A Review on Design of Upper Limb Exoskeletons



Abstract
1. Introduction
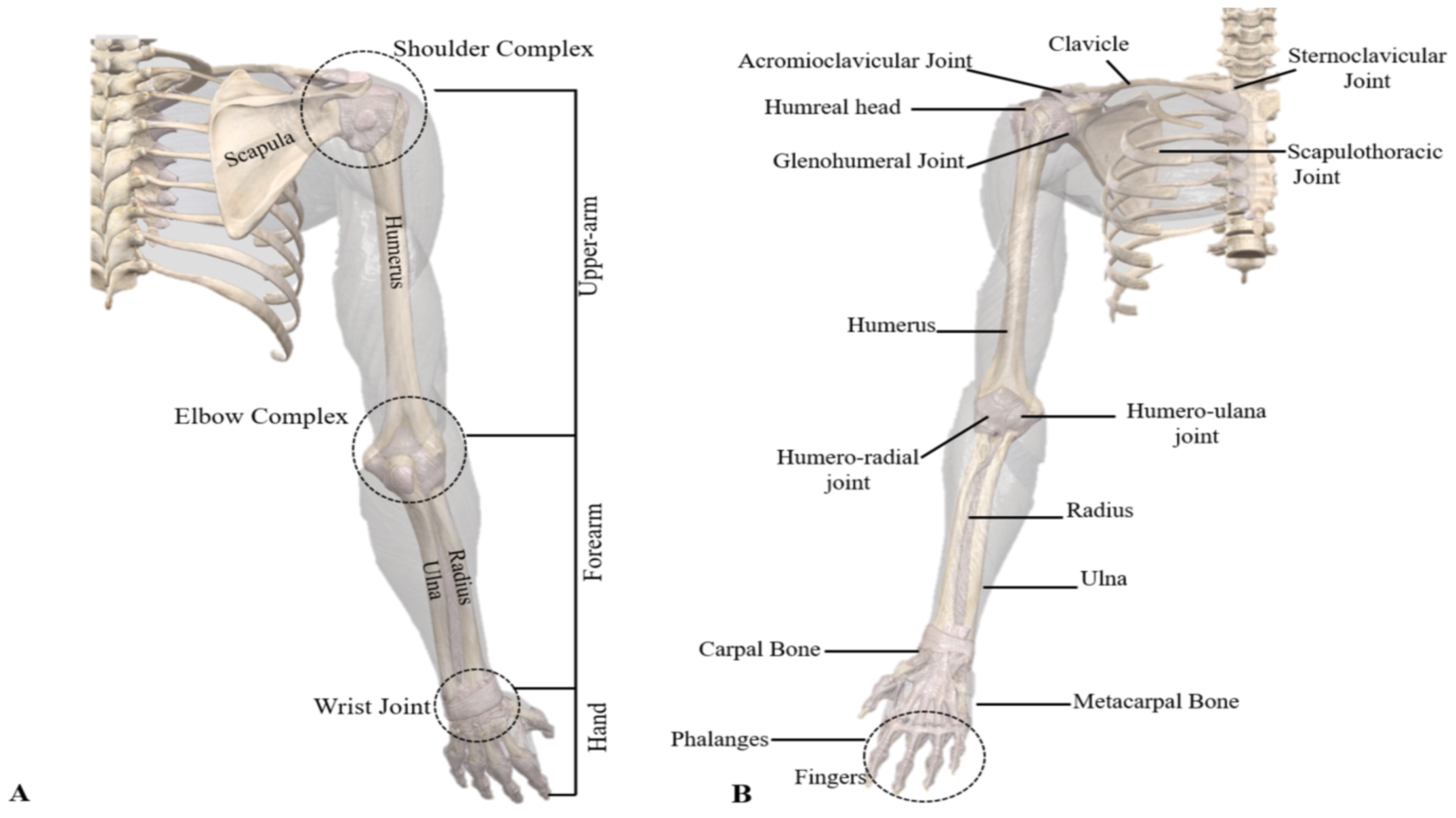
2. Upper Limb Anatomy and Design Challenges
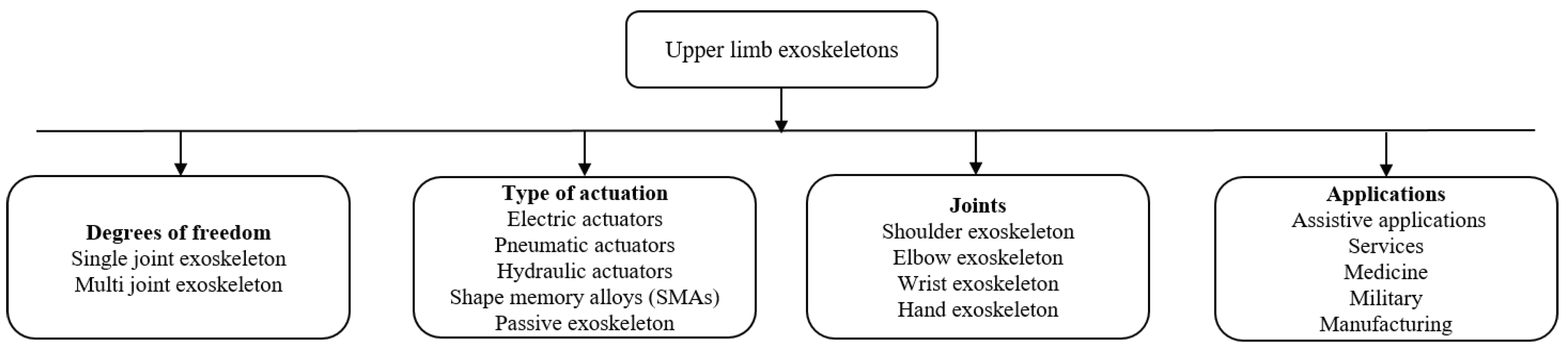
3. Upper Limb Exoskeletons
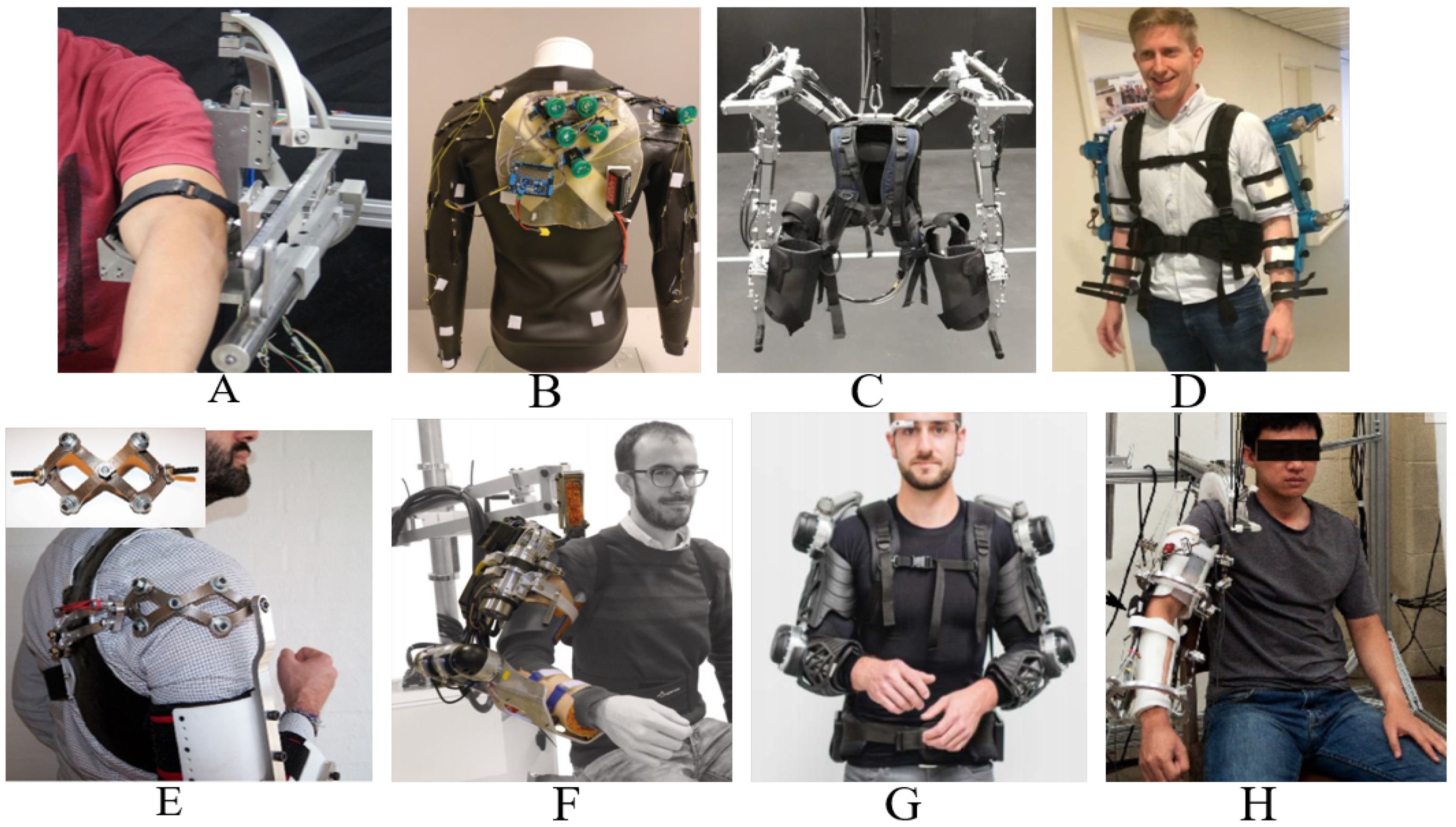
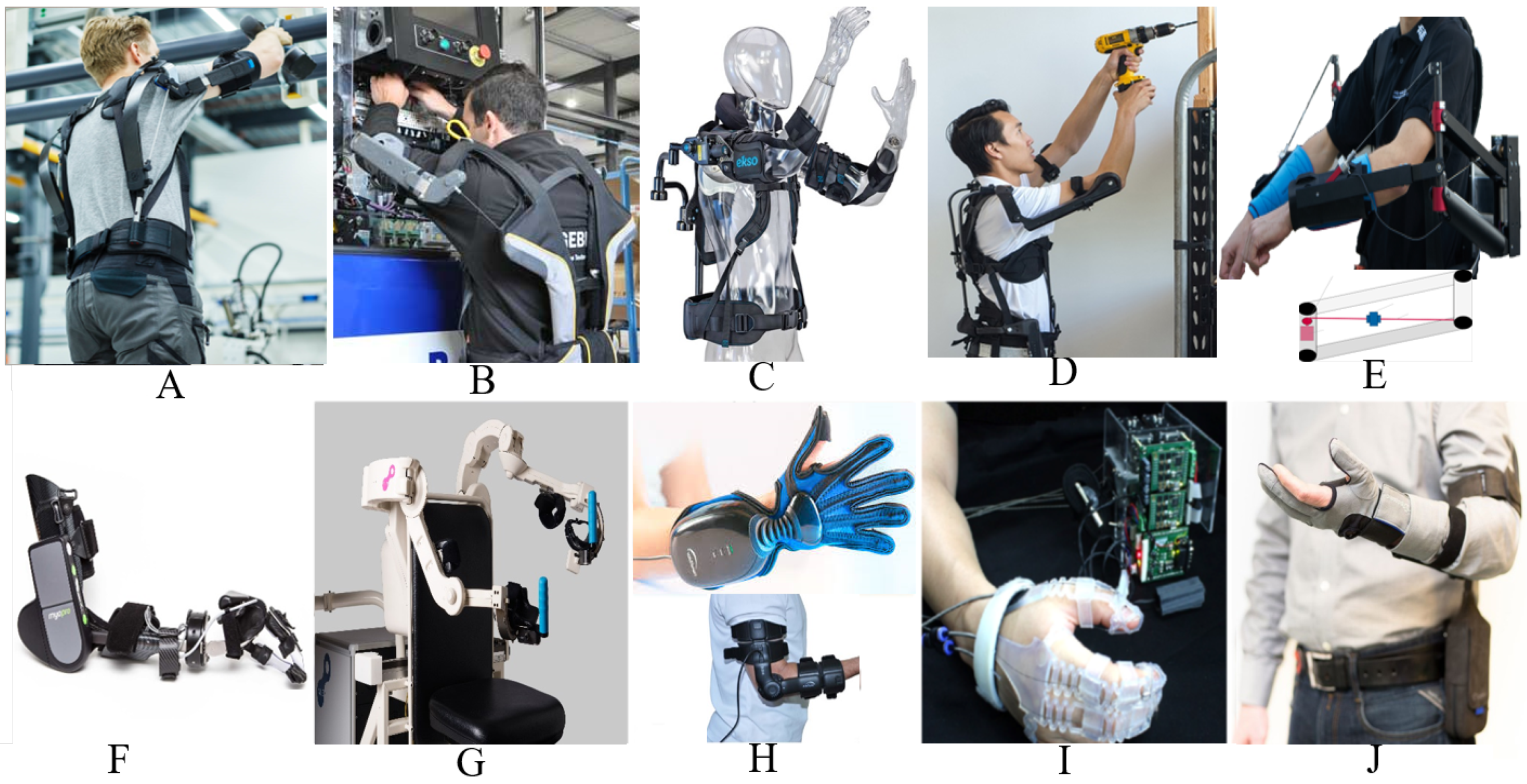
3.1. Exoskeletons for Motion Assistance
3.1.1. EksoVest
3.1.2. AAU Upper Body Exo
3.1.3. Five-DOF Wearable Upper-Limb Exoskeleton
3.1.4. CAREX-7
3.1.5. 6-REXOS
3.1.6. Stuttgart Exo-Jacket
3.1.7. Robo-Mate Exoskeleton
3.1.8. Compliant Robotic Upper-Extremity eXosuit (CRUX)
3.1.9. Soft Extra Muscle (SEM) Glove
3.2. Exoskeletons for Medical Rehabilitation
3.2.1. Upper-Body Exoskeleton for Rehabilitation (Harmony)
3.2.2. Parallel Actuated Shoulder Exoskeleton
3.2.3. 5-DOF Parallel Actuated Shoulder Exoskeleton
3.2.4. NEUROExos
3.2.5. EAsoft Module for Neuro-Rehabilitation
3.2.6. Cable-Driven Upper-Limb Exoskeleton
3.2.7. Upper-Limb Exoskeleton for Rehabilitation
3.2.8. Active Elbow Orthosis
3.2.9. eWrist
3.2.10. Under-Actuated Hand Exoskeleton
3.2.11. Advanced Service Robot (ASR) Glove
3.2.12. Hand Exoskeleton for Post-Stoke Patients
3.2.13. Spring-Assisted Hand-Opening Exoskeleton Module for Functional Rehabilitation
3.2.14. Spring-Assisted Exoskeleton Module for Wrist and Hand Rehabilitation
4. Control Strategies
4.1. Assistive Mode
4.1.1. Passive Control
4.1.2. Partially Assistive Control
4.2. Corrective Mode
Tunneling
5. Actuation and Power Transmission
6. Exoskeleton Design Modeling
7. Possible Challenges in Upper-Limb Exoskeleton Development
7.1. Kinematic Compatibility
7.2. Workspace Limitation
7.3. Singularity Problem of Mechanical System
7.4. Discomfort and Misalignment
7.5. Human–Robot Interaction
7.6. Sensing and Estimation
8. Discussion and Future Directions
8.1. Ergonomic and Standardized Design
8.2. Exoskeleton Design Modeling
8.3. Compliant Joint and Actuation
8.4. Performance Assessment
- Duration and speed: Maximum time and sustainable speed to perform the set of designed tasks with or without exoskeleton must be considered and compared.
- Ergonomics: Measuring the comfort level while wearing an exoskeleton must be considered.
- Pose uncertainty: It should provide a certain level of positioning accuracy and repeatability.
- Others: Cost, range of use, environment, and ease of use.
8.5. Adaptive Control
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bai, S.; Virk, G.S.; Sugar, T. Wearable Exoskeleton Systems: Design, Control and Applications; Institution of Engineering and Technology: London, UK, 2018. [Google Scholar]
- Kim, S.; Nussbaum, M.A.; Esfahani, M.I.M.; Alemi, M.M.; Jia, B.; Rashedi, E. Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part II–“Unexpected” effects on shoulder motion, balance, and spine loading. Appl. Ergon. 2018, 70, 323–330. [Google Scholar] [CrossRef]
- Carmeli, E.; Peleg, S.; Bartur, G.; Elbo, E.; Vatine, J.J. HandTutorTM enhanced hand rehabilitation after stroke—A pilot study. Physiother. Res. Int. 2011, 16, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.; Ingvast, J.; Wikander, J.; von Holst, H. The Soft Extra Muscle system for improving the grasping capability in neurological rehabilitation. In Proceedings of the IEEE-EMBS Conference on Biomedical Engineering and Sciences, Langkawi, Malaysia, 17–19 December 2012; pp. 412–417. [Google Scholar]
