

Human Factors Assessment of a Novel Pediatric Lower-Limb Exoskeleton


Abstract
:1. Introduction
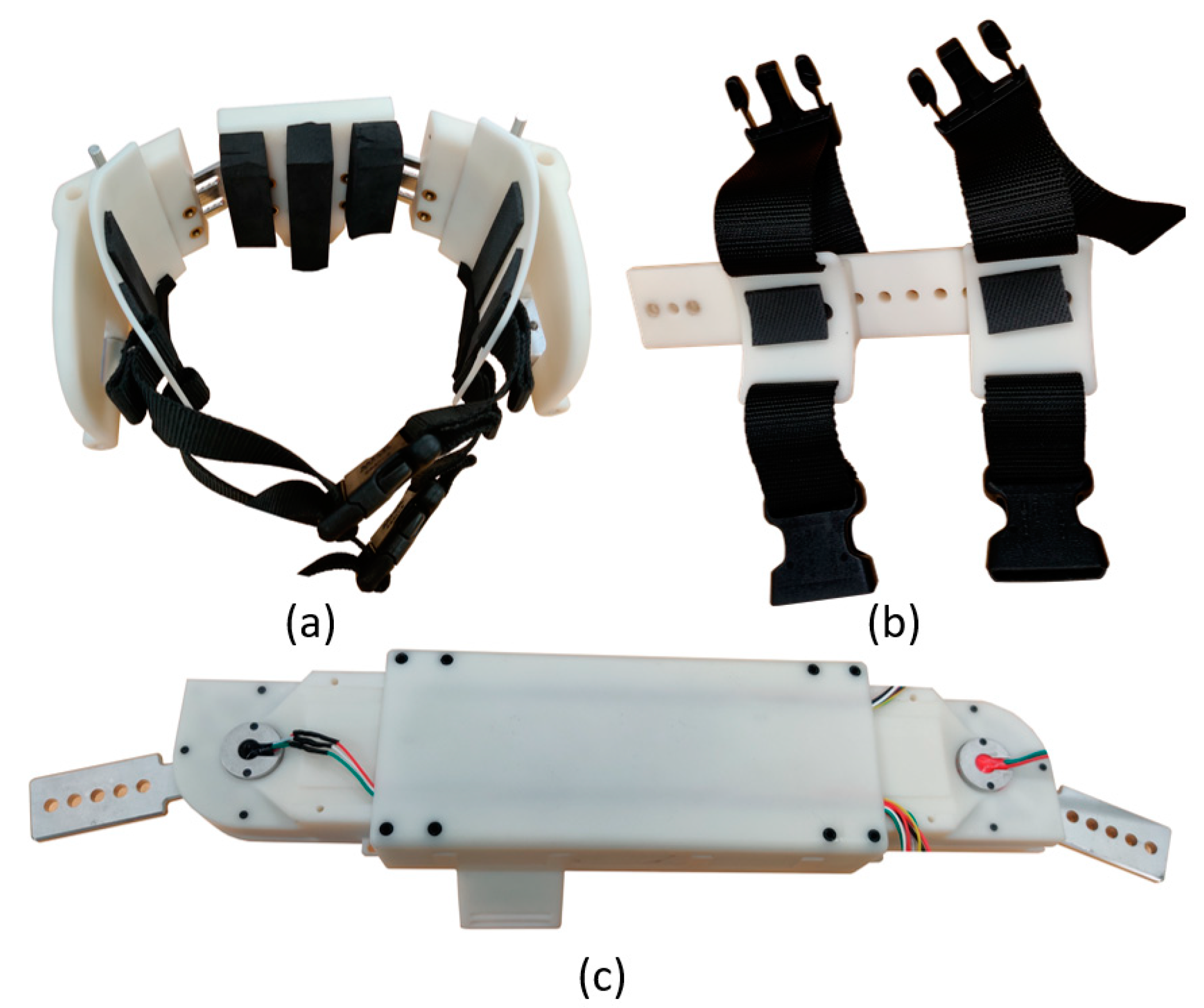
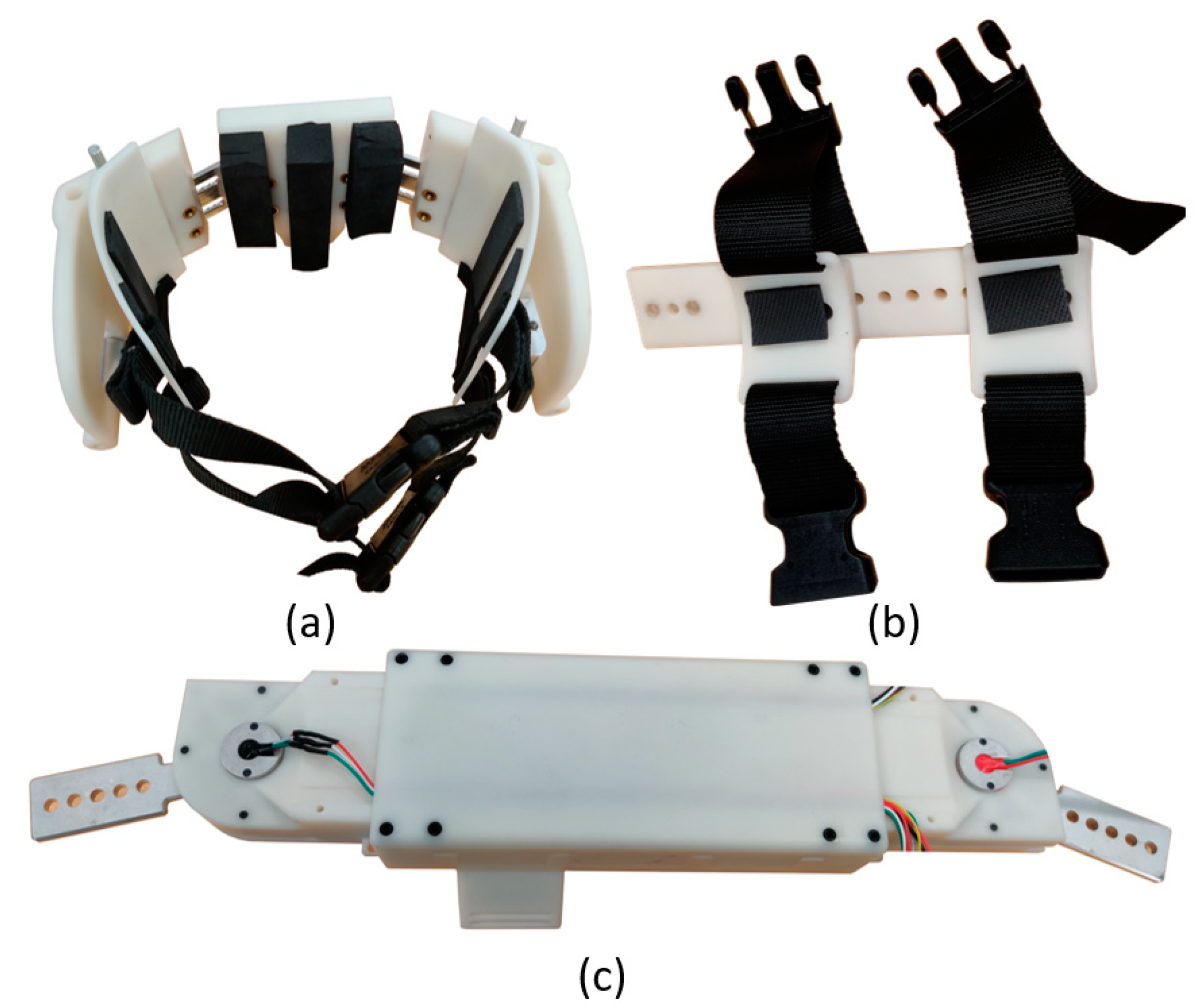
2. Adjustable Pediatric Lower-Limb Exoskeleton
3. Human Factor Assessment Procedure
3.1. Exoskeleton Donning
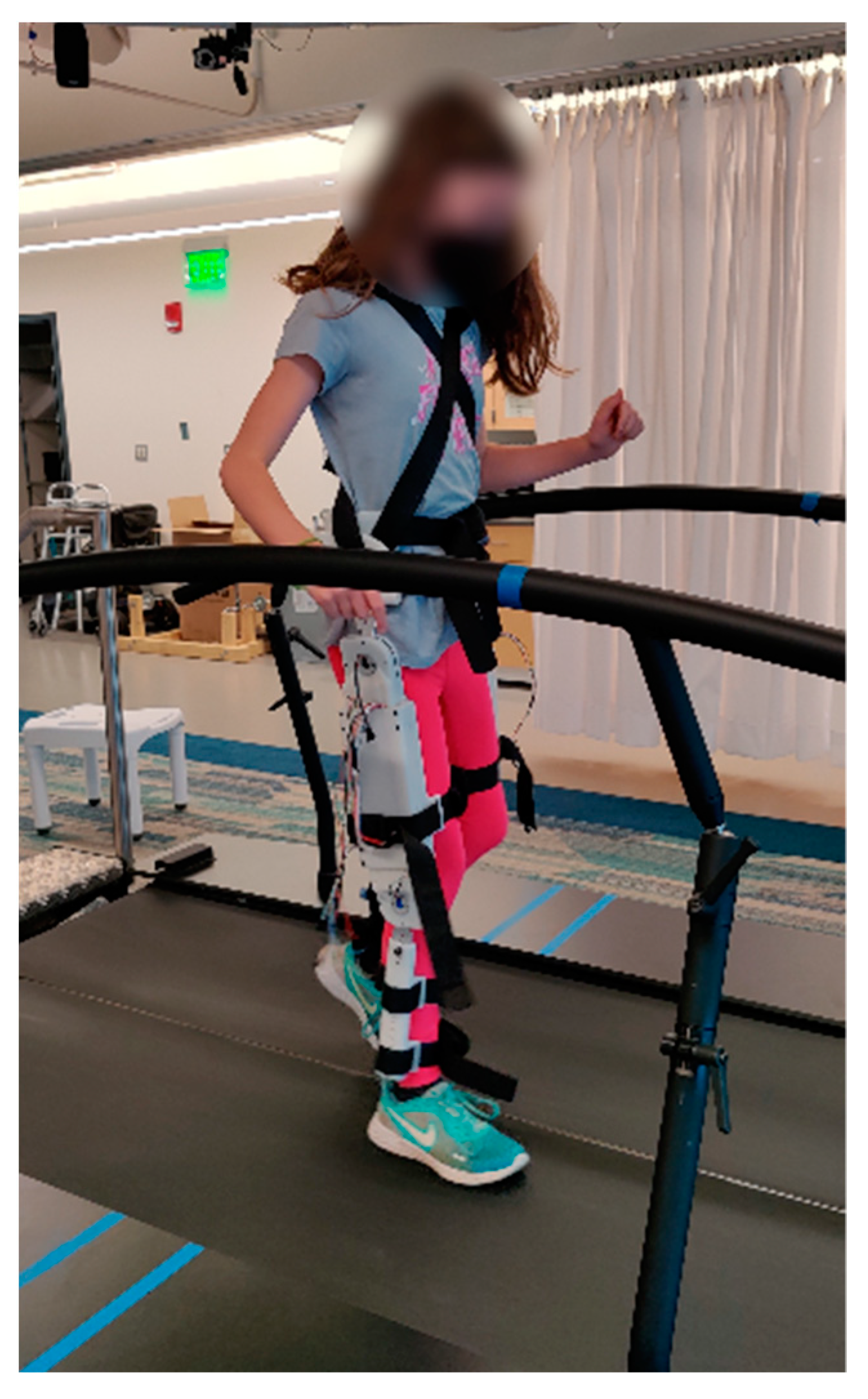
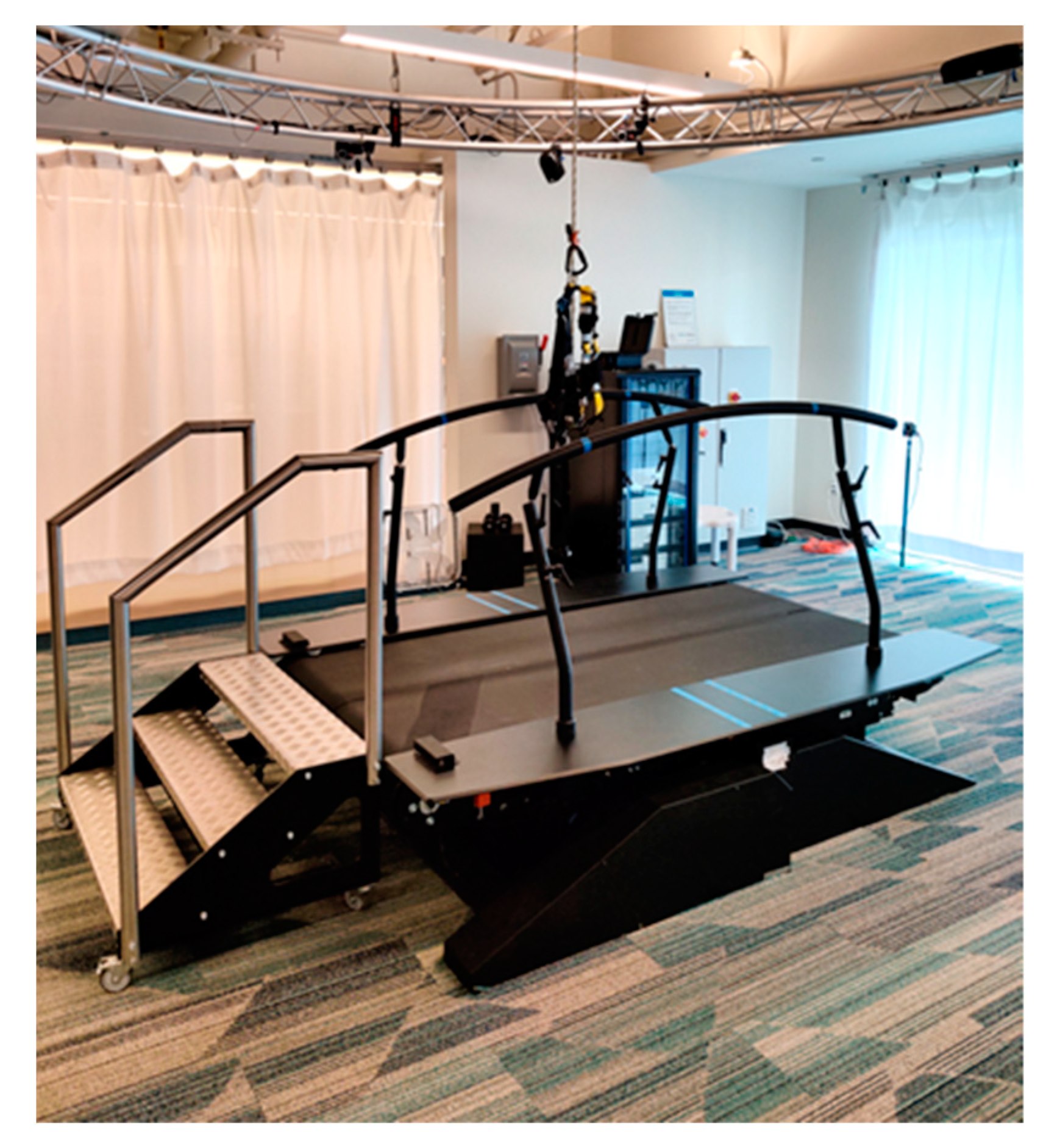
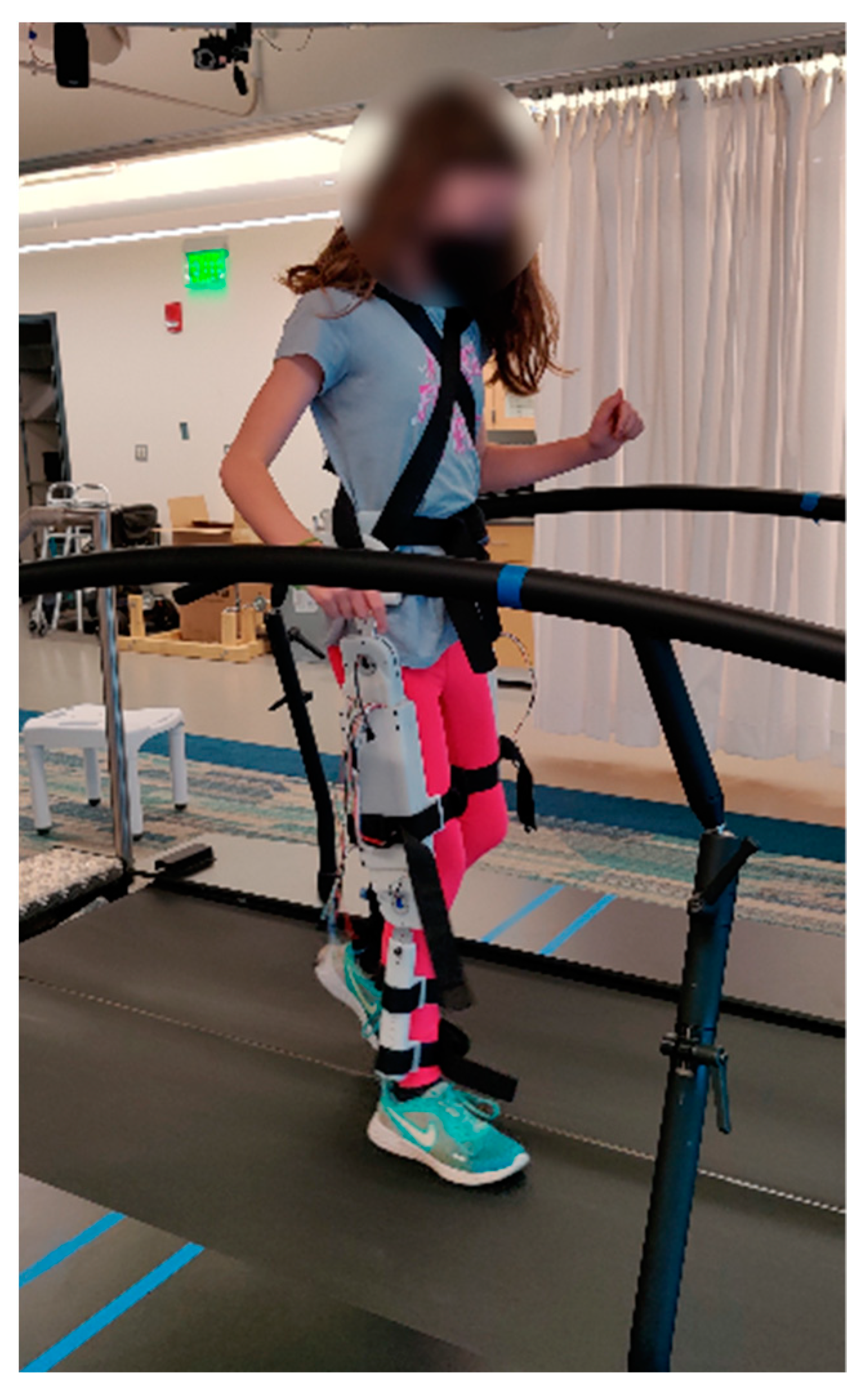
3.2. Six Minute Walk Test
3.3. Exoskeleton Doffing
3.4. Exoskeleton Reconfiguration
4. Results
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viteckova, S.; Kutilek, P.; Jirina, M. Wearable Lower Limb Robotics: A Review. Biocybern. Biomed. Eng. 2013, 33, 96–105. [Google Scholar] [CrossRef]
- Westlake, K.P.; Patten, C. Pilot Study of Lokomat Versus Manual-Assisted Treadmill Training for Locomotor Recovery Post-Stroke. J. NeuroEng. Rehabil. 2009, 6, 18. [Google Scholar] [CrossRef]
- Baunsgaard, C.B.; Nissen, U.; Brust, A.; Frotzler, A.; Ribeill, C.; Kalke, Y.; Leon, N.; Gómez, B.; Samuelsson, K.; Antepohl, W.; et al. Gait Training After Spinal Cord Injury: Safety, Feasibility and Gait Function Following 8 Weeks of Training with the Exoskeletons from Ekso Bionics. Spinal Cord 2017, 56, 106–116. [Google Scholar] [CrossRef]
