
Exploring the Value of Real-Time Medication Adherence Monitoring: A Qualitative Study


Abstract
1. Background
2. Objectives
3. Methods
3.1. Study Design
3.2. Ethics Approval
3.3. Theoretical Framework
3.4. Recruitment and Sampling
3.5. Data Collection
3.6. Data Analysis
4. Results
4.1. Participants
4.2. Themes and Sub-Themes
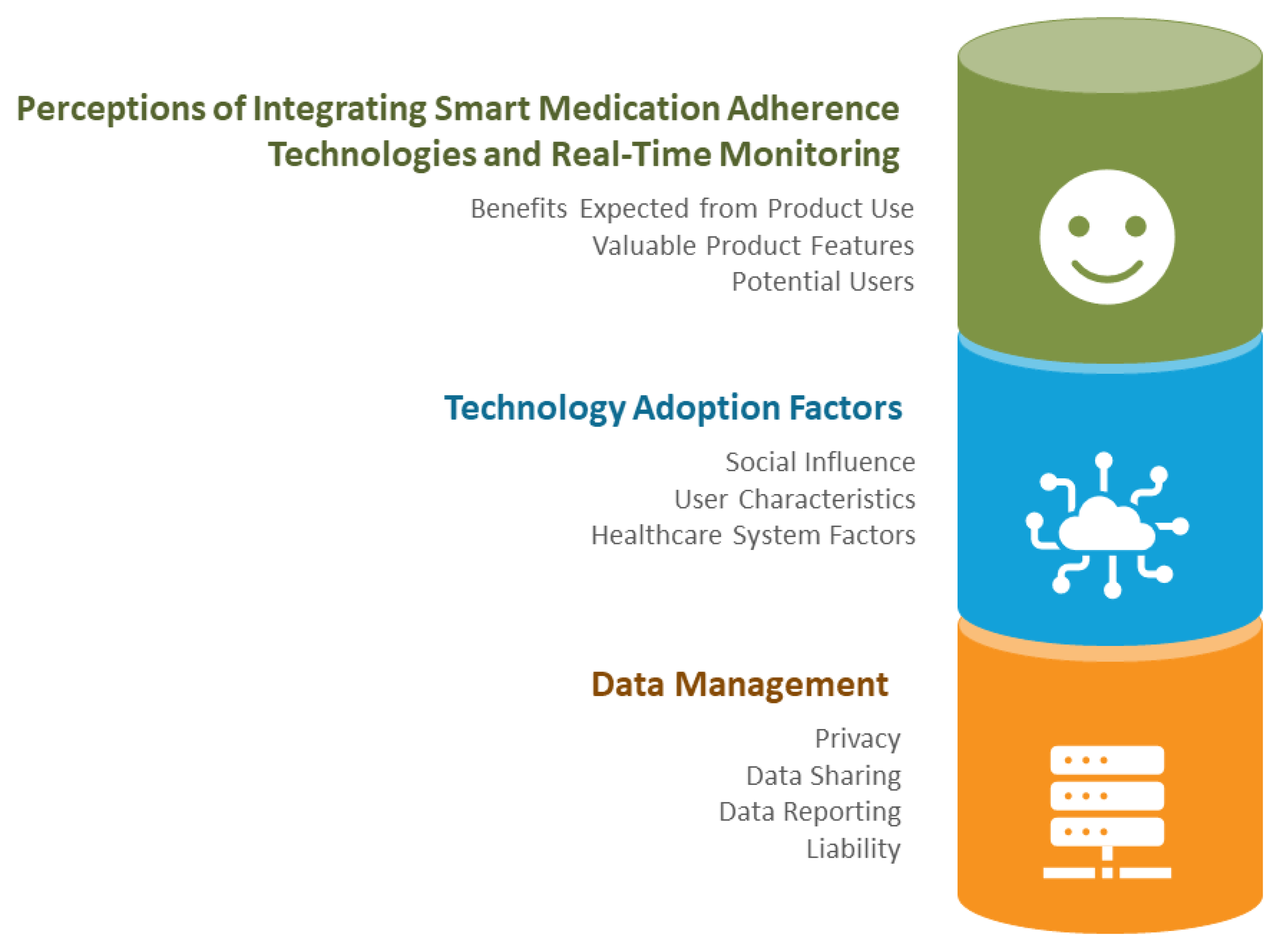
4.2.1. Theme 1: Stakeholder Perceptions of Integrating Smart Medication Adherence Technologies and Real-Time Monitoring of Medication Dispensing
Sub-Theme 1: Benefits Expected from Product Use
“I’d say they would have less hospital visits because… they’d be taking their medication, so they’d have their chronic condition managed.”—015 Pharmacist
“… improved like [my] relationship with my primary care provider, probably, like I feel like we would be more on the same page, I wouldn’t feel like they think that I’m this non-adherent patient who doesn’t care about my health type of thing.”—005 Patient
“I think it would reduce the stress of the caregiver in addition to building some independence for the individual patient. I think it would be a win for all the stakeholders.”—021 Caregiver
“If the family is involved, it gives the family some sort of a comfort knowing that they will get a message if someone in the family is not taking their medications on time so they can call them and find out what’s going on.”—001 Pharmacy Owner
“I think this [real-time medication intake data] would be a good thing, it’d be much easier to know whether a person is taking [medications] versus not.”—010 Physician
“If you’re on a high-cost biologic drug that costs $50,000 a year, or hundreds of thousands of dollars a year. [There are only] small numbers of patients that we really need to monitor and make sure that the dollars we’re spending, like the drug is working for them.”—029 Insurance Provider
“Maybe they see us as really being part of the team… rather than you know, the person that just dispenses something to them in a vial, you know. We play, maybe, a little bit more of an active role in and supporting them with their journey… with their medication.”—006 Pharmacy Owner
Sub-Theme 2: Valuable Product Features
“It has to be really easy to use and it should be simple.”—009 Pharmacist
“I would like something like that… wouldn’t be too heavy to carry around.”—027 Caregiver
“Having an option that was childproofed for those folks that have kids around or some people have grandkids or whatever around too…”—012 Pharmacist
“If you’re running low, they [pharmacy] probably know that and so they [pharmacy] can also give you your medications, right, [so] you don’t have to call them [pharmacy] all the time either.”—004 Patient
