Nutrition Education and Community Pharmacy: A First Exploration of Current Attitudes and Practices in Northern Ireland

Abstract
1. Introduction
- Undertake a preliminary mapping of Northern Ireland pharmacists’ attitudes and practices relating to diet-related health promotion and disease prevention.
- Develop and pilot a nutrition education intervention for pre-registration pharmacists.
2. Materials and Methods
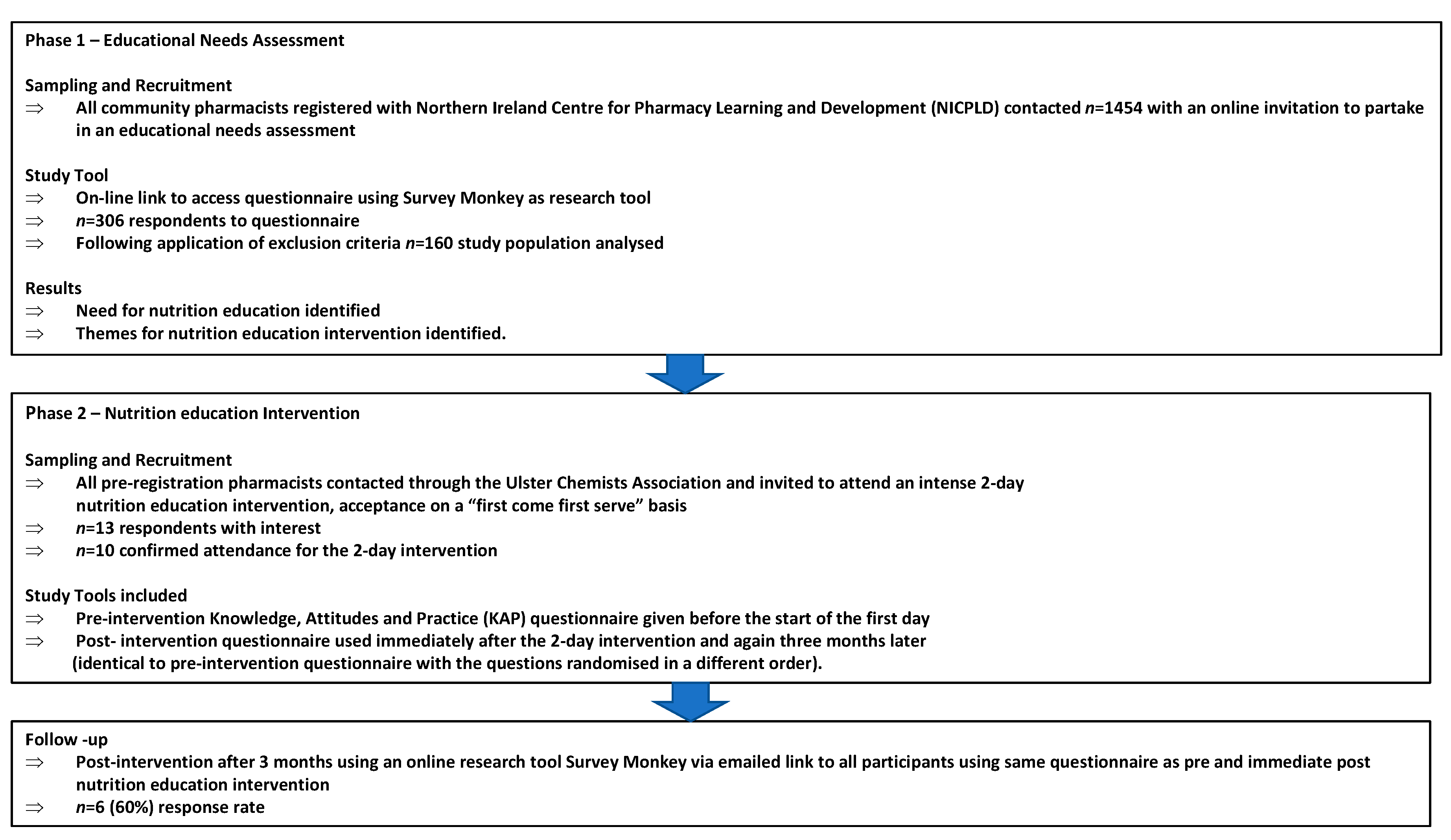
2.1. Phase 1
2.1.1. Study Design
- Attitudes towards the importance of nutrition in public health;
- Attitudes towards community pharmacists’ confidence in providing nutritional advice to patients.
