Adverse Drug Reactions in Norway: A Systematic Review




Abstract
1. Introduction
ADR Reporting and Handling in the Norwegian Healthcare System
2. Materials and Methods
2.1. Design of the Study
2.2. Search Strategy and Data Collection
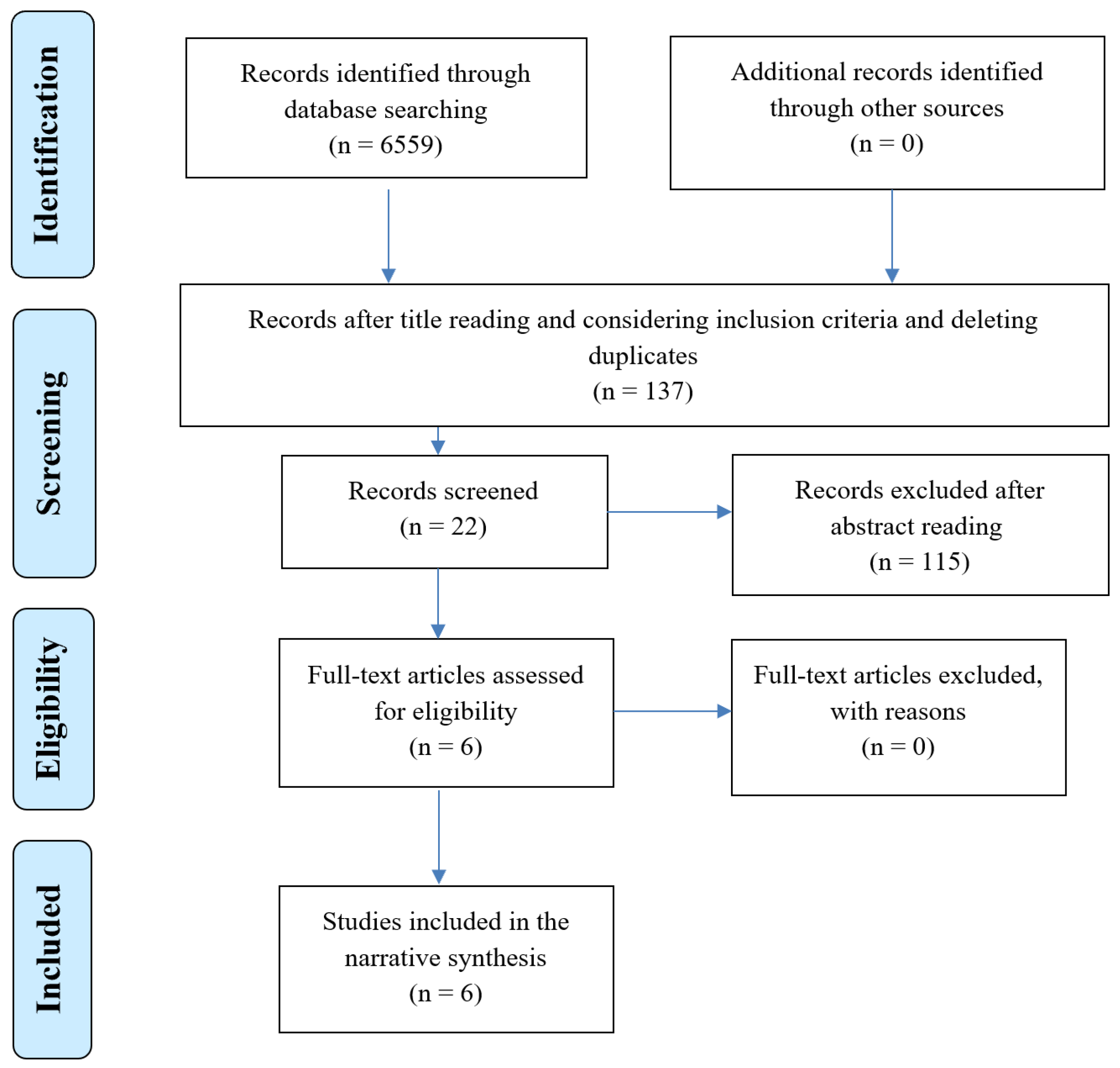
2.3. Progression of Systematic Review and Quality of Studies
3. Results
3.1. General Description of the Studies
3.2. Patient Reporting Schema
3.3. Healthcare Provider Reporting Schema
3.4. The Current Pharmacovigilance System
4. Discussion
4.1. Patients vs. Healthcare Providers’ Reporting of ADRs
4.2. The Need for ADR Profiles for Identifying, Documenting and Reporting ADRs
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Essential Medicines and Health Products Information Portal: A World Health Organization Resource. 2018. Available online: http://apps.who.int/medicinedocs/en/d/Jh2992e/2.html (accessed on 20 July 2019).
