
Medication Review: What’s in a Name and What Is It about?

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
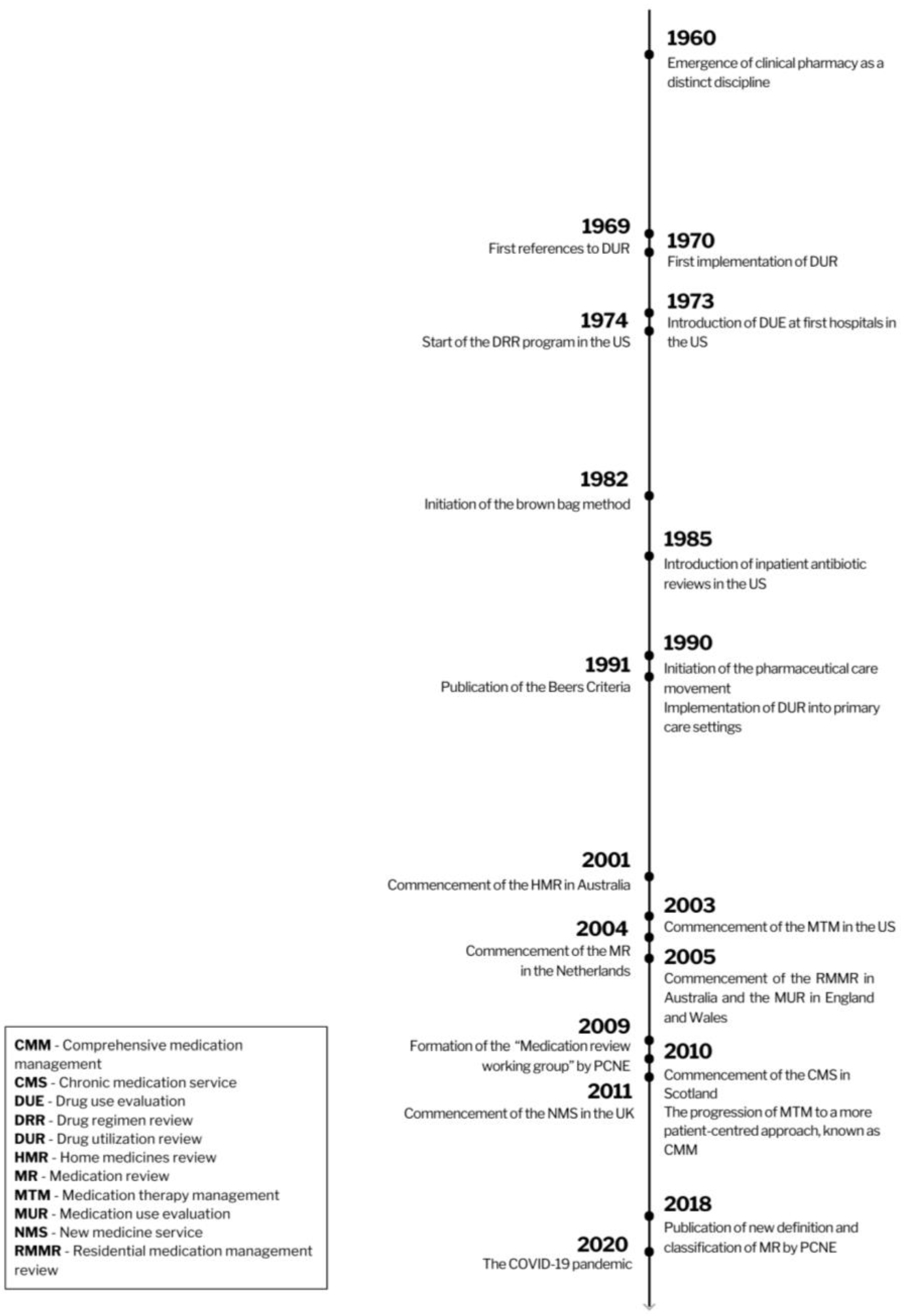
3.1. History of Medication Review

{kind=link}
| Abbreviation | Service | Description |
|---|---|---|
| AUR | Antibiotic Utilization Review | DUR performed among hospitalized patients treated with antibiotics [18]. |
| CMM CMTM | Comprehensive Medication Management Comprehensive Medication Therapy Management | An individualized care plan to achieve the intended goals of therapy with appropriate follow-up to determine actual patients’ outcomes, involving their active participation [19]. A CMM program includes several similar elements to a CMR, yet it extends its scope to address additional facets of the patient’s overall care [20]. CMM not only incorporates the patient’s history into recommendations, similar to CMR, but it also aims to influence elements of that history through measurable clinical outcomes [20]. |
| CMR | Collaborative Medication Review | An internationally accepted term for medication review practices involving pharmacists collaborating closely with other healthcare professionals to review patients’ medicines. Their shared goal is to optimize the use of medications and prevent inappropriate medication use [21]. |
| CMR | Comprehensive Medication Review | A comprehensive, annual, systematic review of all available patient-specific information and medication assessments to identify and resolve potential medication-related problems. CMR involves collaboration between the patient, pharmacist, and prescriber to determine appropriate options for resolving identified problems [22,23]. |
| CMS | Chronic Medication Service | A service established at pharmacies in Scotland dedicated to helping patients with long-term conditions manage their medicines [24]. |
| DRUM | Dispensing Review of Use of Medicines | A review of the use of medicines with the purpose of helping patients understand their medicines and identify medicine-related problems [6]. |
| DUE | Drug Use Evaluation Drug Usage Evaluation | A group of structured reviews of prescribing, dispensing, and use of medication to ensure their appropriate and safe use while also optimizing the economic aspect of drug utilization [15,18]. |
| DRR | Drug Regimen Review | |
| DUR | Drug Utilization Review Drug Use Review | |
| MUE | Medication Use Evaluation | |
| MUM | Medication Use Management | |
| DMMR HMR | Domiciliary Medication Management Review Home Medicines Review | An Australian MR program involving pharmacists conducting a domiciliary visit to review patients medications [25,26]. |
| MAP | Medication-related Action Plan | One of the core elements of an MTM service; it is a patient-centered document equipped with a list of action steps for the patient to use in tracking progress for self-management of medication-related problems [23]. |
| MR | Medication Review | A structured evaluation of a patient’s medicines with the aim of optimizing medicine use and improving health outcomes [27]. |
| MR1 | Medication Review type 1 | |
| MR2 | Medication Review type 2 Intermediate medication review | |
| MR3 | Medication Review type 3 Clinical medication review Advanced medication review | |
| MRF | Medication Review with Follow-up | An ongoing and structured assessment of the patient’s pharmacotherapy performed in Spain that comprises detection of drug-related problems and negative outcomes related to medicines (NOMs), the development of a care plan, and monthly follow-up to provide continuing care [28]. |
| MTA | Medicines Therapy Assessment | A clinical MR program conducted in New Zealand by pharmacists in collaboration with prescribers to review the use and understanding of prescribed therapy, identify medication-related problems, and work with the patient and wider healthcare team to resolve these issues and optimize medication use [29]. |