- Strausser, K.A.; Swift, T.A.; Zoss, A.B.; Kazerooni, H.; Bennett, B.C. Mobile Exoskeleton for Spinal Cord Injury: Development and Testing. In Proceedings of the ASME 2011 Dynamic Systems and Control Conference and Bath/ASME Symposium on Fluid Power and Motion Control; American Society of Mechanical Engineers Digital Collection, Arlington, VA, USA, 5 May 2012; pp. 419–425. [Google Scholar]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk Powered Exoskeleton to Restore Ambulatory Function to Individuals with Thoracic-Level Motor-Complete Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2012, 91, 911–921. [Google Scholar] [CrossRef]
- Kawamoto, H.; Sankai, Y. Power Assist System HAL-3 for Gait Disorder Person. In Computers Helping People with Special Needs; Miesenberger, K., Klaus, J., Zagler, W., Eds.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2002; Volume 2398, pp. 196–203. ISBN 978-3-540-43904-2. [Google Scholar]
- Tefertiller, C.; Hays, K.; Jones, J.; Jayaraman, A.; Hartigan, C.; Bushnik, T.; Forrest, G.F. Initial Outcomes from a Multicenter Study Utilizing the Indego Powered Exoskeleton in Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2018, 24, 78–85. [Google Scholar] [CrossRef]
- Birch, N.; Graham, J.; Priestley, T.; Heywood, C.; Sakel, M.; Gall, A.; Nunn, A.; Signal, N. Results of the First Interim Analysis of the RAPPER II Trial in Patients with Spinal Cord Injury: Ambulation and Functional Exercise Programs in the REX Powered Walking Aid. J. NeuroEng. Rehabil. 