- International Conference on Harmonisation (ICH). ICH Harmonised Tripartite Guideline for Good Clinical Practice; Institute of Clinical Research: Marlow, UK, 1996; Available online: http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E6/E6_R1_Guideline.pdf (accessed on 31 January 2018).
- Jordan, S.; Logan, P.A.; Panes, G.; Vaismoradi, M.; Hughes, D. Adverse Drug Reactions, Power, Harm Reduction, Regulation and the ADRe Profiles. Pharmacy 2018, 6, 102. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Banner, T.; Gabe-Walters, M.; Mikhail, J.M.; Round, J.; Snelgrove, S.; Storey, M.; Wilson, D.; Hughes, D. Medicines Management Group. Nurse-led medicines’ monitoring in care homes study protocol: A process evaluation of the impact and sustainability of the adverse drug reaction (ADRe) profile for mental health medicines. BMJ Open 2018, 8, e023377. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). WHO Launches Global Effort to Halve Medication-Related Errors in 5 Years. 2017. Available online: http://www.who.int/mediacentre/news/releases/2017/medication-related-errors/en/ (accessed on 18 October 2018).
- Frontier Economic. Exploring the Costs of Unsafe Care in the NHS: A Report Prepared for the Department of Health; Frontier Economics: London, UK, 2014; Available online: http://www.frontier-economics.com/documents/2014/10/exploring-the-costs-of-unsafe-care-in-the-nhs-frontier-report-2-2-2-2.pdf (accessed on 4 June 2015).
- NICE Medicines & Prescribing Centre. Medicines Optimisation: The Safe and Effective Use of Medicines to Enable the Best Possible Outcomes; NICE Guideline 5; NICE: London, UK, 2015; Available online: http://www.nice.org.uk/guidance/ng5/evidence/full-guideline-6775454 (accessed on 4 June 2015).
- Schork, N.J. Personalized medicine: Time for one-person trials. Nature 2015, 520, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Hakkarainen, K.M.; Andersson Sundell, K.; Petzold, M.; Hägg, S. Prevalence and perceived preventability of self-reported adverse drug events-a population-based survey of 7099 adults. PLoS ONE 2013, 8, e73166. [Google Scholar] [CrossRef]
- Zhang, H.; Du, W.; Gnjidic, D.; Chong, S.; Glasgow, N. Trends in adverse drug reaction-related hospitalisations over 13 years in New South Wales, Australia. Intern. Med. J. 2019, 49, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Angamo, M.T.; Chalmers, L.; Curtain, C.M.; Bereznicki, L.R. Adverse-Drug-Reaction-Related Hospitalisations in Developed and Developing Countries: A Review of Prevalence and Contributing Factors. Drug Saf. 2016, 39, 847–857. [Google Scholar] [CrossRef] [PubMed]
- Parameswaran Nair, N.; Chalmers, L.; Bereznicki, B.J.; Curtain, C.M.; Bereznicki, L.R. Repeat Adverse Drug Reaction-Related Hospital Admissions in Elderly Australians: A Retrospective Study at the Royal Hobart Hospital. Drugs Aging 2017, 34, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Jennings, E.; Murphy, K.; Gallagher, P.; O’Mahony, D. Inhospital Adverse Drug Reactions in Hospitalised Older Adults—A Systematic Review. In Proceedings of the 14th International Congress of the EuGMS, Berlin, Germany, 10–12 October 2018; Available online: https://cora.ucc.ie/bitstream/handle/10468/7224/EJ_SR_Poster_In-hopsital_ADRs_in_hospitalised_older_adults.pdf?sequence=1&isAllowed=y (accessed on 23 July 2019).