| MTM MTMS | Medication Therapy Management Medication Therapy Management Services | A distinct service or group of services to optimize therapeutic outcomes for individual patients [30]. The MTM service model can be divided into the five core elements: Medication Therapy Review (MTR), intervention and referral, Personal Medication Record (PMR), Medication-related Action Plan (MAP), and documentation and follow-up [23]. |
| MTR | Medication Therapy Review Medicine Therapy Review | One of the core elements of an MTM service; a systematic process that involves collecting patient-specific information, evaluating medication therapies to identify medication-related problems, creating a prioritized list of these problems, and devising a resolution plan. MTR can be comprehensive (CMR) or targeted (TMR) [23]. |
| MUR | Medicines Use Review | A subtype of MR where pharmacists partner with patients to improve their medicine use and adherence [31]. Referring to the Pharmaceutical Care Network Europe (PCNE) definition, type MR2a includes MUR [32]. |
| NMS | New Medicine Service | A service providing help and advice about medicines to patients who are prescribed a medicine to treat a long-term condition for the first time [33]. |
| PMR | Personal Medication Record | One of the core elements of an MTM service; it contains an up-to-date list of medications, helping patients manage their pharmacotherapy [20]. |
| QUM | Quality Use of Medicines | A package of services performed by Australian pharmacists to support the quality use of medicines, including HMR and RMMR [26]. |
| RMMR | Residential Medication Management Review | An Australian program involving pharmacists conducting MRs of patients residing in aged care facilities [26,34]. |
| SMR | Structured Medicine Review | A review of a patient’s medication, taking into consideration all aspects of the patient’s health in the form of shared decision-making conversations between a clinician and a patient [35]. |
| TMR | Targeted Medication Review | Ongoing medication monitoring to assess medication use and identify and address specific actual or potential medication-related problems [20]. TMR involves follow-up with a healthcare professional or a patient to resolve identified medication-related problems. TMR must be performed quarterly, which enables identifying issues on a more regular basis than through yearly CMR [20]. |
3.2. Definitions and Various Types of Medication Review
| Definition | Source | Year |
|---|---|---|
| A structured, critical examination of a patient’s medicines with the objective of reaching an agreement with the patient about treatment, optimizing the impact of medicines, minimizing the number of medication-related problems, and reducing waste [60]. | Medicines Partnership | 2002 |
| A structured, critical examination of a patient’s medicines by a healthcare professional: reaching an agreement with the patient about treatment, optimizing the use of medicines, minimizing the number of medication-related problems, avoiding wastage. Regular medication review maximizes the therapeutic benefit and minimizes the potential harm of drugs. It ensures the safe and effective use of medicines by patients. A medication review provides an opportunity for patients to discuss their medicines with a healthcare professional. Medication review is the cornerstone of medicine management [59]. | Oxford Handbook of Clinical Pharmacy, 1st edition | 2007 |
| A structured, critical examination of a person’s medicines with the objective of reaching an agreement with the person about treatment, optimizing the impact of medicines, minimizing the number of medication-related problems, and reducing waste [31]. | National Prescribing Centre (NPC) | 2008 |
| A structured evaluation of a patient’s medicines with the aim of optimizing medicine use and improving health outcomes. This entails detecting drug-related problems and recommending interventions [27]. | Pharmaceutical Care Network Europe (PCNE) | 2018 |
- Level 0—Ad hoc—unstructured, opportunistic review.
