
Dupilumab in Inflammatory Skin Diseases: A Systematic Review

 , ,
, ,  and
and
Abstract
1. Introduction
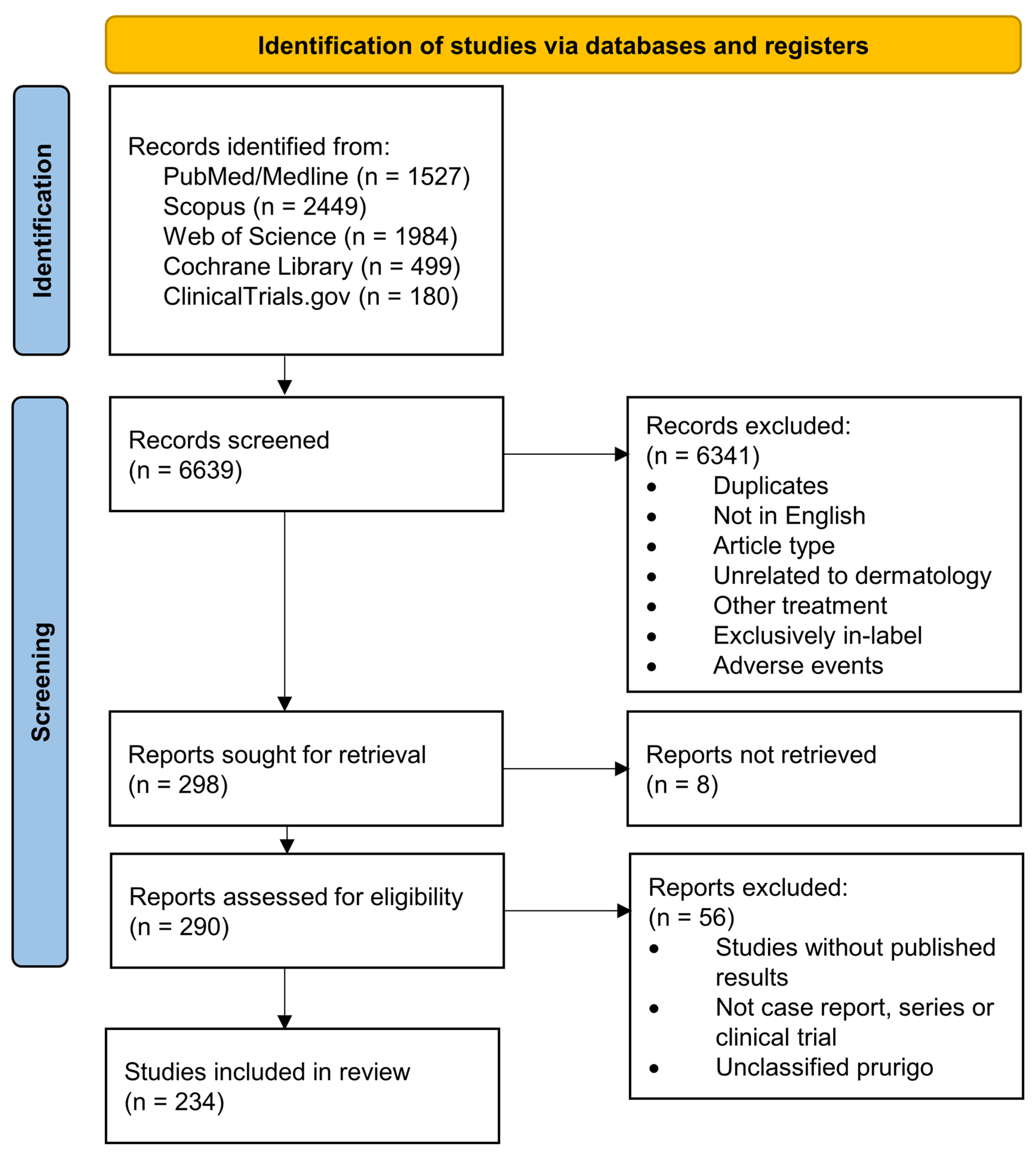
2. Methods
3. Results and Discussion
3.1. Eczema

{kind=link}
{kind=link}
| Disease | Study Type | n | Sex/Age | Presentation | Medical History | Prior Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| Nummular dermatitis | retrospective study (4) | 30 | 38.2 (mean, 19–78 range), females: 12/30 | nummular eczema associated with AD (30/30) | AD (30/30) | topical (18/30) and systemic (28/30) steroids, topical calcineurin inhibitors (8/30), ciclosporin (22/30) | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in skin manifestations (EASI -32.87 mean), itch (NRS -7.17 mean) and quality of life (DLQI -14.57 mean) at 16 wk | [40] | |
| Nummular dermatitis | case series (4) | 6 | 73.5 (median, 45–90 range), females: 1/6 | nummular eczema without AD | no AD (0/6), allergic rhinitis (2/6), asthma (1/6), allergic contact dermatitis (2/6), CHE (1/6) Grover’s disease (1/6) | topical (6/6) and systemic (2/6) steroids, topical calcineurin inhibitor (4/6), topical Vitamin-D analogue (1/6), phototherapy (3/6), MTX (1/6), mycophenolic acid (2/6), ciclosporin (2/6) | ciclosporin (1/6) | Dupilumab 600 mg s.c., then 300 mg q2w | sustained complete response with BSA < 1% (5/6) at up to 2 years follow-up, temporary improvement (1/6) | [41] |
| Contact dermatitis | retrospective study (4) | 15 | 55 (median, 28–72 range), females: 9/15 | allergic contact dermatitis, hand involvement in 11/15 | various type-IV sensitivities (15/15, including cocamidoylpropyl betaine in 40%, nickel in 33%), AD (11/15) | systemic steroid (15/15), ciclosporin (13/15), mycophenolic acid (8/15), MTX (2/15), apremilast (1/15), azathioprin (2/15), ustekinumab (2/15), etanercept (1/15) | Dupilumab 600 mg s.c., then 300 mg q2w | 85% mean improvement in BSA (range 70–100%) | [43] | |
