
Telemedicine: A Survey of Telecommunication Technologies, Developments, and Challenges

 , , ,
, , ,  , , , ,
, , , ,
Abstract
1. Introduction
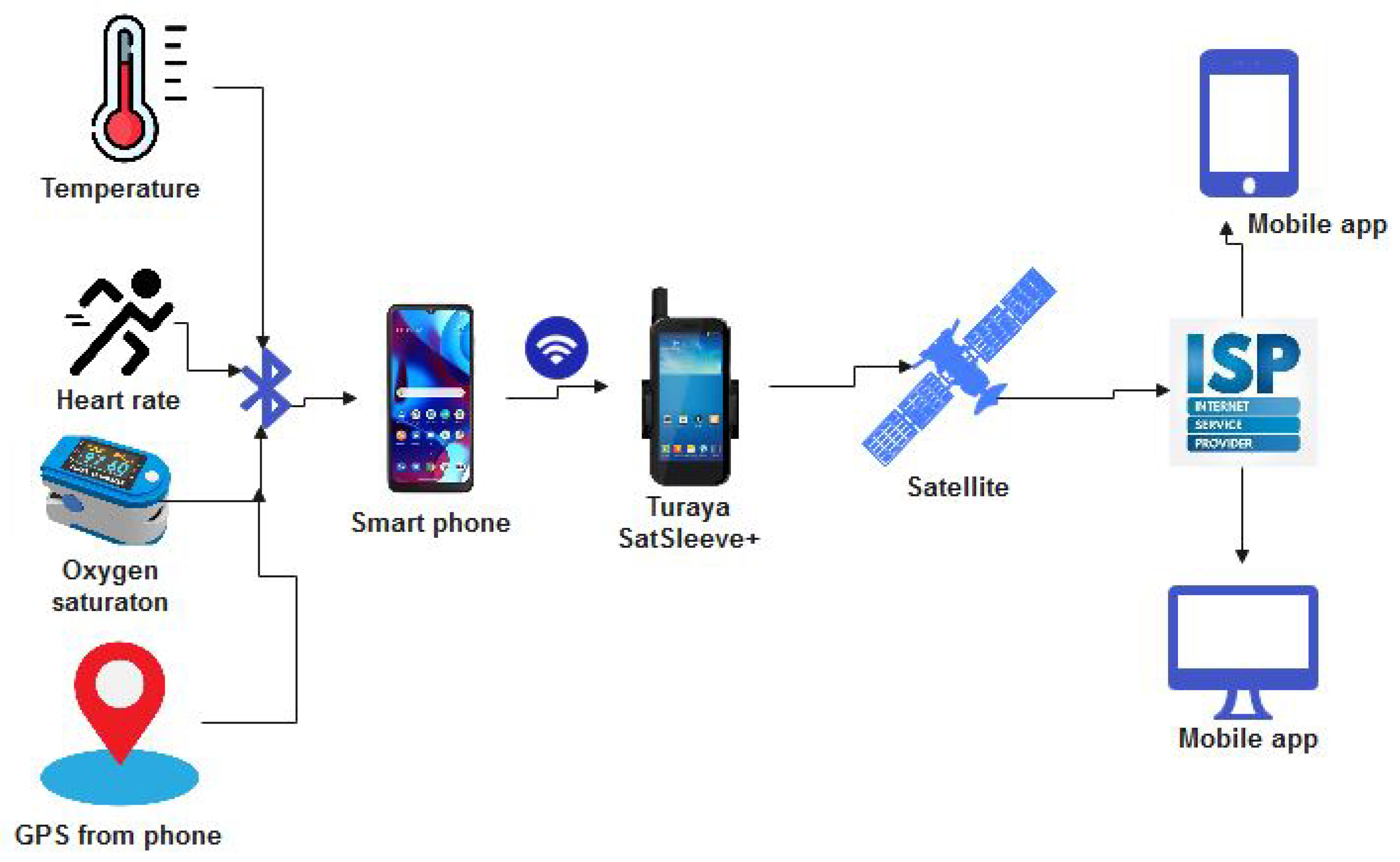
- Body Area Communication: communication between patients and telemedical devices such as the wearable sensors;
- Remote Communications: communication between the telemedical devices and remote servers, including satellite, internet, GSM, and WAN communications;
- Communication based on application area, including communication for emergency telemedicine, video conferencing, and transmission of medical images.
- An overview of telemedicine and the evolution of telecommunications technology;
- A review of the various standards and protocols present in telemedicine, with a focus on the current trends;
- Identification of several deployment challenges along with the state-of-the-art in this research area.
2. Related Work
3. Overview of Telemedicine
- User Interface Device: this is the device that the patient or healthcare provider uses to access the telemedicine system; it could be a smartphone, tablet, computer, or any other device that has an internet connection.
- Communication Device: this device is responsible for establishing and maintaining the communication channel between the user interface device and the virtual medical device; it could be a modem, router, or any other networking device that can transmit data over the internet
- Communication Channel: this is the pathway through which data are transmitted between the user interface device and the virtual medical device; it could be a wired or wireless connection, depending on the type of communication device being used.
- Video Conferencing Device: this is a feature of the telemedicine system that enables live video and audio communication between the patient and healthcare provider; it allows for real-time interaction, examination, and diagnosis
- Control Set: this is a set of rules that governs the transmission of data over the communication channel; it ensures that the data is transmitted in a secure, reliable, and efficient manner.
- Protocol: This is a set of rules that govern the transmission of data over the communication channel. It ensures that that data are transmitted in a secure, reliable, and efficient manner.
- Backplane: this is the backbone of the telemedicine system that connects all the components together; it provides a high-speed and low-latency connection that enables real-time communication and data transfer. The backplane presents two kinds of interface to the system, namely, registry interface and object-supporting interface. The registry interface notes when parts join the system, change their inner state, or leave the system. Protocol components use registry data to find resources required for their activities. The object-supporting interface contains objects that aid local communications.
- Virtual Medical Device: this is a device that simulates the functions of a physical medical device; it could be a software program that runs on a computer or a specialized device that connects to the telemedicine system, and allows for remote examination, diagnosis, and treatment of the patient.
- Medical Device: this is a physical device that is used to examine, diagnose, or treat the patient; it could be a blood pressure monitor, stethoscope, or any other medical instrument that can be connected to the telemedicine system.
- EMR and Data Storage: these are electronic medical records (EMR) of patients stored in the telemedicine system; they include the patient’s medical history, diagnosis, treatment plan, and other relevant information. The data storage component ensures that the data are stored securely and can be accessed by authorized personnel.
3.1. Components of Telemedicine
3.1.1. Patient’s WBAN Unit
- Electrocardiogram (ECG), which records the heart’s electrical signals.
- Pulse oximeter, which records the hemoglobin oxygen concentration in the blood.
- Pulse/heart rate.
- Blood pressure.
- Body temperature.
- Electroencephalogram (EEG), for measuring electrical activity in the human brain.
- Electromyography [57], for the assessment of nerve and muscle cells.
- Photoplethysmography (PPG).
- Electrooculogram (EOG), for eye diagnosis.
- Diet sensors, for monitoring eating patterns and assessing Type II diabetes and coronary heart disease.
- Galvanic Skin Response (GSR).
- Field Effect Transistor-based (FET-based) sensors; these are ultrasensitive, and are used to detect Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) antigens.
- Laser-engraved graphene-based immunosensors, which are used o obtain a diagnosis from saliva.
- Nanomaterial-based hybrid sensors for exhaled breath analysis, which enable machine learning-assisted COVID-19 diagnosis.
3.1.2. Communications Technology Unit
- Bluetooth stack of protocols;
- Zigbee stack of protocols;
- Wireless Application Protocol (WAP);
- File Transfer Protocol (FTP);
- Hypertext Transfer Protocol (HTTP);
- TCP/IP;
- UDP.
3.1.3. Remote Medical Server Unit
3.1.4. Medical Professional Unit
3.2. Specialist Application of Telemedicine
- Teleradiology: in the field of telemedicine, teleradiology was one of the earliest subspecialties to emerge, having first been used in the 1960s [69]. In order to improve people’s access to radiologists, many teleradiology services have been created. It is quite possible that smaller hospitals around the globe may not always have a radiologist on staff, or may not have access to one at all hours of the day. This means that emergency room visitors, especially those who show up outside of normal business hours, have to wait for a diagnosis. Today, a skilled radiologist can be consulted remotely and quickly by sending a patient’s x-rays and documents to them through a secure teleradiology system [70].
- Telepsychiatry: using telepsychiatry, experienced psychiatrists can treat patients remotely, increasing patient access to mental health care. Psychiatrists are in short supply across many countries, and unlike other medical specialties psychiatry often does not necessitate extensive physical exams.
- Teledermatology: with the help of teledermatology technology, primary care physicians can remotely diagnose skin conditions such as rashes, moles, and other abnormalities. Primary care physicians and nurses are frequently the first in the medical field to recognize a problem and refer patients to specialists. Using teledermatology, high-resolution cameras can relate skin conditions to a remote primary care physicians, who can continue coordinating their patients’ care while providing prompt response as to whether or not a blood sample test examination is warranted.