2017, 14, 60. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, A.; Lobo-Prat, J.; Font-Llagunes, J.M. Systematic Review on Wearable Lower-Limb Exoskeletons for Gait Training in Neuromuscular Impairments. J. NeuroEng. Rehabil. 2021, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.D.; Potgieter, J.; Noble, F.K. A Review of Commercially Available Exoskeletons’ Capabilities. In Proceedings of the 2017 24th International Conference on Mechatronics and Machine Vision in Practice (M2VIP), Auckland, New Zealand, 21–23 November 2017; pp. 1–5. [Google Scholar]
- Fosch-Villaronga, E.; Čartolovni, A.; Pierce, R.L. Promoting Inclusiveness in Exoskeleton Robotics: Addressing Challenges for Pediatric Access. Paladyn J. Behav. Robot. 2020, 11, 327–339. [Google Scholar] [CrossRef]
- Wren, T.A.L.; Rethlefsen, S.; Kay, R.M. Prevalence of Specific Gait Abnormalities in Children With Cerebral Palsy: Influence of Cerebral Palsy Subtype, Age, and Previous Surgery. J. Pediatr. Orthop. 2005, 25, 79–83. [Google Scholar] [PubMed]
- Bell, K.J.; Õunpuu, S.; DeLuca, P.A.; Romness, M.J. Natural Progression of Gait in Children With Cerebral Palsy. J. Pediatr. Orthop. 2002, 22, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Emery, A.E.H. Population Frequencies of Inherited Neuromuscular Diseases—A World Survey. Neuromuscul. Disord. 1991, 1, 19–29. [Google Scholar] [CrossRef]
