
Considering the Possible Role of Pharmacists According to the Presence or Absence of Lifestyle-Related Diseases at the Time of Coronary CT Examination and Trends of Medication Use for These Diseases by Medical Doctors

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement of Coronary Stenosis by CCTA
2.3. Assessments of Patient Characteristics including Coronary Risk Factors, Medications, Etc.
2.4. Measurement of baPWV
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics in All Patients and in the Absence or Presence of CAD
3.2. Medications of All Patients and in the Absence or Presence of CAD
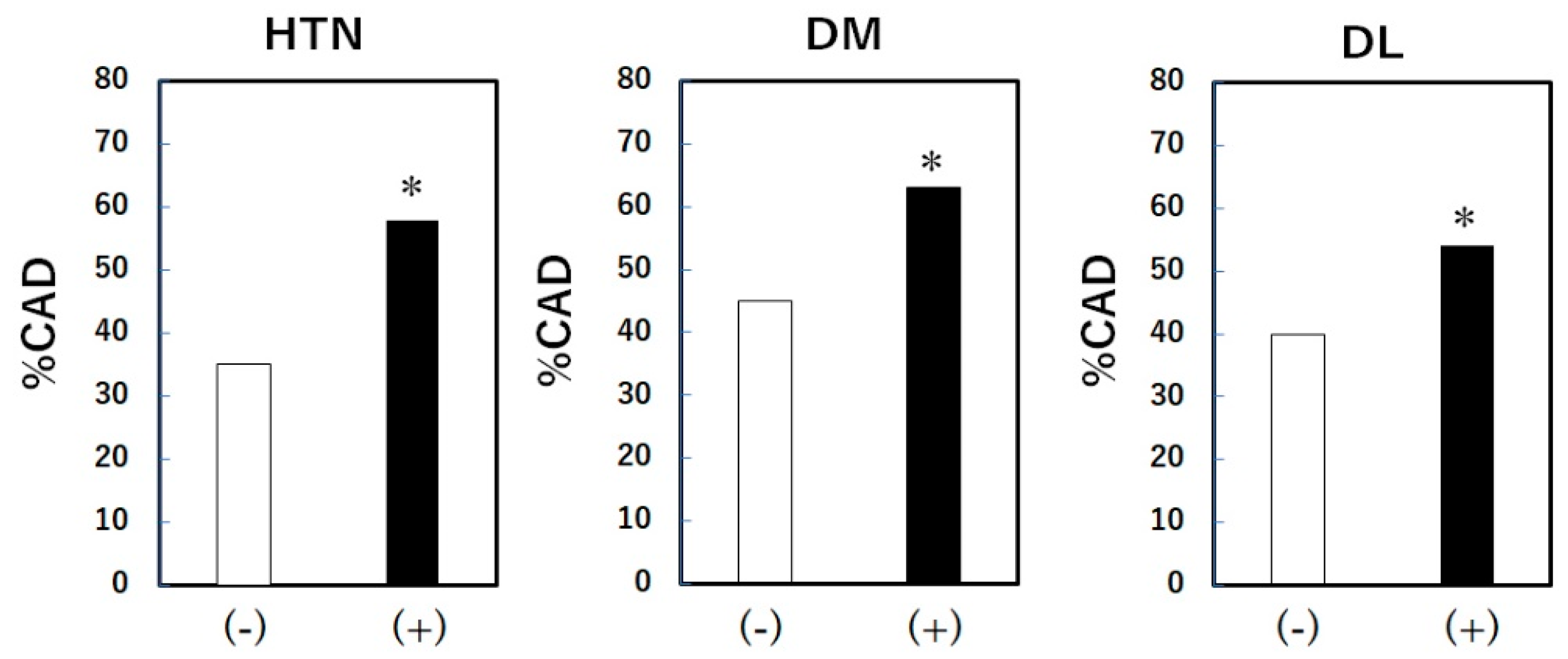
3.3. The % CAD in the Absence or Presence of HTN, DL and DM
3.4. Control Conditions of HTN, DM and DL
3.5. Medications for HTN, DM and DL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tachibana, T.; Shiga, Y.; Hirata, T.; Tashiro, K.; Higashi, S.; Kawahira, Y.; Kato, Y.; Kuwano, T.; Sugihara, M.; Miura, S.I. Association Between the Presence of Coronary Artery Disease or Peripheral Artery Disease and Left Ventricular Mass in Patients Who Have Undergone Coronary Computed Tomography Angiography. Cardiol. Res. 2023, 14, 387–395. [Google Scholar] [CrossRef]
- Hirata, T.; Shiga, Y.; Tashiro, K.; Higashi, S.; Tachibana, T.; Kawahira, Y.; Suematsu, Y.; Kuwano, T.; Sugihara, M.; Miura, S.I. Investigating the Association between Coronary Artery Disease and the Liver Fibrosis-4 Index in Patients Who Underwent Coronary Computed Tomography Angiography: A Cross-Sectional Study. J. Cardiovasc. Dev. Dis. 2023, 10, 301. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, K.; Ishikawa, H.; Yamaura, H.; Hojo, K.; Kono, Y.; Shimada, K.; Kasayuki, N.; Fukuda, D. Thoracic Aortic Plaque Burden and Prediction of Cardiovascular Events in Patients Undergoing 320-row Multidetector CT Coronary Angiography. J. Atheroscler. Thromb. 2024, 31, 273–287. [Google Scholar] [CrossRef]
- Koide, Y.; Miyoshi, T.; Nishihara, T.; Nakashima, M.; Ichikawa, K.; Miki, T.; Osawa, K.; Ito, H. The Association of Triglyceride to High-Density Lipoprotein Cholesterol Ratio with High-Risk Coronary Plaque Characteristics Determined by CT Angiography and Its Risk of Coronary Heart Disease. J. Cardiovasc. Dev. Dis. 2022, 9, 329. [Google Scholar] [CrossRef]
- Omboni, S.; Caserini, M. Effectiveness of pharmacist’s intervention in the management of cardiovascular diseases. Open Heart 2018, 5, e000687. [Google Scholar] [CrossRef]
- Swieczkowski, D.; Merks, P.; Gruchala, M.; Jaguszewski, M.J. The role of the pharmacist in the care of patients with cardiovascular diseases. Kardiol. Pol. 2016, 74, 1319–1326. [Google Scholar] [CrossRef]
