
Exploring Muslims’ Health-Related Behaviours in Portugal: Any Impact on Quotidian Community Pharmacy Practice?



Abstract
:1. Introduction
2. Materials and Methods
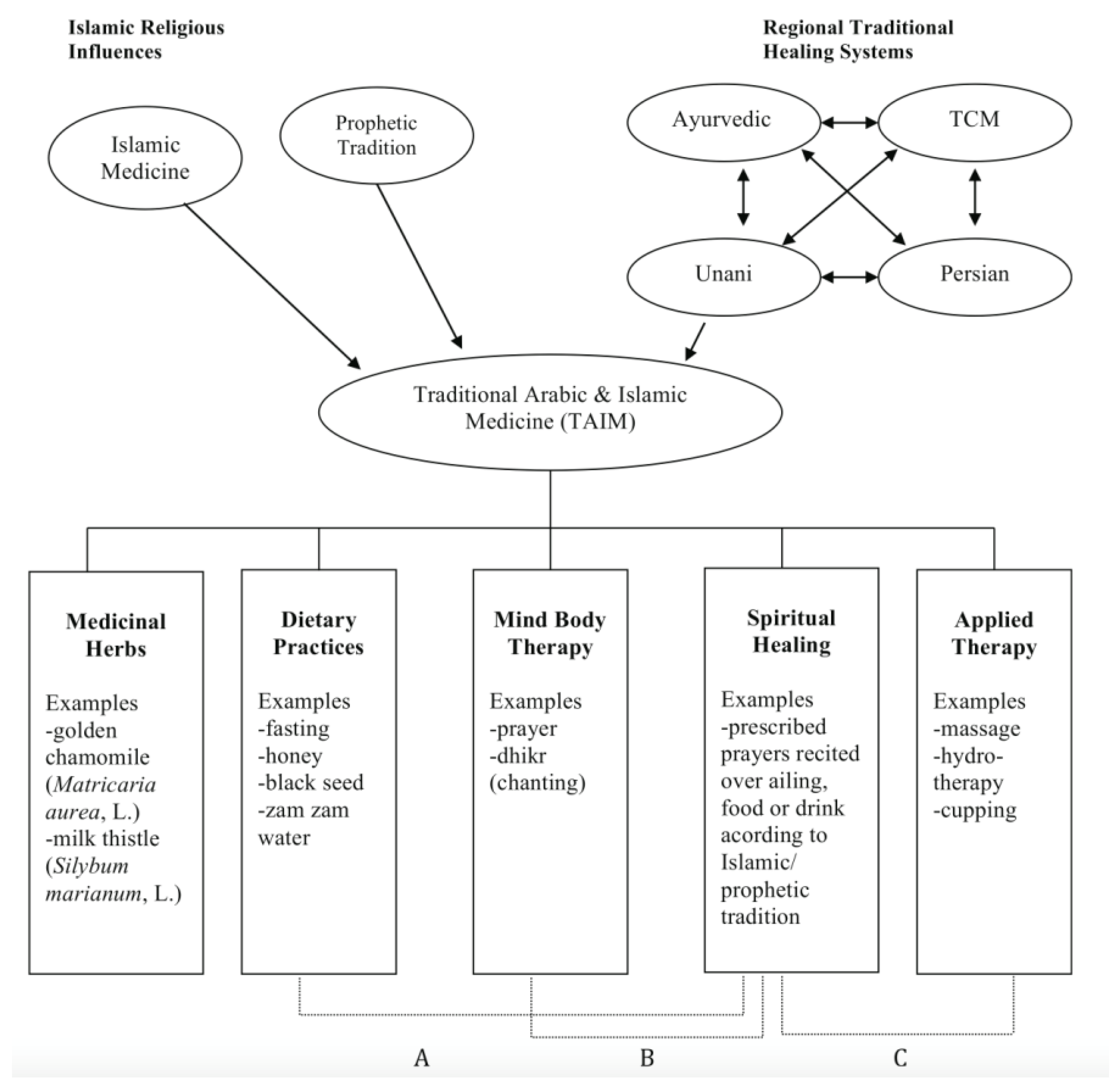
2.1. Traditional Arabic and Islamic Medicine
2.1.1. Dietary Practices (A)
2.1.2. Mind and Body Therapy (B)
2.1.3. Applied Therapy (C)
2.2. Survey Instrument
2.3. Sample and Sampling Procedures
2.4. Data Collection and Analysis
3. Results
3.1. Sociodemographic and Religious Data
3.2. Health Data and Conventional Healthcare
3.3. Complementary and Alternative Medicines
3.4. Religion and Healthcare
3.5. TAIM and Healthcare Products Usage
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pew Research Center. The Future of the Global Muslim Population; Projections for 2010–2030; Pew Research Center: Washington, DC, USA, 2011; Volume 13. [Google Scholar]
- Tiesler, N.C. Muslims on the Margin: The New Islamic Presence in Portugal. Sociol. Probl. Práticas 2000, 34, 117–144. [Google Scholar]
- Tiesler, N.C.; Cairns, D. Representing Islam and Lisbon Youth Portuguese Muslims of Indian-Mozambican Origin. Lusotopie 2007, 14, 223–238. [Google Scholar] [CrossRef]
- Dix, S. Religious Plurality within a Catholic Tradition: A Study of the Portuguese Capital, Lisbon, and a Brief Comparison with Mainland Portugal. Religion 2009, 39, 182–193. [Google Scholar] [CrossRef]
- Araújo, M. Islamophobia and Its Narratives in Portugal: Knowledge, Politics, Media and Cyberspace; Centre for Social Studies: Coimbra, Portugal, 2019; Volume 447, pp. 1–34. [Google Scholar]
- Zaidi, D. Influences of Religion and Spirituality in Medicine. AMA J. Ethics 2018, 20, E609–E612. [Google Scholar]
- Odeh Yosef, A.R. Health Beliefs, Practice, and Priorities for Health Care of Arab Muslims in the United States: Implications for Nursing Care. J. Transcult. Nurs. 2008, 19, 284–291. [Google Scholar] [CrossRef]
- Padela, A.I.; Gunter, K.; Killawi, A.; Heisler, M. Religious Values and Healthcare Accommodations: Voices from the American Muslim Community. J. Gen. Intern. Med. 2012, 27, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Arousell, J.; Carlbom, A. Culture and Religious Beliefs in Relation to Reproductive Health. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 32, 77–87. [Google Scholar] [CrossRef]
- Vu, M.; Azmat, A.; Radejko, T.; Padela, A.I. Predictors of Delayed Healthcare Seeking among American Muslim Women. J. Women’s Heal. 2016, 25, 586–593. [Google Scholar] [CrossRef] [Green Version]
- Daher, M.; Chaar, B.; Saini, B. Impact of Patients’ Religious and Spiritual Beliefs in Pharmacy: From the Perspective of the Pharmacist. Res. Soc. Adm. Pharm. 2015, 11, e31–e41. [Google Scholar] [CrossRef]
