Abstract
Coronavirus disease 2019 (COVID-19) has extensively spread worldwide with high mortality. Besides vaccination, the United States Food and Drug Administration approved only one oral medication as a treatment. Medicinal plants with antiviral and immunomodulatory properties could be explored as complementary treatments for COVID-19. Ogbomosho is home to such plants traditionally used to treat infectious diseases in Nigeria, making it relevant in complementary medicine. An ethnobotanical survey of medicinal plants used to treat COVID-19 and related ailments, including cough and flu in Ogbomosho South and North Local Government Areas, Nigeria, was conducted using a semi-structured questionnaire. Information was obtained from 56 participants, consisting of different groups of individuals with native knowledge of medicinal plants, and ethnobotanical indices, including the frequency of citation (FC), relative frequency of citation (RFC), and fidelity level (FL) were computed. Twenty-six medicinal plants (17 families) were used to treat COVID-19, 31 (20 families) for cough, and 29 (19 families) for flu. The most cited plant was Zingiber officinale (FC = 10; RFC = 0.18; FL = 18%) for treating COVID-19, Citrus limon (FC = 13; RFC = 0.23; FL = 23%) for cough, and Zingiber officinale (FC = 9; RFC = 0.16; FL = 16%) for flu. Leaves were the most used plant part for treating COVID-19 and flu, while the bark was the most used for cough. Trees and herbs were the most cited plant growth forms. The herbal remedies were mostly prepared by decoction and infusion and were mainly administered orally. Further research should be conducted on the identified species for the scientific validation of their antiviral and immunomodulatory efficacies and safety for use.
1. Introduction
Upper respiratory tract infections (URTIs) are one of the most common diseases in primary care globally [1]. Mainly caused by viruses, the most commonly occurring symptoms of URTIs are sore throat, nasal congestion, runny nose, cough, headache, etc. Whilst these conditions are not usually fatal, the symptoms may significantly affect human efficiency and quality of life [1]. Some poorly managed URTIs can result in complications, including myocarditis, pneumonia, otitis media, etc., accounting for significant morbidity and mortality globally [2]. In December 2019, a novel virus known as the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), which causes respiratory illness, emerged in Wuhan, China, and has spread to almost all parts of the world [3]. As a result of its massive spread globally, the World Health Organization (WHO) declared the coronavirus disease 2019 (COVID-19) a pandemic on the 11 March 2020 [4,5]. Common symptoms of COVID-19 include headache, fever, fatigue, malaise, and dry cough, while less commonly occurring symptoms include sore throat, nausea, diarrhea, generalized body pain, discoloration of fingers and toes, conjunctivitis, and loss of smell or taste [3,6]. In severe cases, COVID-19 results in life-threatening symptoms such as difficulty in breathing, loss of speech or movement, chest pain, shortness of breath and pressure, typical of acute respiratory distress syndrome (ARDS) [3,7]. The WHO reported 14.9 million deaths linked to the COVID-19 pandemic globally between 1 January 2020 and 31 December 2021 [8].
The Nigerian Federal Ministry of Health confirmed the first national case of COVID-19 in Lagos State on 27 February 2020. Over 256,000 infections have been recorded since the pandemic began while over 3000 COVID-19-related deaths have been reported, making Nigeria one of the 20 countries accounting for over 80% of global mortality resulting from COVID-19 from January 2020 to December 2021 [8].
The increasing spread and mortality resulting from COVID-19 across the globe have led to different interventions, including personal hygiene, quarantine, isolation, and the development of vaccines, to control the spread of the virus [9]. Although an oral medication, Paxlovid, has been developed to treat mild to moderate COVID-19 in vulnerable and severely ill individuals aged 12 and older (weighing at least 40 kg), no other evidence-based oral drugs have been developed to prevent COVID-19 infection. While there may be limited access to Paxlovid in low- and middle-income countries, no evidence-based and cost-saving medications have been adapted for treating or preventing COVID-19 in people living in low-resource countries [10,11]. Besides, no vaccine has been identified to be 100 percent effective against the virus and its emerging variants. Hence, scientists have searched more for safe natural products with antiviral and immunomodulatory activities that can serve as potential prophylactic complementary and/or alternative therapeutics for COVID-19 [12,13].
For ages, medicinal plants have been used by different people worldwide as traditional medical treatments and for the prevention of various ailments, including acute respiratory infections [14]. Medicinal plant use has been recognized in some countries (e.g., Uganda, Ghana, Tanzania, etc.) as the leading primary care medication, and over 80% of people in low and middle-income countries depend directly on it [15,16,17]. Medicinal plants are widely used due to their availability, accessibility, affordability, and perceived safety relative to modern medicine [18]. In many African countries, including Nigeria, herbal medicine is well embraced, as up to 90% of rural dwellers rely on it for their primary health care [16,19]. The efficacy of medicinal plants is attributed to the presence of bioactive compounds that confer several bioactivities with therapeutic properties, such as antiviral, antimicrobial, anti-inflammatory, and immunomodulatory activities, etc. [12].
Since the emergence of COVID-19, the use and demand for some medicinal plants has increased worldwide, particularly those used to treat symptoms (for example, sore throat, flu, and cough) associated with COVID-19 [20]. Ethnobotanical surveys focus on multiplex links between local plants and inhabitants, including cultural beliefs and practices linked to several forms of application [21,22]. These surveys are vital in expressing the importance of plant species, that is, for discovering new therapeutic agents [23]. An ethnobotanical survey of medicinal plants is thus applicable as a vital approach for identifying and selecting plants that can be subjected to further phytochemical and pharmacological screening for developing novel therapeutic agents [24].
In Nigeria, the Yoruba people comprise about 40% of the total population and are largely distributed in the southwestern states (Oyo, Ondo, Osun, Ekiti, Ogun, and Lagos) of Nigeria [25,26]. The southwestern zone of Nigeria is a humid tropical area with rainy and dry seasons; hence, the states in this zone have rich floristic diversity and cultural heritage [25,26]. The major cities and towns in the southwestern states include Ogbomosho, Abeokuta, Ibadan, Ede, Ikire, Osogbo, Ile-Ife, and Lagos [25,26]. The major traditional occupations of the inhabitants of this zone are fishing, pottery, farming, indigenous medical practices, and blacksmithing [25]. The recent study of Ajao et al. [26], which compiled the list of angiosperms in the southwestern zone of Nigeria, identified a total of 493 angiosperm species belonging to 99 families, out of which 418 species are utilized for traditional medicinal purposes. Despite the rich floristic diversity of medicinal species in this zone, studies focusing on the indigenous use and traditional medicinal plant applications are limited [26]. Ogbomosho, one of the major towns in the south-western zone of Nigeria, is endowed with a wide variety of indigenous medicinal plants that local herbalists commonly utilize to treat several ailments, including infectious diseases [27]. The present study aimed to document and provide basic knowledge of medicinal plants used by herb sellers, traditional health practitioners, and other people with indigenous knowledge in the treatment of COVID-19, cough, and flu in Ogbomosho South and North Local Government in Ogbomosho, Oyo State, Nigeria. The ethnobotanical survey of medicinal plants used in the management of COVID-19 in Ogbomosho Local Government Areas of Oyo State, Nigeria, will provide information on the availability, classification, preparation, and therapeutic potential of medicinal plants used in the region for treating COVID-19 and related respiratory ailments, particularly cough and flu.
