Extending Pharmacist Roles in Primary Healthcare to Meet the Needs of Universal Health Coverage in Zimbabwe: A Pharmacist Perspective and Curriculum Evaluation


Abstract
:1. Introduction
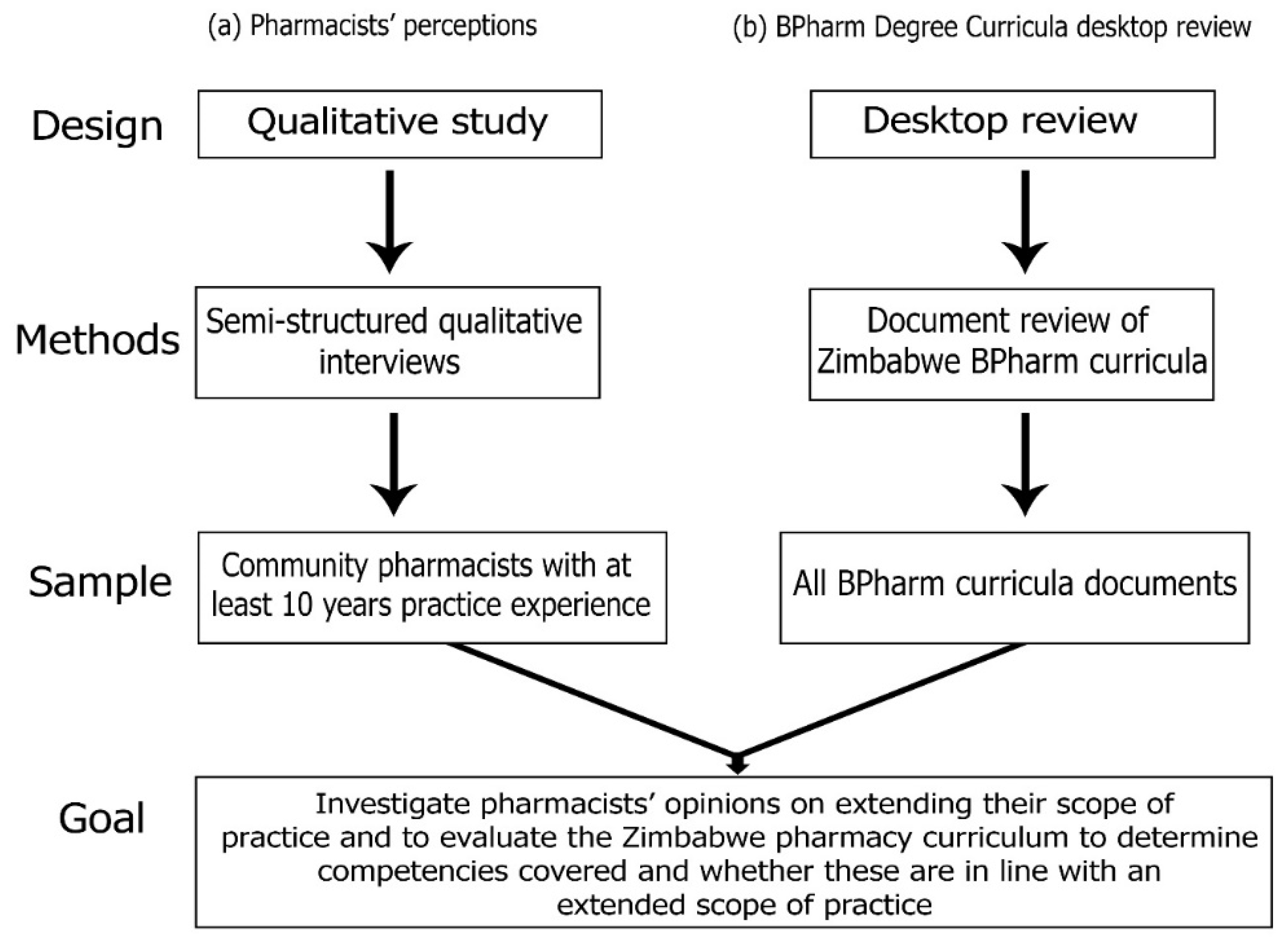
2. Materials and Methods
2.1. Arm a: Pharmacists’ Perceptions
2.1.1. Study Design and Setting
2.1.2. Study Population and Sampling Strategy
2.1.3. Development of the Data Collection Tool
- (i)
- Perceived knowledge on universal health coverage and the current role of the Zimbabwean pharmacist
- (ii)
- Pharmacist views on extending Zimbabwean pharmacists’ roles in patient care
- (iii)
- Pharmacists’ views on the BPharm curricula and if it equipped pharmacists with exit level competencies supporting extended pharmacist roles in patient care
- (iv)
- Pharmacists’ desired roles in the Zimbabwe healthcare system to achieve universal health coverage.