- Bianchi, M.; Fanelli, F.; Conti, R.; Governi, L.; Meli, E.; Ridolfi, A.; Rindi, A.; Vannetti, F.; Allotta, B. Design and Motion Analysis of a Wearable and Portable Hand Exoskeleton. In Wearable Robotics: Challenges and Trends, Proceedings of the 2nd International Symposium on Wearable Robotics, Segovia, Spain, 18–21 October 2016; Springer: Berlin, Germany, 2016; pp. 373–377. [Google Scholar]
- Kim, B.; Deshpande, A.D. An upper-body rehabilitation exoskeleton Harmony with an anatomical shoulder mechanism: Design, modeling, control, and performance evaluation. Int. J. Robot Res. 2017, 36, 414–435. [Google Scholar] [CrossRef]
- Christensen, S.; Bai, S. Kinematic Analysis and Design of a Novel Shoulder Exoskeleton Using a Double Parallelogram Linkage. J. Mech. Robot 2018, 10, 041008. [Google Scholar] [CrossRef]
- Groshaw, P. Hardiman I Arm Test, Hardiman I Prototype, General Electric Rep; Technical report S-70-1019; General Electric Co.: Schenectady, NY, USA, 1969. [Google Scholar]
- Kazerooni, H. Human-robot interaction via the transfer of power and information signals. IEEE Trans. Syst. Man Cybern. 1990, 20, 450–463. [Google Scholar] [CrossRef]
- Kawamoto, H.; Lee, S.; Kanbe, S.; Sankai, Y. Power assist method for HAL-3 using EMG-based feedback controller. In Proceedings of the 2003 IEEE International Conference on Systems, Man and Cybernetics, Conference Theme—System Security and Assurance (Cat. No.03CH37483), Washington, DC, USA, 8 October 2003; pp. 1648–1653. [Google Scholar]
- Islam, M.R.; Spiewak, C.; Rahman, M.H.; Fareh, R. A Brief Review on Robotic Exoskeletons for Upper Extremity Rehabilitation to Find the Gap between Research Porotype and Commercial Type. Adv. Robot Autom. 2017, 6, 408–417. [Google Scholar] [CrossRef]
- Young, A.J.; Ferris, D.P. State of the art and future directions for lower limb robotic exoskeletons. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 171–182. [Google Scholar] [CrossRef]
- Gopura, R.; Bandara, D.; Kiguchi, K.; Mann, G.K. Developments in hardware systems of active upper-limb exoskeleton robots: A review. Robot. Autom. Syst. 2016, 75, 203–220. [Google Scholar] [CrossRef]
- Bogue, R. Exoskeletons—A review of industrial applications. Ind. Robot. Int. J. 2018. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef]
- Stewart, A.M.; Pretty, C.G.; Adams, M.; Chen, X. Review of Upper Limb Hybrid Exoskeletons. IFAC-PapersOnLine 2017, 50, 15169–15178. [Google Scholar] [CrossRef]
- Jarrassé, N.; Proietti, T.; Crocher, V.; Robertson, J.; Sahbani, A.; Morel, G.; Roby-Brami, A. Robotic exoskeletons: A perspective for the rehabilitation of arm coordination in stroke patients. Front. Hum. Neurosci. 2014, 8, 947. [Google Scholar] [CrossRef] [PubMed]
- Engín, A. On the biomechanics of the shoulder complex. J. Biomech. 1980, 13, 575–590. [Google Scholar] [CrossRef]
- Pan, G.X.; Fu, H.Q.; Zhang, X.F.; Ma, F.L. Research on Bionic Mechanism of Shoulder Joint Rehabilitation Movement. In Wearable Sensors and Robots; Springer: Berlin, Germany, 2017; pp. 181–194. [Google Scholar]
- Stienen, A.H.; Hekman, E.E.; Van Der Helm, F.C.; Van Der Kooij, H. Self-aligning exoskeleton axes through decoupling of joint rotations and translations. IEEE Trans. Robot. 2009, 25, 628–633. [Google Scholar] [CrossRef]
- Prinold, J.A.; Masjedi, M.; Johnson, G.R.; Bull, A.M. Musculoskeletal shoulder models: A technical review and proposals for research foci. J. Eng. Med. 2013, 227, 1041–1057. [Google Scholar] [CrossRef] [PubMed]
