1. Introduction
Warfarin is the most commonly prescribed oral anticoagulant [
1]. The newer therapeutic options for anticoagulation e.g. dabigatran and rivaroxaban, were thought to signal the demise of warfarin, and indeed they have been found to be non-inferior to warfarin therapy [
2]. Currently however, they are not without their disadvantages having no known antidote; hence warfarin will remain an important therapy for the foreseeable future. Safe and effective oral anticoagulation therapy requires an individual evaluation of each patient's clinical condition and risk factors for bleeding. Warfarin therapy requires frequent monitoring and dose adjustments are made based upon International Normalised Ratio (INR) levels to maintain anticoagulation intensity within the narrow therapeutic window [
3]. A recent review of strategies for patient education about warfarin concluded that many of the published studies were hard to compare due to the variation in the strategy, content and patient testing. The authors of this review recommended that by prioritizing the educational domains and standardizing the educational content, greater anticoagulation control and hence better outcomes could be achieved [
4]. Standardisation of content is however only one side of the story and an appreciation of patient-related factors should not be underestimated.
Health literacy can be defined as “
The degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” [
5]. Patients with limited health literacy have a fifty per cent increased risk of hospitalisation, compared with patients who had adequate health literacy skills [
6]. Patients with limited health literacy are more likely to have deficiencies in knowledge relating to warfarin’s (i) mechanism of action; (ii) side-effects; (iii) interactions; and (iv) frequency of monitoring, relative to their more health-literate counterparts [
7]. One study found that low health literacy levels increase the risk of bleeding complications (e.g., blood in urine, unusual bruising) [
8]. Properly assessing the health literacy level of individual patients or groups may avoid problems in clinical care and research. The Rapid Estimate of Adult Literacy in Medicine (REALM) tool is a word-recognition test, of 66 medical related words that increase in difficulty as the reader advances through the list to provide reading estimates for patients who read below a 9th grade level [
9]. A score of 61 or greater indicates “adequate” HL, whilst 60 or below indicates “limited” HL. The REALM also has the advantage of an administration time of less than three minutes and validation in many studies and settings [
10,
11,
12].
Patient educational brochures about anticoagulants are frequently written at a ninth-grade educational level or higher which, for patients with lower health literacy skills, can be a major obstacle to effective healthcare communication and education [
13,
14,
15]. The National Literacy Work Group on Literacy and Health in the US has suggested that written patient education materials be written at or below sixth grade level [
16]. The computerised FKGL and Flesch Reading Ease Score (FRES) available on Microsoft Office Word
®™ 2003 were used, to test the warfarin booklet provided by the hospital to patients, for quick evaluation of general reading ability [
17]. The FKGL appraises text on an American grade-school level based on the average number of syllables per word and words per sentence. The FRES ranges from 0 to 100, where a text with a lower score is harder to read than one with a higher score. The level of difficulty is calculated based upon sentence length and polysyllabic words.
A patient’s warfarin-related knowledge is a vital component in maintaining optimal therapy. Lack of sufficient patient knowledge of warfarin therapy can result in lower therapy adherence and hence poorer outcomes. Despite efforts to counsel patients we know that there is huge variation in the knowledge that patient’s possess upon initiation to warfarin therapy [
18]. Psychosocial issues including health literacy can further challenge anticoagulant patient management situations. A possible solution involves the prompt (i) identification and, (ii) decision of whether supplemental resources are required to manage the patient effectively [
19]. In a prospective study a positive correlation was observed between patients' warfarin knowledge and the number of INR values within the target range in the previous four clinic visits [
18]. Studies have found that both written and verbal information given together, rather than alone, result in not only improved knowledge, but also better patient outcomes and fewer visits to healthcare providers [
19,
20].
The Anticoagulation Knowledge Assessment (AKA) test is a validated and reliable tool for measurement of warfarin knowledge [
21]. An important consideration in the development of AKA items was that the instrument was designed to collect information from the general population including those with lower levels of literacy hence this was deemed to be more suitable for our study. The 29-question tool covers content areas such as administration, interactions, activity, diet, side effects, and monitoring.