- Eriksson, A.; Burcharth, J.; Rosenberg, J. Animal Derived Products May Conflict with Religious Patients’ Beliefs. BMC Med. Ethics 2013, 14, 1–5. [Google Scholar] [CrossRef] [Green Version]
- da Costa, F.A.; Pedro, A.R.; Teixeira, I.; Bragança, F.; da Silva, J.A.; Cabrita, J. Primary Non-Adherence in Portugal: Findings and Implications. Int. J. Clin. Pharm. 2015, 37, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Martins, S.F.; van Mil, J.W.F.; da Costa, F.A. The Organizational Framework of Community Pharmacies in Europe. Int. J. Clin. Pharm. 2015, 37, 896–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, N.; Mota-Filipe, H.; Guerreiro, M.P.; da Costa, F.A. Primary Health Care Policy and Vision for Community Pharmacy and Pharmacists in Portugal. Pharm. Pract. 2020, 18, 2043. [Google Scholar] [CrossRef] [PubMed]
- International Pharmaceutical Federation. Quality Assurance of Pharmacy Education: The FIP Global Framework; FIP: The Hague, The Netherlands, 2014. [Google Scholar]
- International Pharmaceutical Federation. Pharmacy Education Taskforce: A Global Competency Framework; FIP: The Hague, The Netherlands, 2012. [Google Scholar]
- O’Connell, M.B.; Jackson, A.N.; Karaoui, L.R.; Rodriguez De Bittner, M.; Chen, A.M.H.; Echeverri, M.; Vyas, D.; Poirier, T.; Lee, S.Y.; O’Neil, C.K. Cultural Competency in Health Care and Its Implications for Pharmacy Part 3B: Emphasis on Pharmacy Education Policy, Procedures, and Climate. Pharmacotherapy 2013, 33, e368–e381. [Google Scholar] [CrossRef] [PubMed]
- Alrawi, S.N.; Fetters, M.D. Traditional Arabic & Islamic Medicine: A Conceptual Model for Clinicians and Researchers. Glob. J. Health Sci. 2012, 4, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Blades, M. Functional Foods or Nutraceuticals. Nutr. Food Sci. 2000, 30, 73–76. [Google Scholar] [CrossRef]
- El Sohaimy, S. Functional Foods and Nutraceuticals-Modern Approach to Food Science. World Appl. Sci. J. 2012, 20, 691–708. [Google Scholar] [CrossRef]
- Kahrizi, D.; Molsaghi, M.; Faramarzi, A.; Yari, K.; Kazemi, E.; Farhadzadeh, A.M.; Hemati, S.; Hozhabri, F.; Asgari, H.; Chaghamirza, K. Medicinal Plants in Holy Quran. Am. J. Sci. Res. 2012, 42, 62–71. [Google Scholar]
- Ahmad, A.; Husain, A.; Mujeeb, M.; Khan, S.A.; Najmi, A.K.; Siddique, N.A.; Damanhouri, Z.A.; Anwar, F. A Review on Therapeutic Potential of Nigella Sativa: A Miracle Herb. Asian Pac. J. Trop. Biomed. 2013, 3, 337–352. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, P.; Jena, S.; Satpathy, S.; Sahu, P.K. Nigella Sativa: Phytochemistry, Pharmacology and Its Therapeutic Potential. Res. J. Pharm. Technol. 2019, 12, 3111–3116. [Google Scholar] [CrossRef]