- Alexander, M.A.; Matthews, D.J.; Murphy, K.P. Pediatric Rehabilitation, Fifth Edition: Principles and Practice; Demos Medical Publishing: New York, NY, USA, 2015; ISBN 978-1-62070-061-7. [Google Scholar]
- Koenig, A.; Wellner, M.; Köneke, S.; Meyer-Heim, A.; Lünenburger, L.; Riener, R. Virtual Gait Training for Children with Cerebral Palsy Using the Lokomat Gait Orthosis. Stud. Health Technol. Inform. 2008, 132, 204–209. [Google Scholar]
- Brütsch, K.; Koenig, A.; Zimmerli, L.; Mérillat, S.; Riener, R.; Jäncke, L.; van Hedel, H.J.A.; Meyer-Heim, A. Virtual Reality for Enhancement of Robot-Assisted Gait Training in Children with Central Gait Disorders. J. Rehabil. Med. 2011, 43, 493–499. [Google Scholar] [CrossRef]
- Lee, D.R.; Shin, Y.K.; Park, J.-H.; You, J.H. Concurrent Validity and Test-Retest Reliability of the Walkbot-K System for Robotic Gait Training. J. Mech. Med. Biol. 2016, 16, 1640029. [Google Scholar] [CrossRef]
- Diot, C.M.; Thomas, R.L.; Raess, L.; Wrightson, J.G.; Condliffe, E.G. Robotic Lower Extremity Exoskeleton Use in a Non-Ambulatory Child with Cerebral Palsy: A Case Study. Disabil. Rehabil. Assist. Technol. 2021, 16, 1–5. [Google Scholar] [CrossRef]