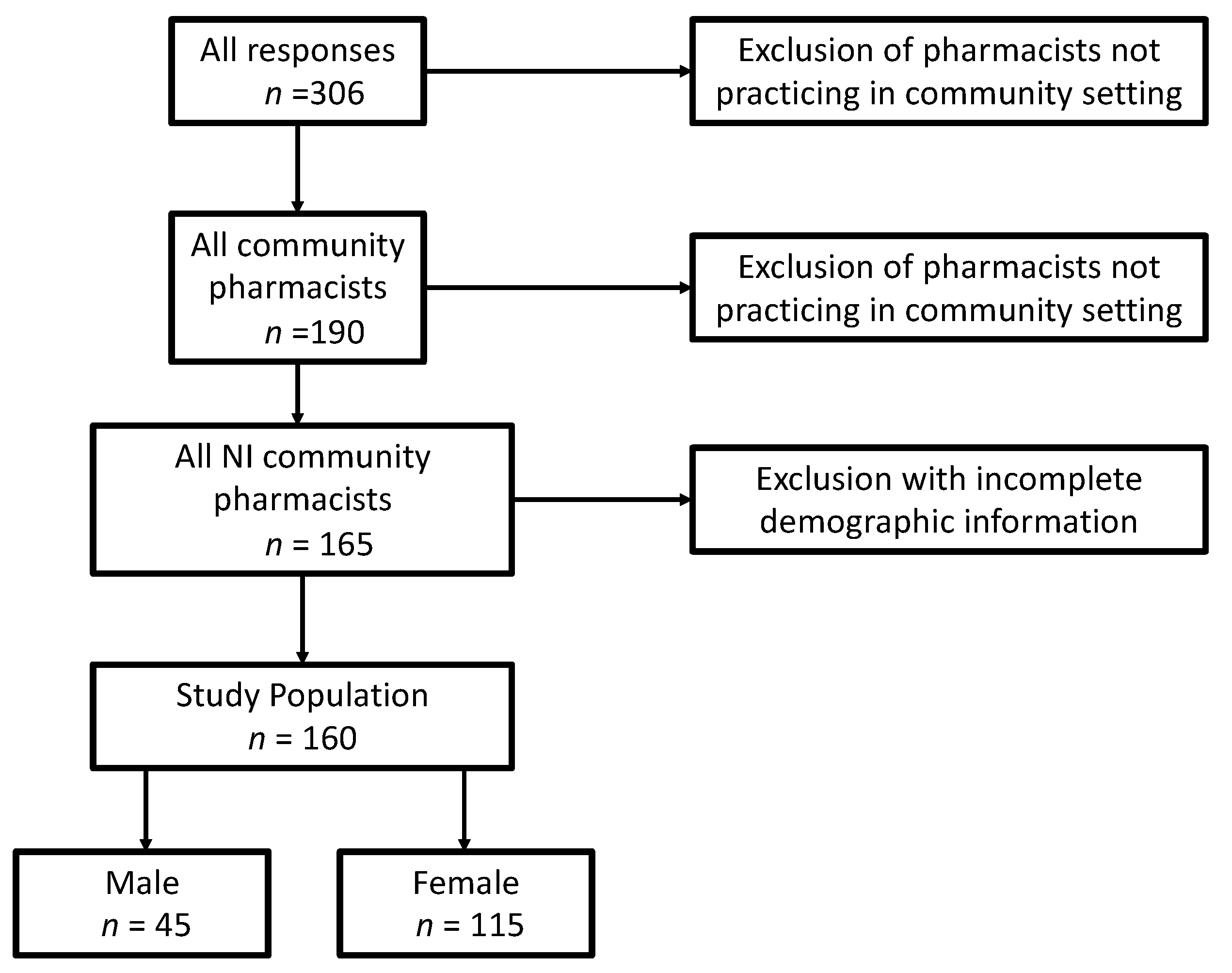
2.1.2. Recruitment
2.1.3. Data Collection
2.1.4. Data Analysis
2.1.5. Ethical Approval
2.2. Phase 2
2.2.1. Study Design
2.2.2. Recruitment
2.2.3. Data Collection
2.2.4. Data Analysis
2.2.5. Ethical Approval
3. Results
3.1. Phase 1: Needs Assessment
3.2. Phase 2 Pilot Nutrition Education Intervention
4. Discussion
4.1. Phase 1: Needs Assessment
4.2. Phase 2: Pilot Nutrition Education Intervention
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Question | Response Options | Pre- (n = 10) | Post- (n = 10) | Three Months After (n = 6) |
|---|---|---|---|---|
| How well do you think nutrition problems are managed in the community? (A) | Badly | 1 | 0 | 0 |
| Inadequately | 5 | 9 | 4 | |
| Adequately | 4 | 1 | 1 | |
| Very well | 0 | 0 | 1 | |
| Is there good evidence to suggest that fish oil consumption (omega-3 fatty acids) is helpful in the management of: (K) | ||||
| Respiratory disease? | Yes | 1 | 8 | 5 |
| Cardiovascular disease? | Yes | 10 | 10 | 6 |
| Gastrointestinal disease? | Yes | 2 | 7 | 6 |
| Endocrine disease? | Yes | 2 | 8 | 6 |
| How confident are you in recommending dietary patterns for clients with diabetes? (P) | Not confident | 4 | 0 | 0 |
| Somewhat confident | 5 | 1 | 1 | |
| Confident | 1 | 7 | 4 | |
| Very confident | 0 | 2 | 1 | |
| What key nutrient would you recommend that weaning babies particularly require? (K) | Vitamin C | 3 | 0 | 1 |
| Calcium | 2 | 6 | 2 | |
| Iron | 4 | 3 | 3 | |
| Sodium | 1 | 1 | 0 | |
| Would you feel equipped to give general nutritional advice to clients where appropriate or required? (A) | Not at all | 2 | 0 | 0 |
| Inadequately | 6 | 0 | 1 | |
| Adequately | 1 | 9 | 4 | |
| Very well | 1 | 1 | 1 | |
| Have you ever advised a client on how to increase their energy intake when prescribed long-term use of a medication that has an anorexic side effect? (P) | Never | 10 | 9 | 5 |
| Occasionally | 0 | 1 | 0 | |
| Frequently | 0 | 0 | 1 | |
| All the time | 0 | 0 | 0 | |
| Do you think that, from a public health perspective, nutrition is important in reducing the global burden of disease? (A) | Not at all | 0 | 0 | 0 |
| Not much | 1 | 0 | 0 | |
| Somewhat | 2 | 1 | 0 | |
| Very much | 7 | 9 | 6 | |
| Which micronutrient deficiency should you be aware of in people of Southeast Asian origin? (K) | Vitamin A | 3 | 1 | 4 |