- Srinivasan, K. Cumin (Cuminum Cyminum) and Black Cumin (Nigella Sativa) Seeds: Traditional Uses, Chemical Constituents, and Nutraceutical Effects. Food Qual. Saf. 2018, 2, 1–16. [Google Scholar] [CrossRef]
- Al-Waili, N.S.; Salom, K.; Butler, G.; Al Ghamdi, A.A. Honey and Microbial Infections: A Review Supporting the Use of Honey for Microbial Control. J. Med. Food 2011, 14, 1079–1096. [Google Scholar] [CrossRef] [PubMed]
- Taghavizad, R. The Healing Effect of Honey as Stated in Quran and Hadith. J. Quran Med. 2011, 1, 3–8. [Google Scholar] [CrossRef]
- Bulotta, S.; Celano, M.; Lepore, S.M.; Montalcini, T.; Pujia, A.; Russo, D. Beneficial Effects of the Olive Oil Phenolic Components Oleuropein and Hydroxytyrosol: Focus on Protection against Cardiovascular and Metabolic Diseases. J. Transl. Med. 2014, 12, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Seedi, H.R.; Khalifa, S.A.; Yosri, N.; Khatib, A.; Chen, L.; Saeed, A.; Efferth, T.; Verpoorte, R. Plants Mentioned in the Islamic Scriptures (Holy Qur’ân and Ahadith): Traditional Uses and Medicinal Importance in Contemporary Times. J. Ethnopharmacol. 2019, 243, 112007. [Google Scholar] [CrossRef]
- Mousavi, T.; Rafiei, A.; Yoosefpour, M. Nutritional Value and Health Benefits of Dates According to Islamic Recourses and Traditional Medicine. J. Maz. Univ. Med. Sci. 2014, 24, 247–265. [Google Scholar]
- Khalid, N.; Ahmad, A.; Khalid, S.; Ahmed, A.; Irfan, M. Mineral Composition and Health Functionality of Zamzam Water: A Review. Int. J. Food Prop. 2014, 17, 661–677. [Google Scholar] [CrossRef]
- Shomar, B. Zamzam Water: Concentration of Trace Elements and Other Characteristics. Chemosphere 2012, 86, 600–605. [Google Scholar] [CrossRef]
- Ibrahimi, M.A.; Shah, M.S.M.; Mohd, R.A. Concept of Shifa in Al-Quran: Quranic Medicine Approach in Healing Physical Ailment. Al-Qanatir Int. J. Islam. Stud. 2015, 1, 1–19. [Google Scholar]
- Ibrahim, M.; Mohd Shah, A.; Mohd, R. Concept of Shifa’ in Al-Quran: Islamic Medicine Approach in Healing Physical Disorder. Al-Qanatir Int. J. Islam. Stud. 2018, 6, 23–39. [Google Scholar]
- Mehta, P.; Dhapte, V. Cupping Therapy: A Prudent Remedy for a Plethora of Medical Ailments. J. Tradit. Complement. Med. 2015, 5, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saad, B. Integrating Traditional Greco-Arab Additionally, Islamic Diet and Herbal Medicines in Research and Clinical Practice. In Phytotherapies: Efficacy, Safety, and Regulation; Ramzan, I., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; pp. 142–182. [Google Scholar]
- Sharafzadeh, S.; Alizadeh, O. German and Roman Chamomile. J. Appl. Pharm. Sci. 2011, 1, 1–5. [Google Scholar]
