Using GIS for Determining Variations in Health Access in Jeddah City, Saudi Arabia

Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. The Database
2.3. Network Analysis
3. Results
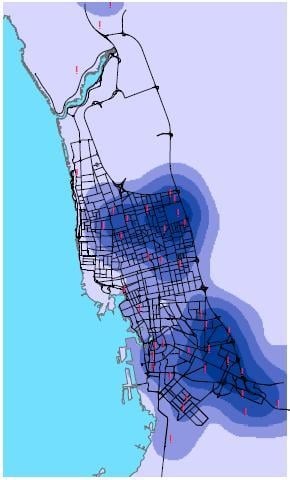
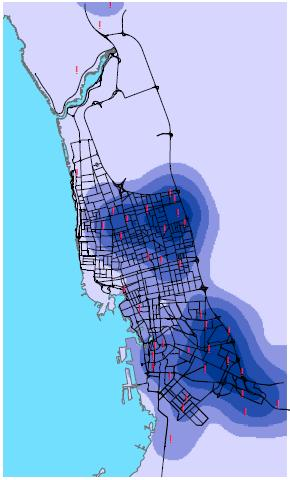
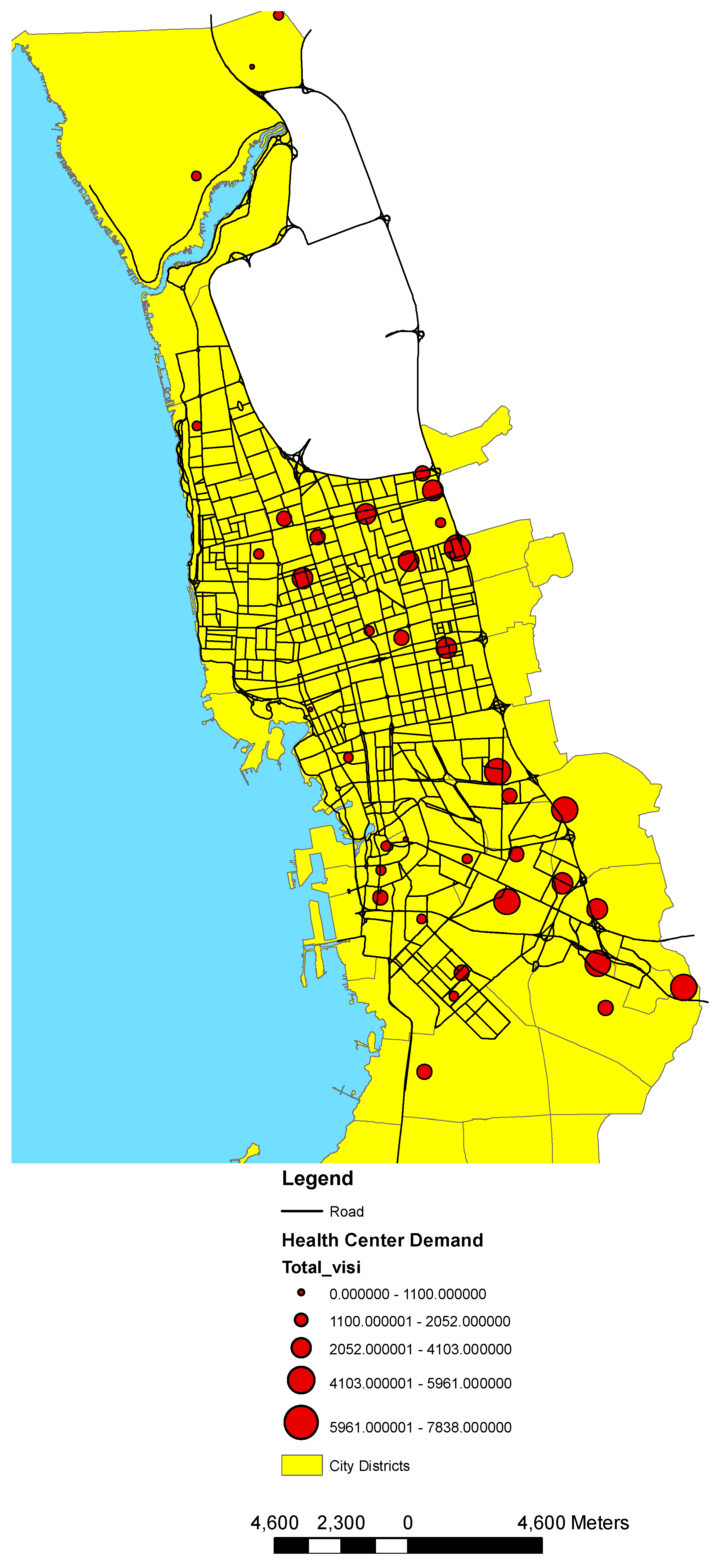