- Santschi, V.; Chiolero, A.; Colosimo, A.L.; Platt, R.W.; Taffé, P.; Burnier, M.; Burnand, B.; Paradis, G. Improving blood pressure control through pharmacist interventions: A meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2014, 3, e000718. [Google Scholar] [CrossRef]
- Ajimu, Y.; Shiga, Y.; Hirata, T.; Tashiro, K.; Higashi, S.; Kawahira, Y.; Suematsu, Y.; Kato, Y.; Kuwano, T.; Sugihara, M.; et al. Association between Major Adverse Cardiovascular Events and the Liver Fibrosis Score in Patients with and without Coronary Artery Disease: From the FU-CCTA Registry. J. Clin. Med. 2023, 12, 5987. [Google Scholar] [CrossRef]
- Ohnishi, N.; Shiga, Y.; Tashiro, K.; Kawahira, Y.; Shibata, Y.; Inoue, H.; Morii, J.; Nishikawa, H.; Kato, Y.; Kuwano, T.; et al. Association between major adverse cardiovascular events and pentraxin-3 in patients who have undergone coronary computed tomography angiography: From the FU-CCTA registry. Heart Vessel. 2023, 38, 309–317. [Google Scholar] [CrossRef]
- Imaizumi, T.; Shiga, Y.; Idemoto, Y.; Tashiro, K.; Ueda, Y.; Yano, Y.M.; Norimatsu, K.; Nakamura, A.; Kuwano, T.; Iwata, A.; et al. Associations between the psoas major muscle index and the presence and severity of coronary artery disease. Medicine 2020, 99, e21086. [Google Scholar] [CrossRef]
- Inoue, H.; Shiga, Y.; Norimatsu, K.; Tashiro, K.; Futami, M.; Suematsu, Y.; Sugihara, M.; Nishikawa, H.; Katsuda, Y.; Miura, S.I. Associations between High-Density Lipoprotein Functionality and Major Adverse Cardiovascular Events in Patients Who Have Undergone Coronary Computed Tomography Angiography. J. Clin. Med. 2021, 10, 2431. [Google Scholar] [CrossRef]
- Mitsutake, R.; Niimura, H.; Miura, S.; Zhang, B.; Iwata, A.; Nishikawa, H.; Kawamura, A.; Kumagai, K.; Shirai, K.; Matsunaga, A.; et al. Clinical significance of the coronary calcification score by multidetector row computed tomography for the evaluation of coronary stenosis in Japanese patients. Circ. J. 2006, 70, 1122–1127. [Google Scholar] [CrossRef]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar]
- Okamura, T.; Tsukamoto, K.; Arai, H.; Fujioka, Y.; Ishigaki, Y.; Koba, S.; Ohmura, H.; Shoji, T.; Yokote, K.; Yoshida, H.; et al. Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2022. J. Atheroscler. Thromb. 2023, 31, 641–853. [Google Scholar]
- American Diabetes Association. Screening for type 2 diabetes. Diabetes Care 2004, 27, S11–S14. [Google Scholar] [CrossRef]
- Milman, T.; Joundi, R.A.; Alotaibi, N.M.; Saposnik, G. Clinical inertia in the pharmacological management of hypertension: A systematic review and meta-analysis. Medicine 2018, 97, e11121. [Google Scholar] [CrossRef]
- Kosoglou, T.; Statkevich, P.; Johnson-Levonas, A.O.; Paolini, J.F.; Bergman, A.J.; Alton, K.B. Ezetimibe: A review of its metabolism, pharmacokinetics and drug interactions. Clin. Pharmacokinet. 2005, 44, 467–494. [Google Scholar] [CrossRef]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278, Erratum in Lancet 2005, 366, 1358; Erratum in Lancet 2008, 371, 2084. [Google Scholar]