2.1.4. Procedure for Carrying out Interviews
2.1.5. Data Collection and Analysis
2.2. Arm b: Curriculum Review
2.2.1. Data Collection and Analysis
2.2.2. Conversion of Credits into Hours
2.2.3. Division of Core Curriculum Content and Comparison
2.3. Ethical Approval
3. Results
3.1. Pharmacists’ Perceptions
3.1.1. Theme 1: Understanding UHC
“Universal health coverage is the concept of ensuring that everybody is able to access good quality health in a way that is affordable, and which is acceptable”.
“Ensuring that everybody is able to access health without financial hardship or strain”.
3.1.2. Theme 2: Current Pharmacist Role in the Community
“The main duties of a retail pharmacist is dispensing medicines to patients. We also counsel patients on prescribed medication and break bulk to meet specific customer needs”.
“I would say dispensing accounts for 95% of our duties, the other 5% is patient counselling, point of care diagnostics tests and stock management”.
3.1.3. Theme 3: Potential Extended Roles of Community Pharmacists
Providing Vaccines and Immunisations
“With the current curriculum pharmacists are obviously not equipped to administer injections but with appropriate training, they can effectively administer immunisations and vaccines just like village health workers some without even O Levels (“O Level” examinations are taken after four years of secondary school) but can test for malaria and prescribe Coartem [artemether/lumefantrine tablets] in the rural areas after undergoing training”.
“A three-day course is enough to recap and educate pharmacists on how vaccines and immunisations can be administered”.
Pharmacist Physical Examinations and Prescribing in Minor Ailments, HIV/AIDS
“Pharmacists have been doing minor physical examinations including ear and eye check, tonsillitis, minor injuries and burns and recommending over the counter treatments and pharmacist-initiated medicines. Where there is need for further examinations, they have always referred to the appropriate cadre for further assistance”.
“Minor ailments must be fully described and the management options fully described and documented into an Essential Drug List for Pharmacists with clear standard treatment guidelines and protocols for referral”.
Ordering and Reviewing Laboratory Data for Monitoring Services in the Management of Disease Conditions
“I understand that pharmacists are using rapid diagnostic tests in the pharmacy to check for BP (blood pressure), cholesterol, HIV, malaria amongst other tests. These point of care diagnostics may not be the gold standard but pharmacists are already ordering these tests in their premises and interpreting the results”.
“Pharmacists should be involved directly with patient care and allowed to take responsibility for their actions in improving patient health outcomes. Pharmacists should be allowed to order glycated haemoglobin concentration, INR in patients on warfarin and so on. This service will definitely improve patient health outcomes and lower costs”.
“I think pharmacists have the capacity to order laboratory tests and review prescriptions. I would strongly recommend that pharmacists get practical courses and training in the principles behind interpretation of laboratory tests and adjustment of doses”.
Change Drug Dosage/Formulation and Renew or Extend Prescriptions
“This practice of extending prescriptions has been going on but without monitoring the patient. Patients usually come to the pharmacy asking for their repeat drugs and pharmacists usually dispense these chronic medications without asking for the prescription as long as the patient is in their database”.
“Allowing pharmacists to extend physician prescriptions will confer responsibility on the pharmacist and eliminate the bad practices that have been going on”
“Pharmacists may not be capable or competent to extend prescriptions at the moment but that is an area that they should embrace in an effort to achieve Universal Health Coverage”.
3.1.4. Theme 4: Barriers to Extended Pharmacist Services
“I think the expanded roles are sort of specialist branches of pharmacy and would need specialisation through training and certification”.
“Our premises do not offer privacy, you can’t give an injection in the eyes of everyone, pharmacies would need a new design and there is also need for a quiet room equipped to handle emergencies, for example anaphylaxis and sedation”.
“I think we lack confidence in doing our duties. We are too scared to bend the law and we always refer. I personally fail to make basic simple decisions that help the patient and simply refer for the fear of responsibility”.