- Copaci, D.; Flores, A.; Rueda, F.; Alguacil, I.; Blanco, D.; Moreno, L. Wearable elbow exoskeleton actuated with shape memory alloy. In Converging Clinical and Engineering Research on Neurorehabilitation II; Springer: Berlin, Germany, 2017; pp. 477–481. [Google Scholar]
- London, J. Kinematics of the elbow. J. Bone Jt. Surg. 1981, 63, 529–535. [Google Scholar] [CrossRef]
- Andrews, J.; Youm, Y. A biomechanical investigation of wrist kinematics. J. Biomech. 1979, 12, 83–93. [Google Scholar] [CrossRef]
- Neu, C.; Crisco, J., Jr.; Wolfe, S. In vivo kinematic behavior of the radio-capitate joint during wrist flexion–extension and radio-ulnar deviation. J. Biomech. 2001, 34, 1429–1438. [Google Scholar] [CrossRef]
- Gopura, R.; Kiguchi, K. Mechanical designs of active upper-limb exoskeleton robots: State-of-the-art and design difficulties. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 178–187. [Google Scholar]
- Ferguson, P.W.; Shen, Y.; Rosen, J. Hand Exoskeleton Systems—Overview. In Wearable Robotics; Elsevier: Amsterdam, The Netherlands, 2020; pp. 149–175. [Google Scholar]
- Proietti, T.; Crocher, V.; Roby-Brami, A.; Jarrassé, N. Upper-limb robotic exoskeletons for neurorehabilitation: A review on control strategies. IEEE Rev. Biomed. Eng. 2016, 9, 4–14. [Google Scholar] [CrossRef]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef]
- Yu, H.; Choi, I.S.; Han, K.L.; Choi, J.Y.; Chung, G.; Suh, J. Development of a upper-limb exoskeleton robot for refractory construction. Control Eng. Pract. 2018, 72, 104–113. [Google Scholar] [CrossRef]
- Lessard, S.; Pansodtee, P.; Robbins, A.; Baltaxe-Admony, L.B.; Trombadore, J.M.; Teodorescu, M.; Agogino, A.; Kurniawan, S. Crux: A compliant robotic upper-extremity exosuit for lightweight, portable, multi-joint muscular augmentation. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 1633–1638. [Google Scholar]
- Sui, D.; Fan, J.; Jin, H.; Cai, X.; Zhao, J.; Zhu, Y. Design of a wearable upper-limb exoskeleton for activities assistance of daily living. In Proceedings of the IEEE International Conference on Advanced Intelligent Mechatronics (AIM), Munich, Germany, 3–7 July 2017; pp. 845–850. [Google Scholar]
- Montaño, J.G.; Cena, C.E.G.; Chamorro, L.J.M.; Destarac, M.A.; Pazmiño, R.S. Mechanical Design of a Robotic Exoskeleton for Upper Limb Rehabilitation. In Advances in Automation and Robotics Research in Latin America; Springer: Berlin, Germany, 2017; pp. 297–308. [Google Scholar]
- Sharma, M.K.; Ordonez, R. Design and fabrication of an intention based upper-limb exo-skeleton. In Proceedings of the IEEE International Symposium on Intelligent Control (ISIC), Buenos Aires, Argentina, 19–22 September 2016; pp. 1–6. [Google Scholar]
- Wahyunggoro, O.; Nugroho, H.A. String actuated upper limb exoskeleton based on surface electromyography control. In Proceedings of the 2016 6th International Annual Engineering Seminar (InAES), Yogyakarta, Indonesia, 1–3 August 2016; pp. 176–181. [Google Scholar]
- Cui, X.; Chen, W.; Jin, X.; Agrawal, S.K. Design of a 7-DOF cable-driven arm exoskeleton (CAREX-7) and a controller for dexterous motion training or assistance. IEEE/ASME Trans. Mechatron. 2017, 22, 161–172. [Google Scholar] [CrossRef]
- Gunasekara, M.; Gopura, R.; Jayawardena, S. 6-REXOS: Upper limb exoskeleton robot with improved pHRI. Int. J. Adv. Robot. Syst. 2015, 12, 47. [Google Scholar] [CrossRef]
- EksoVest. Available online: https://eksobionics.com/eksoworks/ (accessed on 4 February 2020).
- Guardian XO. Available online: https://www.sarcos.com/products/guardian-xo/ (accessed on 4 February 2020).