2. Materials and Methods
2.1. Study Area
The study was conducted between October 2021 and March 2022 in Ogbomosho North and Ogbomosho South Local Government Areas of Oyo State, Nigeria (Figure 1). Ogbomosho lies between latitude 8′08′00″ N and longitude 4′16′00″ E, with an approximate population density of 454,690 [28]. The city is inhabited primarily by the Yoruba ethnic group, and agriculture is the major economy.
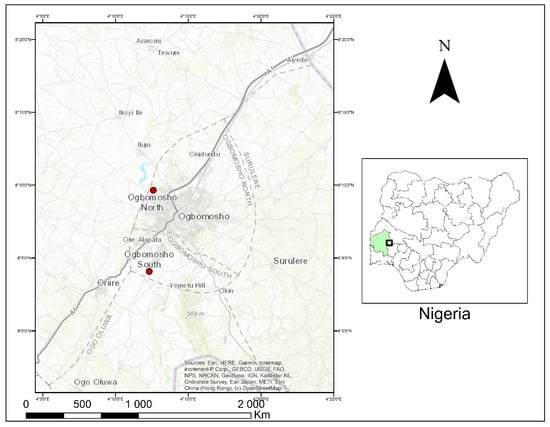
Figure 1.
Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
2.2. Collection of Data
Ethnobotanical information was obtained from participants using a semi-structured questionnaire. The participants were purposively selected, comprising herb sellers, traditional health practitioners, farmers, and individuals with indigenous knowledge. The questionnaire was prepared in English. However, to facilitate efficient communication, informal discussion with herb sellers and traditional health practitioners was done in Yoruba, the local language in these local government areas. A total of 56 participants were interviewed, and the participants were interviewed individually to maintain confidentiality. Data collected included age, gender, occupation, educational background, residence, local names of the plants used in treating COVID-19 and related ailments, plant part used, method of preparation/extraction, and administration method. The study and data collection were done following the regulations made by the International Society of Ethnobiology (available at https://www.ethnobiology.net, accessed on 30 September 2022).
2.3. Collection and Identification of Medicinal Plants
Plant collection was done with the help of herb sellers and traditional health practitioners, using the plants’ local names (in the Yoruba language). The scientific identification of plants was made at IFE herbarium of the Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria (herbarium code IFE, according to Thiers [29]), and voucher specimens were prepared and deposited at the herbarium. In addition, the currently accepted names of all plants identified were verified on “World Flora Online” (www.worldfloraonline.org, accessed on 1 August 2022).
2.4. Data Analysis
Descriptive statistics were carried out on the participants’ demographic information. The data obtained from the documented plants were analyzed using three ethnobotanical indices: frequency of citation (FC), the relative frequency of citation (RFC), and fidelity level (FL).
Following the methods described by Tardio and Pardo-de-santayana [30], RFC was calculated as:
where FC = Frequency of citation/mention, and N = number of participants in the survey.
RCF = FC/N
Fidelity level was calculated as described by Friedman et al. [31]:
where Ip = Number of respondents that mentioned a particular plant species used to treat an ailment being considered, and
FL = (Ip/Iu) × 100
Iu = Total number of respondents in the survey.
2.5. Ethical Approval
The study was approved by the Committee of Ethics of the Forestry Research Institute of Nigeria, Ibadan, Nigeria, with the ethical approval number CFGO711FRIN06. Informed consent was obtained from the participants prior to data collection.
3. Results and Discussion
3.1. Demographic Information
The interview started with an assessment of the demographic characteristics of the participants (Table 1). Fifty-six participants in the age range of 20 to 61 with indigenous knowledge of medicinal plants were interviewed. Most participants were female (58.9%). Individuals aged 51 and above accounted for about 55.4% of the participants. There were more individuals with primary education, constituting about 46.4% of the participants, followed by individuals with secondary education (33.9%). Most of the participants (48.2%) were herb sellers. The participants who all lived in rural areas were either Yoruba (96.4%) or Igbo (3.6%). It is known that variations in gender, age, and educational status of participants have an important relationship with ethnomedicinal knowledge [32].

Table 1.
Demographic information of participants (n = 56) in the study area.
The predominance of the female gender in the present study suggests that women have more knowledge of indigenous medicinal plants than their male counterparts in the study area. The current results corroborate the findings of Chukwuma et al. [33], which reported the dominance of female participants with herbal knowledge in an ethnobotanical survey done in Ado-Ekiti, a Southwestern State in Nigeria. Similarly, women were the most involved and informed in the knowledge and utilization of medicinal plants used for preventing and treating COVID-19, for example, in Algeria [32]. Furthermore, the study conducted by Teixidor-Toneu et al. [34] indicated that women have three-fold more knowledge of medicinal plants than men in Morocco. This was attributed to the frequency of cooking by women (since most medicinal plants are widely used in food preparation), women’s specific conditions, and gender-specific culture. In most African countries, rural areas historically collected different native plants’ parts for their diets and family health needs [35].
Generally, the majority (55.4%) of the people with indigenous knowledge in this study were older than age 51. This result is similar to previous reports on the ethnobotanical survey of indigenous medicinal plants in Nigeria [24] and Northern Morocco [36]. The predominance of elderly participants with indigenous knowledge in the present study agrees with previous reports that older people (above age 50) are usually more knowledgeable about the practice of herbal medicine [24]. The results also revealed a gap between the older and younger generations in the knowledge of indigenous plant use in the study area. The erosion of the knowledge of medicinal plant among younger generations has been reported in other parts of the world. For example, in Western and Northwestern Himalaya, the loss of knowledge regarding the use of medicinal plants in the younger generation was reported [37,38]. This valuable knowledge of medicinal plants and their uses erodes in the younger generation is largely due to westernization, higher education level, and habitat destruction of medicinal plants [34,37,38]. Therefore, it is important that indigenous knowledge is documented, preserved, shared with the younger generations, and that plant resources are conserved.
