Abstract
In this article the design of three master programs (MSc in Pharmacy) and two postgraduate specialization programs for community or hospital pharmacist is described. After a preceding BSc in Pharmacy, these programs cover the full pharmacy education capacity for pharmacists in primary and secondary health care in the Netherlands. All programs use the CanMEDS framework, adapted to pharmacy education and specialization, which facilitates the horizontal integration of pharmacists’ professional development with other health care professions in the country. Moreover, it is illustrated that crossing the boundary from formal (university) education to experiential (workplace) education is eased by a gradual change in time spent in these two educational environments and by the use of comparable monitoring, feedback, and authentic assessment instruments. A reflection on the curricula, based on the principles of the Integrative Pedagogy Model and the Self-determination Theory, suggests that the alignment of these educational programs facilitates the development of professional expertise and professional identity of Dutch pharmacists.
1. Introduction
During the last few years of university training and the beginning of professional life pharmacy students have to make the transition from formal “academic” learning to practical “experiential” learning. At the same time, they have to develop professional expertise and a professional identity. This “boundary crossing” process can be complex [1,2]. Students must take increasing responsibility for their own learning, and the role of teachers becomes more and more facilitating, supporting, guiding, and coaching [3,4]. The nature of assessment (in a broad sense) is different: An important function of assessment is to provide students with feedback on their own learning (self-monitoring, assessment-for-learning) [5]. Frequently the same assessment results can be used for summative evaluation of student or trainee performance (assessment-of-learning) and for high-stakes decisions related to declaring a student or trainee “competent” [6]. At the end of this process the student/trainee is expected to be a reflective, self-directed pharmacy practitioner that is committed to life-long learning, is well-embedded in a professional “culture”, and that can bear independent responsibility for pharmaceutical patient care, in collaboration with patients and with other health care professionals [7,8].
Experiential learning has several characteristics that are different from academic learning. Tynjälä describes that “Informal workplace learning is unplanned and implicit, often collaborative and highly contextualised, and the learning outcomes unpredictable, whereas school learning and organized on-the-job training is often formal, planned, largely explicit, focused on individual learning, and the outcomes are often predictable” (ref. [9], p. 133). The tension between science-based and experience-based knowledge is also described by Waterfield [10] for pharmacy education. It is concluded that a close integration of science and practice is needed in pharmacy education [7]. Formal education is needed to obtain and develop generic skills that can be applied in various contexts, but in order to become a true expert a student has to develop situation-specific forms of competence, which only is possible in authentic learning environments.
In the Integrated Pedagogy Model [9] three elements are considered essential for the development of professional expertise: theoretical/conceptual knowledge, practical/experiential knowledge, and self-regulatory knowledge. The development of professional expertise is seen as a process where theory cannot be separated from practice, and where practice cannot be separated from theory. Self-regulatory knowledge is needed to continuously reflect on the differences between both types of knowledge and to help in transforming theoretical knowledge into practical applications and to conceptualize practical experiences in terms of underlying concepts (Figure 1; see also ref. [11]). Several studies have described design principles for study programs that foster the development of self-directed and self-regulated learning at the boundary between higher education and work [12,13]. More explicitly, Elvira et al. [14]—based on the Integrated Pedagogy Model and an integrative literature review—have defined ten design principles, which support and foster the development of professional expertise [15]. These instructional principles are intended to facilitate transformation of theoretical/conceptual knowledge into practical/experiential knowledge (and vice versa) and to stimulate the use of self-regulation for reflecting on both practical and conceptual knowledge. Further details are given below (see Table 4).
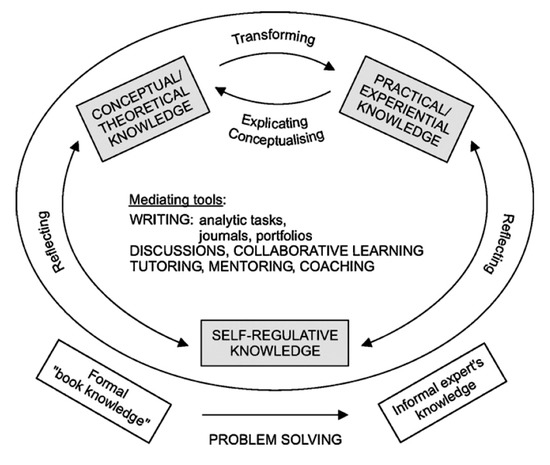
Figure 1.
A model for development of professional expertise. Taken from ref. [9], with permission (nr. 4838831338331).
In addition to developing professional expertise the student or trainee is expected to be (and remain) motivated to become an expert and to develop professional identity. This is consistent with the societal expectations of the profession [7] and is reflected in competency-based frameworks such as CanMEDS. It has been suggested that the Self-determination Theory (SDT; ref. [16]) can be used to monitor the motivation of pharmacy students to develop their professional identity [17]. Recent studies have indeed shown that the SDT can be applied to monitor how motivation of practicing pharmacists [18] and pharmacist trainees (Westein et al., unpublished) is influenced by personal and workplace-dependent factors.
In this article we will examine the design of three different master programs and two postgraduate specializations (community pharmacist and hospital pharmacist) from the Dutch context through the lenses of the Integrated Pedagogy Model and the Self-determination Theory. We intend to illustrate how the design of these curricula, which are all based on an adapted CanMEDS framework, attempts to contribute optimally to the required development of professional expertise and identity.
2. Context: CanMEDS and The Dutch National Framework
Pharmaceutical health care in the Netherlands (17.4 million inhabitants) is provided in 1996 community pharmacies and 79 hospital pharmacies (including 8 academic hospitals). Community pharmacies are relatively large organizations and employ on average 1.6 pharmacists, 5.5 pharmacy technicians and 2.1 support personnel (year 2016, expressed as full-time equivalents, ref. [19]). Pharmacy technicians are involved in dispensing and patient counseling, under the pharmacists’ responsibility. Hospital pharmacies are even larger organizations and employ on average 10 pharmacists and 50 pharmacy technicians. A total of 2887 pharmacists work in a community pharmacy and 880 in a hospital pharmacy in 2019 [20,21].