- Teleophthalmology: using teleophthalmology technology, eye doctors can remotely monitor therapy progress and conduct examinations on patients.
- Telenephronology: telenephrology refers to the practice of remotely consulting a nephrologist; an example of an inter-professional application of telenephrology solutions is the case of a family doctor who requires a specialist opinion concerning a patient who has kidney disease.
- Teleobstetrics: through teleobstetrics, gynecologists can provide prenatal care to expectant mothers from afar; as an example, a doctor at one facility could film an ultrasound of a baby’s heart and send it to an obstetrician in another location for analysis.
- Teleonchology: with the goal of making cancer treatment more accessible, teleoncology has grown rapidly in recent years; among the different teleoncology technologies are store-and-forward mechanisms that transmit images for diagnosis and real-time video platforms that enable oncologists to consult with patients.
- Telepathology: through the use of telepathology technologies, pathologists are able to collaborate remotely on pathology cases for the purposes of diagnosis, study, and instruction; many telepathology solutions are “save and forward” systems that let pathologists send and receive high-resolution images and videos.
- Telerehabilitation: telemedicine allows healthcare providers to remotely provide rehabilitation treatments such as physical therapy to those who need them.
3.3. Benefits of Telemedicine
- Improved Patient Access and Convenience: the primary motivation behind the development of the telemedicine sphere is the desire to provide patients with easier access to high-quality medical care. The United States is widely credited as the birthplace of telemedicine, where it was established to fill the gap in medical care in under-served areas, particularly rural outposts [72]. Today, telemedicine is used all around the world, whether to provide primary care to residents of developing nations or to help an older patients with mobility challenges receive the medical attention they need without leaving the house. In addition to removing the restrictions that distance and time usually place on receipt of medical attention, telemedicine has the potential to streamline the entire healthcare delivery process for patients.
- Reduced Medical Expenses: every year, the United States spends more than any other developed country on healthcare, at nearly USD 2.9 trillion. [73]. Moreover, it is anticipated that almost USD 200 billion of these costs are wasteful and unnecessary expenditures. Because of its potential to improve the efficiency of regular healthcare appointments and reduce wasteful spending on items such as emergency room visits and drug refills, telemedicine has the potential to significantly reduce the national healthcare budget.
- Improving the Availability of Expert Advice: one of the most immediate benefits of implementing telemedicine into a medical facility or practice is the increased availability of subspecialists. This paves the way for primary care physicians to confer with medical specialists on a patient’s condition and for patients to see a required specialist regardless of their location. In addition, telemedicine allows X-Ray examinations to be outsourced, which is particularly useful for small hospitals that do not have a full staff of radiologists [72].
- Increasing Patient Participation: with the use of telemedicine, patients can maintain regular contact with their physician at their own convenience, which increases their level of involvement in their own care. In this way, the doctor–patient relationship is strengthened and patients have a greater sense of control over their health care.
- Higher Standard of Care for Patients: follow-up care is facilitated by telemedicine, as it allows doctors to check in with patients remotely to ensure their health and well-being. Better treatment outcomes are achieved through the use of telemedicine, whether through a more comprehensive remote patient monitoring system to check the patient’s heart or through a video chat that can answer queries about medication after hospital discharge.
3.4. Forms of Telemedicine
3.4.1. Asynchronous Telemedicine
3.4.2. Remote Health Monitoring
3.4.3. Synchronous Telemedicine
4. Evolution of Communications Technologies for Telemedicine
4.1. Communication Network Links for Telemedicine
4.1.1. Point-to-Point Links
4.1.2. Point-to-Multipoint Links
4.2. Classification of Communication Technologies in Telemedicine
4.3. Short Range Communication Technologies
4.3.1. Bluetooth Low-Energy (BLE) Communication
- Frequency hopping: BLE uses adaptive frequency hopping (AFH) as a technique for media access. This means that BLE devices are sensitive to other nearby wireless networks and continuously change their channels to mitigate or reduce interference. Data transmission is hardly ever interrupted, as Bluetooth devices can determine which channels are occupied and use the available channels in the hop sequence.
- Number of nodes: Bluetooth devices can have unlimited active slave connections. Older versions of Bluetooth have a maximum of seven slave nodes, making for a maximum number of eight connections when the master is counted. As can be seen in Table 2, Bluetooth 4 and Bluetooth 5 can support unlimited nodes.
- Cost efficiency [100]: BLE is optimised for devices that use small batteries due to the reduction of the number of channels from 79 channels ay 1 MHz to 40 at 2 MHz.
- Low power consumption: BLE has been developed taking into consideration the minimisation of power requirements, especially when comparing newer Bluetooth versions to older ones.
- BLE is easy to integrate into networks.
- It has a relatively more secure connectivity than Wi-Fi connections.
- High power consumption;
- Frequent connection or pairing loss;
- Non-automatic support of network formation.
4.3.2. ZigBee
- Low latency;
- High data security;
- Collision avoidance and retransmission, ensuring more reliable data transmission;
- Support for multiple network topologies, such as point-to-point, star, and mesh topologies;
- Support for unlimited nodes in a network;
- Scalability;
- Low energy consumption;
- Ease of implementation;
- 128-bit AES encryption ensures data security.
4.3.3. Ultra-Wideband (UWB)
- Multi-band (MB) Optical Frequency Division Multiplexing (OFDM) UWB.
- Impulse Radio (IR) UWB.
4.3.4. Wi-Fi (IEEE 802.11)
4.3.5. Radio Frequency Identification (RFID)
- 125–135 KHz (Low Frequency)
- 23.56 MHz (High Frequency)
- 868–930 MHz (Ultra-High Frequency)
- 2.45 GHz (Microwave Frequency)
- 5.8 GHz (Microwave Frequency)
- A reader
- A tag
4.4. Long-Range Communications
4.4.1. Satellite Communication in Telemedicine
4.4.2. Internet-Based Communication in Telemedicine
4.5. Mobile Networks
4.5.1. GSM
4.5.2. 3G/WCDMA/UMTS
4.5.3. 4G/LTE/WiMAX
- Optimizing the allocation of spectrum resources;
- High energy consumption, leading to high CO2 emissions;
- The difficulty of significantly improving spectral efficiency.
4.5.4. 5G
- A high multi-peak data rate of 10Gbps;
- Ultra-low latency;
- Massive network capacity with high bandwidth;
- A very large number of connected devices; this is crucial for the vision of a breakthrough in IoT applications, which 5G can achieve using small cell sizes such as femtocell, picocell, and microcell;
- Availability of six “nines” (), that is, 5G networks should always be available to deliver as much capacity as possible;
- Maximum coverage;
- Low energy consumption;
- High user experience, with 5G expected to be user-centric rather than operator-centric.
4.5.5. Small Cells
- Scalability of devices in cases where there are many connected devices, meaning that device gateways and protocols need to be carefully designed;
- IoT connectivity;
- Resource optimisation;
- Interoperability;
- Energy requirements of connected devices;
- Data privacy, security, and trust;
- Enormous data computation.
5. Use Cases
5.1. Emergency Telemedicine
5.2. Follow-Up Telemedicine
5.3. Avionics-Associated System
6. Types of Information Transmitted
6.1. Video Conferencing
6.2. Transmission of Medical Images
6.3. Video Streaming
7. Communication Standards/Protocols in Telemedicine
- ZigBee/IEEE 802.15.4: the ZigBee protocol is used for interfacing with data processing devices such as personal data assistants (PDA) and PCs that are directly connected to medical devices (point-to-point). Because of its simplicity, low power usage, and ability to cover large numbers of devices per network, ZigBee is projected to succeed in setting a leading standard for home control applications, which forms a vital component of telemedicine applications [60]. In [49], a ZigBee module was used to connect ECG data to a PC through a Universal Asynchronous Receiver–Transmitter (UART) connected to a USB transceiver device. Although the system supports only point-to-point connection, the end terminal can be any PC with a USB port and an operating system equipped with a USB-to-UART driver.
- Bluetooth/IEEE 802.15.1: Bluetooth is a short-range radio link intended to replace the cables connecting fixed electronic devices. It operates in the unlicensed Industrial Scientific Medicine (ISM) frequency band at 2.4 GHz [82]. A combination of ZigBee and Bluetooth was utilised in [93] to connect four different medical services. The system was interfaced through UART and an analog port, delivering data rates up to 42 kbps. Table 6 shows a comparison between the Bluetooth and Zigbee communication standards.
- WiMAX/IEEE Broadband Wireless Access (BWA) 802.16: according to [128], WiMAX is a communication protocol based on the IEEE 802.16 standard. Developed to provide long distance broadband wireless data connectivity, it serves as an alternative to cable and DSL because of its high bandwidth and provision of BWA for up to 30 miles for fixed stations and 3–10 miles for mobile stations.With respect to telemedicine applications, [38] shows that WiMAX systems for wireless telemedicine provide high mobile connectivity for multimedia traffic with guaranteed QoS, representing advantages over 3G systems, which are designed for more basic data and voice transmission. A number of major communication challenges are addressed by WiMAX standards, including provision of high bandwidth, QoS support, integrated services, and security.