- Bai, S.; Christensen, S.; Islam, M.R.U. An upper-body exoskeleton with a novel shoulder mechanism for assistive applications. In Proceedings of the 2017 IEEE International Conference on Advanced Intelligent Mechatronics (AIM), Munich, Germany, 3–7 July 2017; pp. 1041–1046. [Google Scholar]
- Hsieh, H.C.; Chen, D.F.; Chien, L.; Lan, C.C. Design of a Parallel Actuated Exoskeleton for Adaptive and Safe Robotic Shoulder Rehabilitation. IEEE/ASME Trans. Mechatron. 2017, 22, 2034–2045. [Google Scholar] [CrossRef]
- Lessard, S.; Pansodtee, P.; Robbins, A.; Trombadore, J.M.; Kurniawan, S.; Teodorescu, M. A soft exosuit for flexible upper-extremity rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1604–1617. [Google Scholar] [CrossRef] [PubMed]
- Vlachos, E.; Jochum, E.; Demers, L.P. HEAT: The harmony exoskeleton self-assessment test. In Proceedings of the 2018 27th IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Nanjing, China, 27–31 August 2018; pp. 577–582. [Google Scholar]
- Castro, M.N.; Rasmussen, J.; Andersen, M.S.; Bai, S. A compact 3-DOF shoulder mechanism constructed with scissors linkages for exoskeleton applications. Mech. Mach. Theory 2019, 132, 264–278. [Google Scholar] [CrossRef]
- Crea, S.; Cempini, M.; Moisè, M.; Baldoni, A.; Trigili, E.; Marconi, D.; Cortese, M.; Giovacchini, F.; Posteraro, F.; Vitiello, N. A novel shoulder-elbow exoskeleton with series elastic actuators. In Proceedings of the 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 June 2016; pp. 1248–1253. [Google Scholar]
- Ebrahimi, A.; Gröninger, D.; Singer, R.; Schneider, U. Control parameter optimization of the actively powered upper body exoskeleton using subjective feedbacks. In Proceedings of the 3rd International Conference on Control, Automation and Robotics (ICCAR), Nagoya, Japan, 24–26 April 2017; pp. 432–437. [Google Scholar]
- Mao, Y.; Agrawal, S.K. Transition from mechanical arm to human arm with CAREX: A cable driven ARm EXoskeleton (CAREX) for neural rehabilitation. In Proceedings of the 2012 IEEE International Conference on Robotics and Automation, Saint Paul, MN, USA, 14–18 May 2012; pp. 2457–2462. [Google Scholar]
- Madani, T.; Daachi, B.; Djouani, K. Modular-controller-design-based fast terminal sliding mode for articulated exoskeleton systems. IEEE Trans. Control Syst. Technol. 2017, 25, 1133–1140. [Google Scholar] [CrossRef]
- Jarrett, C.; McDaid, A. Robust control of a cable-driven soft exoskeleton joint for intrinsic human-robot interaction. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 976–986. [Google Scholar] [CrossRef]
- McDonald, C.G.; Dennis, T.A.; O’Malley, M.K. Characterization of surface electromyography patterns of healthy and incomplete spinal cord injury subjects interacting with an upper-extremity exoskeleton. In Proceedings of the International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 164–169. [Google Scholar]
- Khan, A.M.; Yun, D.W.; Ali, M.A.; Zuhaib, K.M.; Yuan, C.; Iqbal, J.; Han, J.; Shin, K.; Han, C. Passivity based adaptive control for upper extremity assist exoskeleton. Int. J. Control Autom. Syst. 2016, 14, 291–300. [Google Scholar] [CrossRef]
- Rosales, Y.; Lopez, R.; Rosales, I.; Salazar, S.; Lozano, R. Design and modeling of an upper limb exoskeleton. In Proceedings of the 2015 19th International Conference on System Theory, Control and Computing (ICSTCC), Cheile Gradistei, Romania, 14–16 October 2015; pp. 266–272. [Google Scholar]
- Mahdavian, M.; Toudeshki, A.G.; Yousefi-Koma, A. Design and fabrication of a 3DoF upper limb exoskeleton. In Proceedings of the 3rd RSI International Conference on Robotics and Mechatronics (ICROM), Tehran, Iran, 7–9 October 2015; pp. 342–346. [Google Scholar]
- Sutapun, A.; Sangveraphunsiri, V. A 4-DOF upper limb exoskeleton for stroke rehabilitation: Kinematics mechanics and control. Int. J. Mech. Eng. Robot. Res. 2015, 4, 269–272. [Google Scholar] [CrossRef]
- Beigzadeh, B.; Ilami, M.; Najafian, S. Design and development of one degree of freedom upper limb exoskeleton. In Proceedings of the 3rd RSI International Conference on Robotics and Mechatronics (ICROM), Tehran, Iran, 7–9 October 2015; pp. 223–228. [Google Scholar]
- Fitle, K.D.; Pehlivan, A.U.; O’Malley, M.K. A robotic exoskeleton for rehabilitation and assessment of the upper limb following incomplete spinal cord injury. In Proceedings of the IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 4960–4966. [Google Scholar]
- Klein, J.; Spencer, S.; Allington, J.; Bobrow, J.E.; Reinkensmeyer, D.J. Optimization of a parallel shoulder mechanism to achieve a high-force, low-mass, robotic-arm exoskeleton. IEEE Trans. Robot. 2010, 26, 710–715. [Google Scholar] [CrossRef]
- Rahman, M.; Ouimet, T.; Saad, M.; Kenné, J.; Archambault, P. Development and control of a wearable robot for rehabilitation of elbow and shoulder joint movements. In Proceedings of the IECON 2010-36th Annual Conference on IEEE Industrial Electronics Society, Glendale, AZ, USA, 7–10 November 2010; pp. 1506–1511. [Google Scholar]
- Garrec, P.; Friconneau, J.; Measson, Y.; Perrot, Y. ABLE, an innovative transparent exoskeleton for the upper-limb. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, Nice, France, 22–26 September 2008; pp. 1483–1488. [Google Scholar]
- Stadler, K.S.; Altenburger, R.; Schmidhauser, E.; Scherly, D.; Ortiz, J.; Toxiri, S.; Mateos, L.; Masood, J. Robo-mate an exoskeleton for industrial use—Concept and mechanical design. In Advances in Cooperative Robotics; World Scientific: Singapore, 2017; pp. 806–813. [Google Scholar]
- van der Vorm, J.; Nugent, R.; O’Sullivan, L. Safety and risk management in designing for the lifecycle of an exoskeleton: A novel process developed in the robo-mate project. Procedia Manuf. 2015, 3, 1410–1417. [Google Scholar] [CrossRef]
- Baltaxe-Admony, L.B.; Robbins, A.S.; Jung, E.A.; Lessard, S.; Teodorescu, M.; SunSpiral, V.; Agogino, A. Simulating the human shoulder through active tensegrity structures. In Proceedings of the International Design Engineering Technical Conferences and Computers and Information in Engineering Conference 2016, Charlotte, NC, USA, 21–24 August 2016; p. V006T09A027. [Google Scholar]
- de Oliveira, A.C.; Rose, C.G.; Warburton, K.; Ogden, E.M.; Whitford, B.; Lee, R.K.; Deshpande, A.D. Exploring the Capabilities of Harmony for Upper-Limb Stroke Therapy. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 637–643. [Google Scholar]
- Ghonasgi, K.; de Oliveira, A.C.; Shafer, A.; Rose, C.G.; Deshpande, A.D. Estimating the Effect of Robotic Intervention on Elbow Joint Motion. In Proceedings of the 2019 28th IEEE International Conference on Robot and Human Interactive Communication (RO-MAN), New Delhi, India, 14–18 October 2019; pp. 1–6. [Google Scholar]
- Nam, H.S.; Koh, S.; Kim, Y.J.; Beom, J.; Lee, W.H.; Lee, S.U.; Kim, S. Biomechanical Reactions of Exoskeleton Neurorehabilitation Robots in Spastic Elbows and Wrists. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2196–2203. [Google Scholar] [CrossRef] [PubMed]
- Accogli, A.; Grazi, L.; Crea, S.; Panarese, A.; Carpaneto, J.; Vitiello, N.; Micera, S. EMG-based detection of user’s intentions for human-machine shared control of an assistive upper-limb exoskeleton. In Wearable Robotics: Challenges and Trends; Springer: Berlin, Germany, 2017; pp. 181–185. [Google Scholar]
- Hunt, J.; Lee, H.; Artemiadis, P. A novel shoulder exoskeleton robot using parallel actuation and a passive slip interface. J. Mech. Robot. 2017, 9, 011002. [Google Scholar] [CrossRef]
- Crea, S.; Cempini, M.; Mazzoleni, S.; Carrozza, M.C.; Posteraro, F.; Vitiello, N. Phase-II clinical validation of a powered exoskeleton for the treatment of elbow spasticity. Front. Neurosci. 2017, 11, 261. [Google Scholar] [CrossRef]
- Shao, Z.F.; Tang, X.; Yi, W. Optimal design of a 3-DOF cable-driven upper arm exoskeleton. Adv. Mech. Eng. 2014, 6, 157096. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, X.; Du, F. Development and analysis of a gravity-balanced exoskeleton for active rehabilitation training of upper limb. J. Mech. Eng. Sci. 2016, 230, 3777–3790. [Google Scholar] [CrossRef]