Pharmacy education has a long tradition in the Netherlands. In addition to university degrees (BSc in Pharmacy and MSc in Pharmacy), two postgraduate specializations have been developed for the field of primary patient care (community pharmacy; since 1995) and secondary patient care (hospital pharmacy; since 1986). Gradual development of these programs has resulted in legal recognition of the “hospital pharmacist” specialization and the “community pharmacist” specialization in 1999 and 2016, respectively (Figure 2).
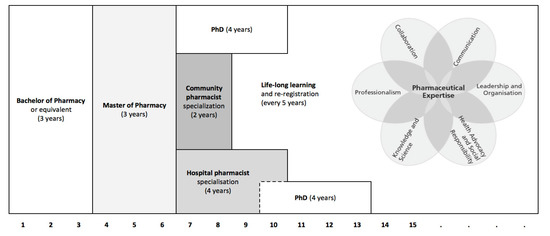
Figure 2.
Dutch Pharmacy education. The curricula described in this article all use the CanMEDS model as a structuring principle. In this model professional competence is described in terms of the seven roles of Pharmaceutical expert, Communicator, Collaborator, Scholar, Health advocate, Leader and Professional.
In 2005 the medical professions in the Netherlands adopted the CanMEDS model as a suitable framework to conceptualise educational programs for a diversity of medical specializations [22]. The CanMEDS model was also introduced as a basis for the updated versions of the hospital [23] and community [24] specialization programs (Table 1).

Table 1.
Required competency levels at the end of the master program.
In 2016 two documents were published, both commissioned by the Dutch pharmacy departments in cooperation with the Royal Dutch Society of Pharmacy. The Domain-specific Frame of Reference for Pharmacy in the Netherlands describes the knowledge domain of pharmacy, the present and future developments in pharmacy, and defines the general tasks and responsibilities of the pharmacist. Moreover, it addresses the complementarity with physicians and the specific responsibilities of the pharmacist in pharmacotherapeutic treatment [25]. The Competency Framework (Table 1) specifies the required learning outcomes for pharmacists graduated from Dutch universities. The purpose of this framework was to guarantee the professional level of a starting pharmacist and to align the university’s bachelor and master degrees with the existing specialization programs in addition to being a future-proof framework that is in alignment with international developments [26,27] and the requirements of the Dutch law (Dutch Individual Healthcare Professions Act, BIG). In the European context it is, furthermore, required that during an undergraduate pharmacy program with a minimum duration of five years at least 26 weeks are spent in hospital and/or community pharmacies (EU directive 2005/36/CE; ref. [28]).
The CanMEDS model (Figure 2) distinguishes seven competency domains, which can be described as the roles of Pharmaceutical expert, Communicator, Collaborator, Scholar, Health advocate, Leader and Professional (see Table 1). Together, these roles cover the areas of responsibility in existing and future pharmacy practice (Product care, Patient care, Medication policy, Quality assurance and Research, education and innovation) as defined by the Dutch Individual Healthcare Professions Act (BIG). In the Competency Framework the competence level, required at the end of the master program, is defined for all competencies in terms of student independence and guidance by a supervisor (Table 1). For 92 out of 140 competencies the framework specifies that a graduated pharmacist “is expected to be able to adequately carry out professional activities in an authentic professional situation […] under supervision of an experienced pharmacy practitioner” (level V). This requirement particularly relates to the CanMEDS domains Pharmaceutical expert and Communication (see Table 1). In other CanMEDS domains (e.g., Interprofessional collaboration, Scientific research and Leadership) it is considered acceptable that recent graduates can function at a lower level of competency, requiring a more intensified level of guidance and/or supervision by experienced colleagues. Competence as such cannot be measured, but can be approached by assessment of behavioral proxies. Usually competencies have to be broken down in their constituent elements in the domains of knowledge, skills, and behaviour to be able to directly assess whether a student or trainee has mastered a particular competency (see ref. [29] for more details). Consequently, a variety of different assessment formats, suitable for assessing performance in authentic learning or training situations have been developed over the past decades (see Section 6 below and ref. [30]). More recently, the concept of Entrustable Professional Activities (EPAs; refs. [27,28]) has been introduced to structure training and assessments in competency-based medical education around those activities that are characteristic for the later professional life of a student or trainee. EPAs also are being considered as tools for structuring training and assessment of pharmacy students at the border between university and working life [29,30] and the use of EPAs has in fact been introduced in 2012 in the specialization program for community pharmacists in the Netherlands [31]. Currently the concept of EPAs is also being introduced as the backbone of the training program of hospital pharmacists.
3. Implementation of Pre- and Postgraduate Education
Translation of a set of required competencies into a curriculum is complicated [29,31]. Designing teaching/learning activities, feedback formats, and assessment tasks requires the adoption of an explicit model of student cognitive development [4,29,32] and alignment of all elements of the curriculum [33]. Mapping of the curriculum elements (teaching/learning tasks, internships, feedback formats, assessments, teacher, and preceptor roles) on a competency framework [34,35] can be helpful in identifying gaps, overlaps, omissions, and duplicates in the designed curriculum [36,37,38] and making comparisons between the experienced curriculum and the designed curriculum can be helpful in optimizing a curriculum [35,39]. Usually several rounds of internal and external reviews (visitation, accreditation) are required to arrive at an effective and efficient curriculum [29]. The curricula, described in this article, have gone through several rounds of internal and external review, either as part of a formal accreditation process by the Accreditation Organization of the Netherlands and Flanders NVAO (the master programs) or as part of internal reviews by professional organizations (Dutch Association of Hospital Pharmacists NVZA and Royal Dutch Pharmacists Association KNMP; see ref. [40]).