“Uh for the pharmacist I think it would be better management for their [pharmacy] inventory and they’re like, you know, if they need to, if they’re running out of something and they have to order um from their distributors they can like, you know, plan ahead a little bit better than they can do right now. Right now, they have to rely on whatever it, of course, it’s not a live record right, like they can only calculate like you know I have dispensed until the next 30 days so if I’m running out I need to order seven days ahead of that right but if it’s live data they can like compile.”—002 Caregiver
“The letters or the writing on it [the product] needs to be big enough so that they [users] can read it.”—009 Pharmacist
“Irrespective of gender, age, you know, religion, you know, understanding of any kind of language.”—023 Insurance Provider
“Read the readouts and all that stuff would certainly, I think, be very important.”—029 Insurance Provider
Sub-Theme 3: Potential Users
“For those who… are in either a more complex medical or medication regime or, uh… have issues where you feel that compliance might be an issue…”—030 Physician
“I think anyone with like mild, even mild MCI would benefit because it eliminates that that question of, you know, ‘have I taken my medication or not?’”—021 Caregiver
“Mental health, as an example, is an area that leads to a lot of disability costs related to mental health and mental health on its own is a rapidly increasing area of concern for employers due to again absentees and disability.”—018 Insurance Provider
4.2.2. Theme 2: Technology Adoption Factors
Subtheme 1: Social Influence
“The current pharmacist that I have, it would be his… pitch that would be most important.”—025 Patient
“I think… the caregivers and the pharmacist and the physicians and all of that, will have to play a bigger role in this, right, as opposed to the people who are actually taking the medication themselves.”—002 Caregiver
“If a physician is recommending it to me, like you know, like you’ve been telling me that your mom has been missing days right, so here’s the solution for you, this is what it can do and like if they can list all the things out right then I’ll be more inclined to trust that um as opposed to me going to pharmacy and then just picking one of these products and be like oh I should try this right?… So I think more influence from the physician and the pharmacist would play a better role in me buying these.”—002 Caregiver
“I think if I pitched it to the caregiver and told them it was in their best interest… I think money may not be an issue if they see the value in it. If I told the patient directly, yes, there may be some resistance.”—013 Pharmacist Owner
“It’s kind of like an interesting loop, because in a situation like mine, you have two people that would have to be brought on board. It would have to be the patient and the physician.”—021 Caregiver
Sub-Theme 2: User Characteristics
“If they have dementia and their progressing potentially, they may not be able to use this technology… and that’s where they might have to be going more into long-term care setting where someone else is administering the medication.”—003 Pharmacist
