
Longitudinal Preceptor Assessment of Entrustable Professional Activities Across Introductory and Advanced Pharmacy Practice Experiences

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Recruitment
2.2. Data Collection
2.3. Outcomes
2.4. Data Analysis
3. Results
3.1. Unconditional Growth Curve by Preceptor Assessment
3.2. Conditional Growth Modeling for Preceptor Assessment
4. Discussion
4.1. Variation in Growth and Achievement
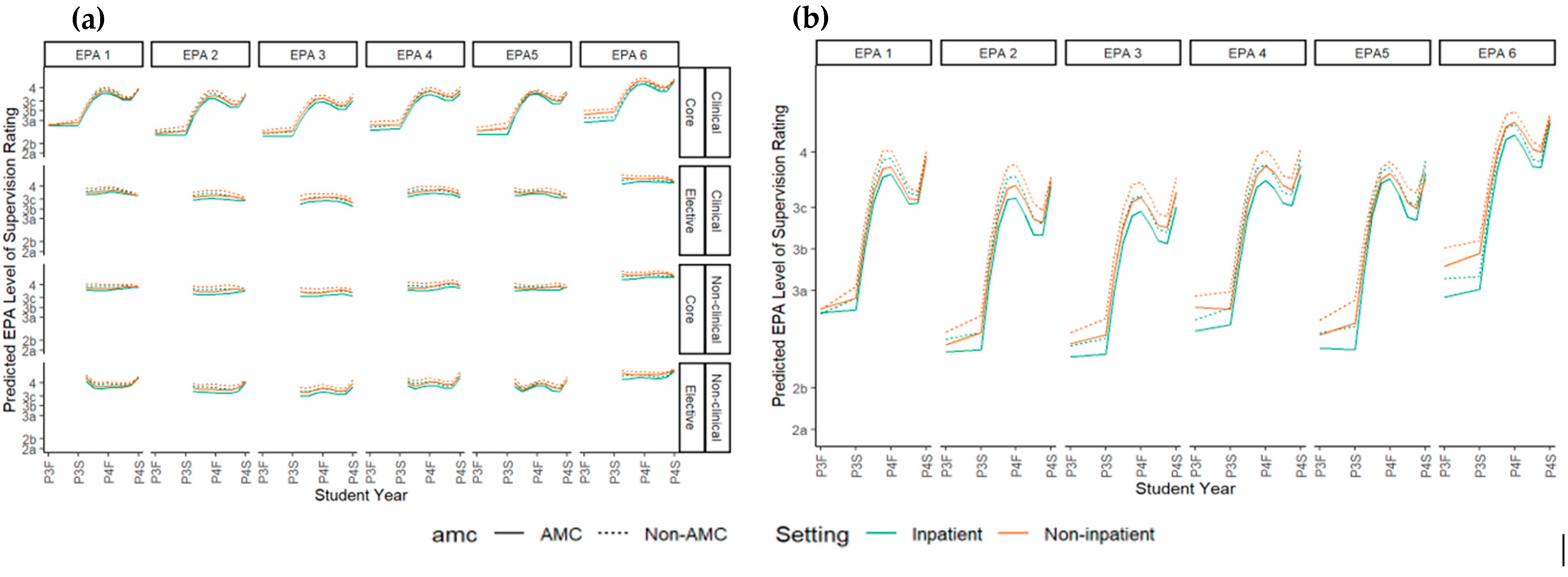
4.1.1. By Training Environment
4.1.2. By Rotation Order
4.2. Limitations
4.3. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AMC | Academic Medical Center |
| APPE | Advanced Pharmacy Practice Experience |
| ES | Entrustment–supervision |
| EPA | Entrustable professional activity |
| IPPE | Introductory Pharmacy Practice Experience |
Appendix A. Entrustable Professional Activity Integration at the University of Illinois Chicago Retzky College of Pharmacy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experiential Course | Course Description | EPA Utilization |
|---|---|---|
| PHAR 411: Introduction to Pharmacy Practice (Skills lab-based course) | Experiential core course offered in the fall semester to first professional year PharmD students. Introduces students to the practice of pharmacy through a combination of lectures, simulations, and a one-week off-site IPPE in an assigned pharmacy environment. Lectures and simulated activities cover communication skills with various audiences, interprofessional interactions, the tenets of professionalism, and medication dispensing, administration, and counseling. Students are expected to learn and recall basic drug information details from a provided list of prescription and non-prescription medications. | Pharmacy Practice Week reflection on EPA utilization at their practice site |
| PHAR 412: Community IPPE | Required experiential course where students are provided with an overview of contemporary pharmacy practice in a community setting. Develops student knowledge of the role of the Community Pharmacist through various lectures, workshops, and activities. Students also engage in a 6-week IPPE experience at a community pharmacy site where they gain valuable working knowledge of the community pharmacy environment and the roles and responsibilities of the pharmacy personnel. The goal of this experience is to engage students in an environment that will enable them to observe and develop the skills necessary to practice in a community setting. At the conclusion of this experience students should be comfortable with interpreting a prescription, filling a prescription, and providing patient counseling at a beginner’s level under pharmacist supervision. | Mid-point and final assessments by preceptor Mid-point and final self-assessment by student |