4. Three Different Master Programmes
Three universities in the Netherlands have a long tradition in carrying out pharmaceutical research and offering pharmacy training. In this article we will only discuss the 3-year Master in Pharmacy (MSc. Pharmacy) programs, but it should be noted that the same universities also offer undergraduate 3-year bachelor programs in pharmacy and pharmaceutical sciences (see endnote A). In September 2019 the annual intake of new students for the three master programs was 85, 140, and 50 in Groningen, Utrecht, and Leiden, respectively. In the Netherlands a license to work as a legally recognized pharmacist (Dutch Individual Health Professions Act) is automatically obtained with the master degree, followed by registration in the so-called BIG-register.
Because all programs are based on a common competency framework (see above), they inevitably have common characteristics. However, at a first glance the curriculum structure appears very different (Figure 3). It can also be seen that the requirement of the European Union that at least 26 weeks are spent in a community and/or hospital pharmacy during the undergraduate training (EU-directive 2005/36/CE, ref. [28]), is implemented differently in the three programs.
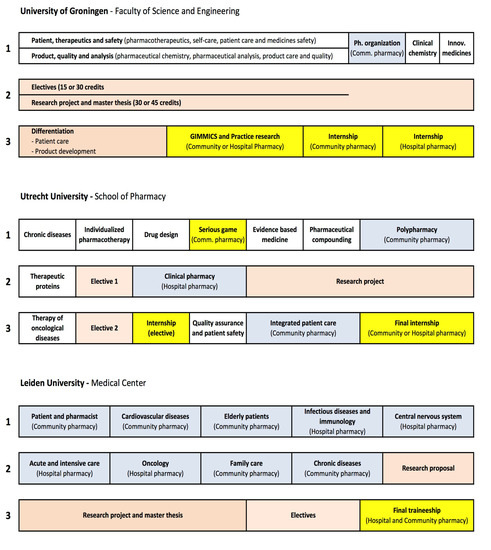
Figure 3.
Three different master programs. All programs last three years (indicated as 1, 2, 3), during 40 weeks every year (left to right in the schemes). Colors indicate structured courses (white; obligatory for all students), individual subjects/electives (salmon), experiential internships (blue; 50–60% workplace) and full-time internships (yellow; at least 80% workplace).
The differences in curriculum structure partly represents historical developments. In Leiden a fundamental choice for introducing “experiential learning” was made recently (see endnote B) and this has resulted in a curriculum, where workplace learning is combined with formal learning to a large extent. In this system most teaching activities are organized around thematically organized experiential internships in a community or hospital pharmacy (e.g., Patient and pharmacist, Cardiovascular diseases). During a typical course, around 50–60% of the students’ time is spent in a pharmacy, the remainder being used for classroom meetings involving small-scale education and dedicated trainings. In Utrecht a similar course design is used for a large part of the required internships (Polypharmacy, Clinical pharmacy and Integrated patient care), while in Groningen this set-up is used for the introductory internship in year-1 (Pharmacy organization). Full-time internships, where more than 80% of the students’ time is spent at the workplace, usually are scheduled in the last year of the master programs (yellow colour in Figure 3). In Groningen and Utrecht serious gaming is used as an initial confrontation and training with the day-to-day complexities of pharmaceutical practice. In the pharmacy game Gimmics® (Groningen Institute Model for Management in Care Services; Groningen, The Netherlands) groups of 5–8 students in their final year, have to organize and run a simulated community pharmacy [41]. In Utrecht a similar set up is used in the first master year.
Article 44 of the EU-directive stipulates that the total duration of undergraduate education must be at least five years. Within Europe the Netherlands is exceptional in having a 6-year academic pharmacy program (i.e., a three-year bachelor and three-year master), as required by Dutch law. The scientific nature of the programs is emphasised by requiring that each student carries out an independent research project during one semester (see Figure 3). Together with a wide choice of electives this gives students the opportunity to follow a path of preference towards a more patient-oriented or product-oriented study program by choosing courses and research topics in different research departments within the same or other universities in the Netherlands or abroad. Only the University of Groningen recognizes a formal (but limited) “differentiation” between a Patient care and a Product development trajectory. Elective internships in pharmaceutical industries or regulatory authorities are allowed in all master programs, but no formal specializations are recognized within the master diploma. In general, students have a wide range of options to shape their own profile (at least 1/3 of their total master program). They have to be proactive in planning their own study program and in making arrangements with their research departments and study coordinators. Therefore, the trajectory of study of an individual student can differ considerably from the scheme in Figure 3, beyond the compulsory elements of the programs.
Part of the programs in Groningen and Utrecht consists of courses, which are obligatory for all students (white colour in Figure 3). In Utrecht these courses all last five weeks (full time) and are organized around relevant themes (e.g., Chronic diseases, Individualized pharmacotherapy and Drug design; see Figure 3). In Groningen disciplinary courses are organized under two large themes, Patient, therapeutics and safety (which includes general pharmacotherapeutics, self-care, patient care and medicines safety), and Product, quality and analysis (which includes pharmaceutical chemistry, pharmaceutical analysis, product care and quality). The students follow these courses in the first year of the master program.
5. Two Postgraduate Specializations
The two postgraduate specializations, for community pharmacist and hospital pharmacist, have similar characteristics (Table 2). Both programs are workplace based. Trainees, which are registered as pharmacists, are employed by a pharmacy or hospital and are further trained under the guidance of experienced colleagues. The main difference between the two programs is duration (two years versus four years), the number of training locations (one versus two) and the possibility for differentiation within the program. In the community pharmacist specialization program differentiation is limited to individual research projects, while in the hospital pharmacist specialization program trainees are expected to follow an individual differentiation, which is characterized by a research project in combination with science training courses (see endnote C). Some trainees in the hospital training continue into a formal PhD trajectory following their research project and after obtaining their registration as a hospital pharmacist (Figure 2). Alternatively, training for hospital or community pharmacist can start after finishing a PhD project.
Table 2.
Characteristics of the postgraduate specializations.