- Hosseini, M.; Meattini, R.; Palli, G.; Melchiorri, C. A wearable robotic device based on twisted string actuation for rehabilitation and assistive applications. J. Robot. 2017, 2017, 1–11. [Google Scholar] [CrossRef]
- Pezent, E.; Rose, C.G.; Deshpande, A.D.; O’Malley, M.K. Design and characterization of the openwrist: A robotic wrist exoskeleton for coordinated hand-wrist rehabilitation. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 720–725. [Google Scholar]
- Ripel, T.; Krejsa, J.; Hrbacek, J.; Cizmar, I. Active elbow orthosis. Int. J. Adv. Robot. Syst. 2014, 11, 143. [Google Scholar] [CrossRef]
- Oguntosin, V.W.; Mori, Y.; Kim, H.; Nasuto, S.J.; Kawamura, S.; Hayashi, Y. Design and Validation of Exoskeleton Actuated by Soft Modules toward Neurorehabilitation—Vision-Based Control for Precise Reaching Motion of Upper Limb. Front. Neurosci. 2017, 11, 352. [Google Scholar] [CrossRef]
- Naidu, D.; Stopforth, R.; Bright, G.; Davrajh, S. A portable passive physiotherapeutic exoskeleton. Int. J. Adv. Robot. Syst. 2012, 9, 137. [Google Scholar] [CrossRef]
- Ruiz, A.F.; Rocon, E.; Forner-Cordero, A. Exoskeleton-based robotic platform applied in biomechanical modelling of the human upper limb. Appl. Bionics Biomech. 2009, 6, 205–216. [Google Scholar] [CrossRef][Green Version]
- Mihelj, M.; Podobnik, J.; Munih, M. HEnRiE-Haptic environment for reaching and grasping exercise. In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008; pp. 907–912. [Google Scholar]
- Sarac, M.; Solazzi, M.; Leonardis, D.; Sotgiu, E.; Bergamasco, M.; Frisoli, A. Design of an underactuated hand exoskeleton with joint estimation. In Advances in Italian Mechanism Science; Springer: Berlin, Germany, 2017; pp. 97–105. [Google Scholar]
- Lambelet, C.; Lyu, M.; Woolley, D.; Gassert, R.; Wenderoth, N. The eWrist—A wearable wrist exoskeleton with sEMG-based force control for stroke rehabilitation. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 726–733. [Google Scholar]
- Hadi, A.; Alipour, K.; Kazeminasab, S.; Elahinia, M. ASR glove: A wearable glove for hand assistance and rehabilitation using shape memory alloys. J. Intell. Mater. Syst. Struct. 2018, 29, 1575–1585. [Google Scholar] [CrossRef]
- Sale, P.; Stellin, G.; Masiero, S.; Becchi, F.; Sieklicki, W. FEX a Fingers Extending eXoskeleton for Rehabilitation and Regaining Mobility. In Proceedings of the International Conference on Robotics in Alpe-Adria Danube Region, Torino, Italy, 21–23 June 2017; pp. 813–824. [Google Scholar]
- Bundy, D.T.; Souders, L.; Baranyai, K.; Leonard, L.; Schalk, G.; Coker, R.; Moran, D.W.; Huskey, T.; Leuthardt, E.C. Contralesional brain–computer interface control of a powered exoskeleton for motor recovery in chronic stroke survivors. Stroke 2017, 48, 1908–1915. [Google Scholar] [CrossRef] [PubMed]
- Butler, N.R.; Goodwin, S.A.; Perry, J.C. Design parameters and torque profile modification of a spring-assisted hand-opening exoskeleton module. In Proceedings of the International Conference on Rehabilitation Robotics (ICORR, London, UK, 17–20 July 2017; pp. 591–596. [Google Scholar]
- Perry, J.C.; Trimble, S.; Machado, L.G.C.; Schroeder, J.S.; Belloso, A.; Rodriguez-de Pablo, C.; Keller, T. Design of a spring-assisted exoskeleton module for wrist and hand rehabilitation. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 594–597. [Google Scholar]
- Sandoval, G.O.; Jacinto-Villegas, J.; Herrera-Aguilar, I.; Portillo-Rodiguez, O.; Tripicchio, P.; Hernandez-Ramos, M.; Flores-Cuautle, A.; Avizzano, C. Design and development of a hand exoskeleton robot for active and passive rehabilitation. Int. J. Adv. Robot. Syst. 2016, 13, 66. [Google Scholar] [CrossRef]
- Rong, W.; Tong, K.Y.; Hu, X.L.; Ho, S.K. Effects of electromyography-driven robot-aided hand training with neuromuscular electrical stimulation on hand control performance after chronic stroke. Disabil. Rehabil. Assist. Technol. 2015, 10, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Hartopanu, S.; Poboroniuc, M.; Serea, F.; Irimia, D.; Livint, G. Design of a hybrid FES-mechanical intelligent haptic robotic glove. In Proceedings of the 17th International Conference System on Theory, Control and Computing (ICSTCC), Sinaia, Romania, 11–13 October 2013; pp. 687–692. [Google Scholar]
- Kawasaki, H.; Ito, S.; Nishimoto, Y.; Ueki, S.; Ishigure, Y.; Mouri, T. Hand Motion Assist Robot for Rehabilitation Therapy. JRM 2014, 26, 103–104. [Google Scholar] [CrossRef]
- Ferguson, P.W.; Dimapasoc, B.; Shen, Y.; Rosen, J. Design of a Hand Exoskeleton for Use with Upper Limb Exoskeletons. In Proceedings of the International Symposium on Wearable Robotics, Pisa, Italy, 16–20 October 2018; pp. 276–280. [Google Scholar]
- Abdallah, I.B.; Bouteraa, Y.; Rekik, C. Design and Development of 3D Printed Myoelectric Robotic Exoskeleton for Hand Rehabilitation. Int. J. Smart Sens. Intell. Syst. 2017, 10, 341. [Google Scholar] [CrossRef]
- Hu, X.; Tong, K.; Song, R.; Zheng, X.; Lui, K.; Leung, W.; Ng, S.; Au-Yeung, S. Quantitative evaluation of motor functional recovery process in chronic stroke patients during robot-assisted wrist training. J. Electromyogr. Kinesiol. 2009, 19, 639–650. [Google Scholar] [CrossRef]
- Helbok, R.; Schoenherr, G.; Spiegel, M.; Sojer, M.; Brenneis, C. Robot-assisted hand training (Amadeo) compared with conventional physiotherapy techniques in chronic ischemic stroke patients: A pilot study. In Proceedings of the DGNR, Bremen, Germany, 9–11 November 2010. [Google Scholar]
- Pirondini, E.; Coscia, M.; Marcheschi, S.; Roas, G.; Salsedo, F.; Frisoli, A.; Bergamasco, M.; Micera, S. Evaluation of a new exoskeleton for upper limb post-stroke neuro-rehabilitation: Preliminary results. In Replace, Repair, Restore, Relieve–Bridging Clinical and Engineering Solutions in Neurorehabilitation; Springer: Berlin, Germany, 2014; pp. 637–645. [Google Scholar]
- Van der Heide, L.A.; van Ninhuijs, B.; Bergsma, A.; Gelderblom, G.J.; van der Pijl, D.J.; de Witte, L. An overview and categorization of dynamic arm supports for people with decreased arm function. Prosthetics Orthot. Int. 2014, 38, 4. [Google Scholar] [CrossRef]
- Brahmi, B.; Saad, M.; Rahman, M.H.; Ochoa-Luna, C. Cartesian trajectory tracking of a 7-DOF exoskeleton robot based on human inverse kinematics. IEEE Trans. Syst. Man Cybern. Syst. 2017, 49, 600–611. [Google Scholar] [CrossRef]
- Lenzi, T.; De Rossi, S.; Vitiello, N.; Chiri, A.; Roccella, S.; Giovacchini, F.; Vecchi, F.; Carrozza, M.C. The neuro-robotics paradigm: NEURARM, NEUROExos, HANDEXOS. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 2430–2433. [Google Scholar]
- Cempini, M.; Giovacchini, F.; Vitiello, N.; Cortese, M.; Moisé, M.; Posteraro, F.; Carrozza, M.C. NEUROExos: A powered elbow orthosis for post-stroke early neurorehabilitation. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 342–345. [Google Scholar]
- Skelex. Available online: https://www.skelex.com/ (accessed on 4 February 2020).
- Ergosquelettes. Available online: https://gobio-robot.com/ (accessed on 4 February 2020).
- MAX by SUIT X. Available online: https://www.suitx.com/ (accessed on 4 February 2020).
- MyoPro Orthosis. Available online: https://myomo.com (accessed on 4 February 2020).
- ALEx Arm. Available online: http://www.wearable-robotics.com/kinetek/ (accessed on 4 February 2020).
- Lee, H.; Kang, B.B.; In, H.; Cho, K.J. Design Improvement of a Polymer-Based Tendon-Driven Wearable Robotic Hand (Exo-Glove Poly). In Wearable Robotics: Challenges and Trends; Springer: Berlin, Germany, 2017; pp. 95–99. [Google Scholar]
- SEM Glove. Available online: https://www.bioservo.com/ (accessed on 4 February 2020).
- Hercule Exoskeleton. Available online: https://www.rb3d.com/en/exoskeletons/ (accessed on 4 February 2020).
- Hand of Hope. Available online: http://www.rehab-robotics.com/index.html (accessed on 4 February 2020).
- ReoGO. Available online: http://motorika.com/reogo/ (accessed on 4 February 2020).
- Armotion. Available online: https://www.rehatechnology.com/en/products/armotion (accessed on 4 February 2020).
- AMENDEO Hand. Available online: https://tyromotion.com/en/ (accessed on 4 February 2020).