- Moller, U.O.; Hansson, E.E.; Ekdahl, C.; Midlöv, P.; Jakobsson, U.; Kristensson, J. Fighting for control in an unpredictable life—A qualitative study of older persons’ experiences of living with chronic dizziness. BMC Geriatr. 2014, 14, 97. [Google Scholar] [CrossRef]
- Deilkas, E.T.; Risberg, M.B.; Haugen, M.; Lindstrøm, J.C.; Nylén, U.; Rutberg, H.; Michael, S. Exploring similarities and differences in hospital adverse event rates between Norway and Sweden using Global Trigger Tool. BMJ Open 2017, 7, e012492. [Google Scholar] [CrossRef] [PubMed]
- Tangiisuran, B.; Wright, J.; Van der Cammen, T.; Rajkumar, C. Adverse drug reactions in elderly: Challenges in identification and improving preventative strategies. Age Ageing 2009, 38, 358–359. [Google Scholar] [CrossRef]
- Bouvy, J.C.; De Bruin, M.L.; Koopmanschap, M.A. Epidemiology of adverse drug reactions in Europe: A review of recent observational studies. Drug Saf. 2015, 38, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Vaz, I.; Silva, A.M.; Costa Santos, C.; Cruz-Correia, R. How to promote adverse drug reaction reports using information systems—A systematic review and meta-analysis. BMC Med. Inform. Decis. Mak. 2016, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Essential Medicines and Health Products, Adverse Drug Reactions Monitoring. 2019. Available online: https://www.who.int/medicines/areas/quality_safety/safety_efficacy/advdrugreactions/en/ (accessed on 17 July 2019).
- Lopez-Gonzalez, E.; Herdeiro, M.T.; Piñeiro-Lamas, M.; Figueiras, A.; GREPHEPI Group. Effect of an educational intervention to improve adverse drug reaction reporting in physicians: A cluster randomized controlled trial. Drug Saf. 2015, 38, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Bracken, L.E.; Nunn, A.J.; Kirkham, J.J.; Peak, M.; Arnott, J.; Smyth, R.; Pirmohamed, M.; Turner, M.A. Development of the Liverpool Adverse Drug Reaction Avoidability Assessment Tool. PLoS ONE 2017, 12, e0169393. [Google Scholar] [CrossRef] [PubMed]
- MeldSt28. Report to the Storting (Norwegian Parliament) White Paper on Medicinal Products, Correct Use—Better Health; Ministry of Health and Care Services (Helse- og omsorgsdepartementet): Oslo, Norway, 2015. Available online: https://www.regjeringen.no/contentassets/1e17b19947224def82e509ca5f346357/en-gb/pdfs/stm201420150028000engpdfs.pdf (accessed on 20 April 2019).
- Forskrift om Legemidler (Legemiddelforskriften). FOR-2009-12-18-1839; Helse- og omsorgsdepartementet: Oslo, Norway, 2010.
- Norwegian Medicines Agency (NoMA). Pharmacovigilance and Adverse Drug Reactions (Bivirkninger og legemiddelsikkerhet). 2019. Available online: https://legemiddelverket.no/bivirkninger-og-sikkerhet (accessed on 25 April 2019).
- RELIS. About RELIS. 21.10.2015. Available online: https://relis.no/about_relis (accessed on 25 April 2019).
- Norwegian Medicines Agency (NoMA). Report on Adverse Drug Reactions (Bivirkningsrapport). 2018. Available online: https://view.publitas.com/norwegian-medicines-agency/bivirkningsrapport-2018/page/8-9 (accessed on 13 May 2019).
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Evans, D. Systematic reviews of nursing research. Intensive Crit. Care Nurs. 2001, 17, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1 [updated March 2011]. Available online: http://handbook-5-1.cochrane.org/ (accessed on 4 March 2019).
- Enhancing the QUAlity and Transparency of Health Research (EQUATOR) Website (EQUATOR). 2019. Available online: http://www.equator-network.org/ (accessed on 4 March 2019).
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Website. 2015. Available online: http://www.prisma-statement.org/ (accessed on 28 June 2019).