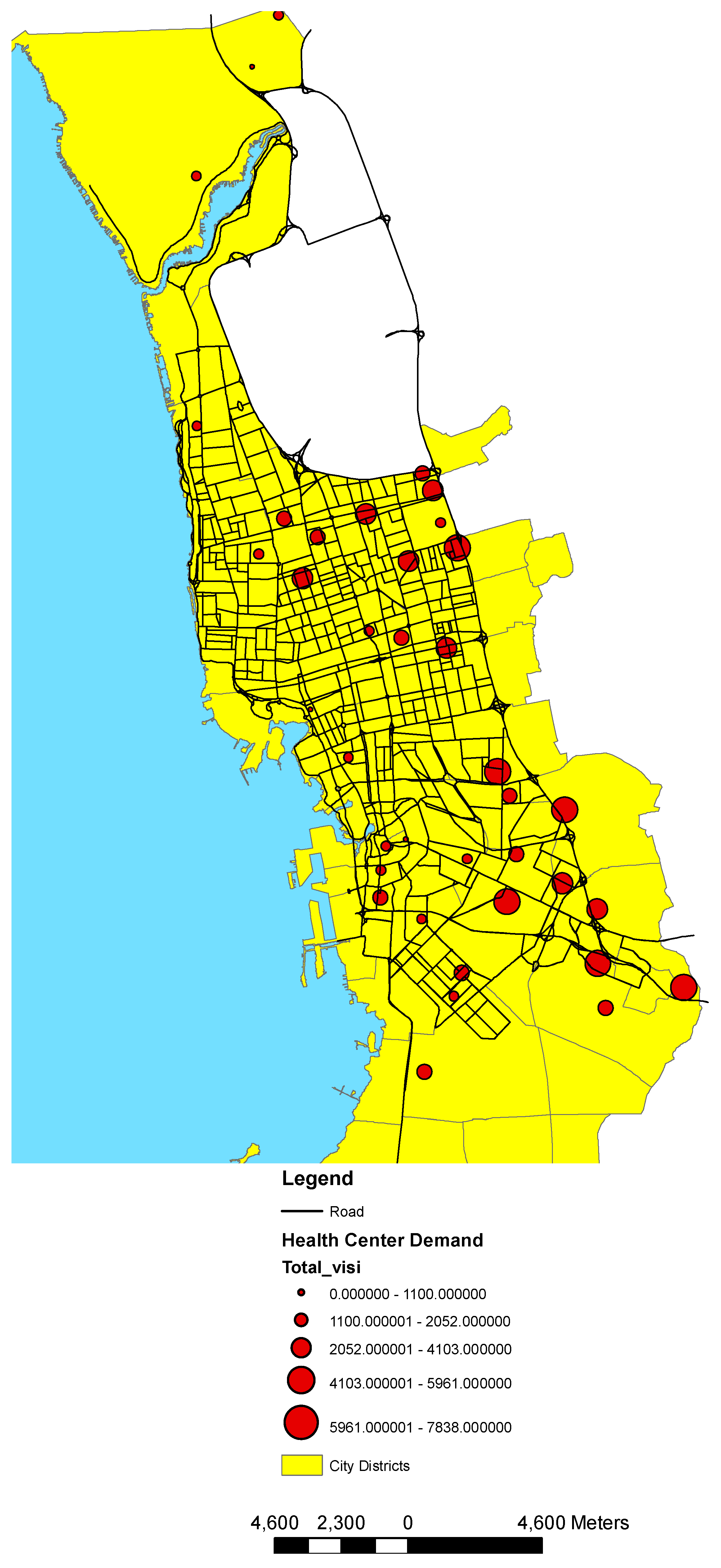
3.1. Health Center Classification and Analysis
- Calculate the mean center of the input points. If a Population field other than None was selected, this, and all the following calculations, will be weighted by the values in that field.