| PHAR 413: Hospital IPPE | Required experiential course where students are provided an overview of contemporary pharmacy practice in a hospital setting. Students spend most of their time engaged in actual (off-site at a hospital pharmacy) or simulated (on-site) hospital pharmacy practice activities. The goal of this course is to expand student understanding of the medication use process in a hospital setting, roles and responsibilities of pharmacists and technicians, as well as an introduction to interprofessional team dynamics. At the conclusion of this course, students should be comfortable with interpreting a medication order, correctly compounding an intravenous medication, verifying, and checking the accuracy of a filled medication order prior to dispensing, and communicating with members of the hospital team. Goals are expected to be completed under pharmacist supervision. | Mid-point and final assessments by preceptor Mid-point and final self-assessment by student |
| PHAR 414: Introduction to Patient Care (Skills lab-based course) | Fourth of six experiential courses required to complete the PharmD program. Students are introduced to the skills necessary to provide direct patient care. The goal of this course is to develop the skills necessary for communication of a pharmacotherapeutic recommendation both verbally and in writing. Upon course completion, students should be comfortable with conducting a medication history, performing medication reconciliation, optimizing pharmacotherapeutic regimens, presenting patient cases, and documenting in the Subjective/Objective/Assessment/Plan (SOAP) note format. | EPA surveys are utilized for student self-reflection after each simulation lab |
| PHAR 515: Institutional/Hospital IPPE | Designed to aid third year pharmacy students with the transition to APPEs. The primary setting for this course is in a direct patient care setting in a hospital where the student applies the didactic and early experiential coursework to the patient care setting. | Mid-point and final assessments by preceptor Mid-point and final self-assessment by student |
| PHAR 516: Ambulatory Care/Community IPPE | PHAR 516 is the Patient Care in an Ambulatory Care/Community setting course in the IPPE) series designed to aid third year pharmacy students with the transition to APPEs. The primary setting for this course is in a direct patient care setting in a hospital where the student will apply the didactic and early experiential coursework to the patient care setting. | Mid-point and final assessments by preceptor Mid-point and final self-assessment by student |
| Advanced Pharmacy Practice Experiences (APPE) | Students are required to complete seven APPEs consisting of four required core areas (Hospital (PHAR 603), Community (PHAR 602), Inpatient General Medicine (PHAR 604), and Ambulatory Care (PHAR 601)) and three elective areas. Each rotation is six weeks long and across different health systems for a broad range of direct and indirect patient care experiences. | Mid-point and final assessments by preceptor Mid-point and final self-assessment by student |
| IPPE | APPE | |||||||
|---|---|---|---|---|---|---|---|---|
| Community (PHAR 412) | Hospital (PHAR 413) | Ambulatory Care (PHAR 516) | Hospital Inpatient (PHAR 515) | Community (PHAR 602) | Hospital (PHAR 603) | Ambulatory Care (PHAR 601) | Inpatient Medicine (PHAR 604) | |
| Patient Care Provider Domain | ||||||||
| x | x | x | x | x | x | ||
| x | x | x | x | ||||