- Level 1—Prescription review—a technical review of the list of a patient’s medicine;
- Level 2—Treatment review—a review of medicines with the patient’s full notes;
- Level 3—Clinical medication review—a face-to-face review of medicines and conditions.
- Type I—Prescription review—addresses technical issues relating to the prescription; the patient is usually not involved; it is a review of medicines.
- Type II—Compliance and concordance review—addresses issues relating to the patient’s medicine-taking behaviors; the patient is usually involved; it focuses on medicine use. This type includes MURs.
- Type III—Clinical medication review—addresses issues relating to the patient’s use of medicines in the context of their clinical conditions; the patient is always involved, and there is also always access to patient information (e.g., clinical conditions and laboratory test results). It reviews medicines and conditions.
- Type 1—Simple MR (MR1)—is based solely on the patient’s medication history available in the pharmacy; it enables the detection of drug interactions, some side effects, unusual dosages, and some adherence issues. This type of MR is part of routine dispensing.
- Type 2—Intermediate MR—classified into two subtypes:
- -
- Type 2A (MR2A)—based on the medication history and patient information; thus, it is useful when the patient can be interviewed; it detects drug interactions, drug–food interactions, side effects, unusual dosages, effectiveness, and adherence issues, but also issues with OTC medications.
- -
- Type 2B (MR2B)—based on the medication history and clinical information obtained from the general practitioner (GP) or physician; detects drug interactions, drug–food interactions, side effects, unusual dosages, adherence issues, effectiveness issues, indication without a drug, and drugs without indication.
- Type 3—Advanced or Clinical MR (MR3)—based on a complete medication history, an extensive patient interview, and clinical data obtained from the GP or the physician; detects drug–drug interactions, drug-food interactions, issues with OTC drugs, side effects, unusual dosages, adherence issues, effectiveness issues, indication without a drug, and drugs without indication.
3.3. The Principal Criteria Delineating Key Features of Medication Review
3.3.1. Participating Healthcare Providers
3.3.2. Target Group of Patients
3.3.3. The Most Crucial Outcome Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pearson, G.J. Evolution in the practice of pharmacy—Not a revolution! Can. Med. Assoc. J. 2007, 176, 1295–1296. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.R. History of clinical pharmacy and clinical pharmacology. J. Clin. Pharmacol. 1981, 21, 195–197. [Google Scholar] [CrossRef]
- Hopkins, J.; Siu, S.; Cawley, M.; Rudd, P. Drug therapy: The impact of managed care. Adv. Pharmacol. 1998, 44, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Hosp. Pharm. 1990, 47, 533–543. [Google Scholar] [CrossRef] [PubMed]
- NICE Medicines and Prescribing Centre (UK). Medicines Optimisation: The Safe and Effective Use of Medicines to Enable the Best Possible Outcomes. 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK355921/ (accessed on 2 November 2023).
- Blenkinsopp, A.; Bond, C.; Raynor, D.K. Medication reviews. Br. J. Clin. Pharmacol. 2012, 74, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Geurts, M.M.; Talsma, J.; Brouwers, J.R.; de Gier, J.J. Medication review and reconciliation with cooperation between pharmacist and general practitioner and the benefit for the patient: A systematic review. Br. J. Clin. Pharmacol. 2012, 74, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Kiles, T.M.; Peroulas, D.; Borja-Hart, N. Defining the role of pharmacists in addressing the social determinants of health. Res. Soc. Adm. Pharm. 2022, 18, 3699–3703. [Google Scholar] [CrossRef] [PubMed]
- Robberechts, A.; Michielsen, M.; Steurbaut, S.; De Meyer, G.R.Y.; De Loof, H. Key elements in the quality assessment of a type 3 medication review. Front. Pharmacol. 2023, 14, 1258364. [Google Scholar] [CrossRef]
- Alharthi, M.; Wright, D.; Scott, S.; Blacklock, J. Terms used to describe and define activities undertaken as a result of the medication review process: Do they require standardisation? A systematic review. Int. J. Clin. Pharm. 2022, 45, 304–319. [Google Scholar] [CrossRef]
- Nesbit, S.A.; Haas, C.E.; Carter, B.L.; Kehoe, W.A.; Jacobi, J.; D’Amico, H.R.; Peace, J.T. Development of clinical pharmacy quality measures: A call to action. J. Am. Coll. Clin. Pharm. 2022, 5, 366–369. [Google Scholar] [CrossRef]
- Hirt, J.; Nordhausen, T.; Appenzeller-Herzog, C.; Ewald, H. Citation tracking for systematic literature searching: A scoping review. Res. Synth. Methods 2023, 14, 563–579. [Google Scholar] [CrossRef] [PubMed]
- Christen, C. Clinical pharmacy and medication safety. Ann. Pharmacother. 2006, 40, 2020–2021. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, S.; Soumerai, S.B.; Lipton, H.L.; Strom, B.L. Drug Utilization Review. In Pharmacoepidemiology, 4th ed.; Strom, B.L., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2005; pp. 439–453. [Google Scholar]
- Kubacka, R.T. A primer on drug utilization review. J. Am. Pharm. Assoc. 1996, 36, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Lee, P. Task Force on Prescription Drugs, Final Report; US Government Print: Washington, DC, USA, 1969.