Patients’ knowledge and anticoagulation control have been shown to improve following the inclusion of patient education as part of the warfarin management plan as well as a reduction in re-admissions. There is a paucity of evidence regarding the effectiveness of warfarin programs and there is no recognized gold standard. For this reason, there is a necessity to evaluate current warfarin education practices in University Hospital Galway (UHG). The validated warfarin knowledge tool can identify gaps in warfarin knowledge and future education can be focused upon the elimination of these deficits. As previously discussed, both low health literacy levels and deficits in warfarin knowledge are associated with poor health outcomes and a potentially significant relationship may exist between both.
2. Aim of the Study
To investigate the effect of pharmacists counselling on the warfarin knowledge of the patient receiving anticoagulation therapy.
To investigate the health literacy of the population and assess whether there were any associations between health literacy and warfarin knowledge.
3. Method
Participants were inpatients at University Hospital Galway (UHG) who met these criteria:
(a) newly commenced (had not taken warfarin previously and had started on warfarin in the hospital within the past 24 h); (b) eighteen years or older on the day of warfarin counselling; (c) spoke English as their first language; (d) absence of visual and hearing difficulties; and (e) had not been prescribed warfarin within the last 5 years.
The REALM and AKA questionnaire were modified to improve legibility for our study population by changing language from “English (U.S.)” to “English (UK)”. Brand names were also removed from the AKA questionnaire and replaced with appropriate generic medicine names. Some phrases were modified in the AKA tool to allow for a post-discharge monitoring setting other than anticoagulation clinic testing. A pass score was defined as at least 21 correct responses on the 29-item AKA questionnaire (72.4% correct) as per a previous study [
22].
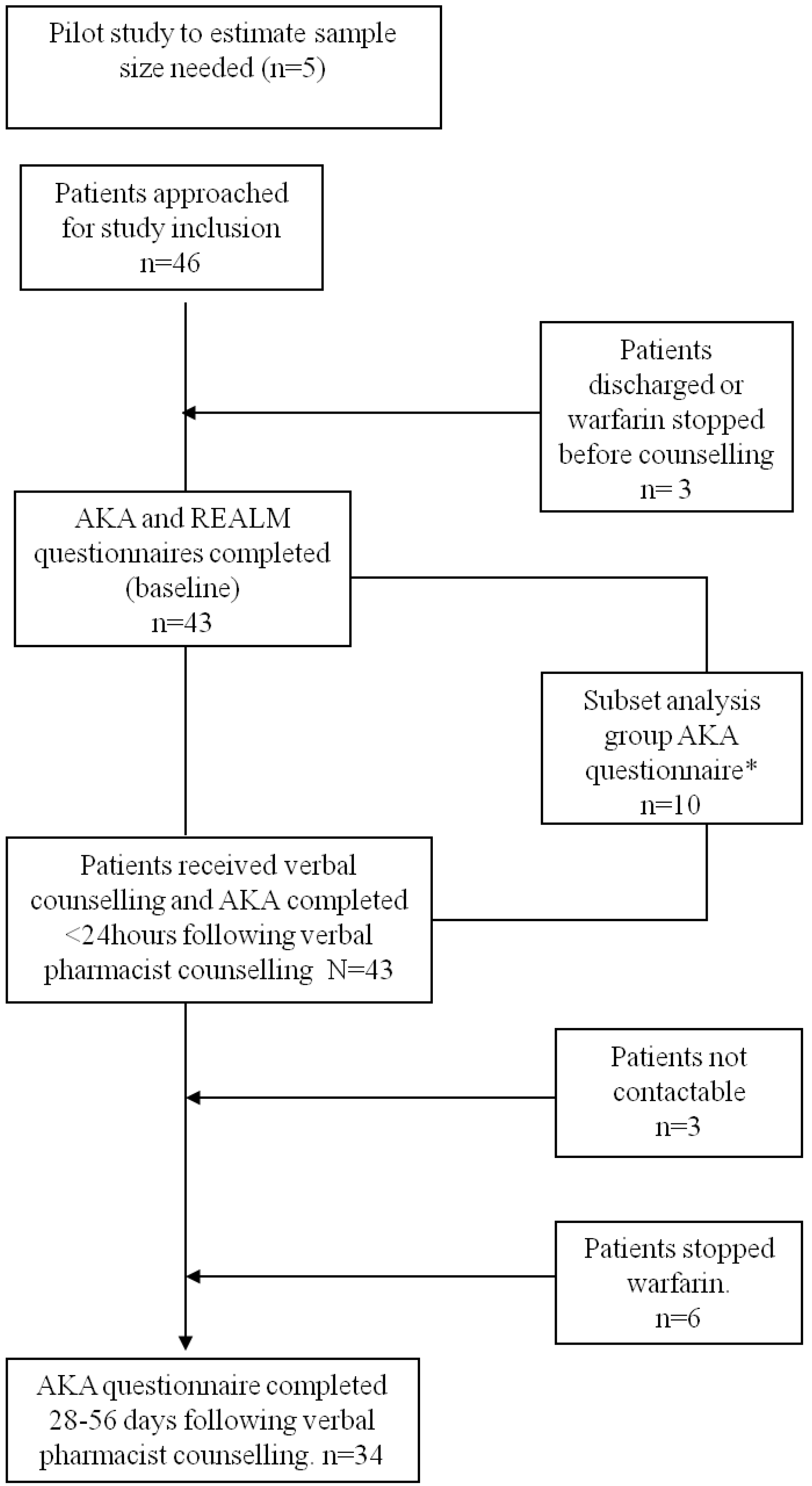
Forty six participants were recruited over an eight week period which was defined on the basis of the sample size calculation. A total of 43 patients met the criteria and consented. The verbal warfarin counselling was performed by the clinical pharmacist assigned to the ward and the investigator was excluded from performing this verbal warfarin counselling. Start and finish times of each verbal warfarin counselling session was recorded by the investigator.