- Pauriah, M.; Elder, D.H.; Ogston, S.; Noman, A.Y.; Majeed, A.; Wyatt, J.C.; Choy, A.M.; Macdonald, T.M.; Struthers, A.D.; Lang, C.C. High-potency statin and ezetimibe use and mortality in survivors of an acute myocardial infarction: A population-based study. Heart 2014, 100, 867–872. [Google Scholar] [CrossRef]
- Jang, J.Y.; Kim, S.; Cho, J.; Chun, S.Y.; You, S.C.; Kim, J.S. Comparative effectiveness of moderate-intensity statin with ezetimibe therapy versus high-intensity statin monotherapy in patients with acute coronary syndrome: A nationwide cohort study. Sci. Rep. 2024, 14, 838. [Google Scholar] [CrossRef]
- Ahrén, B. Novel combination treatment of type 2 diabetes DPP-4 inhibition + metformin. Vasc. Health Risk Manag. 2008, 4, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Lyu, Y.S.; Oh, S.; Kim, J.H.; Kim, S.Y.; Jeong, M.H. Comparison of SGLT2 inhibitors with DPP-4 inhibitors combined with metformin in patients with acute myocardial infarction and diabetes mellitus. Cardiovasc. Diabetol. 2023, 22, 185, Erratum in Cardiovasc. Diabetol. 2023, 22, 242. [Google Scholar] [CrossRef] [PubMed]
- Blacher, J.; Asmar, R.; Djane, S.; London, G.M.; Safar, M.E. Aortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patients. Hypertension 1999, 33, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Blacher, J.; Guerin, A.P.; Pannier, B.; Marchais, S.J.; Safar, M.E.; London, G.M. Impact of aortic stiffness on survival in end-stage renal disease. Circulation 1999, 99, 2434–2439. [Google Scholar] [CrossRef]
- Cruickshank, K.; Riste, L.; Anderson, S.G.; Wright, J.S.; Dunn, G.; Gosling, R.G. Aortic pulse-wave velocity and its relationship to mortality in diabetes and glucose intolerance: An integrated index of vascular function? Circulation 2002, 106, 2085–2090. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| All Patients | CAD (-) Group | CAD (+) Group | CAD (-) Vs. CAD (+) | ||
|---|---|---|---|---|---|
| (n = 1357) | (n = 678) | (n = 668) | p-Value | ||
| Age | yrs. | 66 ± 12 | 62 ± 13 | 69 ± 10 | <0.01 |
| Gender (male) | % | 49 | 41 | 57 | <0.01 |
| Family history | % | 22 | 23 | 22 | 0.466 |
| Smoking | % | 34 | 30 | 39 | <0.01 |
| BMI | kg/m2 | 24 ± 4 | 24 ± 4 | 24 ± 4 | 0.348 |
| HTN | % | 65 | 55 | 76 | <0.01 |
| DM | % | 25 | 19 | 32 | <0.01 |
| DL | % | 68 | 62 | 74 | <0.01 |
| CKD | % | 27 | 23 | 32 | <0.01 |
| eGFR | mL/min/1.73 m2 | 68 ± 16 | 70 ± 15 | 66 ± 17 | <0.01 |
| MetS | % | 25 | 19 | 31 | <0.01 |
| Mean baPWV | cm/sec | 1635 ± 355 | 1626 ± 368 | 1647 ± 342 | 0.292 |
| Medications | All Patients | CAD (-) Group | CAD (+) Group | CAD (-) Vs. CAD (+) | |
|---|---|---|---|---|---|