In addition to workplace-based training, centralized courses are organized for all trainees. For trainees in the community pharmacist specialization program, courses on ethics, leadership, management skills, and relevant aspects of product care and pharmacotherapy are organized. Centralized courses for trainees in the hospital pharmacist specialization program in year-1 are generic and expand on pharmaceutical product knowledge, pharmacotherapeutic topics, toxicology and management aspects of the master programs. In year-2 to -4 specific courses in the area of differentiation (e.g., neurology, oncology, psychiatry, pharmacovigilance, research methodology) can be followed. In addition to contributing to specialised knowledge and skills, these centralized courses also contribute to the development of a community-of-practice because the trainees will follow these courses together with colleagues from other training locations.
Not all pharmacists in the Netherlands choose to specialize as either community or hospital pharmacist. After obtaining their master degree, and registration in the BIG-register, they are entitled to work in any position which requires a pharmacists’ license. Pharmacists working in education, regulatory or industrial positions often become specialized as well by specific research and or dedicated training programs.
6. Feedback, Assessment, and Monitoring
Competency-based education requires that skills are assessed on a regular basis, in addition to knowledge, to identify existing gaps in knowledge and to establish professional growth. Moreover, it is required that students will frequently receive feedback on their performance in authentic assessment situations [29,30]. Preferably a wide range of assessment types is used, which are not limited to the lower levels of Miller’s pyramid (“knows” and “knows how”; ref. [42]). Giving feedback on the higher levels “shows how” and “does” in authentic learning situations becomes increasingly important as students progress in the program(s). Recent literature reviews [30,43] have analysed the validity and reliability of various assessment formats, and these authors conclude that various workplace-based assessment formats have great potential in competency-based education (see Table 3).
Table 3.
Authentic feedback and assessment formats.
Short practice observations (SPO), Directly observed preparation skills (DOPS), Case-based discussions (CBD), Critical appraisals of topics (CAT), and Multisource feedback (MSF), when used in real working situations, are highly authentic and have reasonable validity and reliability [30]. Most of these assessment formats can be adapted to (simulated) learning or training situations at the expense of full authenticity, which makes them suitable for use in earlier stages of student development, e.g., during the master program. The use of Objective structured clinical examinations (OSCE) is relatively well investigated [44,45].
In the master programs in Groningen, Utrecht and Leiden the CBD- and SPO- formats are used frequently for assessment, in addition to conventional multiple-choice and written (closed book or open book) exams; the OSCE-format is used to a limited extent. In almost all courses or internships a combination of various testing formats aims for a balanced assessment of knowledge, skills, and actual performance of students. Assessment in a typical course may consist of a diagnostic test at the start, a mid-course exam, an end-course written exam (with essay-questions) and assessment of patient-consulting or compounding skills with CBD-, SPO-, or DOPS-formats. All universities require that the relationship between intended learning outcomes and assessment formats in individual courses be described in an integrated assessment plan for the program. The integrated assessment plans of the three master-programs were evaluated as “sufficient” or “good” in a recent external evaluation by the Accreditation Organization of the Netherlands and Flanders (2019).
In the two postgraduate specializations, authentic assessment formats are the main feedback and assessment tools used. In addition, MSF is used as an instrument in both programs (see Table 2 for details). In the community pharmacist specialization program the format chosen is dependent on the Entrustable professional activity (EPA) being assessed [40]; in 2021 EPAs and Entrustment-based discussions (EBD, ref. [48]) will also be introduced in the hospital pharmacist specialization program as organizing principles.
In the three master programs and the specializations programs electronic portfolios (EPASS®, Mateum BV, Born, The Netherlands; Scorion®, Parantion Groep BV, Deventer, The Netherlands; or otherwise) are used as monitoring instruments. The results of required assessments and evaluations (Table 3) are recorded in an organized and traceable way for use in performance evaluations. In addition, the portfolio is used to collect individual work, personal development plans and reflection documents of students/trainees [57]. The portfolio is primarily maintained by the student/trainee, but supervisors and/or assessors are allowed to add feedback and performance evaluations. The portfolio functions as a central repository to record the competence development of the student or trainee. Integrated feedback on the competence development of a student or trainee is given in the form of Formative performance evaluations (FPE), where the functioning of a student/trainee in a work environment is evaluated on a regular basis (see Table 3). The results of other assessment formats, usually collected in the students/trainees’ portfolio, function as input for the FPE and the result is described in terms of the seven CanMEDS roles Pharmaceutical expert, Communicator, Collaborator, Scholar, Health advocate, Leader, and Professional (Figure 1 and Table 1). In the specialization programs for community and hospital pharmacist FPEs are used on a regular basis as a feedback and monitoring tool (every three months). In the master program of Utrecht University the FPE is used as an assessment tool during the internships in hospital and community pharmacies, while in Leiden FPEs are used in all experiential internships.
Performance evaluations can be used also as a basis for high-stakes decisions [6,56]. In the specialization programs these so-called Summative performance evaluations (SPE) are used to decide after one year whether a trainee is suitable for continuing with the program (intermediate SPE) and to decide at the end of the program whether the trainee can be registered as a community or hospital pharmacist specialist (final SPE; see Table 2).
7. Common Design Principles
Constructing an effective competency-based educational program requires a careful design, where all elements are aligned with each other both horizontally and longitudinally [58,59,60]. Horizontal integration means that disciplinary knowledge and disciplinary-specific skills become integrated in curriculum elements (courses, etc.). It is advised that integration increases gradually and that student assignments and tasks increase in complexity as the curriculum progresses [29,59]. In the presently described curricula different ways of integrating disciplinary content can be recognized (Figure 3). The first year of the master program of the University of Groningen consists of disciplinary courses, but these courses are scheduled under two overarching themes (Patient, therapeutics and safety and Product, quality and analysis, respectively) to facilitate integration of disciplinary knowledge and skills. Another way of integrating knowledge is by organizing courses around themes (rather than disciplines), which is illustrated by courses on Innovative medicines (Groningen, year 1) and many courses in the program of Utrecht University (e.g., Chronic diseases and Quality assurance and patient safety) and Leiden University.