- Academy of Managed Care Pharmacy. Drug Utilization Review. AMCP. 2019. Available online: https://www.amcp.org/about/managed-care-pharmacy-101/concepts-managed-care-pharmacy/drug-utilization-review (accessed on 24 November 2023).
- Peterson, A.M. Drug use evaluation. In Managing Pharmacy Practice. Principles, Strategies, and Systems; Peterson, A.M., Ed.; CRC Press LLC: Boca Raton, FL, USA, 2005. [Google Scholar]
- Patient-Centered Primary Care Collaborative. The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes Resource Guide. 2012. Available online: https://thepcc.org/sites/default/files/media/medmanagement.pdf (accessed on 3 December 2023).
- National Board of Medication Therapy Management; Thomas, D.; Tran, J. Medication Therapy Management. National Board of Medication Therapy Management. 2020. Available online: https://nbmtm.org/mtm-reference/medication-therapy-management/ (accessed on 10 November 2023).
- Kiiski, A.; Airaksinen, M.; Mantyla, A.; Desselle, S.; Kumpusalo-Vauhkonen, A.; Jarvensivu, T.; Pohjanoksa-Mantyla, M. An inventory of collaborative medication reviews for older adults—Evolution of practices. BMC Geriatr. 2019, 19, 321. [Google Scholar] [CrossRef] [PubMed]
- Ferries, E.; Dye, J.T.; Hall, B.; Ndehi, L.; Schwab, P.; Vaccaro, J. Comparison of Medication Therapy Management Services and Their Effects on Health Care Utilization and Medication Adherence. J. Manag. Care Spec. Pharm. 2019, 25, 688–695. [Google Scholar] [CrossRef] [PubMed]
- American Pharmacists Association; National Association of Chain Drug Stores Foundation. Medication therapy management in pharmacy practice: Core elements of an MTM service model (version 2.0). J. Am. Pharm. Assoc. 2008, 48, 341–353. [Google Scholar] [CrossRef] [PubMed]
- The NHS Chronic Medication Service at Your Local Pharmacy. NHS Scotland. 2010. Available online: https://www.communitypharmacy.scot.nhs.uk/documents/epharmacy/cms/cms_patient_information_leaflet.pdf (accessed on 19 December 2023).
- Pharmacy Programs Administrator (PPA) Australia. Home Medicines Review. PPA Australia. Available online: https://www.ppaonline.com.au/programs/medication-management-programs/home-medicines-review (accessed on 30 October 2023).
- Chen, T.F. Pharmacist-Led Home Medicines Review and Residential Medication Management Review: The Australian Model. Drugs Aging 2016, 33, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Griese-Mammen, N.; Hersberger, K.E.; Messerli, M.; Leikola, S.; Horvat, N.; van Mil, J.W.F.; Kos, M. PCNE definition of medication review: Reaching agreement. Int. J. Clin. Pharm. 2018, 40, 1199–1208. [Google Scholar] [CrossRef]
- Ocampo, C.C.; Garcia-Cardenas, V.; Martinez-Martinez, F.; Benrimoj, S.I.; Amariles, P.; Gastelurrutia, M.A. Implementation of medication review with follow-up in a Spanish community pharmacy and its achieved outcomes. Int. J. Clin. Pharm. 2015, 37, 931–940. [Google Scholar] [CrossRef]
- Pharmaceutical Society of New Zealand (PSNZ). Introduction to MTA. PSNZ. 2011. Available online: https://www.psnz.org.nz/Folder?Action=View%20File&Folder_id=96&File=IntroductionToMTA.pdf (accessed on 22 November 2023).
- Bluml, B.M. Definition of medication therapy management: Development of professionwide consensus. J. Am. Pharm. Assoc. 2005, 45, 566–572. [Google Scholar] [CrossRef]
- Clyne, W.; Blenkinsopp, A.; Seal, R. A Guide to Medication Review; Keele University: Newcastle, UK, 2008. [Google Scholar]
- The Pharmaceutical Care Network Europe (PCNE). Statement Medication Review Types According to PCNE; Pharmaceutical Care Network Europe: Basel, Switzerland, 2013. [Google Scholar]
- National Health Service (NHS), UK. New Medicine Service (NMS). NHS UK. Available online: https://www.nhs.uk/nhs-services/prescriptions-and-pharmacies/pharmacies/new-medicine-service-nms/ (accessed on 30 November 2023).