Regarding the level of education, individuals with a tertiary education level constituted the minority (19.64%) of the participants. This result may be attributed to the fact that the practice of traditional medicine or herbalism does not require a degree but is acquired by experience and learning from older generations [36]. Our result is in line with an ethnobotanical survey of local flora used for medicinal purposes conducted in Lagos, Nigeria, which reported that 79% of the participants with indigenous knowledge had only a primary education [39].
3.2. Medicinal Plants Recorded
In total, 26 medicinal plant species belonging to 17 families were used to treat COVID-19, 31 medicinal plants from 20 families were used to treat cough, and 29 plant species belonging to 19 families were used to treat flu (Table 2, Table 3 and Table 4). For COVID-19 treatment, the most represented families in terms of the number of species were Annonaceae, Meliaceae, Rubiaceae, Asteraceae, Zingiberaceae, Rutaceae, and Fabaceae, with 2–3 species in each family. The most representative families for treating cough were the Amaryllidaceae, Poaceae, Zingiberaceae, Anacardiaceae, Rutaceae, Myrtaceae, Fabaceae, and Arecaceae, with 2–3 species per family. For flu-related symptoms, the most representative families were the Annonaceae (three species), followed by Amaryllidaceae, Zingiberaceae, Compositae, Solanaceae, Myrtaceae, and Fabaceae, with two species each (Figure 2). This result is similar to that reported by Benkhaira et al. [36], where Asteraceae and Zingiberaceae were listed as some of the most representative medicinal plant families used for treating and preventing COVID-19 in Northern Morocco. It is also similar to the findings of Lawal et al. [40], where Fabaceae and Poaceae were listed as some of the most represented plant families used for treating coughs in Osun state, Nigeria. The relatively high number of plants and families identified in this study for the treatment of COVID-19, cough, and flu indicates the richness and diversity of the Nigerian flora for various therapeutic purposes. The diverse phytochemicals present in these florae, which are relatively unexplored, can serve as a potential source of drug development for treating different respiratory ailments [41].
Table 2.
Medicinal plants used to treat and prevent COVID-19 in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
Table 3.
Medicinal plants used to treat and prevent cough in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
Table 4.
Medicinal plants used to treat and prevent flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
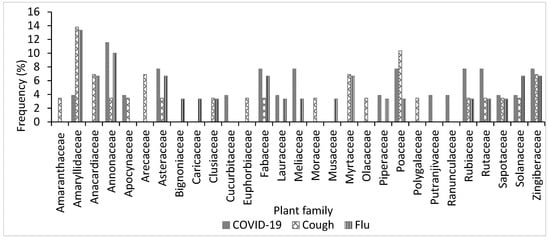
Figure 2.
Frequency of plant families used for treating COVID-19, cough, and flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
3.3. Plant Parts and Growth Forms of Medicinal Plants Used for Treating COVID-19, Cough, and Flu
As participants in the study area reported, diverse plant parts such as bark, bulbs, flower, husk, leaves, rhizomes, and root were used for treating COVID-19, cough, and flu (Figure 3). However, leaves were the most commonly used plant part for treating COVID-19 (39%) and flu (31%), while the bark (20%) was the most commonly used part for treating cough (Figure 3). Several previous studies in Nigeria have also reported that leaves and bark were more utilized in the traditional treatment of different ailments than other plant parts [24,39,40]. The widespread use of leaves for herbal medicine preparation may be attributed to their relatively high abundance, accessibility, and ease of collection [42]. Additionally, the relatively higher photosynthetic and metabolic activities occurring in the aerial parts of most plants (particularly leaves) may have contributed to the build-up of bioactive substances with therapeutic properties [42].
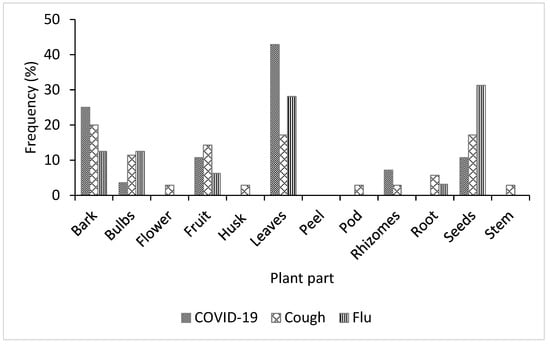
Figure 3.
Frequency of plant parts used for treating COVID-19, cough, and flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
In the study area, the herbal remedies used to treat and prevent COVID-19, cough, and flu were sourced from different growth forms, including trees, shrubs, herbs, grasses, and climbers (Figure 4). However, for the three respiratory infections referenced, a significant number of the medicinal plants were trees (54%, 52%, and 53% for COVID-19, cough, and flu, respectively), followed by herbs (31%, 23%, and 27% for COVID-19, cough, and flu, respectively), and climbers were the lowest growth forms utilized for treating COVID-19, cough, and flu. In terms of sustainability and conservation, harvesting leaves from trees may be more sustainable than other growth forms, given that trees are more resilient due to their sizes [24]. The dominance of woody perennials as sources of herbal remedies may be connected to the rainforest vegetation of the study area. Previous studies [24,43] have reported similar dominance of woody plants in ethnobotanical surveys of plants conducted in the same rainforest zones in Nigeria.
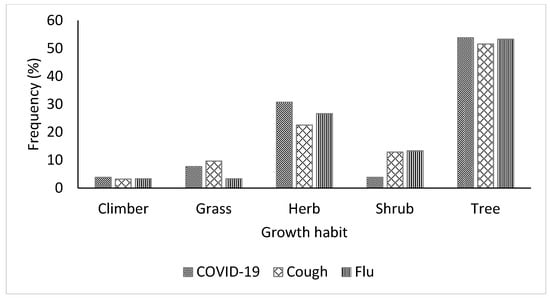
Figure 4.