- Calculate the distance from the (weighted) mean center for all points.
- Calculate the (weighted) median of these distances, Dm.
- Calculate the (weighted) Standard Distance, SD.
- Apply the following formula to calculate the bandwidth:where:
- SD is the standard distance
- Dm is the median distance
- n is the number of points if no population field is used, or if a population field is supplied, n is the sum of the population field value.
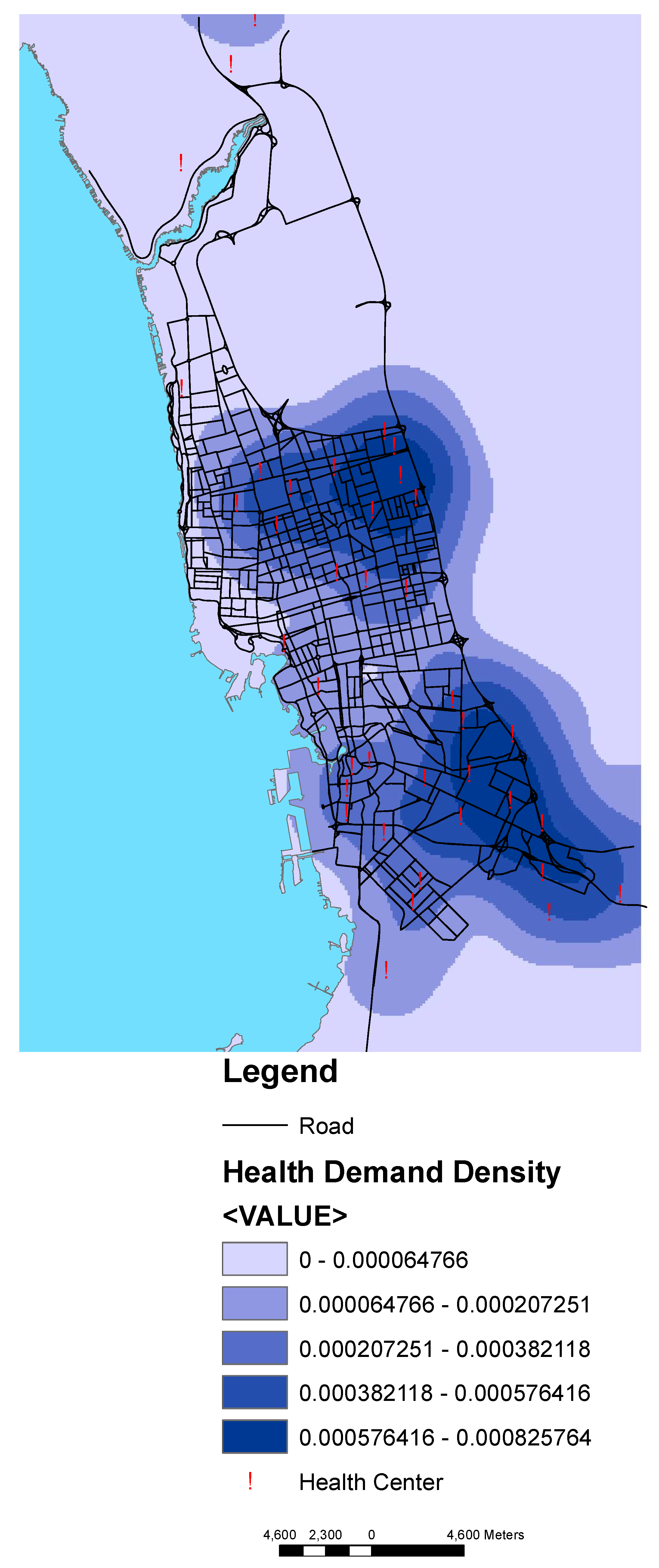
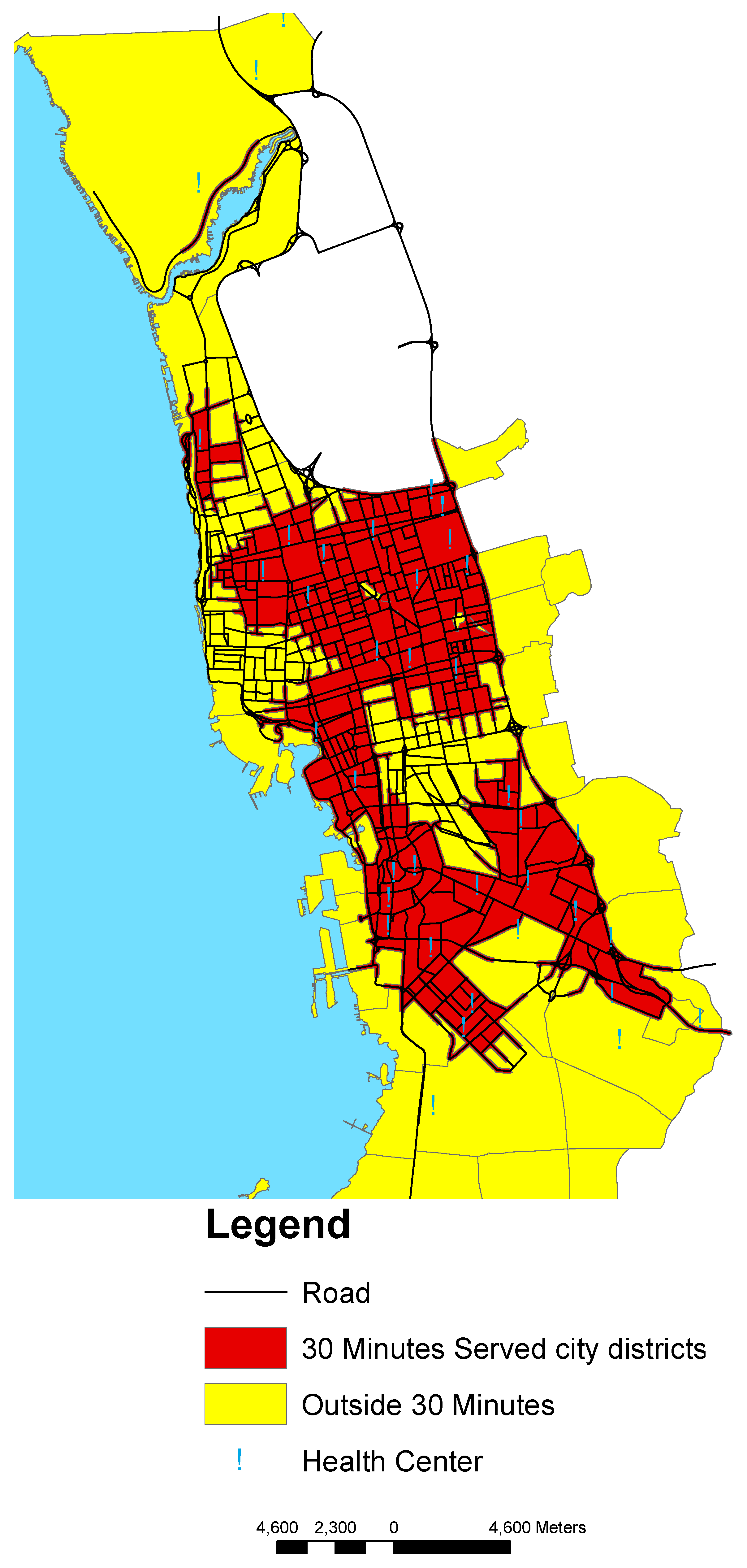
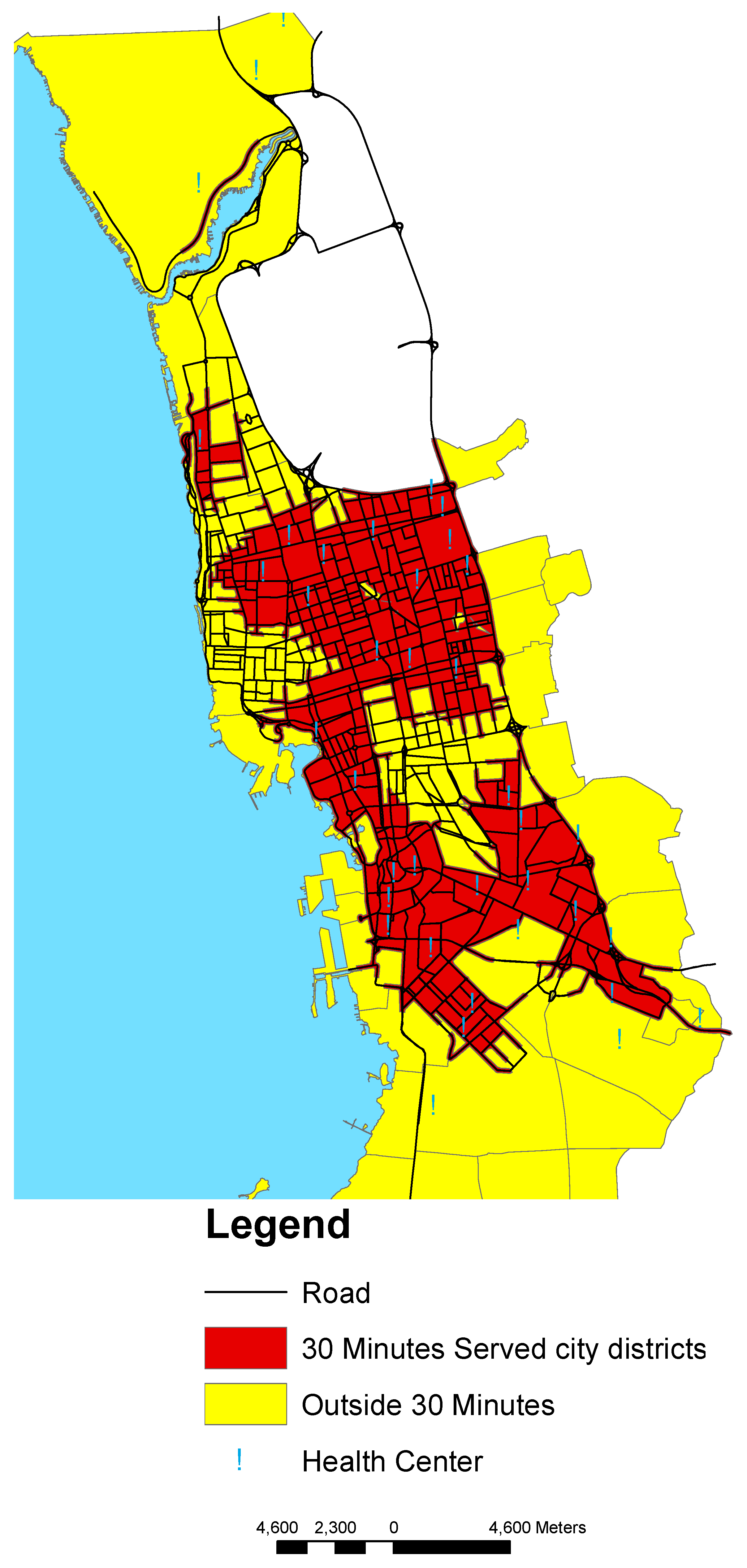
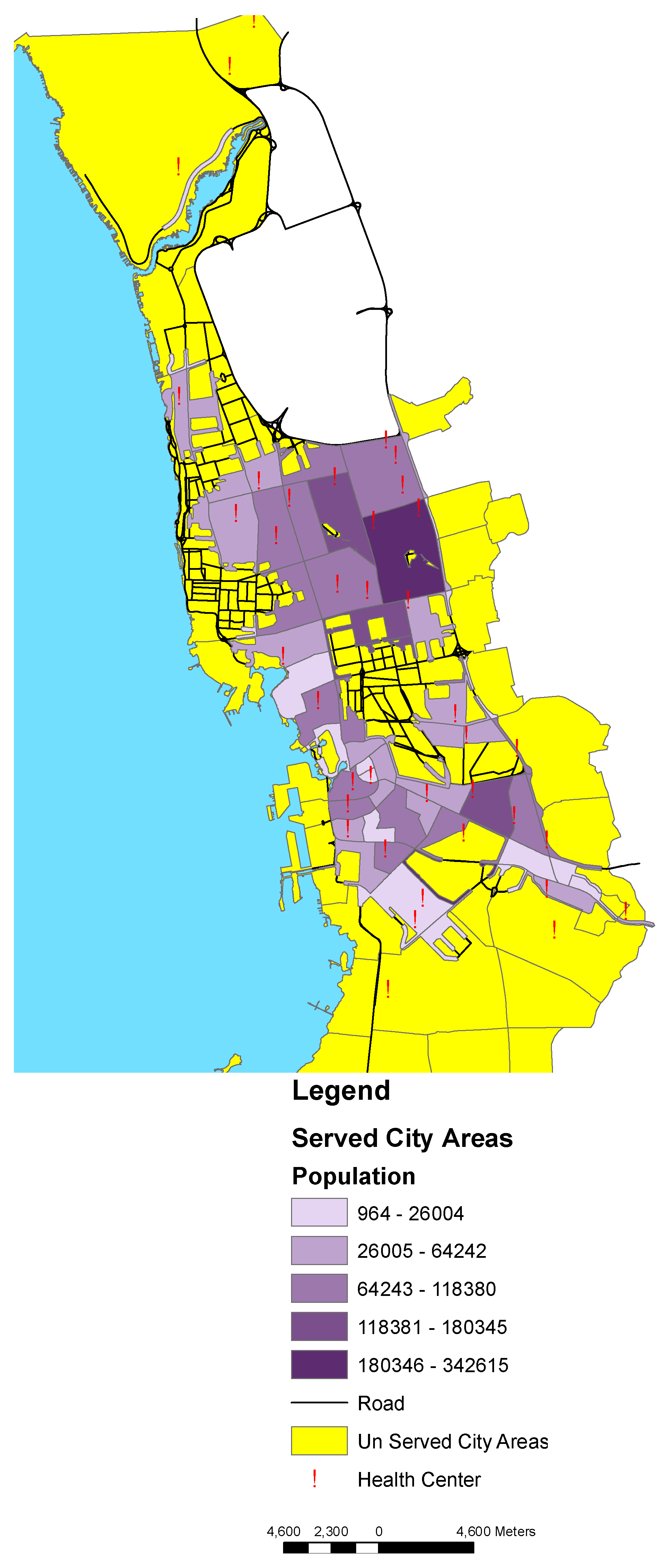
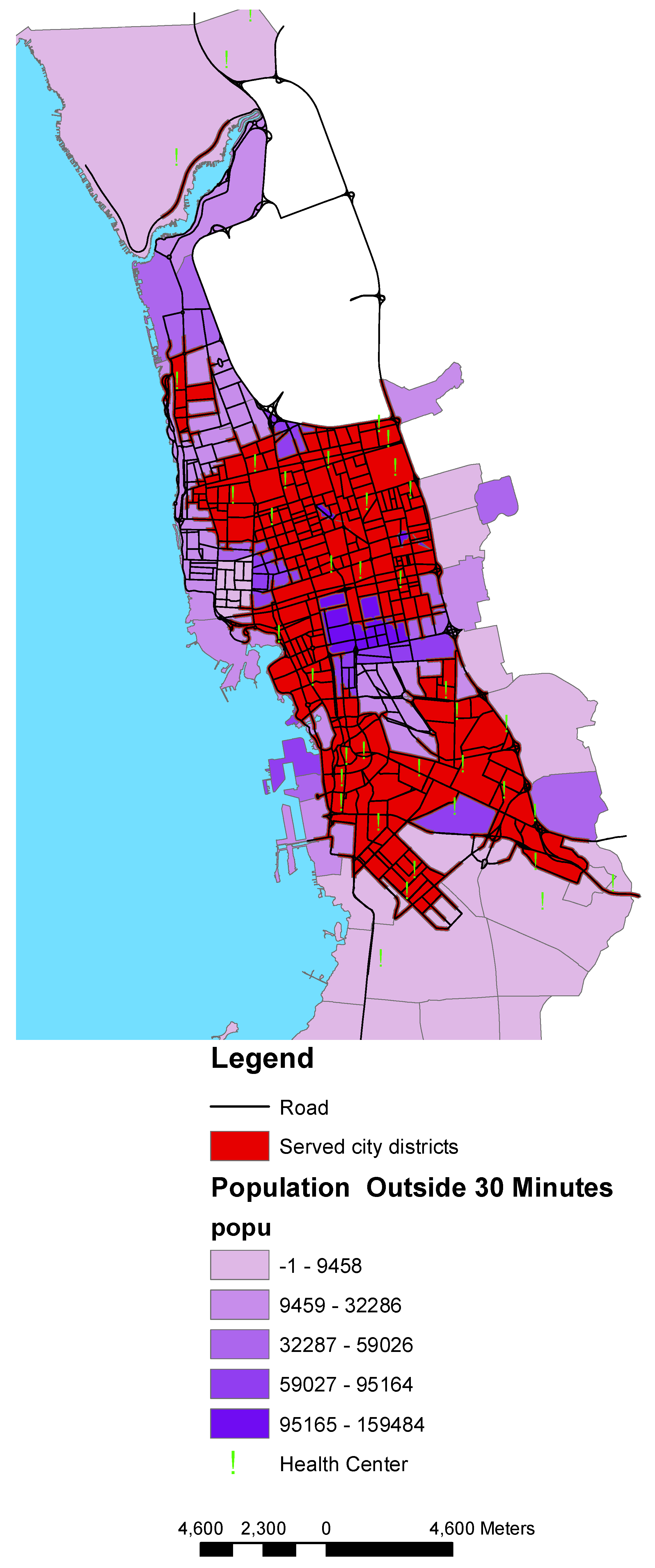
3.2. Access to Health Centers
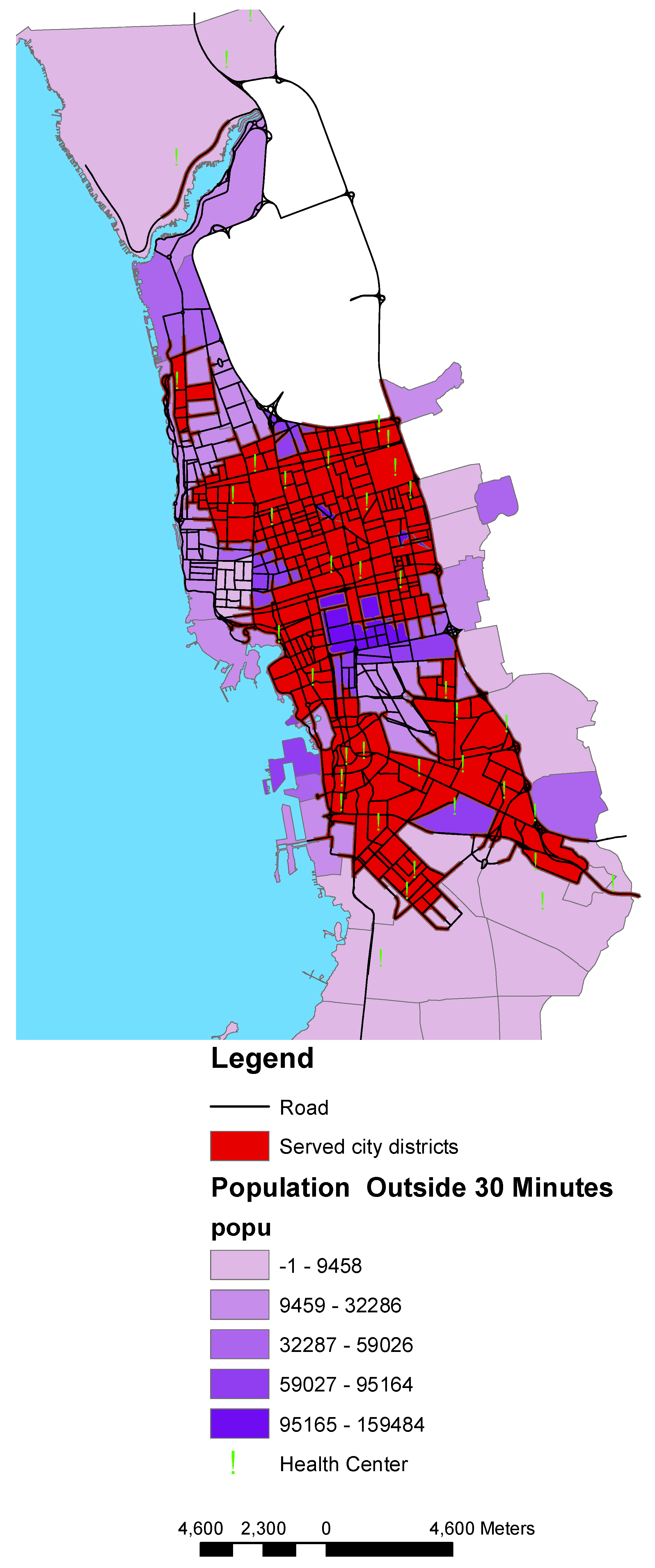