| Iodine | 2 | 2 | 0 | |
| Vitamin D | 1 | 7 | 1 | |
| Zinc | 4 | 0 | 1 | |
| Would you advise clients about food‒drug interactions, such as advising clients prescribed statins or benzodiazepines to avoid grapefruit juice? (P) | Never | 3 | 0 | 1 |
| Occasionally | 6 | 1 | 4 | |
| Frequently | 0 | 6 | 1 | |
| All the time | 1 | 3 | 0 | |
| Have you discussed with clients what specialist gluten-free products they would like to see available in the pharmacy? (P) | Never | 7 | 6 | 3 |
| Occasionally | 2 | 4 | 1 | |
| Frequently | 1 | 0 | 2 | |
| All the time | 0 | 0 | 0 | |
| Would you advise specific client groups about taking nutritional supplements? (P) | Never | 4 | 1 | 0 |
| Occasionally | 4 | 6 | 5 | |
| Frequently | 2 | 3 | 1 | |
| All the time | 0 | 0 | 0 | |
| When should the MUST for adults be used in the community or care home settings? (K) | Never | 0 | 0 | 0 |
| Occasionally | 4 | 4 | 1 | |
| Frequently | 4 | 2 | 1 | |
| All the time | 2 | 4 | 4 | |
| How important do you think nutritional advice is in clients with conditions affecting the digestive system? (A) | Not at all | 0 | 0 | 0 |
| Not much | 0 | 0 | 0 | |
| Somewhat | 1 | 1 | 1 | |
| Very much | 9 | 9 | 5 | |
| Do you think clients would value general nutritional advice from a pharmacist? (A) | Not at all | 0 | 0 | 0 |
| Not much | 0 | 0 | 0 | |
| Somewhat | 6 | 3 | 1 | |
| Very much | 4 | 7 | 5 |
| Day 1 | |
|---|---|
| 09.00 | Registration for Day 1 |
| 09.30 | Welcome & Introduction SR & PD |
| 09.40 | Pre-questionnaire |
| 10.00 | Nutrition LMcC |
| 10.35 | Nutrition, public health and policy: A pharmacist’s responsibility SR |
| 11.15 | Coffee break |
| 11.40 | Nutrition and cardiovascular disease SR & CL |
| 12.30 | Best practice nutrition advice for baby and new mums HMcC |
| 13.00 | Lunch |
| 14.00 | Mini problem-based learning stations (25 min each) All team
|
| 16.15 | Coffee |
| 16.30 | Feedback by students |
| 17.00 | Sum Up |
| 17.15 | Close of Day 1 |
| Day 2 | |
| 09.00 | Registration for Day 2 |
| 09.20 | Nutrition and metabolic/endocrine disease CL & SR |
| 09.50 | Nutrition and gastrointestinal diseases HMcC & LMcC |
| 10.20 | Nutrition and respiratory diseases PD |
| 10.50 | Coffee break |
| 11.10 | Drug and nutrient/food interactions SG |
| 11.40 | Vitamin and mineral supplements: what’s the evidence? SG |