“I think technology access would definitely be a concern for like especially for members that are older. Um for people my age, I don’t think that would really be much of a concern. I think most people have access to at least the required level of technology in order to be able to use something like this.”—019 Patient
“Sometimes there are younger caregivers, maybe younger kids who like the technology version of many things. And we have a few persons like that. But most older adults, I think… generally stick with basics.”—010 Physician
Sub-Theme 3: Healthcare System Factors
“It depends on the situation. And I mean I have a good feel for my patients. I know…the patients that are willing to pay out of pocket and I know the patients that are not.”—013 Pharmacy Owner
“The machine would be nice if it was covered in some way, especially if it’s for people that meet a certain type of criteria, whether it’s age, whether there’s a lot of medication that’s hard to manage.”—002 Caregiver
“I think moving forward, if there was a way to get some subsidized cost for this, almost like [an] assistive devices kind of program, where someone would have some cognitive concerns that there would be a little bit of something towards this technology, I think would be very useful and helpful.”—003 Pharmacist
“I think there’s opportunity for, you know, pharmacy organizations and the pharmaceutical industry to really find the way to fund the models around adherence.”—018 Insurance Provider
“Workflow and time are basically an issue with everything that’s new that’s implemented in pharmacy.”—015 Pharmacist
“They’d be really worried about the increase[d] work for the amount of value that they would get out of it, just because they’re so stretched.”—030 Physician
“If we were to launch this as any kind of a product that we made available, we’d have to create a product team for that. And there would be usually, there are two or three people that would be responsible for, you know, we usually create communication materials, marketing materials… We have, you know, there’s probably legal stuff that has to be signed off on. There’s compliance and regulation.”—029 Insurance Provider
“It would be great if moving forward there was some integration with EMR platforms. I can see that being a question from my docs and my nurse practitioners… To have something just completely link to the EMR would be fantastic so that you wouldn’t have to log on separately to another portal and that we can just have it integrated within the EMR.”—003 Pharmacist
“If you had more than one of these types of portals, you know, like if there were different companies doing the products, which I think maybe you mentioned here… that just makes it doubly hard, right? Because then all of a sudden, you’ve got one patient with this, another patient with this. And it’s just, you know, for primary care is just so hard.”—030 Physician