- Van Hunsel, F.; Härmark, L.; Pal, S.; Olsson, S.; Van Grootheest, K. Experiences with adverse drug reaction reporting by patients: An 11-country survey. Drug Saf. 2012, 35, 45–60. [Google Scholar] [CrossRef]
- Nergard, C.S. Bivirkninger av plantebaserte produkter. Norsk Farmaceutisk Tidsskrift 2017, 7, 36–40. [Google Scholar]
- Schjøtt, J.; Bergman, J. Joint medicine-information and pharmacovigilance services could improve detection and communication about drug-safety problems. Drug Healthc. Patient Saf. 2014, 6, 89–92. [Google Scholar] [CrossRef][Green Version]
- Fjermeros, K.; Werner, M.C.; Harg, P.; Samdal, H.; Slørdal, L.; Spigset, O. Patient reporting of adverse drug reactions in Norway 2010–2013. Tidsskr Nor Laegeforen 2015, 135, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Eek, A.K.; Ström, B.O.; Bakkehöi, G.; Stenberg-Nilsen, H. Bivirkninger ved bruk av antikoagulasjonsmidler i 2013–2015 (Anticoagulant-associated adverse drug reactions in 2013–2015). Tidsskrift for Den Norske Legeforening 2018, 138. [Google Scholar] [CrossRef]
- Svendsen, K.; Halvorsen, K.H.; Vorren, S.; Samdal, H.; Garcia, B. Adverse drug reaction reporting: How can drug consumption information add to analyses using spontaneous reports? Eur. J. Clin. Pharmacol. 2018, 74, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Blenkinsopp, A.; Wilkie, P.; Wang, M.; Routledge, P.A. Patient reporting of suspected adverse drug reactions: A review of published literature and international experience. Br. J. Clin. Pharmacol. 2007, 63, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Golomb, B.A.; McGraw, J.J.; Evans, M.A.; Dimsdale, J.E. Physician response to patient reports of adverse drug effects: Implications for patient-targeted adverse effect surveillance. Drug Saf. 2007, 30, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Leone, R.; Moretti, U.; D’Incau, P.; Conforti, A.; Magro, L.; Lora, R.; Velo, G. Effect of pharmacist involvement on patient reporting of adverse drug reactions: First Italian study. Drug Saf. 2013, 36, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Inch, J.; Watson, M.C.; Anakwe-Umeh, S. Patient versus healthcare professional spontaneous adverse drug reaction reporting: A systematic review. Drug Saf. 2012, 35, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Krska, J.; Murphy, E.; Avery, A. Yellow Card Study Collaboration. The importance of direct patient reporting of suspected adverse drug reactions: A patient perspective. Br. J. Clin. Pharmacol. 2011, 72, 806–822. [Google Scholar] [CrossRef]
- McLernon, D.J.; Bond, C.M.; Hannaford, P.C.; Watson, M.C.; Lee, A.J.; Hazell, L.; Avery, A. Yellow Card Collaboration. Adverse drug reaction reporting in the UK: A retrospective observational comparison of yellow card reports submitted by patients and healthcare professionals. Drug Saf. 2010, 33, 775–788. [Google Scholar] [CrossRef]
- Rolfes, L.; Van Hunsel, F.; Wilkes, S.; Van Grootheest, K.; Van Puijenbroek, E. Adverse drug reaction reports of patients and healthcare professionals-differences in reported information. Pharmacoepidemiol. Drug Saf. 2015, 24, 152–158. [Google Scholar] [CrossRef]
- Al Dweik, R.; Stacey, D.; Kohen, D.; Yaya, S. Factors affecting patient reporting of adverse drug reactions: A systematic review. Br. J. Clin. Pharmacol. 2017, 83, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Sabblah, G.T.; Darko, D.M.; Mogtari, H.; Härmark, L.; Van Puijenbroek, E. Patients’ Perspectives on Adverse Drug Reaction Reporting in a Developing Country: A Case Study from Ghana. Drug Saf. 2017, 40, 911–921. [Google Scholar] [CrossRef]