| (n = 1357) | (n = 678) | (n = 668) | p-Value | ||
| ACEI/ARB | % | 36 | 29 | 43 | <0.01 |
| CCB | % | 39 | 31 | 47 | <0.01 |
| β-blocker | % | 9 | 6 | 11 | <0.01 |
| Diuretic | % | 8 | 7 | 10 | 0.091 |
| Statin | % | 32 | 24 | 39 | <0.01 |
| EPA | % | 3 | 2 | 3 | 0.409 |
| Ezetimibe | % | 2 | 3 | 2 | 0.482 |
| Fibrate | % | 1 | 1 | 1 | 0.449 |
| SU | % | 6 | 4 | 9 | <0.01 |
| α-GI | % | 2 | 1 | 3 | 0.027 |
| Biguanide | % | 6 | 5 | 8 | 0.017 |
| Thiazolidine | % | 2 | 2 | 3 | 0.479 |
| DPP-4I | % | 10 | 8 | 13 | 0.002 |
| GLP-1 | % | 0.3 | 0.3 | 0.3 | 1.000 |
| Insulin | % | 3 | 2 | 3 | 0.731 |
| Medications | HTN (+) | Medications | DL (+) | Medications | DM (+) | |||
|---|---|---|---|---|---|---|---|---|
| (n = 883) | (n = 913) | (n = 342) | ||||||
| ACEI/ARB | % | 52 | Statin | % | 47 | SU | % | 25 |
| CCB | % | 58 | EPA | % | 4 | α-GI | % | 9 |
| β-blocker | % | 13 | Ezetimibe | % | 4 | Biguanide | % | 25 |
| Diuretic | % | 13 | Fibrate | % | 2 | Thiazolidine | % | 41 |
| ARB + CCB | % | 34 | Statin + Ezetimibe | % | 2 | DPP-4I | % | 41 |
| GLP-1 | % | 1 | ||||||
| Insulin | % | 10 | ||||||
| Biguanide + DPP-4I | % | 14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miura-Takahashi, E.; Tashiro, K.; Shiga, Y.; Kawahira, Y.; Higashi, S.; Otsu, Y.; Kamimura, H.; Miura, S.-i. Considering the Possible Role of Pharmacists According to the Presence or Absence of Lifestyle-Related Diseases at the Time of Coronary CT Examination and Trends of Medication Use for These Diseases by Medical Doctors. Pharmacy 2024, 12, 99. https://doi.org/10.3390/pharmacy12040099
Miura-Takahashi E, Tashiro K, Shiga Y, Kawahira Y, Higashi S, Otsu Y, Kamimura H, Miura S-i. Considering the Possible Role of Pharmacists According to the Presence or Absence of Lifestyle-Related Diseases at the Time of Coronary CT Examination and Trends of Medication Use for These Diseases by Medical Doctors. Pharmacy. 2024; 12(4):99. https://doi.org/10.3390/pharmacy12040099
Chicago/Turabian StyleMiura-Takahashi, Erika, Kohei Tashiro, Yuhei Shiga, Yuto Kawahira, Sara Higashi, Yuki Otsu, Hidetoshi Kamimura, and Shin-ichiro Miura. 2024. "Considering the Possible Role of Pharmacists According to the Presence or Absence of Lifestyle-Related Diseases at the Time of Coronary CT Examination and Trends of Medication Use for These Diseases by Medical Doctors" Pharmacy 12, no. 4: 99. https://doi.org/10.3390/pharmacy12040099
APA StyleMiura-Takahashi, E., Tashiro, K., Shiga, Y., Kawahira, Y., Higashi, S., Otsu, Y., Kamimura, H., & Miura, S.-i. (2024). Considering the Possible Role of Pharmacists According to the Presence or Absence of Lifestyle-Related Diseases at the Time of Coronary CT Examination and Trends of Medication Use for These Diseases by Medical Doctors. Pharmacy, 12(4), 99. https://doi.org/10.3390/pharmacy12040099