- Robot, I.A. Interactive Motion Technologies; Bionik, Inc.: Watertown, MA, USA, 2012. [Google Scholar]
- Wagner, T.H.; Lo, A.C.; Peduzzi, P.; Bravata, D.M.; Huang, G.D.; Krebs, H.I.; Ringer, R.J.; Federman, D.G.; Richards, L.G.; Haselkorn, J.K.; et al. An economic analysis of robot-assisted therapy for long-term upper-limb impairment after stroke. Stroke 2011, 42, 2630–2632. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Guo, S.; Pang, M.; Zhang, S.; Xiao, N.; Gao, B.; Shi, L. Implementation of resistance training using an upper-limb exoskeleton rehabilitation device for elbow joint. J. Med. Biol. Eng. 2014, 34, 188–196. [Google Scholar] [CrossRef]
- Huang, V.S.; Krakauer, J.W. Robotic neurorehabilitation: A computational motor learning perspective. J. Neuroeng. Rehabil. 2009, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Wei, R.; Perez, M.; Shepard, B.; Koeneman, E.; Koeneman, J.; He, J. RUPERT: An exoskeleton robot for assisting rehabilitation of arm functions. In Proceedings of the Virtual Rehabilitation, Vancouver, BC, Canada, 25–27 August 2008; pp. 163–167. [Google Scholar] [CrossRef]
- Garrido, J.; Yu, W.; Soria, A. Modular design and modeling of an upper limb exoskeleton. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; pp. 508–513. [Google Scholar] [CrossRef]
- Otten, A.; Voort, C.; Stienen, A.; Aarts, R.; van Asseldonk, E.; van der Kooij, H. LIMPACT: A hydraulically powered self-aligning upper limb exoskeleton. IEEE/ASME Trans. Mechatron. 2015, 20, 2285–2298. [Google Scholar] [CrossRef]
- Staubli, P.; Nef, T.; Klamroth-Marganska, V.; Riener, R. Effects of intensive arm training with the rehabilitation robot ARMin II in chronic stroke patients: Four single-cases. J. Neuroeng. Rehabil. 2009, 6, 46. [Google Scholar] [CrossRef] [PubMed]
- Pignolo, L.; Dolce, G.; Basta, G.; Lucca, L.; Serra, S.; Sannita, W. Upper limb rehabilitation after stroke: ARAMIS a “robo-mechatronic” innovative approach and prototype. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1410–1414. [Google Scholar] [CrossRef]
- Mayr, A.; Kofler, M.; Saltuari, L. ARMOR: Elektromechanischer Roboter für das Bewegungstraining der oberen Extremität nach Schlaganfall. Prospektive randomisierte kontrollierte Pilotstudie. Handchir. Mikrochir. Plast. Chir. 2008, 40, 66–73. [Google Scholar] [CrossRef]
- Klein, J.; Spencer, S.; Allington, J.; Minakata, K.; Wolbrecht, E.; Smith, R.; Bobrow, J.; Reinkensmeyer, D. Biomimetic orthosis for the neurorehabilitation of the elbow and shoulder (BONES). In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008; pp. 535–541. [Google Scholar] [CrossRef]
- Winstein, C.J.; Kay, D.B. Translating the science into practice: Shaping rehabilitation practice to enhance recovery after brain damage. Prog. Brain Res. 2015, 218, 331–360. [Google Scholar] [CrossRef]
- Manna, S.K.; Bhaumik, S. A Bioinspired 10 DOF wearable powered arm exoskeleton for rehabilitation. J. Robot. 2013. [Google Scholar] [CrossRef]
- Mehdi, H.; Boubaker, O. Stiffness and impedance control using Lyapunov theory for robot-aided rehabilitation. Int. J. Soc. Robot. 2012, 4, 107–119. [Google Scholar] [CrossRef]
- Krebs, H.I.; Ferraro, M.; Buerger, S.P.; Newbery, M.J.; Makiyama, A.; Sandmann, M.; Lynch, D.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Pilot trial of a spatial extension for MIT-Manus. J. Neuroeng. Rehabil. 2004, 1, 5. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.; Liu, Q.; Zhou, Z.; Ai, Q.; Sheng, B.; Xie, S.S. Recent development of mechanisms and control strategies for robot-assisted lower limb rehabilitation. Mechatronics 2015, 31, 132–145. [Google Scholar] [CrossRef]
- Kiguchi, K.; Hayashi, Y. An EMG-based control for an upper-limb power-assist exoskeleton robot. IEEE Trans. Syst. Man Cybern. Part Cybern. 2012, 42, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Gopura, R.A.R.C.; Kiguchi, K.; Li, Y. SUEFUL-7: A 7DOF upper-limb exoskeleton robot with muscle-model-oriented EMG-based control. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MO, USA, 10–15 October 2009; pp. 1126–1131. [Google Scholar] [CrossRef]
- Guidali, M.; Duschau-Wicke, A.; Broggi, S.; Klamroth-Marganska, V.; Nef, T.; Riener, R. A robotic system to train activities of daily living in a virtual environment. Med. Biol. Eng. Comput. 2011, 49, 1213. [Google Scholar] [CrossRef] [PubMed]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Kumar, S.; Wöhrle, H.; Trampler, M.; Simnofske, M.; Peters, H.; Mallwitz, M.; Kirchner, E.A.; Kirchner, F. Modular Design and Decentralized Control of the Recupera Exoskeleton for Stroke Rehabilitation. Appl. Sci. 2019, 9, 626. [Google Scholar] [CrossRef]
- Mallwitz, M.; Will, N.; Teiwes, J.; Kirchner, E.A. The capio active upper body exoskeleton and its application for teleoperation. In Proceedings of the 13th Symposium on Advanced Space Technologies in Robotics and Automation. ESA/ESTEC Symposium on Advanced Space Technologies in Robotics and Automation (ASTRA-2015), Noordwijk, The Netherlands, 11–13 May 2015. [Google Scholar]
- Fleischer, C.; Kondak, K.; Wege, A.; Kossyk, I. Research on Exoskeletons at the TU Berlin. In Advances in Robotics Research; Springer: Berlin, Germany, 2009; pp. 335–346. [Google Scholar]
- Li, Z.; Bai, S. A novel revolute joint of variable stiffness with reconfigurability. Mech. Mach. Theory 2019, 133, 720–736. [Google Scholar] [CrossRef]
- Calanca, A.; Muradore, R.; Fiorini, P. A review of algorithms for compliant control of stiff and fixed-compliance robots. IEEE/ASME Trans. Mechatron. 2015, 21, 613–624. [Google Scholar] [CrossRef]
- Pylatiuk, C.; Kargov, A.; Gaiser, I.; Werner, T.; Schulz, S.; Bretthauer, G. Design of a flexible fluidic actuation system for a hybrid elbow orthosis. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 167–171. [Google Scholar] [CrossRef]
- Siciliano, B.; Khatib, O. Springer Handbook of Robotics; Springer: Berlin, Germany, 2016. [Google Scholar]
- Sun, Z.S.; Guo, Z.H.; Tang, W. Design of wearable hand rehabilitation glove with soft hoop-reinforced pneumatic actuator. J. Cent. South Univ. 2019, 26, 106–119. [Google Scholar] [CrossRef]
- Bai, S.; Rasmussen, J. Modelling of physical human-robot interaction for exoskeleton designs. In Proceedings of the Multibody Dynamics 2011, ECCOMAS Thematic Conference, Brussels, Belgium, 4–7 July 2011. [Google Scholar]
- Khatib, O.; Demircan, E.; De Sapio, V.; Sentis, L.; Besier, T.; Delp, S. Robotics-based synthesis of human motion. J.-Physiol.-Paris 2009, 103, 211–219. [Google Scholar] [CrossRef]
- Damsgaard, M.; Rasmussen, J.; Christensen, S.T.; Surma, E.; De Zee, M. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simul. Model. Pract. Theory 2006, 14, 1100–1111. [Google Scholar] [CrossRef]
- Chao, E.Y.; Armiger, R.S.; Yoshida, H.; Lim, J.; Haraguchi, N. Virtual interactive musculoskeletal system (VIMS) in orthopaedic research, education and clinical patient care. J. Orthop. Surg. Res. 2007, 2, 2. [Google Scholar] [CrossRef] [PubMed]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef] [PubMed]
- Braghin, F.; Cheli, F.; Mantegazza, P.; Masarati, P.; Quaranta, G. Multibody dynamics teaching experience at Politecnico di Milano. In Proceedings of the Primo Workshop sulla Dinamica dei Sistemi Multibody, Paestum, Italy, 27–28 Apri 2006; pp. 27–28. [Google Scholar]
- Laitenberger, M.; Raison, M.; Périé, D.; Begon, M. Refinement of the upper limb joint kinematics and dynamics using a subject-specific closed-loop forearm model. Multibody Syst. Dyn. 2015, 33, 413–438. [Google Scholar] [CrossRef]
- Zhou, L.; Li, Y.; Bai, S. A human-centered design optimization approach for robotic exoskeletons through biomechanical simulation. Robot. Auton. Syst. 2017, 91, 337–347. [Google Scholar] [CrossRef]
- Tröster, M.; Schneider, U.; Bauernhansl, T.; Rasmussen, J.; Andersen, M.S. Simulation Framework for Active Upper Limb Exoskeleton Design Optimization Based on Musculoskeletal Modeling. Available online: https://vbn.aau.dk/ws/portalfiles/portal/292649860/M.Tr_ster_SmartASSIST_2018_02112018_Paper_32.pdf (accessed on 4 February 2020).