Two other important aspect of a curriculum design are the progressive integration of content and skills across disciplines [29,59] and the transition from formal learning to experiential learning [9] as the curriculum progresses. In the described master programs training of skills starts in individual courses without having a direct connection with a working environment (e.g., a patient interview training in the course Chronic diseases of Utrecht University). In the experiential internships (indicated by the blue color in Figure 3) knowledge and skills are brought close to each other because students spend half of their time in a pharmacy environment, the remainder being spent in the university. A direct confrontation between conceptual ways of learning (university) and experiential ways of learning (pharmacy) is intended to stimulate the development of self-regulated learning [9,12]. A next step to experiential learning is made, when a student is spending most of the time in a pharmacy during the internships at the end of the master program (indicated by the yellow colour in Figure 3). In the specialization programs trainees are no longer considered “students”; they are employed as legally recognized pharmacists and will have responsibilities in important professional domains, be it under supervision of senior colleagues (Table 1). The work-based environment of the specialization programs for hospital or community pharmacist contributes importantly to the building of practical experience and to the elaboration of specialised knowledge and skills.
During the curricula described in this article the students/trainees typically progress from “advanced beginner” to “proficient” expertise; they are considered “competent” at the boundary between university education and specialization [15]. As the curriculum progresses the role of teachers is expected to change considerably [3]. At the beginning of the master program teachers will have considerably more knowledge and better skills than their students; at the end of a specialization program trainees will have become colleagues of their former teachers. For the teachers this means a shift from “knowledge provider” to “coach” and “critical friend”. In a recent systematic review commitment to teaching, role modelling, and encouragement of self-directed learning were identified as the three main competences for teachers/preceptors in advanced pharmacy practice education, in addition to having the knowledge and skills, relevant for their area of clinical work [61]. It is clear, therefore, that also teachers and supervisors, need to be able to “cross borders” between their pharmacy profession and their student/trainee guidance role on a regular basis. Teachers and supervisor in the specialization programs, described in this paper, are prepared for their role by regular training activities (Table 2). Selection and training of supervisors for the community pharmacist specialization program is guided by an explicit Comprehensive pharmacist supervisor competence profile [24], which forms the basis for a two-day training program.
Development of professional expertise not only takes time, but also requires specific training and coaching trajectories [9,15]. Several teaching and learning principles for effective development of expertise can be derived from the educational research literature [9,14]. The Integrated Pedagogy Model [9] posits that self-directed and self-regulated learning at the boundary between higher education and work is best developed when theoretical/conceptual knowledge and practical/experiential knowledge are confronted with each other and when self-regulation is used to reflect effectively on the differences between both types of knowledge. Based on this model, ten educational design principles, which are considered effective for transforming conceptual knowledge into experiential knowledge (design principles 1–5; see Table 4), for explicating experiential knowledge into conceptual knowledge (design principles 6 and 7) and for reflecting on practical and conceptual knowledge by using self-regulative knowledge (design principles 8–10) have been formulated [14]. In Table 4 it is illustrated how these principles are implemented in the master and specialization programs, described in this article. It can be seen that the major curriculum characteristics (courses, internships, assessment and monitoring tools) potentially facilitate the development of professional expertise. Nevertheless, a deeper level of analysis at the level of teaching/learning activities and teacher roles is required to evaluate whether the full potential of the curricula in this respect is reached. This is, however, beyond the scope of this article.
Table 4.
Curriculum elements contributing to professional expertise and identity formation.
Formation of professional identity is strongly dependent on the experience of students/trainees during their internship placements [1,63]. Being a member of both learning communities (university and workplace) during prolonged time is considered to be essential for crossing the boundary between formal education and workplace-based learning and for the development of a context-specific professional identity [9,14,63]. Being able to observe how positive role models function in the working environment [2] and being exposed to purposeful and relevant learning activities [64] also contribute to the formation of a professional identity. In terms of the Self-determination Theory [16,17] the motivation of trainees to develop a professional identity depends on fulfilment of their basic psychological needs to experience competence, autonomy and relatedness (see Table 4). In the curricula, described in this paper, the gradual development of competence is structurally addressed by giving feedback based on the CanMEDS competency framework, which attends to competence development in all domains of professional life (see Table 1). By offering individual practice-oriented and/or research projects and differentiation options within the educational programs the need for autonomy is also addressed. The development of relatedness is facilitated by structuring teaching–learning activities as group efforts (collaborative or cooperative formats) with fellow students/trainees and by frequent interactions between students/trainees and their supervisors in feedback activities (see Table 4 for details).
8. Conclusions
In the Netherlands the undergraduate programs (MSc. Pharmacy) and the postgraduate specializations for hospital or community pharmacist use the CanMEDS model as a backbone. The CanMEDS competencies have been adapted from medical expertise to the development of pharmaceutical expertise. Using the same framework facilitates the alignment of the different programs with each other and enables interaction with other health care professional education programs, such as the programs for medical specialists [22], including general practitioners [65]. This article also illustrates that the structure of three master programs at a first glance may seem different, even though they are based on the same framework. Furthermore, it is shown that crossing the boundary between formal (university) learning and experiential (workplace) learning is eased by applying common design principles, both in the use of teaching–learning activities and in the use of assessment procedures. A gradual integration of disciplinary content, integration of skills with content, increasing complexity of assignments/problems, and a gradual change in the time spent in the formal and experiential learning environments are supposed to “blur” the boundary between university education and professional life. By making a comparison with established theoretical models for the development of professional expertise and professional identity it is shown that all programs contain design elements that are supposed to contribute to these two important aspects of the professional life of a community or hospital pharmacist.
Endnotes
- BSc. Pharmacy programs are available in Groningen and Utrecht and separate programs in pharmaceutical sciences are offered in Utrecht (College of Pharmaceutical Sciences) and Leiden (BSc. Biopharmaceutical Sciences). Master programs in pharmaceutical sciences are available in Groningen (MSc. Medical Pharmaceutical Sciences), Utrecht (MSc. Drug Innovation) and Leiden (MSc. Biopharmaceutical Sciences).