- Matos, C.; Härmark, L.; Van Hunsel, F. Patient Reporting of Adverse Drug Reactions: An International Survey of National Competent Authorities’ Views and Needs. Drug Saf. 2016, 39, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Mendes Marques, J.I.; Polónia, J.M.; Figueiras, A.G.; Costa Santos, C.M.; Herdeiro, M.T. Nurses’ attitudes and spontaneous adverse drug reaction reporting: A case-control study in Portugal. J. Nurs. Manag. 2016, 24, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Sundaran, S.; Udayan, A.; Hareendranath, K.; Eliyas, B.; Ganesan, B.; Hassan, A.; Subash, R.; Palakkal, V.; Salahudeen, M.S. Study on the Classification, Causality, Preventability and Severity of Adverse Drug Reaction Using Spontaneous Reporting System in Hospitalized Patients. Pharmacy 2018, 6, 108. [Google Scholar] [CrossRef]
- Ribeiro-Vaz, I.; Santos, C.C.; Cruz-Correia, R. Promoting adverse drug reaction reporting: Comparison of different approaches. Revista de Saude Publica 2016, 50, 14. [Google Scholar] [CrossRef]
- Bailey, C.; Peddie, D.; Wickham, M.E.; Badke, K.; Small, S.S.; Doyle-Waters, M.M.; Balka, E.; Hohl, C.M. Adverse drug event reporting systems: A systematic review. Br. J. Clin. Pharmacol. 2016, 82, 17–29. [Google Scholar] [CrossRef]
- Dweik, R.A.; Yaya, S.; Stacey, D.; Kohen, D. Spontaneous adverse drug reaction reporting by patients in Canada: A multi-method study-study protocol. Springerplus 2016, 5, 213. [Google Scholar] [CrossRef]
- Staniszewska, A.; Dąbrowska-Bender, M.; Olejniczak, D.; Duda-Zalewska, A.; Bujalska-Zadrożny, M. Patient knowledge on reporting adverse drug reactions in Poland. Patient Prefer. Adherence 2016, 11, 47–53. [Google Scholar] [CrossRef]


{kind=link}
| Databases | Total in Each Database | Title Selection | Abstract Selection | Full-Text Appraisal |
|---|---|---|---|---|
| PubMed [including Medline] | 5703 | 18 | 2 | 2 |
| Scopus | 85 | 15 | 1 | 1 |
| Embase | 27 | 5 | 0 | 0 |
| Cinahl | 196 | 0 | 0 | 0 |
| Web of Science | 250 | 7 | 1 | 0 |
| Cochrane | 46 | 3 | 0 | 0 |
| Norat | 68 | 26 | 8 | 3 |
| Idunn | 81 | 4 | 0 | 0 |
| SweMed | 103 | 59 | 10 | 0 |
| Manual search/backtracking references | - | - | - | 0 |
| Total | 6559 | 137 | 22 | 6 |
| Title | Authors | Year | Country | Aim | Methods |
|---|---|---|---|---|---|
| Experiences with adverse drug reaction reporting by patients: an 11-country survey. | van Hunsel et al. [33] | 2012 | Netherlands with the inclusion of data from Norway | To review the methods of patient reporting of adverse drug reactions (ADRs) in 11 countries and to compare different aspects of their experiences aimed at describing current practice. | A survey based on telephone interviews, e-mail discussions, and field visits. |
| Bivirkninger av plantebaserte produkter | Nergård [34] | 2013 | Norway | To describe the reports of ADRs of plant-based products in Norway from 2003–2012. | A retrospective cross-sectional study of reported ADRs from plant-based products in Norway 2003–2012. |
| Joint medicine-information and pharmacovigilance services could improve detection and communication about drug-safety problems | Schjøtt & Bergman [35] | 2014 | Norway | To describe the potential of the RELIS’s dual service to improve detection and communication of drug-safety problems. | Searching the RELIS database for question-answer pairs about ADRs using the Norwegian ADRs database. |
| Patient reporting of adverse drug reactions in Norway 2010–2013 | Fjermeros et al. [36] | 2015 | Norway | To review patients’ reports of ADRs to the Norwegian Medicines Agency since 1 March 2010. | A cross-sectional retrospective study of ADRs reporting of patients to the Norwegian Medicines Agency (NoMA). |
| Bivirkninger ved bruk av antikoagulasjonsmidler i 2013-15 (Anticoagulant-associated adverse drug reactions in 2013–2015) | Eek et al. [37] | 2018 | Norway | To obtain a better insight into the ADRs profiles of the new direct-acting oral anticoagulants (DOACs). | A retrospective cross-sectional study of registry data (RELIS database of ADRs and the Norwegian Prescription Database (NorPD)). |