“There is need to work out reimbursement models for pharmacists to be remunerated for these services. They should not be for free because remember the pharmacist is using his professional knowledge and time and the fee charged should promote access to health and not hinder or cast-off patients”.
3.1.5. Theme 5: Current Scope of BPharm Degree
“The BPharm (Hons) 1 pharmacy degree was supposed to be reviewed after every 4 to 5 years. The last review was done in 1994 and that’s more than 20 years ago. The degree has definitely outlived its usefulness”.
“There is need for a patient focused curriculum to meet patient needs. More focus of the degree should be on clinical pharmacy and pharmacy practice experiences and not manufacturing”.
“I think we need to shift from viewing pharmacists as technical people designed to count tablets into professionals who are patient centred. The degree curriculum does not equip the Pharmacists with terminal competencies supporting an extended scope of practice”.
“Pharmacists should be more clinical and hence more clinical roles should be added to the pharmacist duties in the undergraduate curricula. The policy makers want pharmacists to be more technical so that they can manufacture more medicines locally. They cannot support pharmacists giving vaccines when they believe that pharmacists can make medicines locally thereby reducing the import bill”.
3.1.6. Theme 6: Desired Pharmacist Role in UHC
“I will be very happy to see pharmacists adopt all the above extended services that we have been discussing. The pharmacist has to leave dispensing of medications to pharmacy technicians and dispensary assistants”.
“The pharmacist needs to be involved in direct patient care such as identifying and managing drug therapy problems, communicating with the physician, prescription extension, ordering and reviewing laboratory data and administration of vaccines and immunisations”.
“The pharmacy should be a community health centre where people can access health with easy. The pharmacist needs to be more clinical and patient oriented to achieve universal health coverage”.
3.2. Document Review of the BPharm Curriculum in Each School
4. Discussion
4.1. Study Limitations
4.2. Recommendations
5. Conclusions
- Lack of standardization or uniformity in the undergraduate degree programmes leading to be a registered pharmacist
- Lack of confidence by some front-line pharmacists
- Lack of adequate compensation to perform the extended service
- Lack of collaboration or a team-based approach with other healthcare providers.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Child Welfare-Directorate of Pharmacy Services; World Health Organization. Zimbabwe Pharmaceutical Country Profile. 2011. Available online: https://www.who.int/medicines/areas/coordination/Zimbabwe_PSCPNarrativeQuestionnaire_27052011.pdf (accessed on 19 December 2021).
- Hpa.co.zw. Downloads|Health Professions Authority. 2020. Available online: https://www.hpa.co.zw/new/downloads/ (accessed on 31 December 2021).
- Van Mil, J.W.F.; Schulz, M.; Tromp, T.F.D. Pharmaceutical care, European developments in concepts, implementation, teaching, and research: A review. Pharm. World Sci. 2004, 26, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Ecolex.org. Medicines and Allied Substances Control (General) Regulations, 1991 (Cap.15:03). 2021. Available online: https://www.ecolex.org/details/legislation/medicines-and-allied-substances-control-general-regulations-1991-cap1503-lex-faoc117614/ (accessed on 20 November 2021).
- Lloyd, F.; Hughes, C.M. Pharmacists’on and mentors’on views on the introduction of pharmacist supplementary prescribing: A qualitative evaluation of views and context. Int. J. Pharm. Pract. 2007, 15, 31–37. [Google Scholar] [CrossRef]
- Universal Health Coverage Partnership|EU-LUX. Zimbabwe|Universal Health Coverage Partnership. 2020. Available online: https://www.uhcpartnership.net/country-profile/zimbabwe/ (accessed on 19 October 2021).
- Who.int. Universal Health Coverage. Available online: https://www.who.int/health-topics/universal-health-coverage (accessed on 10 May 2021).
- Goode, J.-V.; Owen, J.; Page, A.; Gatewood, S. Community-Based Pharmacy Practice Innovation and the Role of the Community-Based Pharmacist Practitioner in the United States. Pharmacy 2019, 7, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, M. BC Pharmacists Explore Prescribing Rights. Can. Pharm. J. 2007, 140, 87. [Google Scholar] [CrossRef]
- Galt, K.A. The key to pharmacist prescribing: Collaboration. Am. J. Health Pharm. 1995, 52, 1696–1699. [Google Scholar] [CrossRef] [PubMed]
- SAGE Journals. Canadian Pharmacists Scope 20/20: A Vision for Harmonized Pharmacists’on Scope in Canada—Philip Emberley, 2018. 2021. Available online: https://journals.sagepub.com/doi/10.1177/1715163518804148 (accessed on 14 July 2021).