- Zhang, F.; Wang, X.; Fu, Y.; Agrawal, S.K. A human-robot interaction modeling approach for hand rehabilitation exoskeleton using biomechanical technique. In Proceedings of the 2015 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Hamburg, Germany, 28 September–2 October 2015; pp. 5593–5598. [Google Scholar] [CrossRef]
- Jensen, E.F.; Raunsbæk, J.; Lund, J.N.; Rahman, T.; Rasmussen, J.; Castro, M.N. Development and simulation of a passive upper extremity orthosis for amyoplasia. J. Rehabil. Assist. Technol. Eng. 2018, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Li, X.; Angeles, J. A review of spherical motion generation using either spherical parallel manipulators or spherical motors. Mech. Mach. Theory 2019, 140, 377–388. [Google Scholar] [CrossRef]
- Esmaeili, M.; Jarrassé, N.; Dailey, W.; Burdet, E.; Campolo, D. Hyperstaticity for ergonomie design of a wrist exoskeleton. In Proceedings of the 2013 IEEE International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–6. [Google Scholar] [CrossRef]
- Kawanishi, Y.; Oka, K.; Tanaka, H.; Okada, K.; Sugamoto, K.; Murase, T. In vivo 3-dimensional kinematics of thumb carpometacarpal joint during thumb opposition. J. Hand Surg. 2018, 43, 182.e1–182.e7. [Google Scholar] [CrossRef]
- Lee, H.D.; Lee, B.K.; Kim, W.S.; Han, J.S.; Shin, K.S.; Han, C.S. Human–robot cooperation control based on a dynamic model of an upper limb exoskeleton for human power amplification. Mechatronics 2014, 24, 168–176. [Google Scholar] [CrossRef]
- Varghese, R.J.; Mukherjee, G.; King, R.; Keller, S.; Deshpande, A.D. Designing Variable Stiffness Profiles to Optimize the Physical Human Robot Interface of Hand Exoskeletons. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 26–29 August 2018; pp. 1101–1108. [Google Scholar]
- Yun, Y.; Dancausse, S.; Esmatloo, P.; Serrato, A.; Merring, C.A.; Agarwal, P.; Deshpande, A.D. Maestro: An EMG-driven assistive hand exoskeleton for spinal cord injury patients. In Proceedings of the 2017 IEEE International Conference on Robotics and Automation (ICRA), Singapore, 29 May–3 June May 2017; pp. 2904–2910. [Google Scholar]
- Schiele, A. Fundamentals of Ergonomic Exoskeleton Robots. Ph.D. Thesis, Mechanical Maritime and Materials Engineering, University of Applied Sciences Kaiserslautern, Geboren te Bad Bergzabern, Kaiserslautern, Germany, 2008. [Google Scholar]
- Lee, H.; Kim, W.; Han, J.; Han, C. The technical trend of the exoskeleton robot system for human power assistance. Int. J. Precis. Eng. Manuf. 2012, 13, 1491–1497. [Google Scholar] [CrossRef]
- Anam, K.; Al-Jumaily, A.A. Active exoskeleton control systems: State of the art. Procedia Eng. 2012, 41, 988–994. [Google Scholar] [CrossRef]
- Bengtson, S.H.; Bak, T.; Andreasen Struijk, L.N.; Moeslund, T.B. Andreasen Struijk, L.N.; Moeslund, T.B. A review of computer vision for semi-autonomous control of assistive robotic manipulators (ARMs). In Disability and Rehabilitation: Assistive Technology; Taylor & Francis: Abingdon, UK, 2019; pp. 1–15. [Google Scholar]
- Gunasekara, J.; Gopura, R.; Jayawardane, T.; Lalitharathne, S. Control methodologies for upper limb exoskeleton robots. In Proceedings of the 2012 IEEE/SICE International Symposium on System Integration (SII), Fukuoka, Japan, 16–18 December 2012; pp. 19–24. [Google Scholar] [CrossRef]
- Singh, R.M.; Chatterji, S.; Kumar, A. Trends and challenges in EMG based control scheme of exoskeleton robots—A review. Int. Sci. Eng. Res. 2012, 3, 933–940. [Google Scholar]
- Islam, M.R.U.; Bai, S. Intention detection for dexterous human arm motion with FSR sensor bands. In Proceedings of the Companion of the 2017 ACM/IEEE International Conference on Human-Robot Interaction, Vienna, Austria, 6–9 March 2017; pp. 139–140. [Google Scholar] [CrossRef]
- Xiao, Z.G.; Menon, C. An Investigation on the Sampling Frequency of the Upper-Limb Force Myographic Signals. Sensors 2019, 19, 2432. [Google Scholar] [CrossRef]
- Islam, M.R.; Xu, K.; Bai, S. Position Sensing and Control with FMG Sensors for Exoskeleton Physical Assistance. In Proceedings of the 4th WeRob2018, Pisa, Italy, 16–20 October 2018; Springer: Berlin; Springer: Berlin, Germany, 2018; pp. 3–7. [Google Scholar]
- Islam, M.R.U.; Bai, S. Payload estimation using forcemyography sensors for control of upper-body exoskeleton in load carrying assistance. Model. Identif. Control 2019, 40, 189–198. [Google Scholar] [CrossRef]
- De Rossi, S.M.M.; Vitiello, N.; Lenzi, T.; Ronsse, R.; Koopman, B.; Persichetti, A.; Vecchi, F.; Ijspeert, A.J.; Van der Kooij, H.; Carrozza, M.C. Sensing pressure distribution on a lower-limb exoskeleton physical human-machine interface. Sensors 2011, 11, 207–227. [Google Scholar] [CrossRef]
- Yandell, M.B.; Quinlivan, B.T.; Popov, D.; Walsh, C.; Zelik, K.E. Physical interface dynamics alter how robotic exosuits augment human movement: Implications for optimizing wearable assistive devices. J. Neuroeng. Rehabil. 2017, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Rose, C.G.; Kann, C.K.; Deshpande, A.D.; O’Malley, M.K. Estimating anatomical wrist joint motion with a robotic exoskeleton. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 1437–1442. [Google Scholar]
- NeoMano. Available online: https://neomano.neofect.com/ (accessed on 4 February 2020).
- Tendo. Available online: https://www.tendoforpeople.se/tendo (accessed on 4 February 2020).
- Balasubramanian, S.; Klein, J.; Burdet, E. Robot-assisted rehabilitation of hand function. Curr. Opin. Neurol. 2010, 23, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Heo, P.; Gu, G.M.; Lee, S.J.; Rhee, K.; Kim, J. Current hand exoskeleton technologies for rehabilitation and assistive engineering. Int. J. Precis. Eng. Manuf. 2012, 13, 807–824. [Google Scholar] [CrossRef]
- Yue, Z.; Zhang, X.; Wang, J. Hand rehabilitation robotics on poststroke motor recovery. Behav. Neurol. 2017, 2017, 3908135. [Google Scholar] [CrossRef]
- Chu, C.Y.; Patterson, R.M. Soft robotic devices for hand rehabilitation and assistance: A narrative review. J. Neuroeng. Rehabil. 2018, 15, 9. [Google Scholar] [CrossRef]
- Sarac, M.; Solazzi, M.; Frisoli, A. Design Requirements of Generic Hand Exoskeletons and Survey of Hand Exoskeletons for Rehabilitation, Assistive, or Haptic Use. IEEE Trans. Haptics 2019, 12, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Carpino, G.; Accoto, D.; Sergi, F.; Luigi Tagliamonte, N.; Guglielmelli, E. A novel compact torsional spring for series elastic actuators for assistive wearable robots. J. Mech. Des. 2012, 134. [Google Scholar] [CrossRef]
- del Carmen Sanchez-Villamañan, M.; Gonzalez-Vargas, J.; Torricelli, D.; Moreno, J.C.; Pons, J.L. Compliant lower limb exoskeletons: A comprehensive review on mechanical design principles. J. Neuroeng. Rehabil. 2019, 16, 55. [Google Scholar] [CrossRef]
- Grosu, V.; Rodriguez-Guerrero, C.; Grosu, S.; Vanderborght, B.; Lefeber, D. Design of smart modular variable stiffness actuators for robotic-assistive devices. IEEE/ASME Trans. Mechatron. 2017, 22, 1777–1785. [Google Scholar] [CrossRef]
- Mussa-Ivaldi, F.A.; Hogan, N.; Bizzi, E. Neural, mechanical, and geometric factors subserving arm posture in humans. J. Neurosci. 1985, 5, 2732–2743. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, T.; Virk, G.S. ISO 13482-The new safety standard for personal care robots. In Proceedings of the 41st International Symposium on Robotics ISR/Robotik 2014, Munich, Germany, 2–3 June 2014; pp. 1–6. [Google Scholar]
- Bostelman, R.; Li-Baboud, Y.S.; Virts, A.; Yoon, S.; Shah, M. Towards Standard Exoskeleton Test Methods for Load Handling. In Proceedings of the 2019 Wearable Robotics Association Conference (WearRAcon), Scottsdale, AZ, USA, 25–27 July 2019; pp. 21–27. [Google Scholar] [CrossRef]
- Bostelman, R.; Hong, T. Test methods for exoskeletons—Lessons learned from industrial and response robotics. Wearable Exoskeleton Syst. Des. Control Appl. 2018, 13, 335–361. [Google Scholar] [CrossRef]
- Mghames, S.; Laghi, M.; Della Santina, C.; Garabini, M.; Catalano, M.; Grioli, G.; Bicchi, A. Design, control and validation of the variable stiffness exoskeleton flexo. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 539–546. [Google Scholar] [CrossRef]
- Leonardis, D.; Barsotti, M.; Loconsole, C.; Solazzi, M.; Troncossi, M.; Mazzotti, C.; Castelli, V.P.; Procopio, C.; Lamola, G.; Chisari, C.; et al. An EMG-controlled robotic hand exoskeleton for bilateral rehabilitation. IEEE Trans. Haptics 2015, 8, 140–151. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exoskeleton Name | Supported Movements | Degrees of Freedom | Main Control Input | Type of Actuators | References |
|---|---|---|---|---|---|
| AAU Upperbody Exo. | Shoulder (EF, AA, IE), Forearm (EF) | 3-Active 1-Passive | FSR | Maxon DC motor | Bai et al. [7] |