- WiFi/WLAN/IEEE 802.11: WiFi/WLAN is a wireless communication protocol based on the IEEE 802.11 standard. In telemedicine applications, WiFi networks usually comprise multiple access points, with medical sensor nodes moving freely among access points [107].A study by [108] demonstrated a WLAN/IEEE 802.11n standard transmission scheme for wireless telemedicine applications. The WLAN system could transmit measured medical data using digital bits, ECG signals, case histories, and audio/video signals for telemedical purposes. Similarly, medical signal accuracy in WiFi-based telemedicine schemes was presented in [107]. According to the authors, several security threats are associated with WiFi networks due to their use of open an medium to transmit and receive data. Threats which can be detrimental in medical contexts include: denial of service, eavesdropping, and services theft. Another issues is that the WiFi/802.11 protocol is limited to between 30–100 m, which is a disadvantage compared to the WiMAX protocol [128].
- User Datagram Protocol (UDP): protocols for media streaming are usually intended for communication between streaming servers and their users, and handle concerns around transport, session control, and network addressing. UDP is a transport protocol that is widely utilized for data streaming in telemedicine contexts [129]. UDP is the preferred transport protocol for streaming video over fading channels, and can be used in combination with other protocols to further benefit from their advantages. The UDP/IP protocol was utilized in [129]; refs. [130,131] recommend that UDP should be employed for delay-sensitive tasks with tolerance to minor loss of frame traffic, such as video streaming, in preference to TCP. In the work of [92], the UDP protocol was chosen instead of other protocols because of its swiftness and efficiency in real life applications, although [29] mention that video traffic or signals take the lowest priority in the UDP protocol. The UDP protocol uses a simple datagram without congestion control. This issue can be addressed by adopting a rate adjustment measure, as pointed out in [131,132]. While UDP may not be reliable for transmission of packet-based data, it is very good for networked games and streaming media [96].
- Real-Time Protocol (RTP) and Real-Time Transport Control Protocol (RTCP): the RTP and RTCP protocols are internet protocols belonging to the family of transport protocols for media streaming. For real-time applications, the RTP protocol provides an end-to-end transport function. RTCP is often used as a companion control protocol to the RTP protocol, where it helps to improve Quality of Service (QoS) feedback. The authors in [133] used RTP and RTCP protocols in their measurement of the QoS of video streams.
- TCP/IP: another wireless communication protocol utilised in telemedicine is the transmission control protocol (TCP)/internet protocol (IP). Due its low-cost and multiple functions, there has been significant rise in the use of IP-based networks in telemedicine applications [2]. A study by [84] presented an IP-based medical data transmission system that used the TCP/IP protocol to efficiently transmit data over the network, achieving a high bandwidth and low error rate. In their proposed design, data are transmitted between the server and the client in the form of packets using TCP.
8. Research Challenges and Future Directions
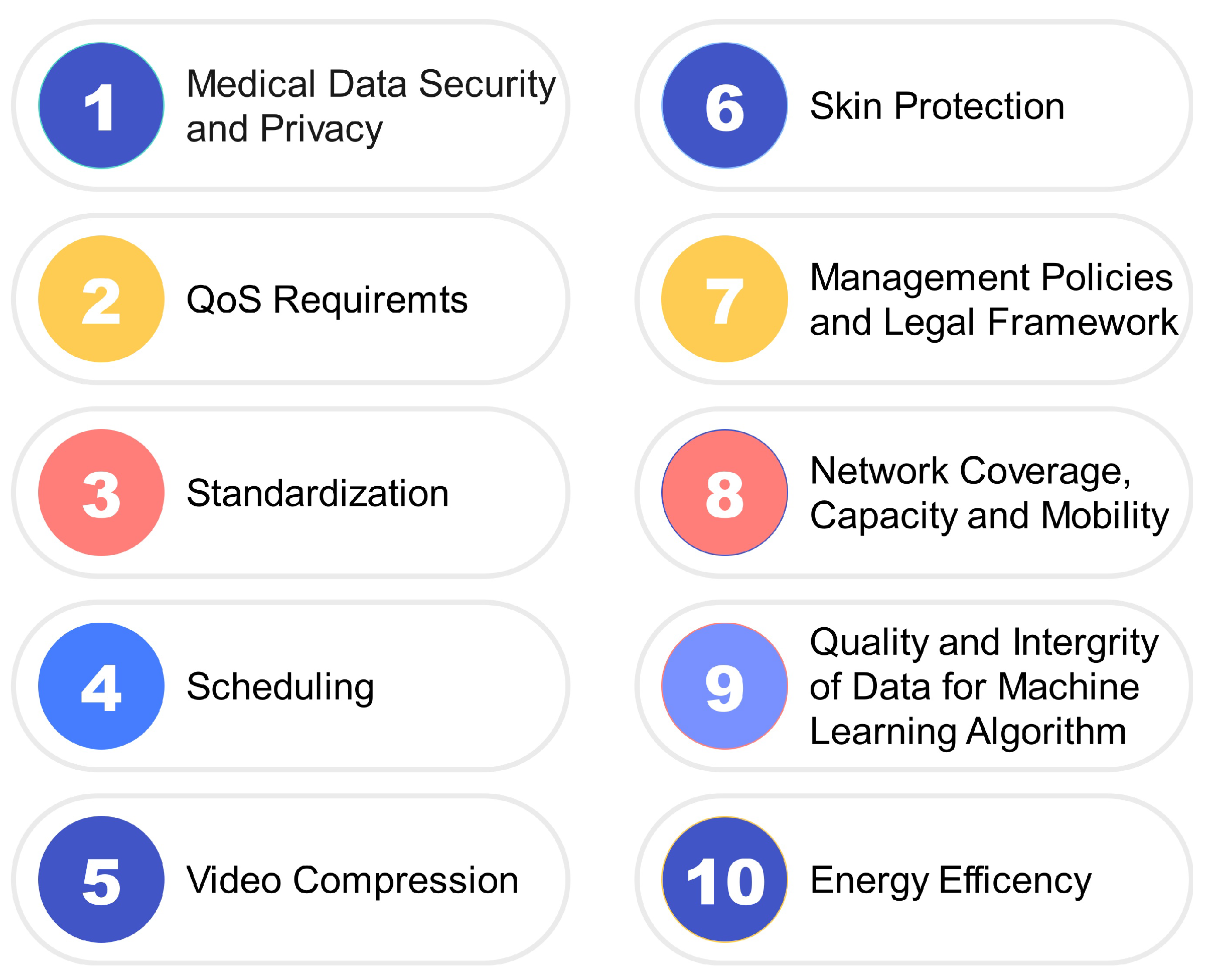
8.1. Classification of Research Challenges in Telemedicine
8.1.1. Medical Data Security and Privacy
8.1.2. QoS Requirements
8.1.3. Standardization
8.1.4. Scheduling
8.1.5. Video Compression
8.1.6. Skin Protection
8.1.7. Cost of Deployment and Legal Framework
8.1.8. Network Coverage, Capacity and Mobility
8.1.9. Quality and Integrity of Data for ML Algorithms
8.1.10. Energy Efficiency
8.2. Future Directions
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Moore, M. The Evolution of Telemedicine. Future Gener. Comput. Syst. 1999, 15, 245–254. [Google Scholar] [CrossRef]
- Pandian, P.S.; Safeer, K.P.; Shakunthala, D.T.I.; Gopal, P.; Padaki, V.C. Store and Forward Applications in Telemedicine for Wireless IP Based Networks. J. Netw. 2007, 2, 58–65. [Google Scholar] [CrossRef]
- Devaraj, S.J.; Ezra, K. Current Trends and Future Challenges in Wireless Telemedicine System. In Proceedings of the 2011 3rd International Conference on Electronics Computer Technology, Kanyakumari, India, 8–10 April 2011; IEEE: Piscataway, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Chakraborty, C.; Gupta, B.; Ghosh, S.K. A Review on Telemedicine-Based WBAN Framework for Patient Monitoring. Telemed. e-Health 2013, 19, 619–626. [Google Scholar] [CrossRef]
- Alenoghena, C.O.; Onumanyi, A.J.; Ohize, H.O.O.; Adejo, A.O.; Oligbi, M.; Ali, S.; Okoh, S.A. eHealth: A Survey of Architectures, Developments in mHealth, Security Concerns and Solutions. Int. J. Environ. Res. Public Health 2022, 19, 13071. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.; Crowley, T.; Keena, B.; Donoghue, S.; McManus, M.; Zackai, E. The experience of one pediatric geneticist with telemedicine-based clinical diagnosis. Am. J. Med. Genet. 2023, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.G.; Watts, I.; Beales, E.; Maudhoo, A.; Hayward, J.; Sheridan, E.; Rafi, I. Videoconferencing to deliver genetics services: A systematic review of telegenetics in light of the COVID-19 pandemic. Am. J. Med. Genet. 2021, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.; Brancolini, S.; Eshraghi, Y.; Guirguis, M.; Durbhakula, S.; Provenzano, D.; Vorenkamp, K.; Shah, S.; Darden, M.; Kohan, L. Telemedicine Implementation in Pain Medicine: A Survey Evaluation of Pain Medicine Practices in Spring. Pain Physician 2022, 25, 387–390. [Google Scholar] [PubMed]
- Der-martirosian, C.; Shin, M.; Upham, M.L.; Douglas, J.H.; Zeliadt, S.B.; Taylor, S.L. Telehealth Complementary and Integrative Health Therapies During COVID-19 at the U.S. Department of Veterans Affairs. Telemed. e-Health 2022, 1–8. [Google Scholar] [CrossRef]
- Everard, K.M.; Schiel, K.A.; Xu, E.; Kulshreshtha, A. Use of Telemedicine in the Family Medicine Clerkship: A CERA Study. PRiMER 2022, 6, 25. [Google Scholar] [CrossRef]
- Muschol, J.; Heinrich, M.; Heiss, C.; Knapp, G.; Repp, H.; Schneider, H.; Thormann, U.; Uhlar, J.; Unzeitig, K.; Gissel, C. Assessing Telemedicine Efficiency in German Follow-up Care With Video Consultations for Patients in Orthopedic and Trauma Surgery: A Randomized Controlled Trial. J. Med. Internet Res. 2022, 24. [Google Scholar] [CrossRef]
- Yamin, M.A.Y.; Alyoubi, B.A. Adoption of telemedicine applications among Saudi citizens during COVID-19 pandemic: An alternative health delivery system. J. Infect. Public Health 2020, 13, 1845–1855. [Google Scholar] [CrossRef]
- Giansanti, D.; Morone, G.; Loreti, A.; Germanotta, M.; Aprile, I. A Narrative Review of the Launch and the Deployment of Telemedicine in Italy during the COVID-19 Pandemic. Healthcare 2022, 10, 415. [Google Scholar] [CrossRef]