These patients were given a warfarin booklet and one hour reading time. The REALM and AKA were then administered. The patients then received additional verbal counselling before the re-administration of the AKA questionnaire.
Of the 43 patients initially recruited, 34 patients were re-administered the AKA questionnaire 28–56 days after verbal counselling when followed-up via telephone. See
Figure 1.
Figure 1.
Flow diagram of patient recruitment.
Figure 1.
Flow diagram of patient recruitment.
* This is a subset analysis and describes the knowledge score of 10 patients who completed AKA questionnaires at two time points—(1) Prior to verbal pharmacist counselling (AKA at baseline); (2) Prior to verbal pharmacist counselling but 24 hours post baseline administration of the AKA.
All questionnaires were completed by the study investigator. A clinical pharmacist (n = 11) performed the verbal warfarin counselling.
The statistical analysis was performed using Predictive Analytics SoftWare (PASW®) version 18 (SPSS, Inc.; 2009, Chicago, IL, USA). A pre-defined power level of 90% was used in this study and a 2-sided alpha level of 0.05. Bi-variate analyses were conducted to determine any statistically significant relationships between varying parameters e.g., health literacy and warfarin knowledge. The limit value of statistical significance was 0.05. Normally distributed data were tested for Pearson’s Correlation whilst data that were not normally distributed were analysed using the Spearman’s Rank test. Mean ± SD are reported where appropriate.
4. Results
Forty-three patients (55.8% male), mean age 65.7 years (±14.2), 97.7% white Irish took part in the study. The main indications for warfarin were treatment of atrial fibrillation (32.6%), first-time deep vein thrombosis (DVT) (16.3%) and pulmonary embolism (PE) (16.3%).
The average REALM score was 58.5 (±9.3). Twenty-six patients (60.5%) were found to have adequate health literacy with seventeen patients exhibiting limited health literacy. (
Table 1) There was a significant negative correlation seen between age and REALM score in this study. (r = −0.375).