- Pharmacy Programs Administrator (PPA) Australia. Residential Medication Management Review and Quality Use of Medicines. PPA Australia. Available online: https://www.ppaonline.com.au/programs/medication-management-programs/residential-medication-management-review-and-quality-use-of-medicines (accessed on 30 October 2023).
- National Health Service England. Structured Medication Reviews and Medicines Optimisation: Guidance. NHS England. Available online: https://www.england.nhs.uk/primary-care/pharmacy/smr/ (accessed on 30 October 2023).
- Larrat, E.P.; Taubman, A.H.; Willey, C. Compliance-related problems in the ambulatory population. Am. Pharm. 1990, 30, 18–23. [Google Scholar] [CrossRef]
- Nathan, A.; Goodyer, L.; Lovejoy, A.; Rashid, A. ‘Brown bag’ medication reviews as a means of optimizing patients’ use of medication and of identifying potential clinical problems. Fam. Pr. 1999, 16, 278–282. [Google Scholar] [CrossRef]
- Carver, N.; Jamal, Z.; Dering Anderson, A.M. Drug Utilization Review. In StatPearls; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Beers, M.H.; Ouslander, J.G.; Rollingher, I.; Reuben, D.B.; Brooks, J.; Beck, J.C. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch. Intern. Med. 1991, 151, 1825–1832. [Google Scholar] [CrossRef]
- Pazan, F.; Kather, J.; Wehling, M. A systematic review and novel classification of listing tools to improve medication in older people. Eur. J. Clin. Pharmacol. 2019, 75, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.; Ryan, C.; Byrne, S.; Kennedy, J.; O’Mahony, D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int. J. Clin. Pharmacol. Ther. 2008, 46, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Samsa, G.P.; Hanlon, J.T.; Schmader, K.E.; Weinberger, M.; Clipp, E.C.; Uttech, K.M.; Lewis, I.K.; Landsman, P.B.; Cohen, H.J. A summated score for the medication appropriateness index: Development and assessment of clinimetric properties including content validity. J. Clin. Epidemiol. 1994, 47, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, J.T.; Schmader, K.E. The Medication Appropriateness Index: A Clinimetric Measure. Psychother. Psychosom. 2022, 91, 78–83. [Google Scholar] [CrossRef] [PubMed]
- International Pharmaceutical Federation (FIP); World Health Organization (WHO). Joint FIP/WHO Guidelines on Good Pharmacy Practice: Standards for Quality of Pharmacy Services; World Health Organization: Geneva, Switzerland, 2011.
- Bulajeva, A.; Labberton, L.; Leikola, S.; Pohjanoksa-Mantyla, M.; Geurts, M.M.; de Gier, J.J.; Airaksinen, M. Medication review practices in European countries. Res. Soc. Adm. Pharm. 2014, 10, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Gudi, S.K.; Kashyap, A.; Chhabra, M.; Rashid, M.; Tiwari, K.K. Impact of pharmacist-led home medicines review services on drug-related problems among the elderly population: A systematic review. Epidemiol. Health 2019, 41, e2019020. [Google Scholar] [CrossRef] [PubMed]
- Lewin, G. Medication therapy management services: A critical review. J. Am. Pharm. Assoc. 2005, 45, 580–587. [Google Scholar] [CrossRef]
- Barnett, M.J.; Frank, J.; Wehring, H.; Newland, B.; VonMuenster, S.; Kumbera, P.; Halterman, T.; Perry, P.J. Analysis of pharmacist-provided medication therapy management (MTM) services in community pharmacies over 7 years. J. Manag. Care Pharm. 2009, 15, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. National Service Framework for Older People. 2001. Available online: https://assets.publishing.service.gov.uk/media/5a7b4f16e5274a34770ead1c/National_Service_Framework_for_Older_People.pdf (accessed on 11 November 2023).
- Royal Pharmaceutical Society. Medicines Optimisation: Helping Patients to Make the Most of Medicines; Royal Pharmaceutical Society: London, UK, 2013. [Google Scholar]
- Imfeld-Isenegger, T.L.; Soares, I.B.; Makovec, U.N.; Horvat, N.; Kos, M.; van Mil, F.; Costa, F.A.; Hersberger, K.E. Community pharmacist-led medication review procedures across Europe: Characterization, implementation and remuneration. Res. Soc. Adm. Pharm. 2020, 16, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Jokanovic, N.; Tan, E.C.; Sudhakaran, S.; Kirkpatrick, C.M.; Dooley, M.J.; Ryan-Atwood, T.E.; Bell, J.S. Pharmacist-led medication review in community settings: An overview of systematic reviews. Res. Soc. Adm. Pharm. 2017, 13, 661–685. [Google Scholar] [CrossRef] [PubMed]
- Hatah, E.; Braund, R.; Tordoff, J.; Duffull, S.B. A systematic review and meta-analysis of pharmacist-led fee-for-services medication review. Br. J. Clin. Pharmacol. 2014, 77, 102–115. [Google Scholar] [CrossRef] [PubMed]
- National Health Service England. Summary Care Records (SCR). NHS England. Available online: https://www.england.nhs.uk/long-read/summary-care-records-scr/#:~:text=The%20NHS%20summary%20care%20record,as%20the%20’source%20record’ (accessed on 9 February 2024).