- This program started in 2016 after a more traditional pharmacy program was discontinued in 1985 following a decision of the Dutch government.
- Trainees have to choose between a formal training program in Epidemiology, Clinical pharmacology or Clinical toxicology, a differentiation in the area of compounding, radiopharmacy or laboratory sciences, or a pharmacotherapeutic differentiation in clinical areas such as geriatrics, infectious diseases, intensive care, oncology, pediatrics or psychiatry. The differentiation is described in a personal development plan, which needs to be accepted by the Specialist Registration Commission.
Author Contributions
A.S.K. conceived and wrote a first version of the article. The other authors provided many details about the national framework (T.S., M.P.D.W.), the master programs (H.J.W., B.W., W.M.C.M., A.K.M.-T.) and the specialization programs (I.W., H.B., M.P.D.W.). All authors commented on the draft versions and agreed to the content of the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mylrea, M.F.; Sen Gupta, T.; Glass, B.D. Commencing and Graduating Pharmacy Students’ Perceptions of their Professional Development during Undergraduate Study. Pharm. Educ. 2018, 18, 259–267. [Google Scholar]
- Noble, C.; Coombes, I.; Nissen, L.; Shaw, P.N.; Clavarino, A. Making the Transition from Student to Pharmacist: Australian Interns’ Perceptions of Professional Identity Formation. Int. J. Pharm. Pract. 2015, 23, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Amirfar, V.A.; Chen, A.M.H.; Haley, J.C. Mentoring Plays a Critical Role in Pharmacy Education. J. Am. Pharm. Assoc. 2014, 54, 465–466. [Google Scholar]
- Parojcic, J. Experiential Education for Clinical Pharmacists. Encycl. Pharm. Pract. Clin. Pharm. 2019, 3B, 98–109. [Google Scholar]
- Watling, C.J.; Ginsburg, S. Assessment, Feedback and the Alchemy of Learning. Med. Educ. 2018. [Google Scholar] [CrossRef] [PubMed]
- Van Der Vleuten, C.P.M.; Schuwirth, L.W.T.; Driessen, E.W.; Dijkstra, J.; Tigelaar, D.; Baartman, L.K.J.; Van Tartwijk, J. A Model for Programmatic Assessment Fit for Purpose. Med. Teach. 2012, 34, 205–214. [Google Scholar] [CrossRef]
- Edwards, D.J. Professional Identity Formation: A Shared Responsibility for Academia and Pharmacists. Can. Pharm. J. 2020, 153, 18–20. [Google Scholar] [CrossRef]
- Van Mil, J.W.F.; Schulz, M.; Tromp, T.F.J. Pharmaceutical Care, European Developments in Concepts, Implementation, Teaching, and Research: A Review. Pharm. World Sci. 2004, 26, 303–311. [Google Scholar] [CrossRef]
- Tynjälä, P. Perspectives into Learning at the Workplace. Educ. Res. Rev. 2008, 3, 130–154. [Google Scholar] [CrossRef]
- Waterfield, J. Is Pharmacy a Knowledge-Based Profession? Am. J. Pharm. Educ. 2010, 74, 50. [Google Scholar] [CrossRef]
- Robinson, J.D.; Persky, A.M. Developing Self-Directed Learners. Am. J. Pharm. Educ. 2020, 84, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Jossberger, H.; Brand-Gruwel, S.; Boshuizen, H.; van de Wiel, M. The Challenge of Self-Directed and Self-Regulated Learning in Vocational Education: A Theoretical Analysis and Synthesis of Requirements. J. Voc. Educ. Train. 2010, 62, 415–440. [Google Scholar] [CrossRef]
- Cremers, P.H.M.; Wals, A.E.J.; Wesselink, R.; Mulder, M. Design Principles for Hybrid Learning Configurations at the Interface between School and Workplace. Learn. Environ. Res. 2016, 19, 309–334. [Google Scholar] [CrossRef]
- Elvira, Q.; Imants, J.; Dankbaar, B.; Segers, M. Designing Education for Professional Expertise Development. Scand. J. Educ. Res. 2017, 6, 187–204. [Google Scholar] [CrossRef]
- Persky, A.M.; Robinson, J.D. Moving from Novice to Expertise and its Implications for Instruction. Am. J. Pharm. Educ. 2017, 81, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Kusurkar, R.A.; Ten Cate, T.J.; Van Asperen, M.; Croiset, G. Motivation as an Independent and a Dependent Variable in Medical Education: A Review of the Literature. Med. Teach. 2011, 33, e242–e262. [Google Scholar] [CrossRef]
- Mylrea, M.F.; Sen Gupta, T.; Glass, B.D. Developing Professional Identity in Undergraduate Pharmacy Students: A Role for Self-Determination Theory. Pharmacy 2017, 5, 16. [Google Scholar] [CrossRef]
- Tjin, A.; Tsoi, S.L.N.M.; de Boer, A.; Croiset, G.; Koster, A.S.; Kusurkar, R.A. Factors Influencing Participation in Continuing Professional Development: A Focus on Motivation among Pharmacists. J. Cont. Educ. Health Prof. 2016, 36, 144–150. [Google Scholar] [CrossRef]
- SFK. “Facts and Figures 2017 on Pharmaceutical Care in the Netherlands 2016.” Stichting Farmaceutische Kengetallen. Available online: https://www.sfk.nl/english/facts-and-figures-2017 (accessed on 14 May 2020).
- KNMP. Jaarverslag SRC-OF 2019 (in Dutch). Available online: https://www.knmp.nl/downloads/jaarverslag-2019-src-of.pdf/at_download/file (accessed on 14 May 2020).
- KNMP. Jaarverslag RSC-ZF 2019 (in Dutch). Available online: https://www.knmp.nl/downloads/jaarverslag-src-zf-2019.pdf/at_download/file (accessed on 14 May 2020).