- Bayón, C.; Ramírez, O.; Castillo, M.D.D.; Serrano, J.I.; Raya, R.; Belda-Lois, J.M.; Poveda, R.; Mollà, F.; Martín, T.; Martínez, I.; et al. CPWalker: Robotic Platform for Gait Rehabilitation in Patients with Cerebral Palsy. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation (ICRA), Long Beach, CA, USA, 16–21 May 2016; pp. 3736–3741. [Google Scholar]
- Lerner, Z.F.; Damiano, D.L.; Park, H.-S.; Gravunder, A.J.; Bulea, T.C. A Robotic Exoskeleton for Treatment of Crouch Gait in Children with Cerebral Palsy: Design and Initial Application. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 650–659. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Damiano, D.L.; Bulea, T.C. A Lower-Extremity Exoskeleton Improves Knee Extension in Children with Crouch Gait from Cerebral Palsy. Sci. Transl. Med. 2017, 9, eaam9145. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Gasparri, G.M.; Bair, M.O.; Lawson, J.L.; Luque, J.; Harvey, T.A.; Lerner, A.T. An Untethered Ankle Exoskeleton Improves Walking Economy in a Pilot Study of Individuals with Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1985–1993. [Google Scholar] [CrossRef]
- Sancho-Pérez, J.; Pérez, M.; García, E.; Sanz-Merodio, D.; Plaza, A.; Cestari, M. Mechanical Description of Atlas 2020, a 10-DoF Paediatric Exoskeleton. In Proceedings of the Advances in Cooperative Robotics, World Scientific, London, UK, 12–14 September 2016; pp. 814–822. [Google Scholar]
