for communication skills training. In Proceedings of the International Conference on Communication in Healthcare, ICCH, London, UK, 9–11 September 2020. [Google Scholar]
- Rickles, N.M.; Tieu, P.; Myers, L.; Galal, S.; Chung, V. The impact of a standardized patient program on student learning of com-munication skills. Am. J. Pharm. Educ. 2009, 73, 1. [Google Scholar] [CrossRef]
- May, W.; Park, J.H.; Lee, J.P. A ten-year review of the literature on the use of standardized patients in teaching and learning: 1996–2005. Med. Teach. 2009, 31, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, C.; Woermann, U.; Shaha, M.; Rethans, J.J.; van der Vleuten, C. Effects of communication training on real practice per-formance: A role-play module versus a standardized patient module. J. Nurs. Educ. 2012, 51, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.C.; Chen, S.; Chao, S.; Chen, Y. Using standardized patient with immediate feedback and group discussion to teach inter-personal and communication skills to advanced practice nursing students. Nurse Educ. Today 2013, 33, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Bosse, H.M.; Schultz, J.-H.; Nickel, M.; Lutz, T.; Möltner, A.; Jünger, J.; Huwendiek, S.; Nikendei, C. The effect of using standardized patients or peer role play on ratings of undergraduate communication training: A randomized controlled trial. Patient Educ. Couns. 2012, 87, 300–306. [Google Scholar] [CrossRef]
- Gillette, C.; Stanton, R.B.; Anderson, H.G., Jr. Student performance on a knowledge-based exam may predict student ability to communicate effectively with a standardized patient during an objective structured clinical examination. Curr. Pharm. Teach. Learn. 2017, 9, 201–207. [Google Scholar] [CrossRef]
- Newble, D. Techniques for measuring clinical competence: Objective structured clinical examinations. Med. Educ. 2004, 38, 199–203. [Google Scholar] [CrossRef]
- Khan, K.Z.; Ramachandran, S.; Gaunt, K.; Pushkar, P. The objective structured clinical examination (OSCE): AMEE Guide no. 81. Part I: An historical and theoretical perspective. Med. Teach. 2013, 35, e1437–e1446. [Google Scholar] [CrossRef]
- Pell, G.; Fuller, R.; Homer, M.; Roberts, T. How to measure the quality of the OSCE: A review of metrics–AMEE Guide no. 49. Med. Teach. 2010, 32, 802–811. [Google Scholar] [CrossRef]
- Sturpe, D. Objective structured clinical examinations in doctor of Pharmacy programs in the United States. Am. J. Pharm. Educ. 2010, 74, 148. [Google Scholar] [CrossRef]
- Fens, T.; Dantuma-Wering, C.M.; Taxis, K. The pharmacy game-GIMMICS® a simulation game for competency-based education. Pharmacy 2020, 8, 198. [Google Scholar] [CrossRef]
- Watson, M.C.; Bond, C.M.; Grimshaw, J.M.; Johnston, M. Factors predicting the guideline compliant supply (or non-supply) of non-prescription medicines in the community pharmacy setting. BMJ Qual. Saf. 2006, 15, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Sabate, E. Adherence to Long Term Therapies. Evidence to Action, 1st ed.; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Jokanovic, N.; Tan, E.C.; van den Bosch, D.; Kirkpatrick, C.M.; Dooley, M.J.; Bell, J.S. Clinical medication review in Australia: A systematic review. Res. Soc Adm. Pharm. 2016, 12, 384–418. [Google Scholar] [CrossRef]
- Bulajeva, A.; Labberton, L.; Leikola, S.; Pohjanoksa-Mäntylä, M.; Geurts, M.; De Gier, J.; Airaksinen, M. Medication review practices in European countries. Res. Soc. Adm. Pharm. 2014, 10, 731–740. [Google Scholar] [CrossRef]
- Hatah, E.; Braund, R.; Tordoff, J.; Duffull, S.B. A systematic review and meta-analysis of pharmacist-led fee-for-services medication review. Br. J. Clin. Pharmacol. 2014, 77, 102–115. [Google Scholar] [CrossRef]