Growth forms of medicinal plants used for the treatment of COVID-19, cough, and flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
3.4. Method of Preparation and Mode of Administration of Medicinal Plants Species Used for Treating COVID-19, Cough, and Flu
While the participants in the study area identified 10 methods used for preparing the medicinal plant species, the majority of the herbal remedies were formulated by decoction for COVID-19 (81%) and by infusion for cough (28%) and flu (33%) (Figure 5). Several ethnobotanical studies have reported that decoction and infusion are the most cited methods of herbal remedy preparation [32,40,44,45]. Decoction and infusion are the most common forms of herbal remedy preparation in local communities, primarily because of the simplicity of the process [40]. Decoction involves heating the required quantity of the plant part in water for 30 min until about half of the water is lost [46], while the infusion is done by soaking the plant material in pre-warmed or cold water [44]. The herbal preparations in this study were administered orally, by snorting (nasal), and topically. However, the majority of the remedies were administered orally for COVID-19 (88%), cough (94%), and flu (87%) Figure 6. The dominance of oral administration may be explained by the fact that the oral route is simple and rapid and allows for better absorption of bioactive constituents in the medicinal plant [32].
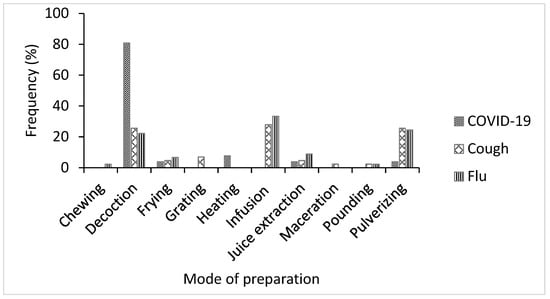
Figure 5.
Methods of preparing medicinal plant species used for the treatment of COVID-19, cough, and flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
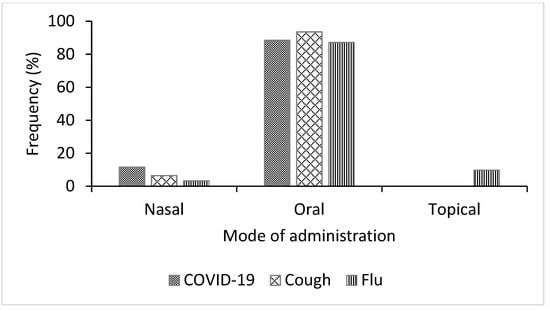
Figure 6.
Mode of administration of medicinal plant species used for the treatment of COVID-19, cough, and flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
3.5. Ethnobotanical Indices of Medicinal Plants Recorded
Ethnobotanical indices are commonly used to deduce the local importance and relevance of medicinal plants in a given study area [45,47,48]. The indices can be used to rank medicinal plant species based on their acclaimed efficacy, cultural significance, and value. Additionally, these indices are valuable tools that give cues for further scientific investigation of medicinal plant species to discover their therapeutically bioactive constituents and for setting conservation and sustainable use plans [39]. In the present study, RF, RFC, and FL were used to determine the importance of the identified medicinal plant species used for treating and preventing COVID-19, cough, and flu in the study area (Table 2). The top five most cited species for treating COVID-19 were Zingiber officinale (FC = 10; RFC = 0.18; FL = 18%), Curcuma longa (FC = 8; RFC = 0.14; FL = 14%), Azadirachta indica (FC = 8; RFC = 0.14; FL = 14%), Capsicum frutescens (FC = 6; RFC = 0.11; FL = 11%), and Citrus limon (FC = 5; RFC = 0.09; FL = 9%). For cough, the top five cited species were C. limon (FC = 13; RFC = 0.23; FL = 23%), Allium sativum (FC = 12; RFC = 0.21; FL = 21%), Citrus aurantiifolia (FC = 11; RFC = 0.20; FL = 20%), Vitellaria paradoxa (FC = 11; RFC = 0.20; FL = 20%), and Garcinia kola (FC = 8; RFC = 0.14; FL = 14%). The top five most cited species for treating flu were Z. officinale (FC = 9; RFC = 0.16; FL = 16%), Cymbopogon citratus (FC = 7; RFC = 0.13; FL = 13%), A. sativum (FC = 6; RFC = 0.11; FL = 11%), Chromolaena odorata (FC = 6; RFC = 0.11; FL = 11%), and A. indica (FC = 6; RFC = 0.11; FL = 11%) (Figure 7a–c).
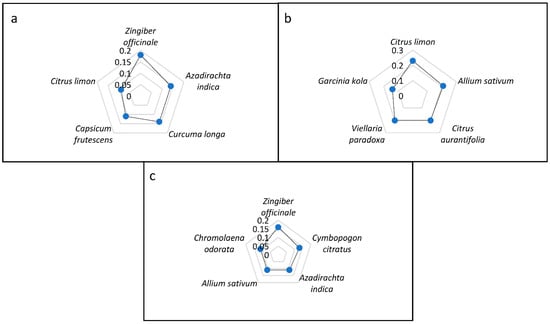
Figure 7.
Relative frequency of citation of top five plant species used for the treatment of (a) COVID-19, (b) cough, and (c) flu in Ogbomosho North and South Local Government Areas, Oyo State, Nigeria.
While ethnobotanical indices are claimed to be representations of the efficacy of medicinal plants and their potential use for drug development, it should be noted that these indices were not established by pharmacologists and statisticians [49]. Hence, the proof of concept is lacking. Additionally, the medicinal importance of plants and their cultural value cannot be summed up by numbers but are rather better obtained from a critical evaluation of the primary data based on the scope and objectives of the research [39,49].
The study’s most cited medicinal plants for treating COVID-19, including some major phytochemical components of these plants, have been reported to display antiviral and immunomodulatory activities, summarized in Table 5. For example, in an in silico docking study, Rajagopal et al. [50] reported that 8-gingerol and 10-gingerol isolated from Z. officinale were active against COVID-19 with significantly higher Glide scores when compared to hydroxychloroquine. Curcumin, a bioactive compound from C. longa, has been reported to exhibit antiviral activity against different types of enveloped viruses via several mechanisms such as induction of host antiviral responses, direct interaction with viral membrane proteins, and disruption of the viral envelope [13].
Table 5.
Antiviral and immunomodulatory properties of top-cited species used for the treatment of COVID-19, cough, and flu.
In a recent in vivo study, Supriyanto et al. [51] investigated the effect of the methanolic extract of A. indica leaf as an immunomodulator on different immune surveillance cells (CD4+, CD8+, CD25+, and CD62L). The results showed that A. indica demonstrated significant immunomodulatory activities against the cells by increasing pressure molecules and decreasing pro-inflammatory molecules. Capsaicin, the major bioactive component in Capsicum species, including C. frutescens identified in this study, has demonstrated antiviral activity and even structural disruption of viral 3CL-protease of COVID-19. Using molecular dynamics and strategies docking, Gonzalez-Paz et al. [52] evaluated the effect of capsaicin on viral 3CL-protease of COVID-19. The preliminary results from the study suggested that capsaicin can bind to the 3CL-protease of COVID-19, causing structural changes in the viral protease.