- Scheele, F.; Teunissen, P.; Luijk, S.V.; Heineman, E.; Fluit, L.; Mulder, H.; Meininger, A.; Wijnen-Meijer, M.; Glas, G.; Sluiter, H.; et al. Introducing Competency-Based Postgraduate Medical Education in the Netherlands. Med. Teach. 2008, 30, 248–253. [Google Scholar] [CrossRef]
- NVZA. ELOZ III, Landelijk Opleidingsplan Voor De Opleiding Tot Ziekenhuisapotheker (National Training Plan for Hospital Pharmacist). NVZA (Dutch Association of Hospital Pharmacists). Available online: https://www.knmp.nl/downloads/eloz-iii-052019.pdf/view (accessed on 11 April 2020).
- KNMP. Education Plan Advanced Community Pharmacist Education Programme. KNMP (Royal Dutch Pharmacists Association). Available online: https://www.knmp.nl/downloads/OpleidingsprogrammaENGMarnix.pdf/view (accessed on 11 April 2020).
- Schalekamp, T.; Haisma, H.J. Domain-Specific Frame of Reference for Pharmacy in the Netherlands and 2016-Pharmacist Competency Framework. The Hague: KNMP (Royal Dutch Pharmacists Association). 2012. Available online: www.Knmp.Nl/Downloads/Pharmacist-Competency-frameworkandDSFR-Netherlands.Pdf (accessed on 11 April 2020).
- FIP. Pharmacy Education Taskforce—A Global Competency Framework. International Pharmaceutical Federation (FIP). Available online: https://www.fip.org/files/fip/PharmacyEducation/GbCF_v1.pdf (accessed on 11 April 2020).
- Atkinson, J.; De Paepe, K.; Sanchez Pozo, A.; Rekkas, D.; Volmer, D.; Hirvonen, J.; Bozic, B.; Skowron, A.; Mircioiu, C.; Marcincal, A.; et al. The Second Round of the PHAR-QA Survey of Competences for Pharmacy Practice. Pharmacy 2016, 4, 27. [Google Scholar] [CrossRef]
- EU directive 2005/36/CE. Directive on the Recognition of Professional Qualifications. European Parliament and Council. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2005:255:0022:0142:en:PDF (accessed on 11 April 2020).
- Koster, A.; Schalekamp, T.; Meijerman, I. Implementation of Competency-Based Pharmacy Education (CBPE). Pharmacy 2017, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Croft, H.; Gilligan, C.; Rasiah, R.; Levett-Jones, T.; Schneider, J. Current Trends and Opportunities for Competency Assessment in Pharmacy Education-A Literature Review. Pharmacy 2019, 7, 67. [Google Scholar] [CrossRef]
- Moreau, P.; Al-Taweel, D.; Qaddoumi, M.; Alowayesh, M. Becoming a Pharmacist: Education and Training. Encycl. Pharm. Pract. Clin. Pharm. 2019, 3B, 1–14. [Google Scholar] [CrossRef]
- Katajavuori, N.; Hakkarainen, K.; Kuosa, T.; Airaksinen, M.; Hirvonen, J.; Holm, Y. Curriculum Reform in Finnish Pharmacy Education. Am. J. Pharm. Educ. 2009, 73, 151. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Biggs, J.; Tang, C. Teaching for Quality Learning at University, 4th ed.; SRHE and Open University Press, McGraw-Hill: Maidenhead, UK, 2011; ISBN 978-0-33-524275-7. [Google Scholar]
- Malone, D.T.; Short, J.L.; Naidu, S.; White, P.J.; Kirkpatrick, C.M. Mapping of the Australian Qualifications Framework Standards Onto an Undergraduate Bachelor of Pharmacy Course. Pharm. Educ. 2015, 15, 261–269. [Google Scholar]
- Plaza, C.M.; Draugalis, J.R.; Slack, M.K.; Skrepnek, G.H.; Sauer, K.A. Curriculum Mapping in Program Assessment and Evaluation. Am. J. Pharm. Educ. 2007, 71, 20. [Google Scholar] [CrossRef]
- Volmer, D.; Sepp, K.; Veski, P.; Raal, A. The Implementation of Pharmacy Competence Teaching in Estonia. Pharmacy 2017, 5, 18. [Google Scholar] [CrossRef]
- Gmeiner, T.; Horvat, N.; Kos, M.; Obreza, A.; Vovk, T.; Grabnar, I.; Bozic, B. Curriculum Mapping of the Master’s Program in Pharmacy in Slovenia with the PHAR-QA Competency Framework. Pharmacy 2017, 5, 24. [Google Scholar] [CrossRef]
- Skowron, A.; Dymek, J.; Golda, A.; Polak, W. Are we Ready to Implement Competence-Based Teaching in Pharmacy Education in Poland? Pharmacy 2017, 5, 25. [Google Scholar] [CrossRef]
- Kirkpatrick, M.A.F.; Pugh, C.B. Assessment of Curricular Competency Outcomes. Am. J. Pharm. Educ. 2001, 65, 217–224. [Google Scholar]
- Westein, M.P.D.; De Vries, H.; Floor, A.; Koster, A.S.; Buurma, H. Development of a Postgraduate Community Pharmacist Specialization Program using canMEDS Competencies, and Entrustable Professional Activities. Am. J. Pharm. Educ. 2019, 83, 1354–1365. [Google Scholar] [CrossRef] [PubMed]
- Van der Werf, J.J.; Dekens-Konter, J.; Brouwers, J.R.B.J. A New Model for Teaching Pharmaceutical Care Services Management. Pharm. Educ. 2004, 4, 165–169. [Google Scholar] [CrossRef][Green Version]
- Miller, G.E. The Assessment of Clinical Skills/Competence/Performance. Acad. Med. 1990, 65, S63–S67. [Google Scholar] [CrossRef] [PubMed]
- Albarquoni, L.; Hoffman, T.; Glasziou, P. Evidence-Based Practice Educational Intervention Studies: A Systematic Review of what is Taught and how it is Measured. BMC Med. Educ. 2018, 18, 177. [Google Scholar] [CrossRef]