- Bryant, L.J.; Coster, G.; Gamble, G.D.; McCormick, R.N. The General Practitioner–Pharmacist Collaboration (GPPC) study: A ran-domised controlled trial of clinical medication reviews in community pharmacy. Int. J. Pharm. Pract. 2011, 19, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Burns, A. Medication therapy management in pharmacy practice: Core elements of an MTM service model (version 2.0). J. Am. Pharm. Assoc. 2008, 48, 341–353. [Google Scholar] [CrossRef]
- Blenkinsopp, A.; Bond, C.; Raynor, D.K. Medication reviews. Br. J. Clin. Pharmacol. 2012, 74, 573–580. [Google Scholar] [CrossRef] [PubMed]
- NHG. NHG, en Verzorging, Landelijk Expertisecentrum Verpleging. In Multidisciplinaire Richtlijn Polyfarmacie Bij Ouderen 2012; NHG: Utrecht, The Netherlands, 2012. [Google Scholar]
- Meijer, W.M.; Daemen, B. KNMP-Richtlijn Medicatiebeoordeling; KNMP: The Hague, The Netherlands, 2013. [Google Scholar]
- Miller, W.R.; Rollnick, S. Ten things that motivational interviewing is not. Behav. Cogn. Psychother. 2009, 37, 129–140. [Google Scholar] [CrossRef]
- Lonie, J.M.; Austin, Z.; Nguyen, R.; Gill, I.; Lucas, C. Pharmacist-based health coaching: A new model of pharmacist-patient care. Res. Soc. Adm. Pharm. 2017, 13, 644–652. [Google Scholar] [CrossRef]
- Sisson, E.; Kuhn, C. Pharmacist roles in the management of patients with type 2 diabetes. J. Am. Pharm. Assoc. 2009, 49, S41–S45. [Google Scholar] [CrossRef]


{kind=link}
| Stages | Learning Objective | Teaching/Learning Method | Assessment Method (Formative and Summative) |
|---|---|---|---|
| 1. Knowing what and why | Gaining insight in:
| Self-study:
| Written reflection assignment Written exam |
| 2. Knowing how | Understanding:
| Demonstration by experts (life or video):
| Written reflection assignment Written exam |
| 3. Showing | Demonstrating:
| Small group training:
Formative assessment Video feedback and reflection assignments Simulation pharmacy | Objective Structured Clinical Exam (OSCE) Video-feedback Feedback on roleplay |
| 4. Does | Performing:
| Internships:
| Internship: assessment of learning activities regarding patient centered communication Assessment of student’s portfolio |
| Topic * | Learning Objectives the Student … | Teaching/Learning Activities |
|---|---|---|
| 1. Standard first prescription consultation |
| Two lectures on pharmaceutical care and pharmaceutical consultations Two preparatory e-modules Small group training (12–15 students); practicing with other students led by teacher/practicing pharmacist Workshop (12–15) on applying pharmaceutical knowledge during consultations Formative OSCE Written reflection assignment on the video recordings of the OSCE Practicing with a simulation patient (individually) |
| 2. Standard second prescription consultation |
| One preparatory e-module Small group training (12–15); practicing with other students led by teacher/practicing pharmacist Formative OSCE Written reflection assignment on the video recordings of the OSCE Practicing with a simulation patient (individually) |
| 3. Involving a distracted patient in the consultation, (e.g., absentminded, in a hurry or in pain) |
| One preparatory e-module Small group training (6–8); practicing with a simulation patient led by communication skills trainer Formative OSCE Written reflection assignment on the video recordings of the OSCE Practicing with a simulation patient (individually) |
| 4. Coping with a talkative patient |
| One preparatory e-module Small group training (6–8); practicing with a simulation patient led by communication skills trainer Formative OSCE Written reflection assignment on the video recordings of the OSCE Practicing with a simulation patient (individually) |
| 5. Handling patient’s emotion |
| Two lectures on health psychology and patient centered communication One preparatory e-module Small group training (6–8); practicing with a simulation patient led by communication skills trainer Formative OSCE Practicing with a simulation patient (individually) |