C. limon, one of the most cited species used in treating and preventing COVID-19 and cough in this study, is a well-known natural immune-modulator. Using different in silico and computational approaches, Khan et al. [53] investigated the effects of 25 phytochemicals isolated from C. limon against SARS-CoV-2 main protease (Mpro), and their docking scores compared to remdesivir. The results revealed that six flavonoid compounds (diosmetin, quercetin, eriodictoyl, luteolin, spinacetin, and apigenin) exhibited good docking scores against SARS-CoV-2 Mpro without violating any drug-like activity standard parameters. Among these six compounds, diosmetin showed better docking values than the standard antiviral drug (remdesivir).
The promising antiviral and immunomodulatory activities displayed by some of the identified medicinal plants suggest that they are potential candidates for discovering new drugs in the fight against COVID-19 and related respiratory infections. Further in vivo and clinical studies should be done to evaluate their mechanism of action and antagonistic effects against COVID-19.
4. Conclusions
This ethnobotanical survey indicated high usage of medicinal remedies in Ogbomosho North and South Local Government Areas to prevent and treat COVID-19 and related respiratory infections, particularly cough and flu. Most plants documented for COVID-19 are also used to treat other respiratory tract infections, including the common cold. The phytochemical richness and biological activities (e.g., immunomodulatory, antiviral, antimicrobial, etc.) of some of the identified species have been documented. However, further studies on these plants’ phytochemical analysis and pharmacological potentials, particularly those with relatively high ethnobotanical indices, should be conducted. This will help identify bioactive constituents and inform potential drug development to treat respiratory ailments, including COVID-19. Although the increasing global demand for herbal medicine is attributed to the belief that natural products (in this case, medicinal plants) are safe, toxicity studies should be done on the documented species to assess and establish their safety for human use. It is noteworthy that the increasing exploitation of medicinal plants for different uses might endanger the species. Hence, the conservation of these medicinal species should be prioritized for continual and sustainable use.
Author Contributions
Conceptualization, T.L.A.; methodology, C.A.O.; data analysis; C.A.O. and A.E.A.; writing—original draft preparation, C.A.O., T.L.A., A.E.A., A.O. and T.O.A.; writing—review and editing C.A.O., T.L.A., A.E.A., O.E.O., I.A.A., A.O.E., C.E.I. and T.O.A.; funding acquisition, O.E.O., I.A.A., A.O.E., C.E.I., and T.O.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee) of the Forestry Research Institute of Nigeria, Ibadan, Nigeria, with the ethical approval number CFGO711FRIN06 and approval date (5 May 2022).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jin, X.; Ren, J.; Li, R.; Gao, Y.; Zhang, H.; Li, J.; Zhang, J.; Wang, X.; Wang, G. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. E Clin. Med. 2021, 37, 100986. [Google Scholar] [CrossRef]
- José, R.J. Respiratory infections: A global burden. Ann. Res. Hosp. 2018, 2, 1–4. [Google Scholar] [CrossRef]
- Kyere, K.; Aremu, T.O.; Ajibola, O.A. Availability bias and the COVID-19 pandemic: A case study of Legionella Pneumonia. Cureus 2022, 14, e25846. [Google Scholar] [CrossRef]
- Juscamayta-Lopez, T.D.; Valdivia, F.R.; Carhuaricra, D.M. Phylogenomics reveals multiple introductions and early spread of SARS-CoV-2 into Peru. BioRxiv 2020, 10, 5961–5968. [Google Scholar] [CrossRef]
- González-Bustamante, B. Evolution and early government responses to COVID-19 in South America. World Dev. 2021, 1, 105180. [Google Scholar] [CrossRef]
- Viner, R.M.; Ward, J.L.; Hudson, L.D.; Ashe, M.P.; Hargreaves, D.; Whittaker, E. Systematic review of reviews of symptoms and signs of COVID-19 in children and adolescents. Arch. Dis. Child. 2021, 106, 802–807. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). Coronavirus: Symptoms. Available online: https://www.who.int/health-topics/coronavirus#tab%20=%20tab_32021 (accessed on 2 June 2022).
- World Health Organization (WHO). 14.9 Million Excess Deaths Associated with the COVID-19 Pandemic in 2020 and 2021. 2022. Available online: https://www.who.int/news/item/05-05-2022-14.9-million-excess-deaths-were-associated-with-the-covid-19-pandemic-in-2020-and-2021 (accessed on 27 May 2022).
- Pradhan, D.; Biswasroy, P.; Naik, P.K.; Ghosh, G.; Rath, G. A review of current interventions for COVID-19 prevention. Arch. Med. Res. 2020, 51, 363–374. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration (FDA). Coronavirus (COVID-19) Update: FDA Authorizes First Oral Antiviral for Treatment of COVID-19. FDA. 2021. Published 22 December 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19 (accessed on 26 June 2022).
- Farly, J. FDA Updates on Paxlovid for Health Care Providers. U.S. Food & Drug Administration (FDA). 2022. Published online 4 May 2022. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-updates-paxlovid-health-care-providers (accessed on 26 June 2022).