| x | x | x | x | ||||
| x | x | x | x | ||||
| x | x | x | x | ||||
| Interprofessional Team Member Domain | ||||||||
| x | x | x | x | x | x | x | x |
| Population Health Promoter Domain | ||||||||
| x | x | ||||||
| x | x | x | x | ||||
| x | x | x | x | ||||
| x | x | ||||||
| Information Master Domain | ||||||||
| x | x | x | x | x | x | ||
| x | x | x | x | ||||
| Practice Manager Domain | ||||||||
| x | x | x | x | ||||
| x | x | x | x | ||||
| Self-developer Domain | ||||||||
| x | |||||||
Appendix B. Modeled Response Level Mapped to Entrustment–Supervision Level
| Mapped Response Level | ||
|---|---|---|
| Level | Linear Model | Ordinal Model |
| Not Observed | 0 | 1 |
| 1a | 1 | 2 |
| 1b | 1.3 | 3 |
| 2a | 2 | 4 |
| 2b | 2.3 | 5 |
| 3a | 3 | 6 |
| 3b | 3.3 | 7 |
| 3c | 3.6 | 8 |
| 4 | 4 | 9 |
| 5 | 5 | 10 |
Appendix C. Preceptor Assessment of Student Performance in Entrustable Professional Activities
| Number of Assessments by Graduation Year | ||
|---|---|---|
| Graduation Year | Students (n) | Assessments per Student (n) |
| 2022 | 190 | 8748 |
| 2023 | 163 | 1887 |
| 2024 | 156 | 1791 |
| Number of Assessments per EPA by Preceptors | ||
| EPA | Assessments by Preceptors (n) | |
| 1 | 2110 | |
| 2 | 2134 | |
| 3 | 2030 | |
| 4 | 2013 | |
| 5 | 1981 | |
| 6 | 2158 | |
| Comparator | EPA | Difference in ES Level | p-Value |
|---|---|---|---|
| Based on setting for any point in time | |||
| Inpatient to Outpatient | 1 | −0.05 | 0.02 |
| Inpatient to Outpatient | 2 | −0.09 | <0.05 |
| Inpatient to Outpatient | 3 | −0.11 | <0.05 |
| Inpatient to Outpatient | 4 | −0.12 | <0.05 |
| Inpatient to Outpatient | 5 | −0.10 | <0.05 |
| Inpatient to Outpatient | 6 | −0.07 | <0.05 |
| AMC to non-AMC | 1 | −0.07 | 0.01 |
| AMC to non-AMC | 2 | −0.12 | <0.05 |
| AMC to non-AMC | 3 | −0.10 | <0.05 |
| AMC to non-AMC | 4 | −0.11 | <0.05 |
| AMC to non-AMC | 5 | −0.12 | <0.05 |
| AMC to non-AMC | 6 | −0.09 | <0.05 |
References
- Rhoney, D.H.; Chen, A.M.H.; Churchwell, M.D.; Daugherty, K.K.; Jarrett, J.B.; Kleppinger, E.L.; Nawarskas, J.J.; Sibicky, S.L.; Stowe, C.D.; Meyer, S.M. Recommendations and Next Steps For Competency-Based Pharmacy Education. Am. J. Pharm. Educ. 2023, 87, 100549. [Google Scholar] [CrossRef] [PubMed]
- Medina, M.S.; Plaza, C.M.; Stowe, C.D.; Robinson, E.T.; DeLander, G.; Beck, D.E.; Melchert, R.B.; Supernaw, R.B.; Roche, V.F.; Gleason, B.L.; et al. Center for the Advancement of Pharmacy Education 2013 Educational Outcomes. Am. J. Pharm. Educ. 2013, 77, 162. [Google Scholar] [CrossRef]
- Medina, M.S.; Farland, M.Z.; Conry, J.M.; Culhane, N.; Kennedy, D.R.; Lockman, K.; Malcom, D.R.; Mirzaian, E.; Vyas, D.; Stolte, S.; et al. The AACP Academic Affairs Committee’s Final 2022 Curricular Outcomes and Entrustable Professional Activities (COEPA) for Pharmacy Graduates to Replace 2013 CAPE and 2016 EPAs. Am. J. Pharm. Educ. 2023, 87, 100558. [Google Scholar] [CrossRef]
- Joint Commission of Pharmacy Practitioners. Pharmacists’ Patient Care Process. Available online: https://jcpp.net/wp-content/uploads/2016/03/PatientCareProcess-with-supporting-organizations.pdf (accessed on 15 April 2025).