3.3. Population within Access to Health Centers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fletcher-Lartey, S.M.; Caprarelli, G. Application of GIS technology in public health: Successes and challenges. Parasitology 2016, 143, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Hanchette, C.L. Geographic Information Systems. In Public Health Informatics; O’Carroll, P.W., Yasnoff, Y.A., Ward, M.E., Ripp, L.H., Martin, E.L., Eds.; Springer: New York, NY, USA, 2003; pp. 431–466. [Google Scholar]
- Comber, A.; Brunsdon, C.; Green, E. Using a GIS-based network analysis to determine urban greenspace accessibility for different ethnic and religious groups. Landsc. Urban Plan. 2008, 86, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Nichols, E.N.; Bradley, D.L.; Zhang, X.; Faruque, F.; Duhé, R.J. The geographic distribution of mammography resources in Mississippi. Online J. Public Health Inform. 2014, 5, 226. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, N.; Benwell, G.; Holt, A. Measuring spatial accessibility to primary health care. In Proceedings of the SIRC 2005—The 17th Annual Colloquium of the Spatial Information Research Centre University of Otago, Dunedin, New Zealand, 24–25 November 2005. [Google Scholar]
- Mushonga, H.T.; Banda, F.; Mulolwa, A. Development of a web based GIS for health facilities mapping, monitoring and reporting: A case study of the Zambian Ministry of health. S. Afr. J. Geomat. 2017, 6, 321–332. [Google Scholar] [CrossRef]
- Gao, F.; Kihal, W.; Le Meur, N.; Souris, M.; Deguen, S. Assessment of the spatial accessibility to health professionals at French census block level. Int. J. Equity Health 2016, 15, 125. [Google Scholar] [CrossRef] [PubMed]