- Nugraha, R.V.; Ridwansyah, H.G.; Khairani, A.F.; Atik, N. Traditional herbal medicine candidates as complementary treatments for COVID-19: A review of their mechanisms, pros and cons. Evid. -Based Complement. Altern. Med. 2020, 2560645. [Google Scholar] [CrossRef]
- Thimmulappa, R.K.; Mudnakudu-Nagaraju, K.K.; Shivamallu, C.; Subramaniam, K.T.; Radhakrishnan, A.; Bhojraj, S.; Kuppusamy, G. Antiviral and immunomodulatory activity of curcumin: A case for prophylactic therapy for COVID-19. Heliyon 2021, 7, e06350. [Google Scholar] [CrossRef]
- Paudyal, V.; Sun, S.; Hussain, R.; Abutaleb, M.H.; Hedima, E.W. Complementary and alternative medicines use in COVID-19: A global perspective on practice, policy and research. Res. Soc. Adm. Pharm. 2022, 18, 2524–2528. [Google Scholar] [CrossRef]
- Shrestha, P.M.; Dhillion, S.S. Medicinal plant diversity and use in the highlands of Dolakha district, Nepal. J. Ethnopharmacol. 2003, 86, 81–96. [Google Scholar] [CrossRef]
- Hughes, G.D.; Aboyade, O.M.; Okonji, C.O.; Clark, B.; Mabweazara, S.Z. Comparison of the prevalence of non-communicable diseases and traditional herbal medicine use in urban and rural communities in South Africa. Adv. Integr. Med. 2021, 8, 136–143. [Google Scholar] [CrossRef]
- Ssenku, J.E.; Okurut, S.A.; Namuli, A.; Kudamba, A.; Tugume, P.; Matovu, P.; Walusansa, A. Medicinal plant use, conservation, and the associated traditional knowledge in rural communities in Eastern Uganda. Trop. Med. Health 2022, 50, 39. [Google Scholar] [CrossRef]
- Iwu, M.M.; Duncan, A.R.; Okunji, C.O. New Antimicrobials of Plant Origin. In Perspectives on New Crops and New Uses; Janick, J., Ed.; ASHS Press: Alexandria, VA, USA, 1999; pp. 457–462. ISBN 13: 9780961502706. [Google Scholar]
- Okaiyeto, K.; Oguntibeju, O.O. African herbal medicines: Adverse effects and cytotoxic potentials with different therapeutic applications. Int. J. Environ. Res. Public Health 2021, 18, 5988. [Google Scholar] [CrossRef]
- Khadka, D.; Dhamala, M.K.; Li, F.; Aryal, P.C.; Magar, P.R.; Bhatta, S. The use of medicinal plants to prevent COVID-19 in Nepal. J. Ethnobiol. Ethnomed. 2021, 17, 26. [Google Scholar] [CrossRef]
- Silva, F.S.; Ramos, M.A.; Hanazaki, N.; UPd, A. Dynamics of traditional knowledge of medicinal plants in a rural community in the Brazilian semi-arid region. Rev. Bras. Farmacogn. 2011, 21, 382–391. [Google Scholar] [CrossRef]
- Arshad, M.; Ahmad, M.; Ahmed, E.; Saboor, A.; Abbas, A.; Sadiq, S. An ethnobiological study in Kala Chitta hills of Pothwar region, Pakistan: Multinomial logit specification. J. Ethnobiol. Ethnomed. 2014, 10, 13. [Google Scholar] [CrossRef]
- Cox, P.A. Will tribal knowledge survive the millennium? Science 2000, 287, 44–45. [Google Scholar] [CrossRef]
- Falemara, B.C.; Joshua, V.I.; Ogunkanmi, T.I.; Mbeng, W.O. Ethnomedicinal survey of indigenous medicinal plants in Jos Metropolis, Nigeria. J. Med. Plants Econ. Dev. 2021, 5, 128. [Google Scholar] [CrossRef]
- Borokini, T.I.; Lawal, I.O. Traditional medicine practices among the Yoruba people of Nigeria: A historical perspective. J. Med. Plants Stud. 2014, 2, 20–33. [Google Scholar]
- Ajao, A.A.; Mukaila, Y.O.; Sabiu, S. Wandering through southwestern Nigeria: An inventory of Yoruba useful angiosperm plants. Heliyon 2021, 8, e08668. [Google Scholar] [CrossRef]
- Olorunnisola, O.S.; Adetutu, A.; Afolayan, A.J. An inventory of plants commonly used in the treatment of some disease conditions in Ogbomoso, South West, Nigeria. J. Ethnopharmacol. 2015, 161, 60–68. [Google Scholar] [CrossRef]
- Federal Republic of Nigeria, 2006 Population Census. Available online: http://www.nigerianstat.gov.ng/nbsapps/Connections/Pop2006.pdf (accessed on 20 May 2022).
- Thiers, B. Index Herbariorum: A global Directory of Public Herbaria and Associated Staff. New York Botanical Garden’s Virtual Herbarium. (continuously updated). Available online: http://sweetgum.nybg.org/ih/ (accessed on 4 October 2022).
- Tardìo, J.; Pardo-De-Santayana, M. Cultural importance indices: A comparative analysis based on the useful wild plants of Southern Cantabria (Northern Spain). Econ. Bot. 2008, 62, 24–39. [Google Scholar] [CrossRef]
- Friedman, J.; Yaniv, Z.; Dafni, A.; Palewitch, D. A preliminary classification of the healing potential of medicinal plants, based on a rational analysis of an ethnopharmacological field survey among Bedouins in the Negev Desert, Israel. J. Ethnopharmacol. 1986, 16, 275–287. [Google Scholar] [CrossRef]
- Brahmi, F.; Iblhoulen, Y.; Issaadi, H.; Elsebai, M.F.; Madani, K.; Boulekbache-Makhlouf, L. Ethnobotanical survey of medicinal plants of bejaia localities from algeria to prevent and treat coronavirus (COVID-19) infection shortened title: Phytomedicine to manage COVID-19 pandemic. Adv. Tradit. Med. 2022, 1–13. [Google Scholar] [CrossRef]
- Chukwuma, D.M.; Chukwuma, E.C.; Adekola, O.O. An ethnobotanical survey of Malaria-treating plants in Ado-Ekiti Local Government Area, Ekiti State, Nigeria. Ethnobot. Res. Appl. 2019, 18, 1–10. [Google Scholar] [CrossRef][Green Version]
- Tavilla, G.; Crisafulli, A.; Ranno, V.; Picone, R.M.; Redouan, F.Z.; del Galdo, G.G. First contribution to the ethnobotanical knowledge in the Peloritani Mounts (NE Sicily). Res. J. Ecol. Environ. Sci. 2022, 4, 1–34. [Google Scholar] [CrossRef]
- Olatokun, W.M.; Ayanbode, O.F. Use of indigenous knowledge by women in a Nigerian rural community. Indian J. Tradit. Knowl. 2009, 8, 287–295. [Google Scholar]
- Benkhaira, N.; Koraichi, S.I.; Fikri-Benbrahim, K. Ethnobotanical survey on plants used by traditional healers to fight against COVID-19 in Fez city, Northern Morocco. Ethnobot. Res. Appl. 2021, 21, 1–18. [Google Scholar] [CrossRef]