| 12.10 | Mini problem-based learning stations All team |
| 13.00 | Lunch |
| 14.00 | Mini problem-based learning stations All team |
| 14.25 | Feedback by students |
| 15.00 | Post-questionnaire |
| 15.20 | Coffee |
| 15.35 | Wrap up |
| 16.00 | Certificates |
| 16.15 | Close of Day 2 |
References
- Ball, L.; Hughes, R.; Leveritt, M. Health professionals’ views of the effectiveness of nutrition care in general practice setting. Nutr. Diet. 2012, 70, 35–41. [Google Scholar] [CrossRef]
- Avery, A.J.; Rodgers, S.; Cantrill, J.A.; Armstrong, S.; Cresswell, K.; Eden, M.; Elliott, R.A.; Howard, R.; Kendrick, D.; Morris, C.J.; et al. A pharmacist-led information technology intervention for medication errors (PINCER): A multicentre, cluster randomised, controlled trial and cost-effectiveness analysis. Lancet 2012, 379, 1310–1319. [Google Scholar] [CrossRef]
- Pogge, E. A Team-Based Learning Course on Nutrition and Lifestyle Modification. Am. J. Pharm. Educ. 2013, 77, 5. [Google Scholar] [CrossRef] [PubMed]
- Lenders, C.M.; Deen, D.D.; Bistrian, B.; Edwards, M.S.; Seidner, D.L.; McMahon, M.M.; Kohlmeier, M.; Krebs, N.F. Residency and specialties training in nutrition: A call for action. Am. J. Clin. Nutr. 2014, 99, 1174S–1183S. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, Social Services and Public Safety Northern Ireland. Making It Better through Pharmacy in the Community—A Five Year Strategy for Pharmacy in the Community. Available online: https://www.communitypharmacyni.co.uk/wpcontent/uploads/2014/03/making_it_better_through_pharmacy_in_the_community-Strategy-2014.pdf (accessed on 29 January 2019).
- Smith, J.; Picton, C.; Dayan, M. Now or Never: Shaping Pharmacy to the Future. The 2013 Report of the Commission on Future Models of Care Delivery through Pharmacy the Royal Pharmaceutical Society. Available online: https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Publications/Now%20or%20Never%20-%20Report.pdf (accessed on 28 November 2018).
- Balanda, K.P.; Barron, S.; Fahy, L.; McLaughlin, A. Making Chronic Conditions Count: Hypertension, Stroke, Coronary Heart Disease, Diabetes. A Systematic Approach to Estimating and Forecasting Population Prevalence on the Island of Ireland. Institute of Public Health in Ireland: Dublin. Available online: https://www.publichealth.ie/files/chronic_main.pdf (accessed on 29 January 2019).