- Guillaume, L.; Cooper, R.; Avery, A.; Mitchell, S.; Ward, P.; Anderson, C.; Bissell, P.; Hutchinson, A.; James, V.; Lymn, J.; et al. Supplementary prescribing by community and primary care pharmacists: An analysis of PACT data, 2004–2006. J. Clin. Pharm. Ther. 2008, 33, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Dalton, K.; Byrne, S. Role of the pharmacist in reducing healthcare costs: Current insights. Integr. Pharm. Res. Pract. 2017, 6, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, J. Expanded pharmacy practice: Where are we, and where do we need to go? Can. Pharm. J./Rev. Des Pharm. Can. 2013, 146, 365–367. [Google Scholar] [CrossRef] [Green Version]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Health Pharm. 1990, 47, 533–543. [Google Scholar] [CrossRef]
- Guest, G.; MacQueen, K.; Namey, E. Applied Thematic Analysis; Sage Publications: Los Angeles, CA, USA, 2012; pp. 7–18. [Google Scholar]
- Acpe-accredit.org. Accreditation Council of Pharmacy Education’on s (ACPE). Accreditation Standards and Guidelines for the Professional Program in Pharmacy Leading to the Doctor of Pharmacy. Available online: https://www.acpe-accredit.org/pdf/CS_PoliciesandProceduresAugust2020.pdf (accessed on 9 September 2020).
- Knoer, S.; Eck, A.; Lucas, A. A review of American pharmacy: Education, training, technology, and practice. J. Pharm. Health Care Sci. 2016, 2, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Association of Boards of Pharmacies. Pharmacy Curriculum Outcomes Assessment (PCOA) Guidelines. 2020. Available online: http://www.nabp.net/programs/assessment/pcoa (accessed on 29 October 2020).
- Pharm.D. Curriculum. Available online: https://curriculum.pharmacy.ufl.edu/curriculum-courses (accessed on 13 January 2021).
- Who.int. Joint Fip/Who Guidelines on Good Pharmacy Practice: Standards for Quality of Pharmacy Services. Available online: https://www.who.int/medicines/areas/quality_safety/quality_assurance/FIPWHOGuidelinesGoodPharmacyPracticeTRS961Annex8.pdf (accessed on 4 March 2022).
- World Health Organization. WHO Policy Perspectives on Medicines. 2021. Available online: https://www.who.int/medicines/publications/policyperspectives/en/ (accessed on 4 May 2021).
- Thamby, S.A.; Subramani, P. Seven-star pharmacist concept by World Health Organization. J. Young-Pharm. 2014, 6, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Malangu, N. The Future of Community Pharmacy Practice in South Africa in the Light of the Proposed New Qualification for Pharmacists: Implications and Challenges. Glob. J. Health Sci. 2014, 6, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickware, C. A Quiet Revolution: How Pharmacist Prescribers Are Reshaping Parts of the NHS. Available online: https://pharmaceutical-journal.com/article/feature/a-quiet-revolution-how-pharmacist-prescribers-are-reshaping-parts-of-the-nhs (accessed on 25 March 2022).
- Pharmacist.com. Scope of Practice. 2021. Available online: https://pharmacist.com/Practice/Practice-Resources/Scope-of-Practice (accessed on 30 December 2021).
- Dennis, S.; May, J.; Perkins, D.; Zwar, N.; Sibbald, B.; Hasan, I. What evidence is there to support skill mix changes between GPs, pharmacists and practice nurses in the care of elderly people living in the community? Aust. New Zealand Health Policy 2009, 6, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, A.; Khan, M.U.; Moorthy, J.; Kumar, B.D.; Kumar, G.S.; Patel, I. Comparison of knowledge, attitudes and perceived barriers towards adverse drug reactions reporting between Bachelor of Pharmacy and Doctor of Pharmacy students in Southern India. J. Pharm. Health Serv. Res. 2016, 7, 63–69. [Google Scholar] [CrossRef]
- Perepelkin, J.; Ulrich, E. Community Pharmacy Professional Service Availability: An International Comparison. Res. Soc. Adm. Pharm. 2014, 10, e13. [Google Scholar] [CrossRef]
- The Independent. Doctors Strike Reflect National Crisis. Available online: https://www.theindependent.co.zw/2018/12/21/doctors-strike-reflects-national-crisis/> (accessed on 17 July 2020).