“The health outcomes of these products um… and seeing what impact they actually have. To know that it is useful, and it can be useful. There has to be, you know, buy in.”—023 Insurance Provider
“I would package that as a service, because my return on investment would be through the med checks, through the follow up med checks.”—011 Pharmacist
4.2.3. Theme 3: Data Management
Sub-Theme 1: Privacy
“I think that any product should be um secure… if it’s a cloud-based information transmitter or whatever, like the LibreView is… there would be information that we could share to reassure them [the patient] of the [product’s] security.”—012 Pharmacist
“I don’t think there’s any, uh you know, impact on privacy. They already have that information. They already have your medication information, your medical history, all of that right, as long as… the app or the prod—the equipment is not collecting any other data… that it’s not supposed to collect, right, like it’s not connected to your bank.”—002 Caregiver
Sub-Theme 2: Data Sharing
“I think anybody who has the information or has access to the information requires patient permission. They need to get that permission to have it.”—011 Pharmacist
“Insurance companies don’t need to know everything about me, you know? Yes, I have to be truthful if I’m going to an application say for travel insurance industry to make sure I get proper coverage. But I don’t want them to run the risk of denying me coverage because I’m on something that has no bearing on my health or whatever.”—028 Caregiver
Sub-Theme 3: Data Reporting
“I think one would have to be careful not to um unnecessarily burden physicians with information that they can’t really act on, they don’t have the time to act on versus I think this kind of detailed information may be more helpful for a caregiver or somebody who’s actually responsible for administering medicines and monitoring medicines, maybe.”—010 Physician
I’m just looking at this graph and if I’m looking at it and if the caregivers looking at it and they’re starting to freak out about something I can explain because we can both see.”—011 Pharmacist
Sub-Theme 4: Liability
“I think on the surface, it sounds amazing. But I know how busy pharmacists and physicians are. Do they have opportunity to look into patient files and get alerts and do something with it?”—018 Insurance Provider
5. Discussion
5.1. Principal Findings
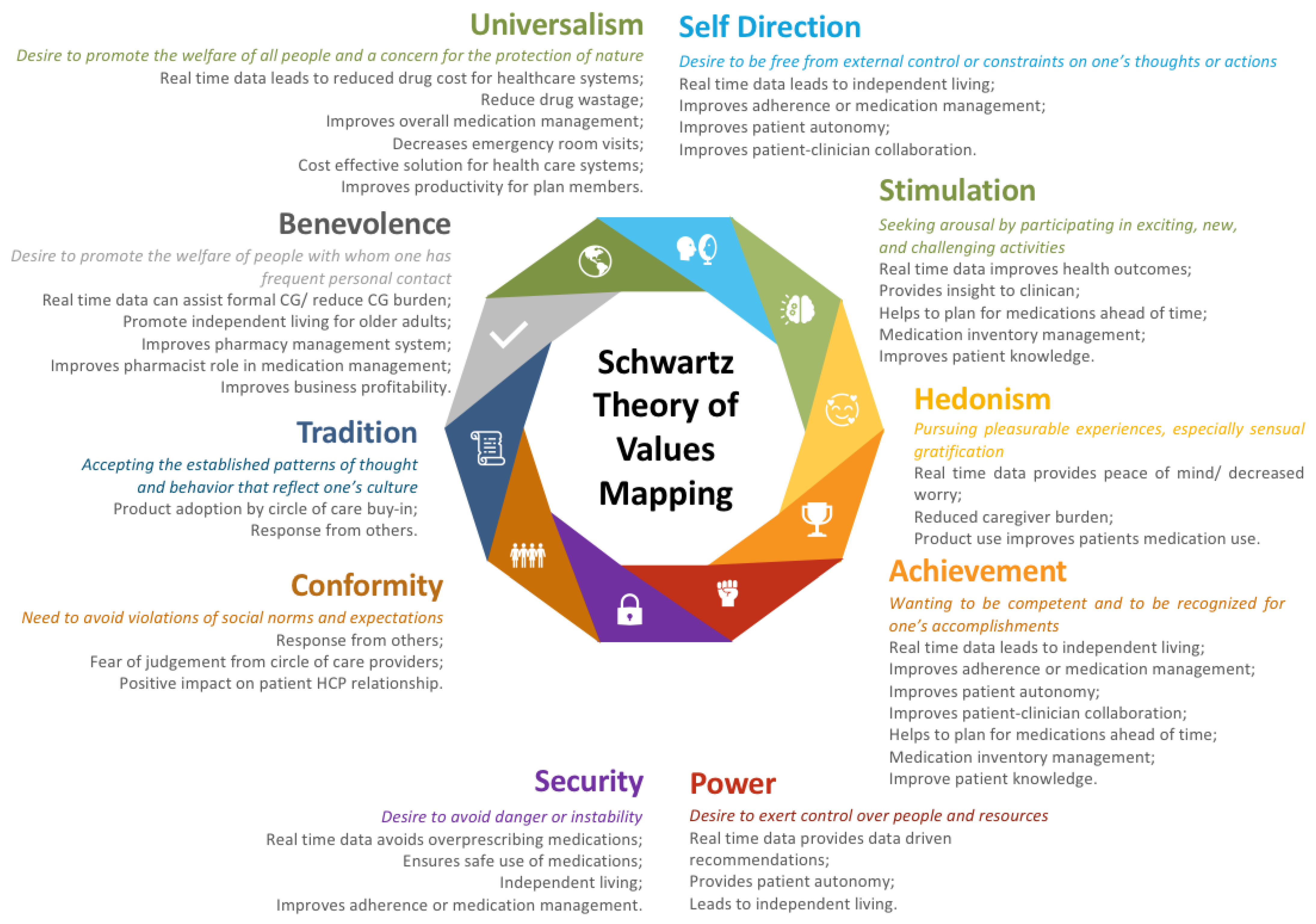
5.2. Mapping Codes to Schwartz’s Value Theory
5.3. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; Sabate, D.G., Ed.; World Health Organization: Geneva, Switzerland, 2003; Available online: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf?sequence=1&isAllowed=y (accessed on 14 August 2022).