- Post-White, J.; Ladas, E.J.; Kelly, K.M. Advances in the Use of Milk Thistle (Silybum Marianum). Integr. Cancer Ther. 2007, 6, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Lavrakas, P. Encyclopedia of Survey Research Methods; Sage: Thousand Oaks, CA, USA, 2008; Volume 1, 2, pp. 140–141. [Google Scholar]
- Marôco, J. Statistical Analysis with SPSS Statistics, 7th ed.; ReportNumber, Lda: Lisbon, Portugal, 2018. [Google Scholar]
- Costa, S.; Santos, C.; Silveira, J. Community Pharmacy Services in Portugal. Ann. Pharmacother. 2006, 40, 2228–2234. [Google Scholar] [CrossRef]
- Alsharif, N.Z.; Dakkuri, A.; Abrons, J.P.; Williams, D.; Ombengi, D.N.; Zheng, H.A.; Al-Dahir, S.; Tofade, T.; Gim, S.; O’Connell, M.B.; et al. Current Practices in Global/International Advanced Pharmacy Practice Experiences: Home/Host Country or Site/Institution Considerations. Am. J. Pharm. Educ. 2016, 80, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazaldua, O.V.; Sias, J. Cultural Competence: A Pharmacy Perspective. J. Pharm. Pract. 2004, 17, 160–166. [Google Scholar] [CrossRef]
- Tiesler, N.C. Portugal. In Yearbook of Muslims in Europe; Nielsen, J.S., Akgönül, S., Alibašić, A., Maréchal, B., Moe, C., Eds.; Briil: Leiden, NL, USA, 2010; Volume 2, pp. 413–422. [Google Scholar]
- Abdul-Rauf, M. Marriage in Islam. Is Marriage Desirable? In Marriage in Islam; Al-Saadawi Publications: Alexandria, VA, USA, 1995; pp. 1–4. [Google Scholar] [CrossRef]
- Quinaz Romana, G.; Kislaya, I.; Salvador, M.R.; Cunha Gonçalves, S.; Nunes, B.; Dias, C. Multimorbidity in Portugal: Results from the First National Health Examination Survey. Acta Med. Port. 2019, 32, 30–37. [Google Scholar] [CrossRef]
- Canadian Agency for Drugs and Technologies in Health. Pharmacist-Led Medication Reviews: A Review of Clinical Utility and Cost-Effectiveness; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2019; pp. 1–26. [Google Scholar]
- Yuan, C.; Ding, Y.; Zhou, K.; Huang, Y.; Xi, X. Clinical Outcomes of Community Pharmacy Services: A Systematic Review and Meta-Analysis. Heal. Soc. Care Community 2019, 27, e567–e587. [Google Scholar] [CrossRef] [Green Version]
- Adib, S.M. From the Biomedical Model to the Islamic Alternative: A Brief Overview of Medical Practices in the Contemporary Arab World. Soc. Sci. Med. 2004, 58, 697–702. [Google Scholar] [CrossRef]
- Levin, J.S.; Vanderpool, H.Y. Is Religion Therapeutically Significant for Hypertension? Soc. Sci. Med. 1989, 29, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Attum, B.; Hafiz, S.; Malik, A.; Shamoon, Z. Cultural Competence in the Care of Muslim Patients and Their Families. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020; pp. 1–10. [Google Scholar]