- Singh, B.; Singh, B.; Kishor, A.; Singh, S.; Bhat, M.N.; Surmal, O.; Musarella, C.M. Exploring plant-based ethnomedicine and quantitative ethnopharmacology: Medicinal plants utilized by the population of Jasrota Hill in Western Himalaya. Sustainability 2020, 12, 7526. [Google Scholar] [CrossRef]
- Bhat, M.N.; Singh, B.; Surmal, O.; Singh, B.; Shivgotra, V.; Musarella, C.M. Ethnobotany of the Himalayas: Safeguarding medical practices and traditional uses of Kashmir regions. Biology 2021, 10, 851. [Google Scholar] [CrossRef] [PubMed]
- Lawal, I.O.; Rafiu, B.O.; Ale, J.E.; Majebi, O.E.; Aremu, A.O. Ethnobotanical survey of local flora used for medicinal purposes among indigenous people in five areas in Lagos State, Nigeria. Plants 2022, 11, 633. [Google Scholar] [CrossRef] [PubMed]
- Lawal, I.O.; Olufade, I.I.; Rafiu, B.O.; Aremu, A.O. Ethnobotanical survey of plants used for treating cough associated with respiratory conditions in Ede South local government area of Osun State, Nigeria. Plants 2020, 9, 647. [Google Scholar] [CrossRef] [PubMed]
- Zakariya, A.M.; Adamu, A.; Nuhu, A.; Kiri, I.Z. Assessment of indigenous knowledge on medicinal plants used in the management of malaria in Kafin Hausa, north-western Nigeria. Ethnobot. Res. Appl. 2021, 22, 1–18. [Google Scholar] [CrossRef]
- Ahmad, M.; Sultana, S.; Fazl-i-Hadi, S.; Ben Hadda, T.; Rashid, S.; Zafar, M.; Yaseen, G. An ethnobotanical study of medicinal plants in high mountainous region of Chail valley (District Swat-Pakistan). J. Ethnobiol. Ethnomed. 2014, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Tugume, P.; Kakudidi, E.K.; Buyinza, M. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J. Ethnobiol. Ethnomed. 2016, 12, 5. [Google Scholar] [CrossRef]
- Suroowan, S.; Mahomoodally, M.F. A comparative ethnopharmacological analysis of traditional medicine used against respiratory tract diseases in Mauritius. J. Ethnopharmacol. 2016, 177, 61–80. [Google Scholar] [CrossRef]
- Ishtiaq, M.; Maqbool, M.; Ajaib, M.; Ahmed, M.; Hussain, I.; Khanam, H.; Mushtaq, W.; Hussain, T.; Azam, S.; Hayat, B.K.; et al. Ethnomedicinal and folklore inventory of wild plants used by rural communities of valley Samahni, District Bhimber Azad Jammu and Kashmir, Pakistan. PLoS ONE 2021, 16, e0243151. [Google Scholar] [CrossRef]
- Nagalingam, A. Drug Delivery Aspects of Herbal Medicines. Jpn Kampo Med. Treat Common Dis. Focus Inflamm. 2017, 17, 143. [Google Scholar]
- Hoffman, B.; Gallaher, T. Importance indices in ethnobotany. Ethnobot. Res. Appl. 2007, 5, 201–208. [Google Scholar] [CrossRef]
- Weckerle, C.S.; De Boer, H.J.; Puri, R.K.; Van, A.T.; Bussmann, R.W.; Leonti, M. Recommended standards for conducting and reporting ethnopharmacological field studies. J. Ethnopharmacol. 2018, 210, 125–132. [Google Scholar] [CrossRef]
- Leonti, M. The relevance of quantitative ethnobotanical indices for ethnopharmacology and ethnobotany. J. Ethnopharmacol. 2022, 288, 115008. [Google Scholar] [CrossRef]
- Rajagopal, K.; Byran, G.; Jupudi, S.; Vadivelan, R. Activity of phytochemical constituents of black pepper, ginger, and garlic against coronavirus (COVID-19): An in silico approach. Int. J. Health Allied Sci. 2020, 9, 43–50. [Google Scholar] [CrossRef]
- Supriyanto, S.; Widjanarko, S.; Rifa’i, M.; Yunianta, Y. Immunomodulatory activity of methanol leaf extract of neem (Azadirachta Indica Juss.) against suppressor and proinflammatory molecules. J. Trop. Life Sci. 2021, 11, 309–316. [Google Scholar] [CrossRef]
- Gonzalez-Paz, L.; Lossada, C.; Moncayo, L.; Romero, F.; Paz, J.; Vera-Villalobos, J.; Pérez, A.; San-Blas, E.; Alvarado, Y. Theoretical molecular docking study of the structural disruption of the viral 3CL-protease of COVID19 induced by binding of capsaicin, piperine and curcumin part 1: A comparative study with chloroquine and hydrochloroquine two antimalaric drugs. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Khan, J.; Sakib, S.; Mahmud, S.; Khan, Z.; Islam, M.; Sakib, M.; Simal-Gandara, J. Identification of potential phytochemicals from Citrus limon against main protease of SARS-CoV-2: Molecular docking, molecular dynamic simulations and quantum computations. J. Biomol. Struct. Dyn. 2021, 1–12. [Google Scholar] [CrossRef]
- Josling, P. Preventing the common cold with a garlic supplement: A double-blind, placebo-controlled survey. Adv Ther. 2001, 18(4), 189–193. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yan, Y.X.; Yu, Q.T.; Deng, Y.; Wu, D.T.; Wang, Y.J. Comparison of immunomodulatory effects of fresh garlic and black garlic polysaccharides on RAW 264.7 macrophages. J. Food Sci. 2017, 82, 765–771. [Google Scholar] [CrossRef]
- Rouf, R.; Uddin, S.J.; Sarker, D.K.; Islam, M.T.; Ali, E.S.; Shilpi, J.A.; Sarker, S.D. Antiviral potential of garlic (Allium sativum) and its organosulfur compounds: A systematic update of pre-clinical and clinical data. Trends Food Sci. Technol. 2020, 104, 219–234. [Google Scholar] [CrossRef]
- Ashfaq, U.A.; Jalil, A.; Qamar, M.T. Antiviral phytochemicals identification from Azadirachta indica leaves against HCV NS3 protease: An in silico approach. Nat. Prod. Res. 2016, 30, 1866–1869. [Google Scholar] [CrossRef]
- Olwenyi, O.A.; Asingura, B.; Naluyima, P. In-vitro Immunomodulatory activity of Azadirachta indica A.Juss. Ethanol: Water mixture against HIV associated chronic CD4+ T-cell activation/exhaustion. BMC Complement Med. 2021, 21, 114. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, R.; Majeed, S.; Saghir, S.; Saad, M.; Ashraf, H.; Fayyaz, I. Antiviral activity of extract of neem (Azadirachta Indica) leaves: An in vivo study. Pak. J. Med. Health Sci. 2022, 16, 10. [Google Scholar] [CrossRef]