- Accreditation Council for Pharmacy Education (ACPE). Accreditation Standards and Key Elements for the Professional Program in Pharmacy Leading to the Doctor of Pharmacy Degree (Standards 2016). Available online: https://www.acpe-accredit.org/pdf/ACPEStandards2016FINAL.pdf (accessed on 15 April 2025).
- Haines, S.T.; Pittenger, A.L.; Stolte, S.K.; Plaza, C.M.; Gleason, B.L.; Kantorovich, A.; McCollum, M.; Trujillo, J.M.; Copeland, D.A.; Lacroix, M.M.; et al. Core Entrustable Professional Activities for New Pharmacy Graduates. Am. J. Pharm. Educ. 2017, 81, S2. [Google Scholar] [CrossRef]
- Accreditation Council for Pharmacy Education. Accreditation Standards and Key Elements for the Professional Program in Pharmacy Leading to the Doctor of Pharmacy Degree. Available online: https://www.acpe-accredit.org/pdf/Standard2025DRAFTForComment.pdf (accessed on 15 April 2025).
- Jarrett, J.B.; Berenbrok, L.A.; Goliak, K.L.; Meyer, S.M.; Shaughnessy, A.F. Entrustable Professional Activities as a Novel Framework for Pharmacy Education. Am. J. Pharm. Educ. 2018, 82, 6256. [Google Scholar] [CrossRef] [PubMed]
- Cate, O.T. Nuts and Bolts of Entrustable Professional Activities. J. Grad. Med. Educ. 2013, 5, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Pittenger, A.L.; Chapman, S.A.; Frail, C.K.; Moon, J.Y.; Undeberg, M.R.; Orzoff, J.H. Entrustable Professional Activities for Pharmacy Practice. Am. J. Pharm. Educ. 2016, 80, 57. [Google Scholar] [CrossRef]
- Rekman, J.; Gofton, W.; Dudek, N.; Gofton, T.; Hamstra, S.J. Entrustability scales: Outlining their usefulness for competency-based clinical assessment. Acad. Med. 2016, 91, 186–190. [Google Scholar] [CrossRef]
- Marshall, L.L.; Kinsey, J.; Nykamp, D.; Momary, K. Evaluating Practice Readiness of Advanced Pharmacy Practice Experience Students Using the Core Entrustable Professional Activities. Am. J. Pharm. Educ. 2020, 84, ajpe7853. [Google Scholar] [CrossRef]
- Lounsbery, J.L.; Von Hoff, B.A.; Chapman, S.A.; Frail, C.K.; Moon, J.Y.; Philbrick, A.M.; Rivers, Z.; Pereira, C. Tracked Patient Encounters During Advanced Pharmacy Practice Experiences and Skill Self-assessment Using Entrustable Professional Activities. Am. J. Pharm. Educ. 2019, 83, 1857–1861. [Google Scholar] [CrossRef]
- Chen, H.C.M.; van den Broek, W.E.S.; Cate, O.T. The Case for Use of Entrustable Professional Activities in Undergraduate Medical Education. Acad. Med. 2015, 90, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, J.B.; Goliak, K.L.; Haines, S.T.; Trolli, E.; Schwartz, A. Development of an Entrustment-Supervision Assessment Tool for Pharmacy Experiential Education Using Stakeholder Focus Groups. Am. J. Pharm. Educ. 2022, 86, 8523. [Google Scholar] [CrossRef] [PubMed]
- Camargo, L.M.A.; Silva, R.P.M.; Meneguetti, D.U.d.O. Research methodology topics: Cohort studies or prospective and retrospective cohort studies. J. Hum. Growth Dev. 2019, 29, 433–436. [Google Scholar] [CrossRef]
- Schwartz, A.; Borman-Shoap, E.; Carraccio, C.; Herman, B.; Hobday, P.M.; Kaul, P.; Long, M.; O’connor, M.; Mink, R.M.; Schumacher, D.J.M.; et al. Learner Levels of Supervision Across the Continuum of Pediatrics Training. Acad. Med. 2021, 96, S42–S49. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.N. Generalized Additive Models: An Introduction with R, 2nd ed.; Chapman and Hall/CRC: London, UK, 2017. [Google Scholar]