There was a moderate correlation (r = 0.386) found between the REALM score and the warfarin knowledge of patients prior to verbal counselling. The mean number of long term medications taken by patients was 5.2 (±3.5) with a statistically significant correlation (r = 0.532) between patient’s age and the number of medications prescribed (
Table 2).
Table 1.
Raw scores of variables (n = 43).
Table 1.
Raw scores of variables (n = 43).
| Variable | Mean | Standard Deviation | Range |
|---|
| Age | 65.72 years | 14.16 | 28−88 |
| Number of long term medications | 5.16 | 3.48 | 0−13 |
| REALM score | 58.51 | 9.25 | 30−66 |
| Correct answers to AKA at baseline | 18.98 | 4.70 | 9−27 |
| Correct answers to AKA (within 24 h of counselling) | 23.77 | 3.72 | 12−29 |
| Correct answers after 28–56 days post counselling | 22.85 | 3.69 | 16−28 |
The Paired Samples t-test performed on the total correct score for the test pre counselling (at baseline) versus post counselling gave a mean difference of −4.791 SD (3.616) and 95% confidence intervals at the lower (−5.903) and upper level (–3.678) ; t = −8.688 (df 42) and p < 0.005. The Paired Samples t-test performed on the total correct score for the test post counselling versus 1 month post counselling gave a mean difference of 1.176 SD (3.089) and 95% confidence intervals at the lower (0.099) and upper level (2.254) ; t = 2.221; (df 33) and p < 0.05.
Table 2.
Statistically significant correlations.
Table 2.
Statistically significant correlations.
| Correlated Variables | Significance (p) | Correlation (r) | N (Number of Participants) |
|---|
| Age vs. Number of Long-term Medications | 0.000 * | 0.598 | 43 |
| REALM Score vs. Total Correct Answers for AKA (at baseline) | 0.010 * | 0.386 | 43 |
| Age vs. REALM Score | 0.013 * | −0.375 | 43 |
| Age vs. Score obtained in AKA (at baseline) | 0.007 * | −0.407 | 43 |
| Scores of AKA (at baseline) vs. AKA (within 24 h of counselling) | 0.000 * | 0.653 | 43 |
| Scores of AKA (within 24 h of counselling) vs. AKA (after 28–56 days) | 0.000 * | 0.659 | 34 |
The University Hospital Galway (UHG) warfarin booklet was found to have a FKGL of 8. A person would need to have attained the equivalent of the American eighth grade level (equivalent to age 13) to be able to read it. 9.3% of the study population would not be expected to be able to read this written warfarin information.
Warfarin knowledge was seen to improve in patients from a mean score of 19.0 (SD4.7) before verbal counselling to 23.8 (SD3.7) less than 24 h after verbal counselling. This knowledge score decreased to a mean score of 22.8 (SD3.7) after 28–56 days following verbal counselling. 39.5% achieved a pass score before verbal counselling whilst 74.4% achieved it following verbal counselling. Score improvement following verbal counselling was similar in those with adequate health literacy; 4.81 (SD3.9) and those with limited health literacy 4.77 (SD3.1) (
Table 3).
Table 3.
Improvement in patients’ knowledge of patient as a function of health literacy level.
Table 3.
Improvement in patients’ knowledge of patient as a function of health literacy level.
| | Adequate Health Literacy | Limited Health Literacy | Statistical Significance between groups |
|---|
| N | 26 | 17 | |
| Improvement in Warfarin Knowledge following Verbal Counselling | Raw scores: Baseline
Mean (SD) 19.77 (4.926)
After counselling:
Mean (SD) 24.58 (2.955)
Improvement 4.81 (SD 3.9) | Raw scores: Baseline
Mean (SD) 17.76 (4.176)
After counselling:
Mean (SD) 22.53 (4.474)
Improvement: 4.77 (SD 3.1) | Not significant (NS) |
% of patients achieving pass score
Pre-verbal counselling | 50.0% | 23.5% | |
% of patients achieving pass score
Post-verbal counselling | 84.6% | 58.8% | |
| % improvement in number of patients passing following verbal counselling | 34.6% | 35.3% | |
5. Discussion
Just under 40% of the study population had limited health literacy which is higher than found in a recent Irish study [
23]. These patients may well struggle with the written materials provided to them [
9]. The negative correlation (r = −0.375) seen between age and REALM score is reflective of other literature which found health literacy to be lower amongst the elderly even after adjusting for differences in health status and visual acuity [
24].