- Bembinov, M.; Soenardi, N. An assessment of client and clinician satisfaction in veterinary teleconsultation compared to in-person consultations. Vet. Evid. 2023, 7, 1–17. [Google Scholar] [CrossRef]
- Arain, S.; Al, M.; Shabeer, S.; Thorakkattil, A.; Iqbal, S.; Fuad, M.; Ghamdi, A. Implementation of Pharmacist-led Telepsychiatry Services: Challenges and Opportunities in the Midst of COVID-19. J. Technol. Behav. Sci. 2022. [Google Scholar] [CrossRef]
- Khaddar, M.A.E.; Harroud, H.; Boulmalf, M.; Elkoutbi, M.; Habbani, A. Emerging Wireless Technologies in e-health Trends, Challenges, and Framework Design Issues. In Proceedings of the 2012 International Conference on Multimedia Computing and Systems, Tangiers, Morocco, 10–12 May 2012; IEEE: Piscataway, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Laxminarayan, S.; Istepanian, R. UNWIRED E-MED: The Next Generation of Wireless and Internet Telemedicine Systems. IEEE Trans. Inf. Technol. Biomed. 2000, 4, 189–193. [Google Scholar] [CrossRef]
- Pattichis, C.; Kyriacou, E.; Voskarides, S.; Pattichis, M.; Istepanian, R.; Schizas, C. Wireless Telemedicine Systems: An Overview. IEEE Antennas Propag. Mag. 2002, 44, 143–153. [Google Scholar] [CrossRef]
- Albahri, A.S.; Alwan, J.K.; Taha, Z.K.; Ismail, S.F.; Hamid, R.A.; Zaidan, A.; Albahri, O.S.; Zaidan, B.; Alamoodi, A.H.; Alsalem, M. Iot-based Telemedicine for Disease Prevention and Health Promotion: State-of-the-Art. J. Netw. Comput. Appl. 2021, 173, 102873. [Google Scholar] [CrossRef]
- Amuomo, N.O. The Evolution of GSM Technologies into 5G and the Imminent Emergence of Transformative Telemedicine Applications: A Review. East Afr. J. Inf. Technol. 2020, 2, 8–17. [Google Scholar] [CrossRef]
- Haddara, M.; Staaby, A. RFID Applications and Adoptions in Healthcare: A Review on Patient Safety. Procedia Comput. Sci. 2018, 138, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Tachakra, S.; Wang, X.; Istepanian, R.S.; Song, Y. Mobile e-Health: The Unwired Evolution of Telemedicine. Telemed. J. e-Health 2003, 9, 247–257. [Google Scholar] [CrossRef]
- Suksmono, A.B.; Sastrokusumo, U.; Mengko, T.L.R.; Pramudito, J.T.; Oktowaty, S. Overview of Telemedicine Activities in Indonesia: Progress and Constraints. In Proceedings of the 6th International Workshop on Enterprise Networking and Computing in Healthcare Industry-Healthcom 2004 (IEEE Cat. No. 04EX842), Odawara, Japan, 29 June 2004; IEEE: Piscataway, NJ, USA, 2004; pp. 37–40. [Google Scholar]
- Ferrante, F.E. Evolving Telemedicine/eHealth Technology. Telemed. e-Health 2005, 11, 370–383. [Google Scholar] [CrossRef]
- Raskovic, D.; Milenkovic, A.; Groen, P.C.D.; Jovanov, E. FromTelemedicine to Ubiquitous M-health: The Evolution of e-health Systems. In Biomedical Information Technology; Elsevier: Amsterdam, The Netherlands, 2008; pp. 479–496. [Google Scholar]
- Rashvand, H.; Salcedo, V.T.; Sánchez, E.M.; Iliescu, D. Ubiquitous Wireless Telemedicine. IET Commun. 2008, 2, 237. [Google Scholar] [CrossRef]
- Cova, G.; Xiong, H.; Gao, Q.; Guerrero, E.; Ricardo, R.; Estevez, J. A Perspective of State-of-the-Art Wireless Technologies for e-health Applications. In Proceedings of the 2009 IEEE International Symposium on IT in Medicine & Education, Jinan, China, 14–16 August 2009; IEEE: Piscataway, NJ, USA, 2009. [Google Scholar] [CrossRef]
- Panayides, A.; Pattichis, M.; Pattichis, C.S.; Schizas, C.N.; Spanias, A.; Kyriacou, E. An Overview of Recent End-to-End Wireless Medical Video Telemedicine Systems Using 3G. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Piscataway, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Wang, Z.; Gu, H. A Review of Telemedicine in China. J. Telemed. Telecare 2009, 15, 23–27. [Google Scholar] [CrossRef]
- Zubiete, E.D.; Luque, L.F.; Rodriguez, A.V.M.; Gonzalez, I.G. Review of Wireless Sensors Networks in Health Applications. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; IEEE: Piscataway, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Lin, C.F.; Hung, S.I.; Chiang, I.H. An 802.11n Wireless Local Area Network Transmission Scheme for Wireless Telemedicine Applications. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2010, 224, 1201–1208. [Google Scholar] [CrossRef]
- Clifford, G.D.; Clifton, D. Wireless Technology in Disease Management and Medicine. Annu. Rev. Med. 2012, 63, 479–492. [Google Scholar] [CrossRef]
- Kayange, D.S.; Massawe, E.A. The Potential for a Tanzania Wireless Telemedicine Network: An Overview. Res. J. Eng. Appl. Sci. 2013, 2, 171–175. [Google Scholar]
- Mahfouz, M.R.; Kuhn, M.J.; To, G. Wireless Medical Devices: A Review of Current Research and Commercial Systems. In Proceedings of the 2013 IEEE Topical Conference on Biomedical Wireless Technologies, Networks, and Sensing Systems, Austin, TX, USA, 20–23 January 2013; IEEE: Piscataway, NJ, USA, 2013. [Google Scholar] [CrossRef]
- Ahmad, N.; Riaz, N.; Hussain, M. Ad hoc Wireless SensorNnetwork Architecture for Disaster Survivor Detection. Int. J. Adv. Sci. Technol. 2011, 34, 16. [Google Scholar]
- Algaet, M.A.; Noh, Z.A.B.M.; Shibghatullah, A.S.; Milad, A.A.; Mustapha, A. Provisioning Quality of Service of Wireless Telemedicine for E-Health Services: A Review. Wirel. Pers. Commun. 2014, 78, 375–406. [Google Scholar] [CrossRef]
- de la Torre Díez, I.; Alonso, S.G.; Hamrioui, S.; López-Coronado, M.; Cruz, E.M. Systematic Review about QoS and QoE in Telemedicine and eHealth Services and Applications. J. Med. Syst. 2018, 42, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rani, B.K.S.; Bhat, S.; Mukhopadhyay, A. A Survey of Wireless Technologies and Vertical Handoff Techniques from the Perspective of Telemedicine Scenarios. In Proceedings of the 2017 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 6–8 April 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Lukas, H.; Xu, C.; Yu, Y.; Gao, W. Emerging Telemedicine Tools for Remote COVID-19 Diagnosis, Monitoring, and Management. ACS Nano 2020, 14, 16180–16193. [Google Scholar] [CrossRef]
- Nawaz, N.A.; Abid, A.; Rasheed, S.; Farooq, M.S.; Shahzadi, A. Impact of telecommunication network on future of telemedicine in healthcare: A systematic literature review. Int. J. Adv. Appl. Sci. 2022, 9, 122–138. [Google Scholar] [CrossRef]
- Chatterjee, S.; Khan, A.M.; Rani, P.; Jayesh, S. A systematic review on tele dentistry in public oral health during COVID-19. NeuroQuantology 2022, 20, 1107–1117. [Google Scholar] [CrossRef]
- Woodward, B.; Rasid, M. Wireless Telemedicine: The Next Step. In Proceedings of the 4th International IEEE EMBS Special Topic Conference on Information Technology Applications in Biomedicine, Birmingham, UK, 24–26 April 2003. [Google Scholar] [CrossRef]
- Pandian, P.S. An Overview of Telemedicine Technologies for Healthcare Applications. Int. J. Biomed. Clin. Eng. 2016, 5, 29–52. [Google Scholar] [CrossRef]
- Craft, R.L.; Funkhouser, D.R.; Gallagher, L.K.; Garcia, R.J.; Parks, R.C.; Warren, S. High-Surety Telemedicine in a Distributed, ‘Plug-and-Play’ Environment; Technical Report; Sandia National Laboratories (SNL): Albuquerque, NM, USA, 1999.