- Levy, M.D.; Loy, L.; Zatz, L.Y. Policy approach to nutrition and physical activity education in health care professional training. Am. J. Clin. Nutr. 2014, 99, 1194S–1201S. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Popovich, N.G.; Iramaneerat, C.; Smith, E.V.; Lutfiyya, M.N. A clinical nutrition course to improve pharmacy students’ skills and confidence in counseling patients. Am. J. Pharm. Educ. 2008, 72, 66. [Google Scholar] [CrossRef] [PubMed]
- Pearce, K.L.; Cross, G. A 4-Week Nutrition and Therapeutics Course in an Undergraduate Pharmacy Program. Am. J. Pharm. Educ. 2013, 77, 154. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.M.; Kohlmeier, M.; Powell, M.; Zeisel, S.H. Nutrition in Medicine: Nutrition Education for Medical Students and Residents. Nutr. Clin. Pract. 2010, 25, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Boggs, S.; Massey, L.; Armstrong, J.; Lassey, W.; Joseph, J. Education of rural community pharmacists to provide nutrition information. Am. J. Pharm. Educ. 2013, 60, 353–358. [Google Scholar]
- Brown, T.J.; Todd, A.; O’Malley, C.; Moore, H.J.; Husband, A.K.; Bambra, C.; Kasim, A.; Sniehotta, F.F.; Steed, L.; Smith, S.; et al. Community pharmacy interventions for public health priorities: A systematic review of community pharmacy-delivered smoking, alcohol and weight management interventions. BMJ Open 2016. Available online: https://bmjopen.bmj.com/content/bmjopen/6/2/e009828.full.pdf (accessed on 4 March 2019). [CrossRef] [PubMed]
- Brown, D.; Portlock, J.; Rutter, P. Review of services provided by pharmacies that promote healthy living. Int. J. Clin. Pharm. 2012, 34, 399–409. [Google Scholar] [CrossRef] [PubMed]
- McNamara, K.P.; O’Reilly, S.L.; Dunbar, J.A.; Bailey, M.J.; George, J.; Peterson, G.M.; Jackson, S.L.; Janus, E.; Bunker, S.; Duncan, G.; et al. A pilot Study evaluating multiple risk factor interventions by community pharmacists to prevent cardiovascular disease The PAART CVD pilot project. Ann. Pharm. 2012, 46, 183–191. [Google Scholar] [CrossRef] [PubMed]
- McNamara, K.P.; George, J.; O’Reilly, S.L.; Jackson, S.L.; Peterson, G.M.; Howarth, H.; Bailey, M.J.; Duncan, G.; Trinder, P.; Morabito, E.; et al. Engaging community pharmacists in primary prevention of cardiovascular disease: Protocol for the Pharmacist Assessment of Adherence Risk and treatment in cardiovascular Disease (PAART CVD) pilot study. BMC Health Serv. Res. 2010, 10, 264. [Google Scholar]
- Corelli, R.L.; Zillich, A.J.; de Moor, C.; Arnold, J.; Fenlon, C.M.; Douglas, C.L.; Magnusson, B.; Zbikowski, S.M.; Prokhoro, A.V.; Hud, K.S. Recruitment of community pharmacies in a randomized trial to generate patient referrals to the tobacco quitline. Res. Soc. Admin. Pharm. 2012, 9, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Davis, W.A.; Bruce, D.G.; Davis, T.M. Economic impact of moderate weight loss in patients with Type 2 diabetes: The Fremantle Diabetes Study. Diabet. Med. 2011, 28, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Laur, C.; Douglas, P.; Rajput-Ray, M.; van der Es, M.; Redmond, J.; Eden, T.; Sayegh, M.; Minns, L.; Griffin, K.; et al. Nutrition education and leadership for improved clinical outcomes: Training and supporting junior doctors to run ‘Nutrition Awareness Weeks’ in three NHS hospitals across England. BMC Med. Educ. 2014, 29, 109. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Udumyan, R.; Rajput-Ray, M.; Thompson, B.; Lodge, K.; Douglas, P.; Sharma, P.; Broughton, R.; Smart, S.; Wilson, R.; et al. Evaluation of a novel nutrition education intervention for medical students from across England. BMJ Open 2012, 2, e000417. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.; Field, P. Nursing research. In The Application of Qualitative Approaches, 2nd ed.; Chapman and Hall: London, UK, 2002. [Google Scholar]
- Harden, R.M. Ten questions to ask when planning a course or curriculum. Med. Educ. 1986, 20, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Health and Social Care Board Northern Ireland. Transforming Your Care-Vision to Action, A Post Consultation Report. Available online: http://www.transformingyourcare.hscni.net/wp-content/uploads/2013/03/Transforming-Your-Care-Vision-to-Action-Post-Consultation-Report.pdf (accessed on 29 January 2019).
- Department of Health. A Vision for Pharmacy in the New NHS; Department of Health: London, UK, 2003.