- Sanz-Merodio, D.; Pereze, M.; Prieto, M.; Sancho, J.; Garcia, E. Result of Clinical Trials with Children with Spinal Muscular Atrophy Using the ATLAS 202 Lower-Limb Active Orthosis. In Human-Centric Robotics, Proceedings of CLAWAR 2017: 20th International Conference on Climbing and Walking Robots and the Support Technologies of Mobile Machines, Porto, Portugal, 11–13 September 2017; World Scientific: Singapore, 2017; pp. 48–55. [Google Scholar]
- Nakagawa, S.; Mutsuzaki, H.; Mataki, Y.; Endo, Y.; Matsuda, M.; Yoshikawa, K.; Kamada, H.; Yamazaki, M. Newly Developed Hybrid Assistive Limb for Pediatric Patients with Cerebral Palsy: A Case Report. J. Phys. Ther. Sci. 2019, 31, 702–707. [Google Scholar] [CrossRef]
- Nakagawa, S.; Mutsuzaki, H.; Mataki, Y.; Endo, Y.; Matsuda, M.; Yoshikawa, K.; Kamada, H.; Iwasaki, N.; Yamazaki, M. Safety and Immediate Effects of Hybrid Assistive Limb in Children with Cerebral Palsy: A Pilot Study. Brain Dev. 2020, 42, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Eguren, D.; Cestari, M.; Luu, T.P.; Kilicarslan, A.; Steele, A.; Contreras-Vidal, J.L. Design of a Customizable, Modular Pediatric Exoskeleton for Rehabilitation and Mobility. In Proceedings of the 2019 IEEE International Conference on Systems, Man and Cybernetics (SMC), Bari, Italy, 6–9 October 2019; pp. 2411–2416. [Google Scholar]