- Viveros-Paredes, J.M.; Puebla-Pérez, A.M.; Gutiérrez-Coronado, O.; Macías-Lamas, A.M.; Hernández-Flores, G.; Ortiz-Lazareno, P.C.; Villaseñor-García, M.M. Capsaicin attenuates immunosuppression induced by chronic stress in BALB/C mice. Int. Immunopharmacol. 2021, 93, 107341. [Google Scholar] [CrossRef]
- Nudo, L.P.; Catap, E.S. Anti-immunosuppressive effects of Chromolaena odorata (Lf.) King & Robinson (Asteraceae) leaf extract in cyclophosphamide-injected Balb/C mice. Philipp. J. Sci. 2012, 141, 35–43. [Google Scholar]
- Boudjeko, T.; Megnekou, R.; Woguia, A.L.; Kegne, F.M.; Ngomoyogoli, J.E.K.; Tchapoum, C.D.N.; Koum, O. Antioxidant and immunomodulatory properties of polysaccharides from Allanblackia floribunda Oliv stem bark and Chromolaena odorata (L.) King and HE Robins leaves. BMC Res. Notes 2015, 8, 759. [Google Scholar] [CrossRef]
- Lappas, C.M.; Lappas, N.T. D-Limonene modulates T lymphocyte activity and viability. Cell. Immunol. 2012, 279, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Nagy, M.M.; Al-Mahdy, D.A.; Abd El Aziz, O.M.; Kandil, A.M.; Tantawy, M.A.; El Alfy, T.S. Chemical composition and antiviral activity of essential oils from Citrus reshni hort. ex Tanaka (Cleopatra mandarin) cultivated in Egypt. J. Essent. Oil Bear. Plants 2018, 21, 264–272. [Google Scholar] [CrossRef]
- Meeran, M.N.; Seenipandi, A.; Javed, H.; Sharma, C.; Hashiesh, H.M.; Goyal, S.N.; Ojha, S. Can limonene be a possible candidate for evaluation as an agent or adjuvant against infection, immunity, and inflammation in COVID-19? Heliyon 2021, 7, e05703. [Google Scholar] [CrossRef]
- Diab, K.A. In vitro studies on phytochemical content, antioxidant, anticancer, immunomodulatory, and antigenotoxic activities of lemon, grapefruit, and mandarin citrus peels. Asian Pac. J. Cancer Prev. 2016, 17, 3559–3567. [Google Scholar]
- Abd, A.J.; Al-Shammarie, A.M.; Abd, A.H. Antiviral activity of limonin against Newcastle disease virus in vitro. Res. J. Biotechnol. 2019, 14, 320–328. [Google Scholar]
- Afolayan, F.I.; Erinwusi, B.; Oyeyemi, O.T. Immunomodulatory activity of curcumin-entrapped poly d, l-lactic-co-glycolic acid nanoparticles in mice. Integr. Med. Res. 2018, 7, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Gu, L.; Su, Y.; Wang, Q.; Zhao, Y.; Chen, X.; Li, K. Inhibition of curcumin on influenza A virus infection and influenzal pneumonia via oxidative stress, TLR2/4, p38/JNK MAPK and NF-κB pathways. Int. Immunopharmacol. 2018, 54, 177–187. [Google Scholar] [CrossRef]
- Duran, N.; Kaya, D.A. Chemical composition of essential oils from Origanum onites L. and Cymbopogon citratus, and their synergistic effects with acyclovir against HSV-1. In Proceedings of the 7th International Conference on Advanced Materials and Systems 2018, Bucharest, Romania, 18–20 October 2018; The National Research & Development Institute for Textiles and Leather: București, Romania, 2018; pp. 243–248. [Google Scholar]
- Goncalves, E.C.; Assis, P.M.; Junqueira, L.A.; Cola, M.; Santos, A.R.; Raposo, N.R.; Dutra, R.C. Citral inhibits the inflammatory response and hyperalgesia in mice: The role of TLR4, TLR2/Dectin-1, and CB2 cannabinoid receptor/ATP-sensitive K+ channel pathways. J. Nat. Prod. 2020, 83, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Rosmalena, R.; Elya, B.; Dewi, B.E.; Fithriyah, F.; Desti, H.; Angelina, M.; Seto, D. The antiviral effect of indonesian medicinal plant extracts against dengue virus in vitro and in silico. Pathogens 2019, 8, 85. [Google Scholar] [CrossRef]
- Nworu, C.S.; Akah, P.A.; Esimone, C.O.; Okoli, C.O.; Okoye, F.B.C. Immunomodulatory activities of kolaviron, a mixture of three related biflavonoids of Garcinia kola Heckel. Immunopharmacol. Immunotoxicol. 2008, 30, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Awogbindin, I.O.; Olaleye, D.O.; Farombi, E.O. Kolaviron improves morbidity and suppresses mortality by mitigating oxido-inflammation in BALB/c mice infected with influenza virus. Viral Immunol. 2015, 28, 367–377. [Google Scholar] [CrossRef]
- Farombi, E.O.; Awogbindin, I.O.; Farombi, T.H.; Ikeji, C.N.; Adebisi, A.; Adedara, I.A.; Aruoma, O.I. Possible role of Kolaviron, a Garcinia kola bioflavonoid in inflammation associated COVID-19 infection. Am. J. Biopharmacy Pharm. Sci. 2022, 2, 1–13. [Google Scholar] [CrossRef]
- Kudi, A.C.; Myint, S.H. Antiviral activity of some Nigerian medicinal plant extracts. J. Eethnopharmacol. 1999, 68, 289–294. [Google Scholar] [CrossRef]
- Foyet, H.S.; Tsala, D.E.; Zogo, E.B.; Carine, A.N.; Heroyne, L.T.; Oben, E.K. Anti-inflammatory and anti-arthritic activity of a methanol extract from Vitellaria paradoxa stem bark. Pharmacogn. Res. 2014, 7, 367–377. [Google Scholar] [CrossRef]
- Abdel-Moneim, A.; Morsy, B.M.; Mahmoud, A.M.; Abo-Seif, M.A.; Zanaty, M.I. Beneficial therapeutic effects of Nigella sativa and/or Zingiber officinale in HCV patients in Egypt. EXCLI J. 2013, 11, 43–55. [Google Scholar]
- Li, C.; Dong, Z.; Zhang, B.; Huang, Q.; Liu, G.; Fu, X. Structural characterization and immune enhancement activity of a novel polysaccharide from Moringa oleifera leaves. Carbohydr. Polym. 2020, 234, 115897. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wei, S.; Lu, X.; Qiao, X.; Simal-Gandara, J.; Capanoglu, E.; Li, N. A neutral polysaccharide with a triple helix structure from ginger: Characterization and immunomodulatory activity. Food Chem. 2021, 350, 129261. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).