- Weidmann, A.E.; Cunningham, S.; Gray, G.; Hansford, D.; McLay, J.; Broom, J.; Stewart, D. Over-the-counter orlistat: Early experiences, views and attitudes of community pharmacists in Great Britain. Int. J. Clin. Pharm. 2011, 33, 627–633. [Google Scholar] [CrossRef] [PubMed]
- BAPEN. Malnutrition Universal Screening Tool. Available online: https://www.bapen.org.uk/pdfs/must/must_full.pdf (accessed on 29 January 2019).
- Lee, L.; Tsai, A.C.; Wang, J.; Hurng, B.; Hsu, H.; Tsai, H. Need-based intervention is an effective strategy for improving the nutritional status of older people living in a nursing home: A randomized controlled trial. Int. J. Nurs. Stud. 2013, 50, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Cork, T.; Guard, H.; Jones, C.; Allinson, M.; White, S. Community pharmacists’ perspectives on malnutrition screening and support: A qualitative study. Int. J. Pharm. Pract. 2016, 24 (Suppl. 3), 3–7. [Google Scholar]
- BAPEN Self Screening. Available online: https://www.malnutritionselfscreening.org (accessed on 29 January 2019).
- Managing Adult Malnutrition in the Community Including a Pathway for the Appropriate Use of Oral Nutritional Supplements, Produced by a Multi-Professional Consensus Panel. May 2012. Available online: http://malnutritionpathway.co.uk/downloads/Managing_Malnutrition.pdf (accessed on 29 January 2019).
- Kris-Etherton, P.M.; Pratt, C.A.; Saltzman, E.; van Horn, L. Introduction to Nutrition Education in Training Medical and Other Health Care Professionals. Am. J. Clin. Nutr. 2014, 99, 1151S–1152S. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Agency, Northern Ireland. National Diet and Nutrition Survey Rolling Programme (NDNS RP) Results from Years 1–4 (Combined) for Northern Ireland (2008.09–2011/12): Survey Carried Out on Behalf of the Food Standards Agency in Northern Ireland and Public Health England. Available online: https://www.gov.uk/government/statistics/national-diet-and-nutrition-survey-rolling-programme-results-from-years-1-4-combined-for-northern-ireland-200809-201112-republication (accessed on 29 January 2019).
- Scientific Advisory Committee on Nutrition. Vitamin D and Health Report; Public Health England: London, UK, 2016.
- DiMaria-Ghalili, R.A.; Edwards, M.; Friedman, G.; Jaferi, A.; Kohlmeier, M.; Kris-Etherton, P.; Lenders, C.; Palmer, C.; Wylie-Rosett, J. Capacity building in nutrition science: Revisiting the curricula for medical professionals. Ann. Rep. 2013, 1306, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Maffeo, C.; Chase, P.; Brown, B.; Tuohy, K.; Kalsekar, I. My First Patient Program to Introduce First-Year Pharmacy Students to Health Promotion and Disease Prevention. Am. J. Pharm. Educ. 2009, 73, 97. [Google Scholar] [CrossRef] [PubMed]
- Garza, K.B.; Westrick, S.C.; Teeter, B.S.; Stevenson, T.L. Incorporating Hypertensive Patient Education on Salt Intake into an Introductory Pharmacy Practice Experience. Am. J. Pharm. Educ. 2013, 77, 199. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.I.; Johnson, T.P.; van Geest, J.B. Enhancing Surveys of Health Care Professionals: A Meta-Analysis of Techniques to Improve Response. Eval. Health Prof. 2013, 36, 382–407. [Google Scholar] [CrossRef] [PubMed]
- van Geest, J.B.; Johnson, T.P.; Welch, V.L. Methodologies for improving response rates in surveys of physicians—A systematic review. Eval. Health Prof. 2007, 30, 303–321. [Google Scholar] [CrossRef] [PubMed]
- DiMaria-Ghalili, R.A.; Mirtallo, J.M.; Tobin, B.W.; Hark, L.; van Horn, L.; Palmer, C.A. Challenges and opportunities for nutrition education and training in the health care professions: Intraprofessional and interprofessional call to action. Am. J. Clin. Nutr. 2014, 99, 1184S–1193S. [Google Scholar] [CrossRef] [PubMed]


| All n = 160 | Nutrition Education in Undergraduate Degree n = 160 | Nutrition Education in Pre-Registration Year n = 160 | Nutrition Education as Qualified Pharmacist n = 160 | The Last Time Nutrition Education Was Received (Years) n = 160 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Inadequate † | Adequate † | P | Inadequate † | Adequate † | P | Inadequate † | Adequate † | P | <2 † | 3–5 † | >6 † | P | ||