- Palisano, R.; Begnoche, D.; Chiarello, L.; Bartlett, D.; McCoy, S.; Chang, H.-J. Amount and Focus of Physical Therapy and Occupational Therapy for Young Children with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2012, 32, 368–382. [Google Scholar] [CrossRef] [PubMed]
- Laubscher, C.A.; Farris, R.J.; van den Bogert, A.J.; Sawicki, J.T. An Anthropometrically Parameterized Assistive Lower-Limb Exoskeleton. ASME J. Biomech. Eng. 2021, 143, 105001. [Google Scholar] [CrossRef]
- Goo, A.; Laubscher, C.A.; Farris, R.J.; Sawicki, J.T. Design and Evaluation of a Pediatric Lower-Limb Exoskeleton Joint Actuator. Actuators 2020, 9, 138. [Google Scholar] [CrossRef]
- Goo, A.; Laubscher, C.A.; Wiebrecht, J.J.; Farris, R.J.; Sawicki, J.T. Hybrid Zero Dynamics Control for Gait Guidance of a Novel Adjustable Pediatric Lower-Limb Exoskeleton. Bioengineering 2022, 9, 208. [Google Scholar] [CrossRef]
- Fryar, C.D.; Carroll, M.D.; Qiuping, G.; Afful, J.; Ogden, C.L. Anthropometric Reference Data for Children and Adults: United States, 2015–2018. In National Center for Health Statistic; United States Department of Health and Human Services: Washington, DC, USA, 2021; Volume 46, pp. 1–44. [Google Scholar]