- Ambali, A.R.; Bakar, A.N. People’s Awareness on Halal Foods and Products: Potential Issues for Policy-Makers. Procedia Soc. Behav. Sci. 2014, 121, 3–25. [Google Scholar] [CrossRef] [Green Version]
- El Sayed, S.M.; Mahmoud, H.S.; Nabo, M.M.H. Methods of Wet Cupping Therapy (Al-Hijamah): In Light of Modern Medicine and Prophetic Medicine. Altern. Integr. Med. 2013, 2, 1000111. [Google Scholar] [CrossRef] [Green Version]
- Akhu-Zaheya, L.M.; Alkhasawneh, E.M. Complementary Alternative Medicine Use among a Sample of Muslim Jordanian Oncology Patients. Complement. Ther. Clin. Pract. 2012, 18, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Jazieh, A.R.; Al Sudairy, R.; Abulkhair, O.; Alaskar, A.; Al Safi, F.; Sheblaq, N.; Young, S.; Issa, M.; Tamim, H. Use of Complementary and Alternative Medicine by Patients with Cancer in Saudi Arabia. J. Altern. Complement. Med. 2012, 18, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Izzo, A.A. Interactions between Herbs and Conventional Drugs: Overview of the Clinical Data. Med. Princ. Pract. 2012, 21, 404–428. [Google Scholar] [CrossRef] [PubMed]
- Sadeeqa, S.; Sarriff, A.; Masood, I.; Atif, M.; Farooqi, M. Evaluation of Knowledge, Attitude, and Perception Regarding Halal Pharmaceuticals, among General Medical Practitioners in Malaysia. Arch. Pharm. Pract. 2013, 4, 139. [Google Scholar] [CrossRef]
- Sarriff, A.; Abdul Razzaq, H.A. Exploring the Halal Status of Cardiovascular, Endocrine, and Respiratory Group of Medications. Malays. J. Med. Sci. 2013, 20, 69–74. [Google Scholar]
- Ali, E.; Sultana, S.; Hamid, S.B.A.; Hossain, M.; Yehya, W.A.; Kader, A.; Bhargava, S.K. Gelatin Controversies in Food, Pharmaceuticals, and Personal Care Products: Authentication Methods, Current Status, and Future Challenges. Crit. Rev. Food Sci. Nutr. 2018, 58, 1495–1511. [Google Scholar] [CrossRef]
- Amin, M.E.K.; Chewning, B. Pharmacist–Patient Communication about Medication Regimen Adjustment during Ramadan. Int. J. Pharm. Pract. 2016, 24, 419–427. [Google Scholar] [CrossRef]
- Almansour, H.A.; Chaar, B.; Saini, B. Pharmacists’ Perspectives about Their Role in Care of Patients with Diabetes Observing Ramadan. Res. Soc. Adm. Pharm. 2017, 13, 109–122. [Google Scholar] [CrossRef]