| Upper limb exoskeleton | Shoulder (EF, AA, IE), Forearm (EF) | 6-Active | Force/Torque sensors | DC motor | Yu et al. [30] |
| CRUX | Shoulder Abduction, Forearm (EF, PS) | 3-Active | Joystick | DC motor | Lessard et al. [42] |
| Wearable upper limb exoskeleton | Shoulder (EF, IE, AA), Elbow (EF, PS) | 5-Active | Joint angle | Cable driven mechanism using BLDC | Sui et al. [32] |
| Stuttgart Exo Jacket | Shoulder (EF, AA), Elbow (EF) | 3-Active 9-Passive | Force Sensors | EC Motor with Spring mechanism | Ebrahimi et al. [46] |
| ULEL | Shoulder (EF), Forearm (EF), Wrist (EF) | 3-Active | EMG | BLDC | Madani et al. [48] |
| Cable driven Soft exoskeleton | Elbow (EF) | 1-Active | Joint angle control | Cable driven | Jarrett et al. [49] |
| Upper limb robotic Exo. | Shoulder (EF, AA, IE), Forearm (PS), Elbow (EF, humeral rotation) | 6-Active | Joint angle | Servo motor | Montano et al. [33] |
| MAHI EXO-II | Forearm (EF, PS), Wrist (EF, rotation) | 4-single DOF 2-Multi DOF | EMG | DC motor | McDonald et al. [50] |
| Upper limb exoskeleton | Shoulder (EF, AA), Forearm (EF, PS) | 3-Active | Joint angle | DC motor | Sharma et al. [34] |
| String actuated exoskeleton | Shoulder (EF), Elbow (EF) | 2-Active | EMG | String actuated | Wahyunggoro et al. [35] |
| Upper limb exoskeleton | Shoulder (EF), Elbow (EF) | 2-Active | Load cell | DC motor | Khan et al. [51] |
| Upper limb exoskeleton | Shoulder (AA, EF, rotation) | 3-Active | - | DC motor | Rosales et al. [52] |
| Upper limb exoskeleton | Shoulder (AA, EF), Forearm (EF) | 3-Active | Impedance control | Servo motor | Mahdavian et al. [53] |
| Upper limb exoskeleton | Shoulder (AA, EF, rotation),Forearm (EF) | 4-Active | Impedance control | Maxon EC 90 | Sutapun et al. [54] |
| CAREX -7 | Shoulder (EF, AA, rotation), Elbow (EF), Wrist (EF, AA, rotation) | 7-Active | Joint angle | Cables driven by motor | Cui et al. [36] |
| 6-REXOS | Elbow (EF, redundant), Forearm (PS), Wrist (EF, UR, redundant) | 4-Active 2-Passive | pHRI | DC motor | Gunasekara et al. [37] |
| Upper limb exoskeleton | Elbow (EF) | 1-Active | EMG | DC motor | Beigzadeh et al. [55] |
| MAHI | Forearm (EF, PS), Wrist (RU, EF) | 5-Active | Admittance control | Frameless DC motor | Fitle et al. [56] |
| BONES | Shoulder (EF, AA rotation), Elbow (EF) | 4-Active | Force control | Pneumatic actuators | Klein et al. [57] |
| ExoRob | Forearm (EF, PS), Wrist (EF, RU) | 4-Active | Sliding mode control | Maxon EC-45 | Rahman et al. [58] |
| ABLE | Shoulder (EF, AA, rotation), Elbow (EF) | 4-Active | Force feedback control | Screw-cable transmission | Garrec et al. [59] |
| Exoskeleton Name | Supported Movements | Degrees of Freedom | Main Control Input | Type of Actuators | References |
|---|---|---|---|---|---|
| Upper body Exoskeleton Harmony | Shoulder (EF, AA, IE rotation), 2DOF for Shoulder girdle Elbow (EF, PS) | 7-Active | Trajectory tracking with impedance control | SEA based actuators | Kim et al. [6,63,64] |
| Spastic elbow and wrist Exoskeleton | Elbow (EF) Wrist (EF) | 2-Active | Joint angle | DC Maxon motor | Nam et al. [65] |
| NESM | Shoulder (EF, AA, IE rotation), Elbow (EF) | 4- Active 8-Passive | EMG | Brushless DC motor | Accogli et al. [66] |
| Parallel actuated Exo for shoulder joint | Shoulder pitch and yaw | 2-Active 4-Passive | Force sensors | DC motor | Hsieh et al. [41] |
| Parallel actuated shoulder exoskeleton | Shoulder (EF, AA, rotation), 2-DOF Passive Slip joint at shoulder | 3-Active 2-Passive | Joint angle | DC motor | Hunt et al. [67] |
| NEURO-Exos elbow module | Elbow (EF) | 1-Active | Joint angle | Maxon DC motor | Crea et al. [68] |
| Upper arm exoskeleton | Shoulder (AA, EF), Elbow (EF) | 3-Active | Joint angle | Cable driven | Shao et al. [69] |
| Gravity balanced exoskeleton | Shoulder EF, AA, IE Elbow (EF, PS) | 4-Active 1-Passive | Joint angle | Brushless servos | Wu et al. [70] |
| Wearable elbow exoskeleton | Elbow (EF, PS) | 2-Passive | Joint angle | SMA | Copaci et al. [22] |
| Wearable robotic device | Elbow (EF) | 1-Active | EMG | Twisted string actuation | Hosseini et al. [71] |
| Robotic wrist exoskeleton | Forearm (PS) Wrist (EF, rotation) | 3-Active | Joint angle | Brushed DC motor | Pezent et al. [72] |
| Active elbow orthosis | Elbow (EF) | 1-Active | Strain gauge | Maxon DC motor | Ripel et al. [73] |
| EAsoftM exoskeleton | Elbow (2-Passive DOF) Wrist (2-Active DOF) | 2-Passive 2-Active | Visual based control | Pneumatic actuator | Oguntosin et al. [74] |
| Passive physio therapeutic exoskeleton | Shoulder (AA, EF, rotation), Elbow (EF), Wrist (PS) | 7-Passive | Joint angle | - | Naidu et al. [75] |
| WOTAS | Forearm (PS, EF), Wrist (RU) | 3-Active | Impedance control | Brushless DC motor | Ruiz et al. [76] |
| HEnRiE | 3-DOF Shoulder Elbow (EF), Wrist (EF, AA) | 5-Active | End-effector velocity control | DC motor | Mihelj et al. [77] |
| Under actuated Hand exoskeleton | Under actuated hand (EF) | 4-Active | Joint angle | DC motor | Sarac et al. [78] |
| The eWrist | Wrist extension | 1-Active | sEMG | DC motor | Lambelet et al. [79] |
| ASR Glove | Finger (MCP, PIP, DIP) | 3-Active for each finger | Force sensor | Shape memory alloy | Hadi et al. [80] |
| FEX | Palm (Op/Cl) | 4-Active | Force sensors | DC motor | Sale et al. [81] |
| Portable hand Exo | 4 X Fingers (EF) | 4-Active | Joint angle | DC servo motor | Bianchi et al. [5] |
| BCI powered exoskeleton | 3 X Fingers pinchGrip (Op/Cl) | 1-Active | EEG | DC motor | Bundy et al. [82] |
| Spring assisted hand exoskeleton | Hand Grasping, Wrist (PS) | Not Given | Joint angle | Springs | Butler [83] |
| Spring-assisted exoskeleton module | Fingers (EF), Thumb (EF, AA) | 3-Passive | Joint angle | - | Perry et al. [84] |
| ExoK’ab 2016 | Palm (Op/Cl) | 6-DOF | Force sensors | DC motor | Sandoval et al. [85] |
| NMES-Robot hand | Grasping | Fingers | EMG | Linear actuator | Rong et al. [86] |
| Haptic robotic glove | Grasping | All Fingers | FES | Pneumatic drive | Hartopanu et al. [87] |
| Hand motion assist robot for therapy | Wrist and fingers | 18-DOF | - | - | Kawasaki et al. [88] |
| Hand exoskeleton | Grasping, pointing & pincer | 6-Active 6-Passive | Admittance control | Bowden cables with BLDC | Ferguson et al. [89] |
| Myoelectric Hand Exoskeleton | Hand (Op/Cl) | 5-Active 10-Passive | EMG | Servo motor | Abdallah et al. [90] |
| Robot-assisted wrist | Wrist (FE) | 1-Active | EMG | - | Hu et al. [91] |
| Company | Product | Application | Reference |
|---|---|---|---|
| RoboMate | Passive parallelogram arm Active parallelogram arm | Assistance power amplification | Stadler et al. [60] |
| GOBIO | Ergosquelettes | Assistance | www.gobio-robot.com [99] |
| Ekso Bionics | EksoVest | Passive Assistance | https://eksobionics.com/eksoworks/ [38] |
| SARCO | Guardian XO | Assistance | www.sarcos.com/products/guardian-xo/ [39] |
| SUIT X | MAX | Assistance (Reduce force at back shoulder) | www.suitx.com [100] |
| RB3D | Hercule Exoskeleton | Assistance (Industrial tool handling) | www.rb3d.com/en/exoskeletons [105] |
| BioServo | Iron hand & SEM glove | Assistance/rehabilitation | Nilsson et al. [4] |
| Rehab-Robotics | Hand of hope | Post stroke rehabilitation | www.rehab-robotics.com/index.html [106] |
| FOCAL meditech | Dynamic arm support | Rehabilitation | Meditech dynamic [94] |
| Kinetek | ALEx Arm | Assistance/rehabilitation | www.wearable-robotics.com/kinetek [102] |
| MediTouch | ArmTutor | Rehabilitation | Carmeli et al. [3] |
| Motorika Medical | ReoGO | Therapy | www.motorika.com/reogo [107] |
| REHA Technology | Armotion | Therapy | www.rehatechnology.com/en/products/armotion [108] |
| Tyromotion | AMENDEO Hand | Therapy | tyromotion.com/en/ [109] |
| BIONIK | InMotion Arm | Therapy | Robot et al. [110] |
| Myomo | MyoPro Orthosis | Therapy | www.myomo.com [101] |
| Sr. | Assistive Mode | Corrective Mode | Resistive Mode |
|---|---|---|---|
| 1. | Passive control a. Passive trajectory tracking b. Passive mirroring | Tunneling | No control development for exoskeletons |
| 2. | Partially assistive control a. Impedance/admittance control |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gull, M.A.; Bai, S.; Bak, T. A Review on Design of Upper Limb Exoskeletons. Robotics 2020, 9, 16. https://doi.org/10.3390/robotics9010016
Gull MA, Bai S, Bak T. A Review on Design of Upper Limb Exoskeletons. Robotics. 2020; 9(1):16. https://doi.org/10.3390/robotics9010016
Chicago/Turabian StyleGull, Muhammad Ahsan, Shaoping Bai, and Thomas Bak. 2020. "A Review on Design of Upper Limb Exoskeletons" Robotics 9, no. 1: 16. https://doi.org/10.3390/robotics9010016
APA StyleGull, M. A., Bai, S., & Bak, T. (2020). A Review on Design of Upper Limb Exoskeletons. Robotics, 9(1), 16. https://doi.org/10.3390/robotics9010016