Following comparison between the reading levels for the study population and the readability of the UHG Warfarin booklet, the results indicate that 90.7% of the study population should be able to read the UHG Warfarin Booklet. This confirms the need to provide simple, easy-to-read warfarin information, which can be read and understood by a wider population inclusive of those with low health literacy skills as suggested by the National Literacy Work Group on Literacy and Health to provide written patient education materials at or below sixth grade level [
16]. The correlation between warfarin knowledge before verbal counselling and health literacy (r = 0.386) shows that the higher the REALM score, the more likely they are to have more correct answers to the AKA test. The statistically significant improvement in warfarin knowledge following verbal counselling confirms the importance of verbal counselling. This is highlighted by the improvement in the numbers of patients who achieved a pass score from 39.5% to 74.4%. The statistically significant deterioration in warfarin knowledge after 28–56 days follow-up period highlights the importance of continuous reinforcement of warfarin information as found in other literature [
25,
26]. Despite the small reduction in warfarin knowledge in 28–56 days, it should be noted that the percentage of patients who achieved a pass score 28–56 days following counselling reduced from 79.4 to 58.1%.
When patients’ warfarin knowledge was studied in terms of their health literacy, it was found that the positive effects of counselling were beneficial regardless of health literacy level (with an improvement in knowledge score of 4.8 for both subgroups).
As shown in this study, approximately 90% of the study population would be able to read the current written warfarin information. Therefore, to appropriately assess the benefit of verbal re-enforcement of warfarin knowledge, the warfarin booklet requires modification to ensure readability for the entire study population. Review is currently underway within the hospital to make the relevant adjustments to the written material.
The study investigator was not involved in the warfarin counselling to eliminate investigator bias which could occur. Had the investigator performed verbal counselling of patients, the contents of the verbal education may be influenced by the knowledge of the design of the AKA questionnaire. None of the pharmacists who performed the verbal counselling were shown the AKA test.
Patients involved in the study were counselled by one of a possible eleven pharmacists which ensured that the study would not be affected by the educational methods used by one pharmacist specifically. The AKA and REALM test was administered with the investigator present which ensured that all study participants completed the tests fully and without eliciting assistance from other resources to help them complete the questionnaire.
Limitations
The power of the study was limited due to the small sample size, length of study period and the fact that it was conducted at a single centre, all of which will affect the generalisability of the results. The modification to the original AKA is also a limitation. It was not possible to discuss appropriateness of duration and therapeutic INR based upon the British Committee of Standards Haematology (BCSH) guidelines as prosthesis thrombogenicity risk of valve replacement patients was not measured. Any future studies wishing to examine this would require the measurement of this information.As shown in this study, approximately 90% of the study population would be able to read the current written warfarin information. Therefore, to appropriately assess the benefit of verbal re-enforcement of warfarin knowledge, the warfarin booklet requires modification to ensure readability for the entire study population. Review is currently underway within the hospital to make the relevant adjustments to the written material.
6. Conclusion
The positive correlation between health literacy and warfarin knowledge based upon information from warfarin booklet was seen in this study and confirms the importance of awareness of patients’ health literacy when providing patients with warfarin counselling. Patients were found to benefit equally from verbal counselling irrespective of their level of health literacy.
This study found that warfarin knowledge improves following pharmacist verbal counselling, however, this diminished with time when there was no further reinforcement of knowledge. This study was one of the first of its kind into this temporal relationship and demonstrates the importance of counselling and ongoing education sessions in the community setting.



{kind=link}