- Khan, K.Z.; Gaunt, K.; Ramachandran, S.; Pushkar, P. The Objective Structured Clinical Examination (OSCE): AMEE Guide no. 81. Part II: Organisation & Administration. Med. Teach. 2013, 35, e1447–e1463. [Google Scholar] [CrossRef]
- Kristina, S.A.; Wijoyo, Y. Assessment of Pharmacy Students’ Clinical Skills using Objective Structured Clinical Examination (OSCE): A Literature Review. Syst. Rev. Pharm. 2019, 10, 55–60. [Google Scholar] [CrossRef]
- Khan, K.Z.; Ramachandran, S.; Gaunt, K.; Pushkar, P. The Objective Structured Clinical Examination (OSCE): AMEE Guide no. 81. Part I: An Historical and Theoretical Perspective. Med. Teach. 2013, 35, e1437–e1446. [Google Scholar] [CrossRef]
- Williamson, J.M.L.; Osborne, A.J. Critical Analysis of Case Based Discussions. Br. J. Med. Pract. 2012, 5, 35–38. [Google Scholar]
- Ten Cate, O.; Hoff, R.G. From Case-Based to Entrustment-Based Discussions. Clin. Teach. 2017, 14, 385–389. [Google Scholar] [CrossRef]
- Harris, J.; Kearney, K.; Heneghan, C.; Meats, E.; Roberts, N.; Perera, R.; Kearney-Shiers, K. Are Journal Clubs Effective in Supporting Evidence-Based Decision Making? A Systematic Review. BEME Guide no. 16. Med. Teach. 2011, 3, 9–23. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Fineout-Overholt, E. Rapid Critical Appraisal of Randomized Controlled Trials (RCs): An Essential Skill for Evidence-Based Practice (EBP). Ped. Nurs. 2005, 31, 50–52. [Google Scholar]
- Hirsch, A.C.; Parihar, H.S. A Capstone Course with a Comprehensive and Integrated Review of the Pharmacy Curriculum and Student Assessment as a Preparation for Advanced Pharmacy Practice Experiences. Am. J. Pharm. Educ. 2014, 78, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, O.; Chen, H.C.; Hoff, R.G.; Peters, H.; Bok, H.; Van Der Schaaf, M. Curriculum Development for the Workplace using Entrustable Professional Activities (EPAs): AMEE Guide no. 99. Med. Teach. 2015, 37, 983–1002. [Google Scholar] [CrossRef]
- Sandars, J. The use of Reflection in Medical Education: AMEE Guide no. 44. Med. Teach. 2009, 31, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.G.; Ciantar, J.; Jubraj, B.; Bates, I.P. Use of a Multisource Feedback Tool to Develop Pharmacists in a Postgraduate Training Program. Am. J. Pharm. Educ. 2013, 77, 52. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.P.; Sharma, A.; West, D.; Bates, I.P.; Davies, J.G.; Abdel-Tawab, R. An Evaluation of using Multi-Source Feedback (MSF) among Junior Hospital Pharmacists. Int. J. Pharm. Pract. 2011, 19, 276–280. [Google Scholar] [CrossRef]
- Tromp, F.; Vernooij-Dassen, M.; Grol, R.; Kramer, A.; Bottema, B. Assessment of CanMEDS Roles in Postgraduate Training: The Validation of the Compass. Patient Educ. Couns. 2012, 89, 199–204. [Google Scholar] [CrossRef]
- Van Tartwijk, J.; Driessen, E.W. Portfolios for Assessment and Learning: AMEE Guide no. 45. Med. Teach. 2009, 31, 790–801. [Google Scholar] [CrossRef]
- Ho, S.S.S.; Kember, D.; Lau, C.B.S.; Au Yeung, M.Y.M.; Leung, D.Y.P.; Chow, M.S.S. An Outcomes-Based Approach to Curriculum Development in Pharmacy. Am. J. Pharm. Educ. 2009, 73, 14. [Google Scholar] [CrossRef][Green Version]
- Pearson, M.L.; Hubball, H.T. Curricular Integration in Pharmacy Education. Am. J. Pharm. Educ. 2012, 76, 204. [Google Scholar] [CrossRef]
- Nelson, M.; Allison, S.D.; McCollum, M.; Luckey, S.W.; Clark, D.R.; Paulsen, S.M.; Malhotra, J.; Brunner, L.J. The Regis Model for Pharmacy Education: A Highly Integrated Curriculum Delivered by Team-Based Learning™ (TBL). Curr. Pharm. Teach. Learn. 2013, 5, 555–563. [Google Scholar] [CrossRef]
- Walter, S.; Mulherin, K.; Cox, C.D. A Preceptor Competency Framework for Pharmacists. Part 2 of a 3-Part Series. Curr. Pharm. Teach. Learn. 2018, 10, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Kusurkar, R.A.; Croiset, G.; Mann, K.V.; Custers, E.; Ten Cate, O. Have Motivation Theories Guided the Development and Reform of Medical Education Curricula? A Review of the Literature. Acad. Med. 2012, 87, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Noble, C.; Coombes, I.; Shaw, P.N.; Nissen, L.M.; Clavarino, A. Becoming a Pharmacist: The Role of Curriculum in Professional Identity Formation. Pharm. Pract. 2014, 12, 380–393. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Chauvin, S. Professional Identity Formation in an Advanced Pharmacy Practice Experience Emphasizing Self-Authorship. Am. J. Pharm. Educ. 2016, 80, 172. [Google Scholar] [CrossRef] [PubMed]
- NHG. Competentieprofiel Van De Huisarts (General Practitioner Competency Profile). NHG (Dutch College of General Practitioners). Available online: https://www.huisartsopleiding.nl/images/opleiding/Competentieprofiel_van_de_huisarts_2016.pdf (accessed on 11 April 2020).
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).