- Portnoy, J.M.; Pandya, A.; Waller, M.; Elliott, T. Telemedicine and emerging technologies for health care in allergy/immunology. J. Allergy Clin. Immunol. 2020, 145, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Hur, J.; Chang, M.C. Usefulness of an Online Preliminary Questionnaire under the COVID-19 Pandemic. Nat. Public Health Emerg. Collect. 2020, 44, 116. [Google Scholar] [CrossRef]
- Khoor, S.; Nieberl, K.; Fugedi, K.; Kail, E. Telemedicine ECG-Telemetry with Bluetooth Technology. In Proceedings of the Computers in Cardiology 2001. Vol.28 (Cat. No.01CH37287), Rotterdam, The Netherlands, 23–26 September 2001; pp. 585–588. [Google Scholar] [CrossRef]
- Orlov, O.I.; Drozdov, D.V.; Doarn, C.R.; Merrell, R.C. Wireless ECG monitoring by telephone. Telemed. J. e-Health 2001, 7, 33–38. [Google Scholar] [CrossRef]
- Auteri, V.; Roffia, L.; Cinotti, T.S. ZigBee-Based Wireless ECG Monitor. In Proceedings of the 2007 Computers in Cardiology, Durham, NC, USA, 30 September–3 October 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar] [CrossRef]
- Aboalseoud, A.; Youssry, A.; El-Nozahi, M.; El-Rafei, A.; Elbialy, A.; Ragaai, H.; Wahba, A. Wireless ECG Monitoring System for Telemedicine Application. In Proceedings of the 2019 IEEE 9th International Conference on Intelligent Computing and Information Systems, ICICIS 2019, Cairo, Egypt, 8–10 December 2019; pp. 300–305. [Google Scholar] [CrossRef]
- Lin, J.L.; Liu, H.C.; Tai, Y.T.; Wu, H.H.; Hsu, S.J.; Jaw, F.S.; Chen, Y.Y. The development of wireless sensor network for ECG monitoring. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 3513–3516. [Google Scholar] [CrossRef]
- D’Souza, M.; Ros, M.; Postula, A. Wireless medical information system network for patient ECG monitoring. In Proceedings of the 9th EUROMICRO Conference on Digital System Design: Architectures, Methods and Tools, DSD 2006, Cavtat, Croatia, 30 August–1 September 2006; pp. 617–624. [Google Scholar] [CrossRef]
- Jimeno, M.; De la Hoz, Y.; Wilches, J. Wireless ECG and PCG Portable Telemedicine Kit for Rural Areas of Colombia. Investig. Innovación en Ing. 2014, 2, 1–9. [Google Scholar] [CrossRef]
- Nopparat, V.; Keeratiwintakorn, P. The three-lead wireless ECG in sensor networks for mobile patients. In Proceedings of the 2008 SICE Annual Conference, Chofu, Japan, 20–22 August 2008; pp. 2308–2311. [Google Scholar] [CrossRef]
- Rashkovska, A.; Tomašić, I.; Trobec, R. A Telemedicine application: ECG data from wireless body sensors on a Smartphone. In Proceedings of the 2011 Proceedings of the 34th International Convention MIPRO, Opatija, Croatia, 23–27 May 2011; pp. 262–265. [Google Scholar]
- Zhang, Z.; Jung, T.P.; Makeig, S.; Rao, B.D. Compressed sensing for energy-efficient wireless telemonitoring of noninvasive fetal ECG via block sparse bayesian learning. IEEE Trans. Biomed. Eng. 2013, 60, 300–309. [Google Scholar] [CrossRef]
- Abdulbaqi, A.S.; Najim, S.A.M.; Mohammed, F.M.; Masunda, T.; Panessai, I.Y. Wireless EEG transmission and evaluation based on iCloud efficiency: Age of telemedicine. J. Eng. Sci. Technol. 2021, 16, 2416–2425. [Google Scholar]
- Kannampallil, T.; Ma, J. Digital Translucence: Adapting Telemedicine Delivery Post-COVID-19. Telemed. e-Health 2020, 26, 1120–1122. [Google Scholar] [CrossRef]
- Hu, X.; Wang, J.; Yu, Q.; Liu, W.; Qin, J. A wireless sensor network based on ZigBee for telemedicine monitoring system. In Proceedings of the 2nd International Conference on Bioinformatics and Biomedical Engineering, iCBBE 2008, Shanghai, China, 16–18 May 2008; pp. 1367–1370. [Google Scholar] [CrossRef]
- Sîrbu, A.N.; Maiorescu, V.A.V.D.; Cleju, I.I. A Zigbee Solution for Telemedicine Applications. ACTA Tech. Napoc. Electron. Telecommun. 2008, 49, 35–39. [Google Scholar]
- Supriyanto, E.; Satria, H.; Mulyadi, I.H.; Putra, E.H. A Novel Low Cost Telemedicine System Using Wireless Mesh Network. In Proceedings of the 3rd SEATUC Symposium, Johor Bahru, Malaysia, 25–26 February 2009; pp. 382–402. [Google Scholar]
- Oh, S.; Kwon, H.; Varadan, V.K. Wireless telemedicine systems for diagnosing sleep disorders with Zigbee star network topology. Nanosyst. Eng. Med. 2012, 8548, 85482L. [Google Scholar] [CrossRef]
- Wang, X. Wireless mesh networks. J. Telemed. Telecare 2008, 14, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Wang, M. A Wireless PDA-based Electrocardiogram Transmission System for Telemedicine. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 1–4 September 2005; Volume 7, pp. 3807–3809. [Google Scholar] [CrossRef]
- Wang, D.; Lu, Y.; Zhang, H.; Zhang, J.; Han, Y. Body Piconet for the Telemedicine System Based on Home Networks. In Proceedings of the 2007 IEEE/ICME International Conference on Complex Medical Engineering, Beijing, China, 23–27 May 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 1202–1205. [Google Scholar]
- Lin, C.F.; Chung, C.H.; Chen, Z.L.; Song, C.J.; Wang, Z.X. A chaos-based unequal encryption mechanism in wireless telemedicine with error decryption. WSEAS Trans. Syst. 2008, 7, 49–55. [Google Scholar]
- Kugean, C.; Krishnan, S.M.; Chutatape, O.; Swaminathan, S.; Srinivasan, N.; Wang, P. Design of a mobile telemedicine system with wireless LAN. In Proceedings of the Asia-Pacific Conference on Circuits and Systems, Denpasar, Indonesia, 28–31 October 2002; Volume 1, pp. 313–316. [Google Scholar] [CrossRef]
- Moshayedi, A.J.; Kolahdooz, A.; Roy, A.S.; Rostami, S.A.L.; Xie, X. Design and promotion of cost-effective IOT-based heart rate monitoring. In Proceedings of the International Conference on Cloud Computing, Internet of Things, and Computer Applications (CICA 2022), Luoyang, China, 22–24 April 2022; Powell, W., Tolba, A., Eds.; International Society for Optics and Photonics: Bellingham, WA, USA, 2022; Volume 12303, pp. 405–410. [Google Scholar] [CrossRef]
- Thrall, J.H.; Boland, G. Teleradiology. In PACS: A Guide to the Digital Revolution; Dreyer, K.J., Mehta, A., Thrall, J.H., Eds.; Springer: New York, NY, USA, 2002; pp. 315–348. [Google Scholar] [CrossRef]
- Latifi, R.; Doarn, C.R.; Merrell, R.C. Telemedicine, Telehealth and Telepresence; Springer International Publishing: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Lin, Y.H.; Jan, I.C.; Ko, P.I.; Chen, Y.Y.; Wong, J.M.; Jan, G.J. A Wireless PDA-BasedPhysiological Monitoring System for Patient Transport. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 439–447. [Google Scholar]
- Takahashi, M. Contribution of teleradiology in Japanese medicine. Int. J. Comput. Assist. Radiol. Surg. 2006, 1, 455–456. [Google Scholar] [CrossRef]
- Committee for a Responsible Budget. American Health Care: Health Spending and the Federal Budget. Available online: https://jamanetwork.com/journals/jama/fullarticle/2594716/ (accessed on 12 December 2022).