- Rhodes, L.A.; Marciniak, M.W.; McLaughlin, J.; Melendez, C.R.; Leadon, K.I.; Pinelli, N.R. Exploratory Analysis of Entrustable Professional Activities as a Performance Measure During Early Pharmacy Practice Experiences. Am. J. Pharm. Educ. 2019, 83, 212–223. [Google Scholar] [CrossRef]
- Smith, C.; Stewart, R.; Smith, G.; Anderson, H.G.; Baggarly, S. Developing and Implementing an Entrustable Professional Activity Assessment for Pharmacy Practice Experiences. Am. J. Pharm. Educ. 2020, 84, 1178–1184. [Google Scholar] [CrossRef]
- Nigro, S.C.; Gernant, S.A.; Csere, M.; Sobieraj, D.M. Determining preceptor perceptions of APPE readiness through the use of entrustable professional activities. Curr. Pharm. Teach. Learn. 2023, 15, 956–960. [Google Scholar] [CrossRef]
- Haines, S.T.; Gleason, B.L.; Kantorovich, A.; McCollum, M.; Pittenger, A.L.; Plaza, C.M.; Stolte, S.K.; Trujillo, J.M. Report of the 2015–2016 Academic Affairs Standing Committee. Am. J. Pharm. Educ. 2016, 80, S20. [Google Scholar] [CrossRef]
- Cate, O.T.; Jarrett, J.B. Would I Trust or Will I Trust? The Gap between Entrustment Determinations and Entrustment Decisions for Trainees in Pharmacy and Other Health Professions. Pharmacy 2023, 11, 107. [Google Scholar] [CrossRef]
- Alanazi, M.A.; Tully, M.P.; Lewis, P.J. A systematic review of the prevalence and incidence of prescribing errors with high-risk medicines in hospitals. J. Clin. Pharm. Ther. 2016, 41, 239–245. [Google Scholar] [CrossRef]
- Young, J.Q.; Van Merrienboer, J.; Durning, S.; Cate, O.T. Cognitive Load Theory: Implications for medical education: AMEE Guide No. 86. Med. Teach. 2014, 36, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Ogur, B.; Hirsh, D.; Krupat, E.; Bor, D. The Harvard Medical School-Cambridge Integrated Clerkship: An Innovative Model of Clinical Education. Acad. Med. 2007, 82, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Tayade, M.C.; Latti, R.G. Effectiveness of early clinical exposure in medical education: Settings and scientific theories—Review. J. Educ. Health Promot. 2021, 10, 117. [Google Scholar] [CrossRef]
- Marty, A.P.; Braun, J.; Schick, C.; Zalunardo, M.P.; Spahn, D.R.; Breckwoldt, J. A mobile application to facilitate implementation of programmatic assessment in anaesthesia training. Br. J. Anaesth. 2022, 128, 990–996. [Google Scholar] [CrossRef] [PubMed]
| Level | Entrustment–Supervision Statement |
|---|---|
| 1a | I would not trust the learner to perform or even observe this task. The learner lacks the professional behavior, knowledge, and related skill to perform or even observe this task. |
| 1b | I would trust the learner to thoughtfully observe (but not perform) this task. The learner has foundational knowledge and skill about the task. |
| 2a | I would trust the learner to perform this task WITH the preceptor and under full supervision. The learner will require direction, guidance and help during their performance of the task. |