- Tsai, K.-T.; Chen, J.-H.; Wen, C.-J.; Kuo, H.-K.; Lu, I.-S.; Chiu, L.-S.; Wu, S.-C.; Chan, D.-C. Medication adherence among geriatric outpatients prescribed multiple medications. Am. J. Geriatr. Pharmacother. 2012, 10, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [PubMed]
- Dunbar-Jacob, J.; Mortimer-Stephens, M. Treatment adherence in chronic disease. J. Clin. Epidemiol. 2001, 54, S57–S60. [Google Scholar] [CrossRef] [PubMed]
- Park, L.G.; Howie-Esquivel, J.; Dracup, K. Electronic measurement of medication adherence. West. J. Nurs. Res. 2014, 37, 28–49. [Google Scholar] [CrossRef]
- Anghel, L.A.; Farcas, A.M.; Oprean, R.N. An overview of the common methods used to measure treatment adherence. Med. Pharm. Rep. 2019, 92, 117–122. [Google Scholar] [CrossRef]
- Lam, W.Y.; Fresco, P. Medication adherence measures: An overview. Biomed. Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Aldeer, M.; Javanmard, M.; Martin, R.P. A Review of Medication Adherence Monitoring Technologies. Appl. Syst. Innov. 2018, 1, 14. [Google Scholar] [CrossRef]
- Mason, M.; Cho, Y.; Rayo, J.; Gong, Y.; Harris, M.; Jiang, Y. Technologies for Medication Adherence Monitoring and Technology Assessment Criteria: Narrative Review. JMIR mHealth uHealth 2022, 10, e35157. [Google Scholar] [CrossRef]
- Checchi, K.D.; Huybrechts, K.F.; Avorn, J.; Kesselheim, A.S. Electronic medication packaging devices and medication adherence. JAMA 2014, 312, 1237–1247. [Google Scholar] [CrossRef]
- Treskes, R.W.; Van der Velde, E.T.; Schoones, J.W.; Schalij, M.J. Implementation of smart technology to improve medication adherence in patients with cardiovascular disease: Is it effective? Expert Rev. Med. Devices 2018, 15, 119–126. [Google Scholar] [CrossRef]
- Van Heuckelum, M.; Ende, C.H.M.V.D.; Houterman, A.E.J.; Heemskerk, C.P.M.; Van Dulmen, S.; Bemt, B.J.F.V.D. The effect of electronic monitoring feedback on medication adherence and clinical outcomes: A systematic review. PLoS ONE 2017, 12, e0185453. [Google Scholar] [CrossRef] [PubMed]
- Faisal, S.; Ivo, J.; Patel, T. Smart electronic medication adherence products: A comparison of features. Can. Pharm. J. 2021, 154, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Faisal, S.; Ivo, J.; Lee, C.; Carter, C.; Patel, T. The usability, acceptability, and functionality of smart oral multidose dispensing systems for medication adherence: A scoping review. J. Pharm. Pr. 2020, 35, 0897190020977756. [Google Scholar] [CrossRef] [PubMed]
- Steinkamp, J.M.; Goldblatt, N.; Borodovsky, J.T.; Lavertu, A.; Kronish, I.M.; Marsch, L.A.; Schuman-Olivier, Z. Technological interventions for medication adherence in adult mental health and substance use disorders: A systematic review. JMIR Ment. Health 2019, 6, e12493. [Google Scholar] [CrossRef]
- Faisal, S.; Ivo, J.; Tennant, R.; Prior, K.-A.; Grindrod, K.; McMillan, C.; Patel, T. Integration of a smart multidose blister package for medication intake: A mixed method ethnographic informed study of older adults with chronic diseases. PLoS ONE 2022, 17, e0262012. [Google Scholar] [CrossRef]
- Patel, T.; Ivo, J.; Faisal, S.; McDougall, A.; Carducci, J.; Pritchard, S.; Chang, F. A prospective study of usability and workload of electronic medication adherence products by older adults, caregivers, and health care providers. J. Med. Internet Res. 2020, 22, e18073. [Google Scholar] [CrossRef]