| 6. Addressing (potential) non-compliance |
| One preparatory e-module Small group training (6–8); practicing with a simulation patient led by communication skills trainer Formative OSCE Practicing with a simulation patient (individually) |
| Phase | Content | Continuously throughout the Consultation |
|---|---|---|
| Initiating the consultation | Establishing the relationship Identifying the reasons for the consultation Agenda setting | Building the relationship |
| Gathering information | Exploring patient’s needs and perspective Reaching a shared understanding of the problem | |
| Explanation, advice and decision making | Providing relevant and clear information and advice Shared decision making on management plan | Providing structure |
| Closing the consultation | Enabling self-management Agreement check Follow up |
| Learning Objectives the Student … | Teaching/Learning Activities |
|---|---|
|
|
| Learning Goals the Student… | Teaching/Learning Activities |
|---|---|
| CMR | |
| Introductory lecture on the medication review process Group work introduction on CMR
|
| Patient Interview | |
| Introductory lecture on the structure of the patient interview and necessary competences (recently replaced by an e-module) Small group training (6–8) on the introduction and intake; practicing with a simulation patient led by communication skills trainer Small group training (6–8) on the medication overview, anamnesis and closure; practicing with a simulation patient led by a pharmacist (teacher) Training session: taking a full patient interview
|
| Internship (community pharmacy) year 1
|
| Training session: taking a full patient interview
|
| Discussing the pharmaceutical care plan with the patient | |
| E-module and training session on motivational interviewing (MI) Applied for discussing the treatment plan with the patient Small group training (6–8); practicing with a simulation patient led by a communication skills trainer |
| Internship (community pharmacy) year 3
|
| Phase | Content |
|---|---|
| Introduction | Acquaintance Introduction on the aim, agenda and follow-up |
| Intake * | Open interview on patient’s personal situation, their experience with diseases and medication, preferences, questions and problems |
| Medication overview * | Patient explains how they use their medication on an average day (giving insight in self-management, practical problems and medication adherence) |
| Anamnesis * | Structured interview on specific topics to get a full understanding of the biomedical situation of the patient (medical condition, usage, effect and side effects of medication) |
| Closure | Summarizing the identified problems and questions Explaining follow-up |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolters, M.; van Paassen, J.G.; Minjon, L.; Hempenius, M.; Blokzijl, M.-R.; Blom, L. Design of a Pharmacy Curriculum on Patient Centered Communication Skills. Pharmacy 2021, 9, 22. https://doi.org/10.3390/pharmacy9010022
Wolters M, van Paassen JG, Minjon L, Hempenius M, Blokzijl M-R, Blom L. Design of a Pharmacy Curriculum on Patient Centered Communication Skills. Pharmacy. 2021; 9(1):22. https://doi.org/10.3390/pharmacy9010022
Chicago/Turabian StyleWolters, Majanne, Jacqueline G. van Paassen, Lenneke Minjon, Mirjam Hempenius, Marie-Rose Blokzijl, and Lyda Blom. 2021. "Design of a Pharmacy Curriculum on Patient Centered Communication Skills" Pharmacy 9, no. 1: 22. https://doi.org/10.3390/pharmacy9010022
APA StyleWolters, M., van Paassen, J. G., Minjon, L., Hempenius, M., Blokzijl, M.-R., & Blom, L. (2021). Design of a Pharmacy Curriculum on Patient Centered Communication Skills. Pharmacy, 9(1), 22. https://doi.org/10.3390/pharmacy9010022