| Total | 126 (79) | 34 (21) | 132 (83) | 28 (17) | 130 (81) | 30 (19) | 58 (36) | 66 (41) | 36 (23) | |||||
| Gender | ||||||||||||||
| Male | 45 (28) | 38 (30) | 7 (21) | 38 (29) | 7 (25) | 35 (27) | 10 (33) | 15 (26) | 17 (26) | 13 (36) | ||||
| Female | 115 (72) | 88 (70) | 27 (79) | 0.271 | 94 (71) | 21 (75) | 0.686 | 95 (73) | 20 (67) | 0.481 | 43 (74) | 49 (74) | 23 (64) | 0.481 |
| Completed UG Degree in NI | ||||||||||||||
| Yes | 128 (80) | 100 (79) | 28 (82) | 104 (79) | 24 (86) | 107 (82) | 21 (70) | 50 (86) | 52 (79) | 26 (72) | ||||
| No | 32 (20) | 26 (21) | 6 (18) | 0.699 | 28 (21) | 4 (14) | 0.405 | 23 (18) | 9 (30) | 0.129 | 8 (14) | 14 (21) | 10 (28) | 0.244 |
| Completed PR in NI | ||||||||||||||
| Yes | 137 (86) | 107 (85) | 30 (88) | 110 (83) | 27 (96) | 111 (85) | 26 (87) | 52 (90) | 58 (88) | 27 (75) | ||||
| No | 23 (14) | 19 (15) | 4 (12) | 0.786 ‡ | 22 (17) | 1 (4) | 0.081 ‡ | 19 (15) | 4 (13) | 1.0 ‡ | 6 (10) | 8 (12) | 9 (25) | 0.114 |
| Registration Status | ||||||||||||||
| 0–5 Years | 55 (34) | 42 (33) | 13 (38) | 42 (32) | 13 (47) | 48 (37) | 7 (23) | 27 (46) | 25 (38) | 3 (8) | ||||
| 5–15 Years | 51 (32) | 36 (29) | 15 (44) | 40 (30) | 11 (39) | 39 (30) | 12 (40) | 16 (28) | 21 (32) | 14 (39) | ||||
| 16+ Years | 54 (34) | 48 (38) | 6 (18) | 0.063 | 50 (38) | 4 (14) | 0.054 | 43 (33) | 11 (37) | 0.338 | 15 (26) | 20 (30) | 19 (53) | 0.003 * |
| Location of NI Employment § | ||||||||||||||
| Rural | 54 (34) | 47 (37) | 7 (21) | 45 (34) | 9 (32) | 42 (32) | 12 (40) | 21 (36) | 18 (27) | 15 (42) | ||||
| Urban | 101 (63) | 76 (60) | 25 (74) | 0.084 | 83 (63) | 18 (64) | 0.857 | 83 (64) | 18 (60) | 0.509 | 36 (62) | 47 (71) | 18 (50) | 0.202 |
| Possible Score Range | Median Score (25th and 75th Percentiles) | |
|---|---|---|
| Attitudinal Theme 1 | ||
| Attitudes towards the importance of nutrition in public health (opinion) | 3–12 | 11 (11–12) |
| How important is nutrition in reducing the global burden of disease? | ||
| How important is nutritional advice in patients with digestive complaints? | ||
| Do you think patients would value nutritional advice from a pharmacist? | ||
| Attitudinal Theme 2 | ||
| Attitudes towards ability to provide nutritional advice (confidence) | 3–12 | 7 (6–8) |
| How well are nutritional problems managed in the community pharmacy setting? | ||
| How confident are you in providing dietary advice to a diabetic? | ||
| How equipped do you feel to offer weight loss advice? | ||
| Practice | 5–20 | 9 (8–10) |
| Advising increased energy intake when required due to medication side effects | ||
| Advising patient about food‒drug interactions | ||
| Advising specific patient groups about nutritional supplements (vitamins) | ||
| Use of the Malnutrition Universal Screening Tool | ||
| Recommendation of OTC supplements |
| Theme Sub-Theme | Quotes |
|---|---|
| Oral Nutrition Support (ONS) | |
| Compliance & follow-up | “If patients dislike what they’re recommended they seem to simply become less compliant, rather than beginning a process of trial and error to find what’s suitable”. “I often ask patients if they take their nutritional supplements (e.g., Fortisip) and they often admit to not tolerating them and not being fully compliant”. “Insufficient review and follow-up, or when changes are made wastage of prescribed supplements when new ones introduced”. “Use of sip feeds and nutritional supplements is very expensive but seems to be poorly managed”. “Nurses and doctors do not really give advice apart from telling people to take a supplement, or just prescribe them Complan or Ensure and that’s it”. “Seems to be infrequent reviews and no follow up if patients actually use supplements appropriately”. |