- Madden, M.; Mills, T.; Atkin, K.; Stewart, D.; McCambridge, J. Early implementation of the structured medication review in England: A qualitative study. Br. J. Gen. Pract. 2022, 72, e641–e648. [Google Scholar] [CrossRef] [PubMed]
- Kieck, D.; Mahalick, L.; Vo, T.T. Medication-Related Problems Identified and Addressed by Pharmacists Dispensing COVID-19 Antivirals at a Community Pharmacy. Pharmacy 2023, 11, 87. [Google Scholar] [CrossRef]
- Hess, K.; Bach, A.; Won, K.; Seed, S.M. Community Pharmacists Roles During the COVID-19 Pandemic. J. Pharm. Pract. 2022, 35, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Zermansky, A.G.; Petty, D.R.; Raynor, D.K.; Lowe, C.J.; Freemantle, N.; Vail, A. Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: A randomised controlled trial. Health Technol. Assess. 2002, 6, 1–86. [Google Scholar] [CrossRef]
- Wiffen, P.; Mitchell, M.; Snelling, M.; Stoner, N. Oxford Handbook of Clinical Pharmacy, 1st ed.; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Medicines Partnership. What is MR/Models of MR. Medicines Partnership. 2002. Available online: https://medicines-partnership.org/medication-review/welcome/room-for-review/what-is-mr (accessed on 30 October 2023).
- Saskatchewan Ministry of Health. Saskatchewan Medication Assessment Program (SMAP). Procedures and Guidelines for Saskatchewan Pharmacists. Available online: https://members.skpharmacists.ca/wp-content/uploads/2023/04/SMAP-Procedures-and-Guidelines.pdf (accessed on 3 December 2023).
- Ontario Ministry of Health and Long-Term Care. Professional Pharmacy Services Guidebook 3.0. MedsCheck, Pharmaceutical Opinion and Pharmacy Smoking Cessation Program. 2016. Available online: https://files.ontario.ca/moh-medscheck-professional-pharmacy-services-guidebook-2016-07-01.pdf (accessed on 3 December 2023).
- The Patient Care Process for Delivering Comprehensive Medication Management (CMM): Optimizing Medication Use in Patient-Centered, Team-Based Care Settings. CMM in Primary Care Research Team. 2018. Available online: https://www.accp.com/docs/positions/misc/CMM_Care_Process.pdf. (accessed on 3 December 2023).
- Pharmaceutical Society of Ireland (PSI). Guidelines on Counselling and Medicine Therapy Review in the Supply of Prescribed Medicinal Products. 2019. Available online: https://www.thepsi.ie/Libraries/Folder_Pharmacy_Practice_Guidance/01_11_Guidelines_on_Counselling_and_Medicine_Therapy_Review_in_the_Supply_of_Prescribed_Medicinal_Products.sflb.ashx (accessed on 14 January 2024).
- Pharmaceutical Society of Australia (PSA). Guidelines for Pharmacists Providing Residential Medication Management Review (RMMR) and Quality Use of Medicines (QUM) services. 2011. Available online: https://www.ppaonline.com.au/wp-content/uploads/2019/01/PSA-RMMR-and-QUM-Guidelines.pdf (accessed on 3 December 2023).
- Pharmaceutical Society of Australia (PSA). Guidelines for Quality Use of Medicines (QUM) Services. 2020. Available online: https://www.ppaonline.com.au/wp-content/uploads/2020/04/PSA-Guidelines-for-Quality-Use-of-Medicines-QUM-services.pdf (accessed on 3 December 2023).
- Pharmaceutical Society of Australia (PSA). Guidelines for Comprehensive Medication Management Review. 2020. Available online: https://www.ppaonline.com.au/wp-content/uploads/2020/04/PSA-Guidelines-for-Comprehensive-Medication-Management-Reviews.pdf (accessed on 3 December 2023).
- The Royal Dutch Pharmacists Association (KNMP). Clinical Medication Review. 2013–2020. Available online: https://www.knmp.nl/richtlijnen/medicatiebeoordeling (accessed on 3 December 2023).
- National Health Service (NHS). Network Contract Directed Enhanced Service. Structured Medication Reviews and Medicines Optimisation: Guidance. 2020. Available online: https://www.england.nhs.uk/wp-content/uploads/2020/09/SMR-Spec-Guidance-2020-21-FINAL-.pdf (accessed on 9 February 2024).
- Department of Health and Aged Care; Australian Government. Guiding Principles for Medication Management in the Community. 2022. Available online: https://www.health.gov.au/sites/default/files/2022-11/guiding-principles-for-medication-management-in-the-community.pdf (accessed on 3 December 2023).
- Foro de Atención Farmacéutica en Farmacia Comunitaria (Foro AF-FC). Practical Guide to Clinical Professional Pharmacy Services in Community Pharmacy. Madrid. General Pharmaceutical Council of Spain. 2022. Available online: https://www.farmaceuticos.com/wp-content/uploads/2021/02/ON_GUIA_SPFA_FORO_2022_ING_PGs.pdf (accessed on 14 January 2024).