- Lewis, J.R. The System Usability Scale: Past, Present, and Future. Int. J. Human–Comput. Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Kozlowski, A.J.; Bryce, T.N.; Dijkers, M.P. Time and Effort Required by Persons with Spinal Cord Injury to Learn to Use a Powered Exoskeleton for Assisted Walking. Top. Spinal Cord Inj. Rehabil. 2015, 21, 110–121. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Donning (m:ss) | Doffing (m:ss) | Reconfiguration (m:ss) | |
|---|---|---|---|
| Full Task Completion | 6:08 | 2:29 | 8:23 |
| Hip Cradle | 0:00–1:20 | -- | 0:00–1:52 |
| Leg 1 | 1:20–3:15 | -- | 1:52–5:21 |
| Leg 2 | 3:15–4:45 | -- | 5:21–8:23 |
| Overhead Straps | 4:45–6:08 | -- | ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goo, A.C.; Wiebrecht, J.J.; Wajda, D.A.; Sawicki, J.T. Human Factors Assessment of a Novel Pediatric Lower-Limb Exoskeleton. Robotics 2023, 12, 26. https://doi.org/10.3390/robotics12010026
Goo AC, Wiebrecht JJ, Wajda DA, Sawicki JT. Human Factors Assessment of a Novel Pediatric Lower-Limb Exoskeleton. Robotics. 2023; 12(1):26. https://doi.org/10.3390/robotics12010026
Chicago/Turabian StyleGoo, Anthony C., Jason J. Wiebrecht, Douglas A. Wajda, and Jerzy T. Sawicki. 2023. "Human Factors Assessment of a Novel Pediatric Lower-Limb Exoskeleton" Robotics 12, no. 1: 26. https://doi.org/10.3390/robotics12010026
APA StyleGoo, A. C., Wiebrecht, J. J., Wajda, D. A., & Sawicki, J. T. (2023). Human Factors Assessment of a Novel Pediatric Lower-Limb Exoskeleton. Robotics, 12(1), 26. https://doi.org/10.3390/robotics12010026