| Full use of range | “Many products available with little guidance about differentiating between them. It would be more helpful if, like has been done for wound care there was a Northern Ireland formulary for dietary products”. “Always the same thing prescribed, e.g., Fortisip, without utilising the specialist versions of Compact, fibre, extra whenever they would be appropriate—unless overseen by secondary care”. “I feel there is a lack of awareness of products available, by patients and healthcare professionals”. |
| More training | “I don’t think pharmacists are able to advise or comment at all appropriate supplements for patients”. “Pharmacists are not given adequate training on these products”. “I know very little about PEG feeding but these patients and their families naturally still expect advice when they are lifting their prescription items”. |
| Education Interprofessional | “A lot of the blame lies with dieticians. They rarely reach out to educate other professionals and allow charlatan nutritionists to propagate nonsense”. “Due to insufficient knowledge base and poor, if any, contact between community dietician team and pharmacist”. “GPs and community pharmacists need to work together to promote good nutrition, weight loss and a healthy lifestyle and diet”. “Not enough emphasis on the information and advice pharmacists could provide for patients”. |
| Bias | “I would be concerned about evidence for certain baby milk prescribed by GPs; it seems to me that the company reps decide what patients get—not the independent experts”. “Infant nutrition advice is limited as the training provided is usually by the formula milk companies so is biased”. |
| More training | “Lack of knowledge”. “Feel it is an important area we can recommend for health promotion but confidence in our knowledge is lacking”. “I always refer to a dietician as I do not have sufficient knowledge to advise”. “Neither doctors or pharmacists are properly trained on nutrition”. “I think there is a lot of education to be done and that poor nutrition is contributing to ill health in many of our patients”. “I believe many health professionals are missing opportunities to intervene in patient nutrition”. “Nutritional problems need to be addressed more proactively. Pharmacy needs to step up a gear to accommodate the public desire for more evidence-based education”. |
| Types of Client Groups | n | Vitamins/Supplements Mentioned | n |
|---|---|---|---|
| Elderly | 22 | Vitamin D | 27 |
| Pregnancy | 21 | Calcium | 14 |
| Children | 13 | Multivitamins/tonics | 10 |
| Teenagers/young females/childbearing age | 8 | Omega/fish oil | 7 |
| Illness/post-illness | 8 | Glucosamine | 5 |
| Housebound/little sunlight | 5 | Vitamin C | 5 |
| Iron | 4 |
| Characteristic | n (%) |
|---|---|
| Male:female | 1 (10): 9 (90) |
| Hospital:community pharmacist | 1 (10): 9 (90) |
| Rural:urban pharmacy | 2 (20): 8 (80) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Douglas, P.L.; McCarthy, H.; McCotter, L.E.; Gallen, S.; McClean, S.; Gallagher, A.M.; Ray, S. Nutrition Education and Community Pharmacy: A First Exploration of Current Attitudes and Practices in Northern Ireland. Pharmacy 2019, 7, 27. https://doi.org/10.3390/pharmacy7010027
Douglas PL, McCarthy H, McCotter LE, Gallen S, McClean S, Gallagher AM, Ray S. Nutrition Education and Community Pharmacy: A First Exploration of Current Attitudes and Practices in Northern Ireland. Pharmacy. 2019; 7(1):27. https://doi.org/10.3390/pharmacy7010027
Chicago/Turabian StyleDouglas, Pauline L., Helen McCarthy, Lynn E. McCotter, Siobhan Gallen, Stephen McClean, Alison M. Gallagher, and Sumantra Ray. 2019. "Nutrition Education and Community Pharmacy: A First Exploration of Current Attitudes and Practices in Northern Ireland" Pharmacy 7, no. 1: 27. https://doi.org/10.3390/pharmacy7010027
APA StyleDouglas, P. L., McCarthy, H., McCotter, L. E., Gallen, S., McClean, S., Gallagher, A. M., & Ray, S. (2019). Nutrition Education and Community Pharmacy: A First Exploration of Current Attitudes and Practices in Northern Ireland. Pharmacy, 7(1), 27. https://doi.org/10.3390/pharmacy7010027