- Abo-Zahhad, M.; Ahmed, S.M.; Elnahas, O. A Wireless Emergency Telemedicine System for Patients Monitoring and Diagnosis. Int. J. Telemed. Appl. 2014, 2014, 380787. [Google Scholar] [CrossRef]
- Hung, K.; Zhang, Y. Usage of Bluetooth/sup TM/in Wireless Sensors for Tele-Healthcare. In Proceedings of the Second Joint 24th Annual Conference and the Annual Fall Meeting of the Biomedical Engineering Society Engineering in Medicine and Biology, Houston, TX, USA, 23–26 October 2002; IEEE: Piscataway, NJ, USA, 2002; Volume 3, pp. 1881–1882. [Google Scholar]
- Yew, H.T.; Kheau, C.; Chin, R.; Chekima, A.; Satria, M.H. Improved-TOPSIS Based Handover Scheme for Telemedicine Service Using Heterogeneous Wireless Networks. In Proceedings of the 2017 IEEE 2nd International Conference on Automatic Control and Intelligent Systems (I2CACIS), Kota Kinabalu, Malaysia, 21 October 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 155–160. [Google Scholar]
- Sukanesh, R.; Rajan, S.P.; Vijayprasath, S.; Aishwarya, N.; Angela, P.G. Intelligent Wireless Mobile Patient Monitoring System. In Proceedings of the 2010 International Conference On Communication Control and Computing Technologies, Nagercoil, India, 7–9 October 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 540–543. [Google Scholar]
- Choi, Y.B.; Krause, J.S.; Seo, H.; Capitan, K.E.; Chung, K. Telemedicine in the USA: Standardization Through Information Management and Technical Applications. IEEE Commun. Mag. 2006, 44, 41–48. [Google Scholar] [CrossRef]
- Yu, X.; Xia, X.; Chen, X. Design and Application of RuBee-Based Telemedicine Data Acquisition System. In Proceedings of the 2011 10th IEEE/ACIS International Conference on Computer and Information Science, Sanya, China, 16–18 May 2011; IEEE: Piscataway, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Saravanan, S.; Sudhakar, P. Telemedicine Technology Using Internet Communication. Int. J. Pure Appl. Math. 2017, 115, 147–156. [Google Scholar]
- Celik, N.; Baker, J.; Youn, H.; Iskander, M.F. An Internet Based Interactive Telemedicine System for Remote Healthcare. In Proceedings of the 2010 IEEE Antennas and Propagation Society International Symposium, Toronto, ON, Canada, 11–17 July 2010; IEEE: Piscataway, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Wang, D.; Lu, Y.; Zhang, H.; Shuliang, C.; Han, Y. A Wireless Sensor Network Based on Bluetooth for Telemedicine Monitoring System. In Proceedings of the 2005 IEEE International Symposium on Microwave, Antenna, Propagation and EMC Technologies for Wireless Communications, Beijing, China, 8–12 August 2005; IEEE: Piscataway, NJ, USA, 2005; Volume 2, pp. 1361–1364. [Google Scholar] [CrossRef]
- de Almeida, J.P.L.; Pinto, A.C.; Pereira, J.; Pinto, S.; de Carvalho, M. Implementation of a Wireless Device for Real-Time Telemedical Assistance of Home-Ventilated Amyotrophic Lateral Sclerosis Patients: A Feasibility Study. Telemed. e-Health 2010, 16, 883–888. [Google Scholar] [CrossRef]
- Pandian, P.; Safeer, K.; Shakunthala, D.; Gopal, P.; Padaki, V. Internet Protocol Based Store and Forward Wireless Telemedicine System for VSAT and Wireless Local Area Network. In Proceedings of the 2007 International Conference on Signal Processing, Communications and Networking, Chennai, India, 22–24 February 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar] [CrossRef]
- Pavlopoulos, S.; Kyriacou, E.; Berler, A.; Dembeyiotis, S.; Koutsouris, D. A Novel Emergency Telemedicine System Based on Wireless Communication Technology-AMBULANCE. IEEE Trans. Inf. Technol. Biomed. 1998, 2, 261–267. [Google Scholar] [CrossRef]
- Lin, C.F. An Advance Wireless Multimedia Communication Application: Mobile Telemedicine. WSEAS Trans. Commun. 2010, 9, 206–215. [Google Scholar]
- Serener, A.; Kavalcioglu, C. Wireless Telemedicine System in Eemergency Medicine Helicopter. In Proceedings of the 11th WSEAS International Conference on Automatic Control, Modelling and Simulation, Istanbul, Turkey, 30 May–1 June 2009. [Google Scholar]
- Ullah. A Telemedicine Network Model for Health Applications in Pakistan: Current Status and Future Prospects. Int. J. Digit. Content Technol. Its Appl. 2009, 3, 149–155. [Google Scholar] [CrossRef]
- Afonso, J.A.; Maio, A.J.F.; Simoes, R. Performance Evaluation of Bluetooth Low Energy for High Data Rate Body Area Networks. Wirel. Pers. Commun. 2016, 90, 121–141. [Google Scholar] [CrossRef]
- Xu, C.; Yang, Y.; Gao, W. Skin-Interfaced Sensors in Digital Medicine: From Materials to Applications. Matter 2020, 2, 1414–1445. [Google Scholar] [CrossRef]
- Krco, S.; Delic, V. Personal wireless sensor network for mobile health care monitoring. In Proceedings of the 6th International Conference on Telecommunications in Modern Satellite, Cable and Broadcasting Service, Nis, Yugoslavia, 1–3 October 2003; Volume 2, pp. 471–474. [Google Scholar] [CrossRef]
- Tarín, C.; Traver, L.; Cardona, N. Wireless Body Area Networks for Telemedicine Applications. Mag. Waves 2009, 1, 124–125. [Google Scholar]
- Mulyadi, I.H.; Supriyanto, E.; Safri, N.M.; Satria, M.H. Wireless Medical Interface Using ZigBee and Bluetooth Technology. In Proceedings of the 2009 Third Asia International Conference on Modelling & Simulation, Bundang, Indonesia, 25–29 May 2009; IEEE: Piscataway, NJ, USA, 2009. [Google Scholar] [CrossRef]
- Salamon, D.; Grigioni, M.; Gianni, M.; Liberti, M.; De Luca, S.; Bei, A.; D’Inzeo, G. Indoor telemedicine in hospital: A PDA-based flexible solution for wireless monitoring and database integration. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 386–389. [Google Scholar] [CrossRef]
- Bai, V.T.; Srivatsa, S.K. Design of wearable cardiac telemedicine system. Int. J. Electron. Healthc. 2007, 3, 303. [Google Scholar] [CrossRef]
- Berggren, M. Wireless Communication in Telemedicine Using Bluetooth and IEEE 802.11b; Technology Report; Department of Information Technology Uppsala University: Uppsala, Sweden, 2001. [Google Scholar]
- Collotta, M.; Pau, G.; Talty, T.; Tonguz, O.K. Bluetooth 5: A Concrete Step Forward toward the IoT. IEEE Commun. Mag. 2018, 56, 125–131. [Google Scholar] [CrossRef]
- Yu, B.; Xu, L.; Li, Y. Bluetooth Low Energy (BLE) based mobile electrocardiogram monitoring system. In Proceedings of the 2012 IEEE International Conference on Information and Automation, Shenyang, China, 6–8 June 2012; pp. 763–767. [Google Scholar] [CrossRef]
- Donati, M.; Celli, A.; Ruiu, A.; Saponara, S.; Fanucci, L. A Telemedicine Service System Exploiting BT/BLE Wireless Sensors for Remote Management of Chronic Patients. Technologies 2019, 7, 13. [Google Scholar] [CrossRef]
- Pramanik, P.K.D.; Nayyar, A.; Pareek, G. WBAN: Driving e-healthcare Beyond Telemedicine to Remote Health Monitoring: Architecture and Protocols; Elsevier Inc.: Amsterdam, The Netherlands, 2019; pp. 89–119. [Google Scholar] [CrossRef]
- ImtiazBinHamid, N.; Twarik Harouna, M.; Salele, N.; Muhammad, R. Comparative Analysis of Various Wireless Multimedia Sensor Networks for Telemedicine. Int. J. Comput. Appl. 2013, 73, 39–44. [Google Scholar] [CrossRef]