- Abdelaziz, T.A.; Abdulraheem, M.A.; Badi, S.A.; Badawi, M.I.; Saeed, A.O.; Elobied, M.A.; Ahmed, M.H. Knowledge, Attitude and Practice of Sudanese Pharmacist with Regard to Management of Diabetes during Ramadan: A Cross-Sectional Survey. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Tourkmani, A.M.; Alharbi, T.J.; Bin Rsheed, A.M.; AlRasheed, A.N.; AlBattal, S.M.; Abdelhay, O.; Hassali, M.A.; Faya, S.I.; Assiri, E.S.; Al Ghishiayan, K.I.; et al. Impact of Ramadan Focused Education Program on Medications Adjustment for Patients with Type 2 Diabetes in a Primary Health Care Institution in Saudi Arabia. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 161–165. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Chronic Diseases | ATC Drug Classification | ||
|---|---|---|---|
| Circulatory system (12%) | |||
| Arterial hypertension | 5% | C09: Agents acting on the renin-angiotensin system | 4% |
| C07: Beta-blocking agents | 5% | ||
| Hypercholesterolemia | 4% | C1: Lipid modifying agents | 3% |
| Hypertriglyceridemia | 1% | ||
| Other circulatory system diseases | 2% | B01: Anti-thrombotic agents | 2% |
| Respiratory system (9%) | |||
| Asthma | 5% | S02B: Corticosteroids | 2% |
| Sinusitis/rhinitis | 4% | R06A: Antihistamines for systemic use | 11% |
| Digestive system (7%) | A02: Drugs for gastric disorders | 2% | |
| N02: Analgesics | 15% | ||
| Immune system diseases (7%) | L04: Immunosuppressants | 2% | |
| Health Products | Frequency of Use (%) | Total n. of Different Uses | Most Frequent Medicinal Use | |
|---|---|---|---|---|
| Medicinal plants | Black cumin (seeds) | 20 | 3 | Helps protect against diseases |
| Milk thistle (fruits and seeds) | 6 | 2 | Helps the digestive system | |
| Golden chamomile (flowers) | 4 | 2 | Helps to relax | |
| Functional foods | Honey | 89 | 8 | Anti-inflammatory properties |
| Olive oil | 87 | 7 | Helps general well-being | |
| Zamzam water | 58 | 4 | Helps general well-being | |
| Dates | 5 | 1 | Helps general well-being | |
| Figs | 1 | 1 | Helps prevent constipation | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omar, A.; Dramce, G.; Lakic, D.; Cavaco, A. Exploring Muslims’ Health-Related Behaviours in Portugal: Any Impact on Quotidian Community Pharmacy Practice? Pharmacy 2022, 10, 55. https://doi.org/10.3390/pharmacy10030055
Omar A, Dramce G, Lakic D, Cavaco A. Exploring Muslims’ Health-Related Behaviours in Portugal: Any Impact on Quotidian Community Pharmacy Practice? Pharmacy. 2022; 10(3):55. https://doi.org/10.3390/pharmacy10030055
Chicago/Turabian StyleOmar, Aisha, Grishma Dramce, Dragana Lakic, and Afonso Cavaco. 2022. "Exploring Muslims’ Health-Related Behaviours in Portugal: Any Impact on Quotidian Community Pharmacy Practice?" Pharmacy 10, no. 3: 55. https://doi.org/10.3390/pharmacy10030055
APA StyleOmar, A., Dramce, G., Lakic, D., & Cavaco, A. (2022). Exploring Muslims’ Health-Related Behaviours in Portugal: Any Impact on Quotidian Community Pharmacy Practice? Pharmacy, 10(3), 55. https://doi.org/10.3390/pharmacy10030055