- Baumgartner, S.L.; Jr, D.E.B.; Rukavina, E.; Jones, J.; Weiler, E.; Carnes, T.C. A novel digital pill system for medication adherence measurement and reporting: Usability validation study. JMIR Hum. Factors 2021, 8, e30786. [Google Scholar] [CrossRef]
- Musiimenta, A.; Tumuhimbise, W.; Mugaba, A.T.; Muzoora, C.; Armstrong-Hough, M.; Bangsberg, D.; Davis, J.L.; Haberer, J.E. Digital monitoring technologies could enhance tuberculosis medication adherence in Uganda: Mixed methods study. J. Clin. Tuberc. Other Mycobact. Dis. 2019, 17, 100119. [Google Scholar] [CrossRef]
- Faisal, S.; Ivo, J.; McDougall, A.; Patel, T. Stakeholder feedback of electronic medication adherence products: Qualitative analysis. J. Med. Internet Res. 2020, 22, e18074. [Google Scholar] [CrossRef]
- Faisal, S.; Ivo, J.; Tennant, R.; Prior, K.-A.; Grindrod, K.; McMillan, C.; Patel, T. Implementation of a real-time medication intake monitoring technology intervention in community pharmacy settings: A mixed-method pilot study. Pharmacy 2021, 9, 105. [Google Scholar] [CrossRef]
- Hill, L.M.; Golin, C.E.; Pack, A.; Carda-Auten, J.; Wallace, D.; Cherkur, S.; Farel, C.; Rosen, E.P.; Gandhi, M.; Prince, H.M.A.; et al. Using Real-Time Adherence Feedback to Enhance Communication About Adherence to Antiretroviral Therapy: Patient and Clinician Perspectives. J. Assoc. Nurses AIDS Care 2020, 31, 25–34. [Google Scholar] [CrossRef]
- Value. Meriam-Webster Dictionary. Available online: https://www.merriam-webster.com/dictionary/value (accessed on 4 June 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.H. An Overview of the Schwartz Theory of Basic Values. Online Read. Psychol. Culture 2012, 2, 1. [Google Scholar] [CrossRef]
- Schwartz, S.H. Basic Human Values: An Overview Basic Human Values: Theory, Methods, and Applications Introduction to the Values Theory. Jerusalem Hebr. Univ. 2006, 48, 49–71. [Google Scholar]
- Young, R.; West, P. Do ‘good values’ lead to ‘good’ health-behaviours? Longitudinal associations between young people’s values and later substance-use. BMC Public Health 2010, 10, 165. [Google Scholar] [CrossRef] [PubMed]
- Seibert, M.; Hillen, H.A.; Pfaff, H.; Kuntz, L. Exploring leading nurses’ work values and their association with team safety climate: Results from a questionnaire survey in neonatal intensive care units. J. Nurs. Manag. 2019, 28, 112–119. [Google Scholar] [CrossRef]
- Pastorelli, B. Hofstede, Schwartz, … Why to Learn Them and When to Forget Them? Medium. 2022. Available online: https://benjamin-pastorelli.medium.com/hofstede-schwartz-why-to-learn-them-and-when-to-forget-them-cc5cd7ea908b (accessed on 1 May 2022).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Chaudhry, B.M.; Dasgupta, D.; Chawla, N.V. Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App. Int. J. Environ. Res. Public Health 2022, 19, 13148. [Google Scholar] [CrossRef]
- Pasina, L.; Brucato, A.L.; Falcone, C.; Cucchi, E.; Bresciani, A.; Sottocorno, M.; Taddei, G.C.; Casati, M.; Franchi, C.; Djade, C.D.; et al. Medication non-adherence among elderly patients newly discharged and receiving polypharmacy. Drugs Aging 2014, 31, 283–289. [Google Scholar] [CrossRef]