- Huckerby, C.; Jaspal, J. Medication Review—Best Practice Guidelines. 2018. Available online: https://www.dudleyformulary.nhs.uk/download/286/medication-review-best-practice-guidelines (accessed on 10 October 2023).
- Frandsen, S.; Drastrup, A.M.; Dalin, D.A.; Vermehren, C. Exploring the value of a multidisciplinary-led medication review for elderly individuals at a long-term care facility performed by four different health-care professions in an equal and closely integrated collaboration. J. Fam. Med. Prim. Care 2022, 11, 4519–4527. [Google Scholar] [CrossRef]
- Robberechts, A.; Van Loon, L.; Steurbaut, S.; De Meyer, G.R.Y.; De Loof, H. Patient experiences and opinions on medication review: A qualitative study. Int. J. Clin. Pharm. 2023, 45, 650–658. [Google Scholar] [CrossRef]
- Robberechts, A.; De Petter, C.; Van Loon, L.; Rydant, S.; Steurbaut, S.; De Meyer, G.; De Loof, H. Qualitative study of medication review in Flanders, Belgium among community pharmacists and general practitioners. Int. J. Clin. Pharm. 2021, 43, 1173–1182. [Google Scholar] [CrossRef]
- Mossialos, E.; Courtin, E.; Naci, H.; Benrimoj, S.; Bouvy, M.; Farris, K.; Noyce, P.; Sketris, I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy 2015, 119, 628–639. [Google Scholar] [CrossRef] [PubMed]
- Milosavljevic, A.; Aspden, T.; Harrison, J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: A systematic review. Int. J. Pharm. Pract. 2018, 26, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Radcliffe, E.; Servin, R.; Cox, N.; Lim, S.; Tan, Q.Y.; Howard, C.; Sheikh, C.; Rutter, P.; Latter, S.; Lown, M.; et al. What makes a multidisciplinary medication review and deprescribing intervention for older people work well in primary care? A realist review and synthesis. BMC Geriatr. 2023, 23, 591. [Google Scholar] [CrossRef] [PubMed]
- van Nuland, M.; Butterhoff, M.; Verwijmeren, K.; Berger, F.; Hogervorst, V.M.; de Jonghe, A.; van der Linden, P.D. Assessment of drug-related problems at the emergency department in older patients living with frailty: Pharmacist-led medication reviews within a geriatric care team. BMC Geriatr. 2023, 23, 215. [Google Scholar] [CrossRef] [PubMed]
- Rojas, E.I.; Dupotey, N.M.; De Loof, H. Comprehensive Medication Management Services with a Holistic Point of View, a Scoping Review. Pharmacy 2023, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Saha, S.; Jarl, J.; Conlon, E.; McGuinness, B.; Trepel, D. An Overview of Systematic Reviews and Meta-Analyses on the Effect of Medication Interventions Targeting Polypharmacy for Frail Older Adults. J. Clin. Med. 2023, 12, 1379. [Google Scholar] [CrossRef] [PubMed]
- Huiskes, V.J.; Burger, D.M.; van den Ende, C.H.; van den Bemt, B.J. Effectiveness of medication review: A systematic review and meta-analysis of randomized controlled trials. BMC Fam. Pract. 2017, 18, 5. [Google Scholar] [CrossRef]
- Deng, Z.J.; Gui, L.; Chen, J.; Peng, S.S.; Ding, Y.F.; Wei, A.H. Clinical, economic and humanistic outcomes of medication therapy management services: A systematic review and meta-analysis. Front. Pharmacol. 2023, 14, 1143444. [Google Scholar] [CrossRef]
- Mizokami, F.; Mizuno, T.; Kanamori, K.; Oyama, S.; Nagamatsu, T.; Lee, J.K.; Kobayashi, T. Clinical medication review type III of polypharmacy reduced unplanned hospitalizations in older adults: A meta-analysis of randomized clinical trials. Geriatr. Gerontol. Int. 2019, 19, 1275–1281. [Google Scholar] [CrossRef]
- Tan, E.C.; Stewart, K.; Elliott, R.A.; George, J. Pharmacist services provided in general practice clinics: A systematic review and meta-analysis. Res. Soc. Adm. Pharm. 2014, 10, 608–622. [Google Scholar] [CrossRef]
- Pazan, F.; Petrovic, M.; Cherubini, A.; Onder, G.; Cruz-Jentoft, A.J.; Denkinger, M.; van der Cammen, T.J.M.; Stevenson, J.M.; Ibrahim, K.; Rajkumar, C.; et al. Current evidence on the impact of medication optimization or pharmacological interventions on frailty or aspects of frailty: A systematic review of randomized controlled trials. Eur. J. Clin. Pharmacol. 2021, 77, 1–12. [Google Scholar] [CrossRef]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur. J. Intern. Med. 2016, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Baxter, S.; Killoran, A.; Kelly, M.P.; Goyder, E. Synthesizing diverse evidence: The use of primary qualitative data analysis methods and logic models in public health reviews. Public Health 2010, 124, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Threlfall, A.G.; Meah, S.; Fischer, A.J.; Cookson, R.; Rutter, H.; Kelly, M.P. The appraisal of public health interventions: The use of theory. J. Public Health 2015, 37, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Reeve, E.; Gnjidic, D.; Long, J.; Hilmer, S. A systematic review of the emerging de fi nition of ‘deprescribing’ with network analysis: Implications for future research and clinical practice. Br. J. Clin. Pharmacol. 