| 2b | I would trust the learner to perform this task under full supervision and the preceptor ready to step in, as needed. The learner is new in performing the task alone and guidance should be immediately available during the task. |
| 3a | I would trust the learner to perform this task with on-demand, nearby preceptor supervision and ALL findings and work are checked immediately afterward. |
| 3b | I would trust the learner to perform this task with on-demand, nearby preceptor supervision and KEY findings and work are checked immediately afterward. |
| 3c | I would trust the learner to perform this task with on-demand, remote preceptor supervision and findings and work is audited soon afterward. |
| 4 | I would trust the learner to perform this task independently and unsupervised. |
| 5 | I would trust the learner to perform this task independently as well as to supervise and teach other learners. |
| Not Observed | Not applicable to this practice setting. |
| Characteristic | Class of 2022 (n = 196) | Class of 2023 (n = 176) | Class of 2024 (n = 186) | |
|---|---|---|---|---|
| Gender, n (%) | Male | 67 (34%) | 69 (37%) | 79 (45%) |
| Female | 129 (66%) | 117 (63%) | 97 (55%) | |
| Age, Mean (Range) | Years | 23 (19–42) | 24 (19–43) | 24 (19–49) |
| Residence, n (%) | Illinois | 144 (73%) | 143 (77%) | 135 (77%) |
| Other US State | 47 (24%) | 35 (19%) | 41 (23%) | |
| International | 5 (3%) | 8 (4%) | 0 (0%) | |
| Highest Degree on Acceptance, n (%) | Associate | 13 (7%) | 26 (14%) | 20 (11%) |
| Bachelor | 159 (81%) | 116 (62%) | 130 (74%) | |
| Master | 4 (2%) | 8 (4%) | 8 (5%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarrett, J.B.; Elmes-Patel, A.T.; Allen, S.M.; Djuric Kachlic, M.; Schriever, A.E.; Driscoll, T.P.; Tekian, A.; Cheung, J.J.H.; Podsiadlik, E.; Haines, S.T.; et al. Longitudinal Preceptor Assessment of Entrustable Professional Activities Across Introductory and Advanced Pharmacy Practice Experiences. Pharmacy 2025, 13, 72. https://doi.org/10.3390/pharmacy13030072
Jarrett JB, Elmes-Patel AT, Allen SM, Djuric Kachlic M, Schriever AE, Driscoll TP, Tekian A, Cheung JJH, Podsiadlik E, Haines ST, et al. Longitudinal Preceptor Assessment of Entrustable Professional Activities Across Introductory and Advanced Pharmacy Practice Experiences. Pharmacy. 2025; 13(3):72. https://doi.org/10.3390/pharmacy13030072
Chicago/Turabian StyleJarrett, Jennie B., Abigail T. Elmes-Patel, Sheila M. Allen, Marlowe Djuric Kachlic, Allison E. Schriever, Tara P. Driscoll, Ara Tekian, Jeffrey J. H. Cheung, Edward Podsiadlik, Stuart T. Haines, and et al. 2025. "Longitudinal Preceptor Assessment of Entrustable Professional Activities Across Introductory and Advanced Pharmacy Practice Experiences" Pharmacy 13, no. 3: 72. https://doi.org/10.3390/pharmacy13030072
APA StyleJarrett, J. B., Elmes-Patel, A. T., Allen, S. M., Djuric Kachlic, M., Schriever, A. E., Driscoll, T. P., Tekian, A., Cheung, J. J. H., Podsiadlik, E., Haines, S. T., & Schwartz, A. (2025). Longitudinal Preceptor Assessment of Entrustable Professional Activities Across Introductory and Advanced Pharmacy Practice Experiences. Pharmacy, 13(3), 72. https://doi.org/10.3390/pharmacy13030072