| Adverse drug reaction reporting: how can drug consumption information add to analyses using spontaneous reports? | Svendsen et al. [38] | 2018 | Norway | To combine ADRs reports with drug consumption data to demonstrate the additional information. | Combining all Norwegian ADR reports 2004–2013 from the EudraVigilance database (n = 14.028) with dispensing data from the Norwegian Prescription Database (more than 800 million dispensed prescriptions during 2004–2013). |
| Studies/Characteristics | Number of Reports | Size of Population Covered | Type of Reporting | Age of Patients | Gender of Patients | Most Commonly Reported Events | Patient Reporting | Healthcare Provider Reporting | Pharmacovigilance System |
|---|---|---|---|---|---|---|---|---|---|
| van Hunsel et al. [33] | 30 consumer reports per month (14% of total) | No data | Electronic | No data | No data | Only on registered drugs | Sophisticated system without follow up | Causality assessment and personal feedback | Reporting only serious events |
| Nergård [34] | 260 reports associated with plant-based products from 2003–2012 | No data | No data | Average age of 52 years; 20% of the sample was >70 years | 72% female | Hypersensitivity reactions (27%), hepatic events (20%), and interactions with anticoagulants (8%) | Not relevant, only reports from healthcare providers included | No data | RELIS database |
| Schjøtt & Bergman [35] | 5427 (26%) of 21,071 question-answer pairs, and 791 (4%) of a total of 22,090 reports in the Norwegian ADR database | No data | Electronic | No data | No data | Dose escalation, craving, and withdrawal reactions to Lyrica® (pregabalin) | No data | Provision of feedback by pharmacists and clinical pharmacologists to healthcare professionals | Norwegian ADR database and the RELIS database |
| Fjermeros et al. [36] | 755 reports from patients and 9629 reports from healthcare staff in the time period of March 2010–December 2013 | No data | No data | Average age not given. The patients most commonly reporting were in the age range of 20–29 years (29%), whereas healthcare providers’ reports most frequently concerned those aged 0–9 years (17%) | 63% female among the patient reports, 58% female among the healthcare staff reports | Adverse mental and neurological reactions were commonly reported by patients, while healthcare providers reported mostly on general symptoms and local reactions. | No data | No data | Norwegian ADR database (NoMA) |
| Eek et al. [37] | 409 reports on ADRs associated with anticoagulants in the time period of June 2013–May 2015 | Approximately 145,000 anti-coagulant users | No data | Average age was 75–80 years | 44% female | Cerebral haemorrhage, haemorrhage in skin/muscle/joint/mucous membranes and gastrointestinal haemorrhage | Not relevant, only reports from healthcare providers included | No data | Norwegian ADRs database (NoMA) and RELIS database |
| Svendsen et al. [38] | 14.028 from the EudraVigilance database and 800 million from the Norwegian Prescription Database | Data from 5.1 million different persons. | Electronic | No data | 22,351 female and 39,391 male users of methylphenidate | Physical and psychological symptoms in both males and females | No data | No data | EudraVigilance database, Norwegian prescription database |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaismoradi, M.; Logan, P.A.; Jordan, S.; Sletvold, H. Adverse Drug Reactions in Norway: A Systematic Review. Pharmacy 2019, 7, 102. https://doi.org/10.3390/pharmacy7030102
Vaismoradi M, Logan PA, Jordan S, Sletvold H. Adverse Drug Reactions in Norway: A Systematic Review. Pharmacy. 2019; 7(3):102. https://doi.org/10.3390/pharmacy7030102
Chicago/Turabian StyleVaismoradi, Mojtaba, Patricia A. Logan, Sue Jordan, and Hege Sletvold. 2019. "Adverse Drug Reactions in Norway: A Systematic Review" Pharmacy 7, no. 3: 102. https://doi.org/10.3390/pharmacy7030102
APA StyleVaismoradi, M., Logan, P. A., Jordan, S., & Sletvold, H. (2019). Adverse Drug Reactions in Norway: A Systematic Review. Pharmacy, 7(3), 102. https://doi.org/10.3390/pharmacy7030102