- Mrtek, R.G.; Catizone, C. Pharmacy and the professions. In Pharmacy Practice, Social and Behavioural Aspects; Wertheimer, A.I., Smith, M.C., Eds.; Williams and Wilkins: London, UK, 1989; pp. 23–41. [Google Scholar]


{kind=link}
| Characteristics | Frequency | |
|---|---|---|
| Age (years) | ||
| 31–40 | 5 | |
| 41–50 | 3 | |
| >51 | 2 | |
| Gender | ||
| Male | 8 | |
| Female | 2 | |
| Qualifications | ||
| BPharm | 8 | |
| PharmD | 1 | |
| MPhil | 1 | |
| Experience (Years) | ||
| 10–14. | 3 | |
| 15–20 | 3 | |
| >21 | 4 | |
| Position in pharmacy | ||
| Employee manager | 7 | |
| Employee owner | 3 | |
| Geographical location of pharmacies | ||
| Urban area | 8 | |
| Rural area | 2 |
| Core Area | BPharm (Hons) 1 | BPharm (Hons) 2 | ||
|---|---|---|---|---|
| Hours | % | Hours | % | |
| Basic and Biomedical Sciences | 305 | 12 | 870 | 33.7 |
| Pharmaceutical Sciences | 1257 | 49.4 | 1200 | 46.5 |
| Social/Behavioural/Administrative Sciences | 542 | 21.3 | 240 | 9.3 |
| Clinical Sciences | 441 | 17.3 | 270 | 10.5 |
| Total Hours | 2545 | 100 | 2580 | 100 |
| Extended Pharmacist | BPharm | BPharm | Comments |
|---|---|---|---|
| Service | (Hons) 1 | (Hons) 2 | |
| Administration of vaccines and immunisations | Yes | No | BPharm(Hons) 1 is thorough on the theoretical aspects of immunological products and vaccines but does not include practical aspects of their administration |
| Prescribing in HIV/AIDS | Yes | No | BPharm(Hons) 1 is exhaustive on the theoretical management of patients with HIV/AIDs |
| Change drug dosage/formulation | No | No | This extended service is not well defined in both pharmacy curricula |
| Order and review laboratory data | No | No | This extended service is not well defined in both pharmacy curricula |
| Review or extend a prescription | No | No | This service is not well defined in both pharmacy curricula |
| Prescribe in minor ailments | No | No | This service is not well defined in both pharmacy curricua |
| Smoking cessation programs | No | No | This extended service is not available in both programmes |
| Drug and substance abuse | No | No | This extended service is not available in both programmes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiutsi, D.; Suleman, F.; Perumal-Pillay, V.A. Extending Pharmacist Roles in Primary Healthcare to Meet the Needs of Universal Health Coverage in Zimbabwe: A Pharmacist Perspective and Curriculum Evaluation. Pharmacy 2022, 10, 54. https://doi.org/10.3390/pharmacy10030054
Chiutsi D, Suleman F, Perumal-Pillay VA. Extending Pharmacist Roles in Primary Healthcare to Meet the Needs of Universal Health Coverage in Zimbabwe: A Pharmacist Perspective and Curriculum Evaluation. Pharmacy. 2022; 10(3):54. https://doi.org/10.3390/pharmacy10030054
Chicago/Turabian StyleChiutsi, Douglas, Fatima Suleman, and Velisha Ann Perumal-Pillay. 2022. "Extending Pharmacist Roles in Primary Healthcare to Meet the Needs of Universal Health Coverage in Zimbabwe: A Pharmacist Perspective and Curriculum Evaluation" Pharmacy 10, no. 3: 54. https://doi.org/10.3390/pharmacy10030054
APA StyleChiutsi, D., Suleman, F., & Perumal-Pillay, V. A. (2022). Extending Pharmacist Roles in Primary Healthcare to Meet the Needs of Universal Health Coverage in Zimbabwe: A Pharmacist Perspective and Curriculum Evaluation. Pharmacy, 10(3), 54. https://doi.org/10.3390/pharmacy10030054