- Camilo, T.; Oscar, R.; Carlos, L. Biomedical signal monitoring using wireless sensor networks. In Proceedings of the 2009 IEEE Latin-American Conference on Communications, Medellin, Colombia, 10–11 September 2009; pp. 1–6. [Google Scholar] [CrossRef]
- Yadav, A.; Singh, V.K.; Bhoi, A.K.; Marques, G.; Garcia-Zapirain, B.; Díez, I.d.l.T. Wireless body area networks: UWB wearable textile antenna for telemedicine and mobile health systems. Micromachines 2020, 11, 558. [Google Scholar] [CrossRef]
- Lin, C.F.; Ching, Y.L. A DS UWB transmission system for wireless telemedicine. WSEAS Trans. Syst. 2008, 7, 578–588. [Google Scholar]
- Taparugssanagorn, A.; Pomalaza-Ráez, C.; Isola, A.; Tesi, R.; Hämäläinen, M.; Iinatti, J. UWB channel modelling for wireless body area networks in a hospital. Int. J. Ultra Wideband Commun. Syst. 2010, 1, 226–236. [Google Scholar] [CrossRef]
- Lin, C.F.; Lee, H.W. Wireless Multimedia Communication toward Mobile Telemedicine. In Proceedings of the AIC ’09: Proceedings of the 9th Wseas International Conference on Applied Informatics and Communications, Moscow, Russia, 20–22 August 2009; pp. 232–237. [Google Scholar]
- Qu, H.; Cheng, J.; Cheng, Q.; Wang, L.Y. WiFi-Based Telemedicine System: Signal Accuracy and Security. In Proceedings of the 2009 International Conference on Computational Science and Engineering, Vancouver, BC, Canada, 29–31 August 2009; IEEE: Piscataway, NJ, USA, 2009. [Google Scholar] [CrossRef]
- Lin, C.F. Mobile Telemedicine: A Survey Study. J. Med. Syst. 2010, 36, 511–520. [Google Scholar] [CrossRef]
- Bisu, A.A.; Gallant, A.; Sun, H.; Brigham, K.; Purvis, A. Telemedicine via Satellite: Improving Access to Healthcare for Remote Rural Communities in Africa. In Proceedings of the 2018 IEEE Region 10 Humanitarian Technology Conference (R10-HTC), Malambe, Sri Lanka, 6–8 December 2018. [Google Scholar] [CrossRef]
- Zhao, Y.; Yagi, Y.; Juzoji, H.; Nakajima, I. A Study of Wireless IP for Telemedicine. In Proceedings of the Fourth International Symposium on Multimediam Communications (WPWC’01), Alborg, Denmark, 3–7 September 2001; Volume 3. [Google Scholar]
- Yamauchi, K.; Chen, W.; Wei, D. 3G Mobile Phone aAplications in Telemedicine—A Survey. In Proceedings of the Fifth International Conference on Computer and Information Technology (CIT’05), Shanghai, China, 21–23 September 2005; IEEE: Piscataway, NJ, USA, 2005. [Google Scholar] [CrossRef]
- Yousef, J.; Lars, A. Validation of a Real-Time Wireless Telemedicine System, Using Bluetooth Protocol and a Mobile Phone, for Remote Monitoring Patient in Medical Practice. Eur. J. Med. Res. 2005, 10, 254–262. [Google Scholar]
- Adarsh, A.; Pathak, S.; Kumar, B. Design and Analysis of a Reliable, Prioritized and Cognitive Radio-Controlled Telemedicine Network Architecture for Internet of Healthcare Things. Int. J. Comput. Netw. Appl. 2021, 8, 54–66. [Google Scholar] [CrossRef]
- Mehta, H.; Patel, D.; Joshi, B.; Modi, H. 0G to 5G Mobile Technology: A Survey. J. Basic Appl. Eng. Res. 2014, 1, 56–60. [Google Scholar]
- Kayyali, S. Resource Management and Quality of Service Provisioning in 5G Cellular Networks. arXiv 2020, arXiv:2008.09601. [Google Scholar]
- Mukhopadhyay, A.; Hegde, R.R.; Thomas, A.S. Handover Mechanisms in Wireless Heterogeneous Telemedicine Networks. In Proceedings of the 2019 3rd International Conference on Computing Methodologies and Communication (ICCMC), Erode, India, 27–29 March 2019; pp. 938–945. [Google Scholar] [CrossRef]
- Agiwal, M.; Roy, A.; Saxena, N. Next Generation 5GWireless Networks: A Comprehensive Survey. IEEE Commun. Surv. Tutorials 2016, 18, 1617–1655. [Google Scholar] [CrossRef]
- Noohani, M.S.; Magsi, K.U. A Review of 5G Technology: Architecture, Security and wide Applications. Int. Res. J. Eng. Technol. (IRJET) 2020, 7, 3440–3471. [Google Scholar] [CrossRef]
- Husni, E.; Heryadi, Y.; Woon, W.; Arifianto, M.; Viswacheda, D.; Barukang, L. Mobile Ad Hoc Network and Mobile IP for Future Mobile Telemedicine System. In Proceedings of the 2006 IFIP International Conference on Wireless and Optical Communications Networks, Bangalore, India, 11–13 April 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 5–11. [Google Scholar]
- Beck, J.A.; Jensen, J.A.; Putzier, R.F.; Stubert, L.A.; Stuart, K.D.; Mohammed, H.; Kreofsky, B.L.; Boles, K.W.; Colby, C.E.; Fang, J.L. Developing a Newborn Resuscitation Telemedicine Program: A Comparison of Two Technologies. Telemed. e-Health 2018, 24, 481–488. [Google Scholar] [CrossRef]
- Vlissidis, N.; Leonidas, F.; Giovanis, C.; Marinos, D.; Aidinis, K.; Vassilopoulos, C.; Pagiatakis, G.; Schmitt, N.; Pistner, T.; Klaue, J. A sensor monitoring system for telemedicine, safety and security applications. Int. J. Electron. 2017, 104, 297–311. [Google Scholar] [CrossRef]
- Chand, R.D.; Kumar, A.; Kumar, A.; Tiwari, P.; Rajnish, R.; Mishra, S.K. Advanced Communication Technologies for Collaborative Learning in Telemedicine and Tele-care. In Proceedings of the 2019 9th International Conference on Cloud Computing, Data Science & Engineering (Confluence), Noida, India, 10–11 January 2019; pp. 601–605. [Google Scholar] [CrossRef]
- LeRouge, C.; Garfield, M.J.; Hevner, A.R. Quality Attributes in Telemedicine Video Conferencing. In Proceedings of the 35th Annual Hawaii International Conference on System Sciences, Big Island, HI, USA, 10 January 2002; IEEE: Piscataway, NJ, USA, 2002; pp. 2050–2059. [Google Scholar]
- Aziz, J.S.; Hussein, O.A.; Naoom, A. Design of Telemedicine Systems for Rural and Urban Areas in Iraq. ARPN J. Eng. Appl. Sci. 2009, 4, 71. [Google Scholar]
- Bowater, M. The Experience of a Rural General Practitioner Using Videoconferencing for Telemedicine. J. Telemed. Telecare 2001, 7, 24–25. [Google Scholar] [CrossRef]
- Yamamoto, L.G.; Williams, D.R. A Demonstration of Instant Pocket Wireless CT Teleradiology to Facilitate Stat Neurosurgical Consultation and Future Telemedicine Implications. Am. J. Emerg. Med. 2000, 18, 423–426. [Google Scholar] [CrossRef]
- Suliman Munawar, H.; Ali Awan, A.; Khalid, U.; Munawar, S.; Maqsood, A. Revolutionizing Telemedicine by Instilling H.265. Int. J. Image Graph. Signal Process. 2017, 9, 20–27. [Google Scholar] [CrossRef]
- Chorbev, I.; Mihajlov, M. Building a Wireless Telemedicine Network within a WiMax Based Networking Infrastructure. In Proceedings of the 2009 IEEE International Workshop on Multimedia Signal Processing, Rio de Janeiro, Brazil, 5–7 October 2009; IEEE: Piscataway, NJ, USA, 2009. [Google Scholar] [CrossRef]
- Garawi, S.; Istepanian, R.; Abu-Rgheff, M. 3G Wireless Communications for Mobile Robotic Tele-Ultrasonography Systems. IEEE Commun. Mag. 2006, 44, 91–96. [Google Scholar] [CrossRef]
- Niyato, D.; Hossain, E.; Diamond, J. IEEE 802.16/WiMAX-Based Broadband Wireless Access and its Application for Telemedicine/e-Health Services. IEEE Wirel. Commun. 2007, 14, 72–83. [Google Scholar] [CrossRef]
- Chu, Y.; Ganz, A. Mobile Telemedicine Systems Using 3G Wireless Networks. Bus. Brief. US Healthc. Strateg. 2005, 20, 2007. [Google Scholar]
- Chu, Y.; Ganz, A. WISTA: A Wireless Telemedicine System for Disaster Patient Care. Mob. Netw. Appl. 2007, 12, 201–214. [Google Scholar] [CrossRef]