2015, 80, 1254–1268. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, E.A.; Albers, K.; Gleason, K.; Pieper, L.E.; Boyd, C.M.; Campbell, N.L.; Ensrud, K.E.; Gray, S.L.; Linsky, A.M.; Mangin, D.; et al. Recommendations for outcome measurement for deprescribing intervention studies. J. Am. Geriatr. Soc. 2022, 70, 2487–2497. [Google Scholar] [CrossRef] [PubMed]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef] [PubMed]

| Organization and Country | Guideline | MR Type by PCNE | Year |
|---|---|---|---|
| American Pharmacists Association; National Association of Chain Drug Stores Foundation, USA | Medication therapy management in pharmacy practice: core elements of an MTM service model (version 2.0) [23] | 3 | 2008 |
| Patient-Centered Primary Care Collaborative, USA | The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes Resource Guide [19] | 3 | 2012 |
| Saskatchewan Ministry of Health, Canada | Saskatchewan Medication Assessment Program (SMAP). Procedures and guidelines for Saskatchewan pharmacists [61] | 3 | 2013 |
| Royal Pharmaceutical Society, UK | Medicines Optimization: Helping patients to make the most of medicines [50] | 2a | 2013 |
| National Institute for Health and Care Excellence (NICE), UK | Medicines Optimization: The Safe and Effective Use of Medicines to Enable the Best Possible Outcomes [5] | 2a | 2015 |
| Ontario Ministry of Health and Long-Term Care, Canada | Professional Pharmacy Services Guidebook 3.0. MedsCheck, Pharmaceutical Opinion and Pharmacy Smoking Cessation Program [62] | 2a | 2016 |
| Comprehensive Medication Management in Primary Care Research Team, USA | The Patient Care Process for Delivering Comprehensive Medication Management (CMM): Optimizing Medication Use in Patient-Centered, Team-Based Care Settings [63] | 3 | 2018 |
| Pharmaceutical Society of Ireland (PSI), Ireland | Guidelines on the Counselling and Medicine Therapy Review in the Supply of Prescribed Medicinal Products from a Retail Pharmacy Business [64] | 2a | 2019 |
| Pharmaceutical Society of Australia (PSA), Australia | Guidelines for pharmacists providing Residential Medication Management Review (RMMR) and Quality Use of Medicines (QUM) services [65] | 3 | 2019 |
| Pharmaceutical Society of Australia (PSA), Australia | Guidelines for Quality Use of Medicines (QUM) services [66] | 3 | 2020 |
| Pharmaceutical Society of Australia (PSA), Australia | Guidelines for comprehensive medication management review [67] | 3 | 2020 |
| The Royal Dutch Pharmacists Association (KNMP), The Netherlands | Guideline for conducting clinical medication review in community pharmacy [68] | 3 | 2020 |
| National Health Service (NHS), UK | Structured medication reviews and medicine optimization: guidance [69] | 3 | 2020 |
| Department of Health and Aged Care, Australia | Guiding Principles for Medication Management in the Community [70] | 3 | 2022 |
| General Pharmaceutical Council of Spain, Spain | Practical guide to Clinical Professional Pharmacy Services (CPPS) in Community Pharmacy [71] | 3 | 2022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robberechts, A.; Brumer, M.; Garcia-Cardenas, V.; Dupotey, N.M.; Steurbaut, S.; De Meyer, G.R.Y.; De Loof, H. Medication Review: What’s in a Name and What Is It about? Pharmacy 2024, 12, 39. https://doi.org/10.3390/pharmacy12010039
Robberechts A, Brumer M, Garcia-Cardenas V, Dupotey NM, Steurbaut S, De Meyer GRY, De Loof H. Medication Review: What’s in a Name and What Is It about? Pharmacy. 2024; 12(1):39. https://doi.org/10.3390/pharmacy12010039
Chicago/Turabian StyleRobberechts, Anneleen, Maja Brumer, Victoria Garcia-Cardenas, Niurka M. Dupotey, Stephane Steurbaut, Guido R. Y. De Meyer, and Hans De Loof. 2024. "Medication Review: What’s in a Name and What Is It about?" Pharmacy 12, no. 1: 39. https://doi.org/10.3390/pharmacy12010039
APA StyleRobberechts, A., Brumer, M., Garcia-Cardenas, V., Dupotey, N. M., Steurbaut, S., De Meyer, G. R. Y., & De Loof, H. (2024). Medication Review: What’s in a Name and What Is It about? Pharmacy, 12(1), 39. https://doi.org/10.3390/pharmacy12010039