- Murad, A. Defining health catchment areas in Jeddah city, Saudi Arabia: An example demonstrating the utility of Geographical Information Systems. Geospat. Health 2008, 2, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Comber, A.; Brunsdon, C.; Radburn, R. A spatial analysis of variations in health access: Linking geography, socio-economic status and access perceptions. Int. J. Health Geogr. 2011, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- ESRI. Getting to Know Arcview; Geoinformation Int.; ESRI: Cambridge, UK, 2004. [Google Scholar]
- Brual, J.; Gravely-Witte, S.; Suskin, N.; Stewart, D.; Macpherson, A.; Grace, S. Drive time to cardiac rehabilitation: At what point does it affect utilization? Int. J. Health Geogr. 2010, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Penchansky, R.; Thomas, J.W. The concept of access. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Aday, L.A.; Andersen, R. A framework for the study of access to medical care. Health Serv. Res. 1974, 9, 208–220. [Google Scholar] [PubMed]
- Gulliford, M.; Figueroa-Munoz, J.; Morgan, M.; Hughes, D.; Gibson, B.; Beech, R.; Hudson, M. What does ‘access to health care’ mean? J. Health Serv. Res. Policy 2002, 7, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Higgs, G. A Literature Review of the Use of GIS-Based Measures of Access to Health Care Services. Health Serv. Outcomes Res. Methodol. 2004, 5, 119–139. [Google Scholar] [CrossRef]
- Papadimitriou, F. Modelling spatial landscape complexity using the Levenshtein algorithm. Ecol. Inform. 2009, 4, 48–55. [Google Scholar] [CrossRef]
- Papadimitriou, F. The Algorithmic Complexity of Landscapes. Landsc. Res. 2012, 37, 1–21. [Google Scholar] [CrossRef]

© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murad, A. Using GIS for Determining Variations in Health Access in Jeddah City, Saudi Arabia. ISPRS Int. J. Geo-Inf. 2018, 7, 254. https://doi.org/10.3390/ijgi7070254
Murad A. Using GIS for Determining Variations in Health Access in Jeddah City, Saudi Arabia. ISPRS International Journal of Geo-Information. 2018; 7(7):254. https://doi.org/10.3390/ijgi7070254
Chicago/Turabian StyleMurad, Abdulkader. 2018. "Using GIS for Determining Variations in Health Access in Jeddah City, Saudi Arabia" ISPRS International Journal of Geo-Information 7, no. 7: 254. https://doi.org/10.3390/ijgi7070254
APA StyleMurad, A. (2018). Using GIS for Determining Variations in Health Access in Jeddah City, Saudi Arabia. ISPRS International Journal of Geo-Information, 7(7), 254. https://doi.org/10.3390/ijgi7070254