- Pedersen, P.C.; Dickson, B.W.; Chakareski, J. Telemedicine Applications of Mobile Ultrasound. In Proceedings of the 2009 IEEE International Workshop on Multimedia Signal Processing, Rio de Janeiro, Brazil, 5–7 October 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 1–6. [Google Scholar]
- Chenthara, S.; Ahmed, K.; Wang, H.; Whittaker, F. Security and Privacy-Preserving Challenges of e-Health Solutions in Cloud Computing. IEEE Access 2019, 7, 74361–74382. [Google Scholar] [CrossRef]
- Ashu, A.; Sharma, S. Ashu, A.; Sharma, S. A Novel Approach of Telemedicine for Managing Fetal Condition Based on Machine Learning Technology from IoT-Based Wearable Medical Device. In Machine Learning and the Internet of Medical Things in Healthcare; Elsevier: Amsterdam, The Netherlands, 2021; pp. 113–134. [Google Scholar] [CrossRef]
- Yew, H.T.; Supriyanto, E.; Haikal, M.; Hau, Y.W. A Vertical Handover Management for Mobile Telemedicine System Using Heterogeneous Wireless Networks. Int. J. Adv. Comput. Sci. Appl. 2016, 7, 1–9. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | Year | Main Focus | Specific Details |
|---|---|---|---|
| [17] | 2000 | Internet in Telemedicine |
|
| [18] | 2002 | Applications and data transmission in e-health |
|
| [5,22] | 2003, 2022 | Wireless technology and architecture in eHealth |
|
| [23] | 2004 | Communication and challenges in telemedicine |
|
| [24] | 2005 | Applications and design in e-health |
|
| [25] | 2008 | Mobile and wireless systems in telemedicine |
|
| [26] | 2009 | ICT, application and architecture in telemedicine |
|
| [27] | 2009 | Wireless, satellite technology and architecture in eHealth |
|
| [29] | 2009 | Internet in Telemedicine |
|
| [28] | 2010 | Wireless technology and architecture in eHealth |
|
| [3] | 2011 | Wireless Telemedicine |
|
| [30] | 2011 | Wireless sensor in ehealth |
|
| [31] | 2012 | Mobile and Satellite communication in ehealth |
|
| [16] | 2012 | Wireless technology and challenges in eHealth |
|
| [32] | 2012 | Wireless technology and challenges in eHealth |
|
| [4] | 2013 | Body Area Network in telemedicine |
|
| [33] | 2013 | Wireless technology for telemedicine in Tanzania |
|
| [34] | 2013 | Wireless devices and Vital signs in telemedicine |
|
| [36] | 2014 | QoS and architecture in healthcare |
|
| [38] | 2017 | Wireless techniques in telemedicine |
|
| [37] | 2018 | QoS and QoE in ehealth |
|
| [21] | 2018 | RFID in Healthcare |
|
| [39] | 2020 | Telemedicine sensors |
|
| [20] | 2020 | ICT in telecommunication |
|
| [19] | 2021 | IoT-based telemedicine architecture |
|
| [40] | 2022 | Telemedicine telecommunication networks |
|
| [8] | 2022 | Telemedicine in pain medicine |
|
| [13] | 2022 | Telemedicine application in Latin America |
|
| [41] | 2022 | Tele dentistry during the COVID-19 pandemic |
|
| Feature | Bluetooth Classic | Bluetooth 4 | Bluetooth 5 | Zigbee IEEE 802.15.4 | Wi-Fi Halow (IEEE 802.11ah) |
|---|---|---|---|---|---|
| Radio Frequency ( MHz) | 2400–2483.5 | 2400–2483.5 | 2400–2483.5 | 868.3, 902 to 928, 2400 to 2483.5 | 900 |
| Range | ≤100 | ≤100 | ≤200 | ≤150 | ≤1000 |
| Medium Acces Technique | Frequency Hopping | Frequency Hopping | Frequency Hopping | CSMA/CA | Restricted Access Window |
| Nominal Data Rate (Mbps) | 1–3 | 1 | 2 | 0.02–0.25 | 0.15–7.8 |
| Latency (ms) | <100 | <6 | <3 | <4 | ≈1000 |
| Network Topology | Piconet, Scatternet | Star-bus, Mesh | Star-bus, Mesh | Mesh | Star-bus |
| Nodes | 7 | Unlimited | Unlimited | Unlimited | Unlimited |
| Message Size (bytes) | ≤358 | 31 | 255 | 100 | 100 |
| Certification Body | Bluetooth (SIG) | Bluetooth (SIG) | Bluetooth (SIG) | ZigBee Alliance | IEEE |
| Frequency Band | Uplink Frequency (GHz) | Downlink Frequency (GHz) | Services | Example |
|---|---|---|---|---|
| C-Band | 5.925–6.425 | 3.700–4.200 | FSS | Palapa-B Indonesia has 20 C-Band transponders |
| Ku-Band (Telecom) | 14.00 -14.80 | 12.20–12.75 | FSS, BSS and Telecom | Superbird-6 satellite has 23 Ku-Band transponders |
| Ka-Band | 27.00–31.00 | 17.00–21.00 | FSS and BSS | Superbird-6 satellite has 6 Ka-Band transponders |
| Feature | 1G | 2G | 3G | 4G | 5G |
|---|---|---|---|---|---|
| Approximate deployment date | 1970–1980 | 1990–2004 | 2004–2010 | 2010 | 2020 |
| Theoretical data rate (Mbps) | 0.002 | 0.384 | 56 | 1000 | 10,000 |
| Latency (ms) | N/A | 629 | 212 | 60–98 | <1 |
| Technology | Analog cellular | GSM (Digital) | CDMA 2000, WCDMA, UMTS | WiMAX, LTE | |
| Service | Voice telephony | Digital voice, SMS, data packet | High quality audio, video and data | Wearable devices, IoT | Wearable devices with AI capabilities |
| Multiplexing | FDMA | FDMA, TDMA | CDMA | MC-CDMA, OFDMA | OFDMA |
| Switching | Circuit | Circuit, packet | Circuit, Packet | All packet | All packet |
| Types | Cell Radius (Km) | Users |
|---|---|---|
| Femtocell | 0.01–0.1 | 1–30 |
| Picocell | 0.25–1 | 30–100 |
| Microcell | 0.2–2 | 100–2000 |
| Macrocell | 8–30 | More than 2000 |
| Standard/Parameter (Characteristic) | ZigBee/IEEE 802.15.4 | Bluetooth/IEEE802.15.1 |
|---|---|---|
| Wireless/Operating frequency | 2.4 GHz/868 MHz/915 Mhz | 2.4 GHz ISM |
| Data rate | 20 kbps up to 250 kbps | 1000 kbps |
| Typical current consumption (Transmission mode) | 30 mA | 50 mA |
| Battery life | 100–1000 days | 1–7 days |
| Network size/Devices per network | Up to 65,536 nodes | Up to 8 nodes |
| Range | 1 to 100 m | 10 to 100 m |
| Stack size | 4 to 32 KB | 250 KB |
| Application | Monitoring & Control | Cable Replacement |
| Range | 10 to 100 m | 100 m |
| Data rate | 20–250 Kbps | 1 Mbps |
| Power profile | Years | Days |
| Complexity | Simple | Complex |
| Network topology | Adhoc, star, mesh hybrid | Adhoc piconet |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alenoghena, C.O.; Ohize, H.O.; Adejo, A.O.; Onumanyi, A.J.; Ohihoin, E.E.; Balarabe, A.I.; Okoh, S.A.; Kolo, E.; Alenoghena, B. Telemedicine: A Survey of Telecommunication Technologies, Developments, and Challenges. J. Sens. Actuator Netw. 2023, 12, 20. https://doi.org/10.3390/jsan12020020
Alenoghena CO, Ohize HO, Adejo AO, Onumanyi AJ, Ohihoin EE, Balarabe AI, Okoh SA, Kolo E, Alenoghena B. Telemedicine: A Survey of Telecommunication Technologies, Developments, and Challenges. Journal of Sensor and Actuator Networks. 2023; 12(2):20. https://doi.org/10.3390/jsan12020020
Chicago/Turabian StyleAlenoghena, Caroline Omoanatse, Henry Ohiani Ohize, Achonu Oluwole Adejo, Adeiza James Onumanyi, Emmanuel Esebanme Ohihoin, Aliyu Idris Balarabe, Supreme Ayewoh Okoh, Ezra Kolo, and Benjamin Alenoghena. 2023. "Telemedicine: A Survey of Telecommunication Technologies, Developments, and Challenges" Journal of Sensor and Actuator Networks 12, no. 2: 20. https://doi.org/10.3390/jsan12020020
APA StyleAlenoghena, C. O., Ohize, H. O., Adejo, A. O., Onumanyi, A. J., Ohihoin, E. E., Balarabe, A. I., Okoh, S. A., Kolo, E., & Alenoghena, B. (2023). Telemedicine: A Survey of Telecommunication Technologies, Developments, and Challenges. Journal of Sensor and Actuator Networks, 12(2), 20. https://doi.org/10.3390/jsan12020020