- Smaje, A.; Weston-Clark, M.; Raj, R.; Orlu, M.; Davis, D.; Rawle, M. Factors associated with medication adherence in older patients: A systematic review. Aging Med. 2018, 1, 254–266. [Google Scholar] [CrossRef]
- Foley, L.; Larkin, J.; Lombard-Vance, R.; Murphy, A.W.; Hynes, L.; Galvin, E.; Molloy, G.J. Prevalence and predictors of medication non-adherence among people living with multimorbidity: A systematic review and meta-analysis. BMJ Open 2021, 11, e044987. [Google Scholar] [CrossRef] [PubMed]
- Semahegn, A.; Torpey, K.; Manu, A.; Assefa, N.; Tesfaye, G.; Ankomah, A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Gadkari, A.S.; McHorney, C.A. Unintentional non-adherence to chronic prescription medications: How unintentional is it really? BMC Health Serv. Res. 2012, 12, 98. [Google Scholar] [CrossRef] [PubMed]
- Arain, M.A.; Ahmad, A.; Chiu, V.; Kembel, L. Medication adherence support of an in-home electronic medication dispensing system for individuals living with chronic conditions: A pilot randomized controlled trial. BMC Geriatr. 2021, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Patel, T.; Ivo, J.; Pitre, T.; Faisal, S.; Antunes, K.; Oda, K. An In-Home Medication Dispensing System to Support Medication Adherence for Patients With Chronic Conditions in the Community Setting: Prospective Observational Pilot Study. JMIR Form. Res. 2022, 6, e34906. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-Z.; Yu, C.-W.; Chao, C.-M.; Lin, F.-C. Influences on medical app adoption by patients: The unified theory of acceptance and use of technology model and the moderating effects of technology readiness. Soc. Sci. J. 2020, 1–14. [Google Scholar] [CrossRef]
- Zhou, L.L.; Owusu-Marfo, J.; Antwi, H.A.; Antwi, M.O.; Kachie, A.D.T.; Ampon-Wireko, S. Assessment of the social influence and facilitating conditions that support nurses’ adoption of hospital electronic information management systems (HEIMS) in Ghana using the unified theory of acceptance and use of technology (UTAUT) model. BMC Med Inform. Decis. Mak. 2019, 19, 230. [Google Scholar] [CrossRef]
- Almegbel, H.; Aloud, M. Factors Influencing the Adoption of mHealth Services in Saudi Arabia: A Patient-centered Study. Int. J. Comput. Sci. Netw. Secur. 2021, 21, 313–324. [Google Scholar] [CrossRef]
- Geber, S.; Friemel, T.N. Tracing-Technology Adoption During the COVID-19 Pandemic: The Multifaceted Role of Social Norms. Int. J. Commun. 2022, 16, 247–266. [Google Scholar]
- Dwivedi, R.; Mehrotra, D.; Chandra, S. Potential of Internet of Medical Things (IoMT) applications in building a smart healthcare system: A systematic review. J. Oral Biol. Craniofacial Res. 2021, 12, 302–318. [Google Scholar] [CrossRef]
- Al-Rawashdeh, M.; Keikhosrokiani, P.; Belaton, B.; Alawida, M.; Zwiri, A. IoT Adoption and Application for Smart Healthcare: A Systematic Review. Sensors 2022, 22, 5377. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient (PT) Participant Characteristics | ||||
| Participant ID | Gender | Age | Number of Medical Conditions | Number of Medications |
| 004-PT | Female | 56 | 1 | 1 |
| 005-PT | Female | 29 | 2 | NA |
| 017-PT | Female | 74 | 2 | 2 |
| 025-PT | Male | 78 | 2 | 2 |
| 019-PT | Male | 25 | 2 | 2 |
| Caregiver (CG) Participant Characteristics | ||||
| Participant ID | Gender | Age | Caring for | |
| 002-CG | Male | 32 | One Parent | |
| 021-CG | Female | 60 | One Parent | |
| 022-CG | Female | 51 | Both Parents | |
| 026-CG | Female | 70 | Both Parents | |
| 027-CG | Female | 64 | Both Parents | |
| Insurance Provider (IP) Participant Characteristics | ||||
| Participant ID | Work Experience | Educational Background | ||
| 014-IP | 10 years | Pharmacy | ||
| 018-IP | 10 years | Pharmacy, Health Economics | ||
| 023-IP | N/A | Pharmacy | ||
| 028-IP | 7 years | Pharmaceutical Policy | ||
| 029-IP | 25 years | Pharmaceutical Consultation | ||
| Physician (PY) Participant Characteristics | ||||
| Participant ID | Work Experience | Practice | ||
| 010-PY | >30 years | Family health team | ||
| 020-PY | 37 years | Family health team | ||
| 030-PY | N/A | Academic family physician | ||
| 031-PY | 13 years | Academic family physician | ||
| Pharmacist (P) and Pharmacy Owner (PO) Participant Characteristics | ||||
| Participant ID | Work Experience | Type of Practice | Prevalent Population | |
| 003-P | 14 years | Chain store | Chronic pain patients, diabetic patients | |
| 008-P | 8 years | Independent | Younger adults | |
| 009-P | 5 years | Chain store | Middle-aged to senior adults | |
| 011-P | 30 years | Chain store | Senior adults | |
| 012-P | 9 years | Chain store and family health team | Senior adults | |
| 015-P | 2 years | Chain store and family health team | Mixed population | |
| 016-P | 3 years | Independent | Geriatric patients | |
| 001-PO | 6 years | Independent | Senior adults | |
| 006-PO | 5 years | Independent | Mixed population | |
| 007-PO | 6 years | Independent | Low income, senior adults | |
| 013-PO | 8 years | Independent | New families | |
| 024-PO | 6 years | Independent, multiple locations | Mixed population | |
| Theme | Sub-Theme | Code |
|---|---|---|
| Perceptions of Integrating Smart Medication Adherence Technologies and Real-Time Monitoring | Benefits Expected from Product Use |
|
| Valuable Product Features |
| |
| Potential Users |
| |
| Technology Adoption Factors | Social Influence |
|
| User Characteristics |
| |
| Healthcare System Factors |
| |
| Data Management | Privacy |
|
| Data Sharing |
| |
| Liability |
| |
| Date Reporting |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faisal, S.; Ivo, J.; Abu Fadaleh, S.; Patel, T. Exploring the Value of Real-Time Medication Adherence Monitoring: A Qualitative Study. Pharmacy 2023, 11, 18. https://doi.org/10.3390/pharmacy11010018
Faisal S, Ivo J, Abu Fadaleh S, Patel T. Exploring the Value of Real-Time Medication Adherence Monitoring: A Qualitative Study. Pharmacy. 2023; 11(1):18. https://doi.org/10.3390/pharmacy11010018
Chicago/Turabian StyleFaisal, Sadaf, Jessica Ivo, Sarah Abu Fadaleh, and Tejal Patel. 2023. "Exploring the Value of Real-Time Medication Adherence Monitoring: A Qualitative Study" Pharmacy 11, no. 1: 18. https://doi.org/10.3390/pharmacy11010018
APA StyleFaisal, S., Ivo, J., Abu Fadaleh, S., & Patel, T. (2023). Exploring the Value of Real-Time Medication Adherence Monitoring: A Qualitative Study. Pharmacy, 11(1), 18. https://doi.org/10.3390/pharmacy11010018