| Contact dermatitis | case report (5) | 1 | M/55 | allergic contact dermatitis | suspected type-IV sensitivity to chromate (no patch-testing performed), bronchitis, viral hepatitis C | topical steroids | Allergen exposure was continued. | Dupilumab 600 mg s.c. q2w | complete resolution of skin lesions at 8 wk | [44] |
| Contact dermatitis | case report (5) | 1 | M/61 | allergic contact dermatitis | type-IV sensitivity to isobornyl acrylate (patch-testing performed), AD, asthma, diabetes mellitus | azathioprin (100 mg/d), topical steroid, antihistamines | Allergen exposure was continued. | Dupilumab 600 mg s.c., then 300 mg q2w | partial resolution of skin manifestations and pruritus at 7 wk, complete resolution at 16 wk | [45] |
| Contact dermatitis | case series (4) | 2 | F/65, M/51 | allergic contact dermatitis | type-IV sensitivity to sesquiterpene lactones (patch-testing performed) (2/2), AD (1/2) | topical (2/2) and systemic (1/2) steroids, MMF (1/2), MTX (1/2), ciclosporin (1/2), azathioprin (150 mg/d, 2/2), ustekinumab (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Partial improvement of skin lesions (2/2), dupilumab paused during winter without deterioration (2/2) | [46] | |
| Contact dermatitis | case report (5) | 1 | M/54 | allergic contact dermatitis, generalized eczema and hand/foot dermatitis | multiple type-IV sensitivities (including nickel, patch-testing performed), AD | topical steroid, phototherapy, acitretin | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of skin manifestations, repeated patch-testing remained positive | [47] | |
| Contact dermatitis | case series (4) | 3 | F/20, F/52, F/53 | allergic contact dermatitis, generalized (1/3), torso and extremities (2/3) | multiple type-IV sensitivities (3/3), type-I allergies (3/3), AD (1/3), allergic rhinitis (1/3) | systemic steroid (3/3), azathioprin (1/3), ciclosporin (1/3) | Dupilumab 600 mg s.c., then 300 mg q2w | ≥90% improvement in BSA (3/3) after 6–12 wk | [48] | |
| Contact dermatitis | case series (4) | 6 | 47.5 (median, 26–67 range), females: 5/6 | occupational irritant contact dermatitis (3/6), allergic contact dermatitis (3/6) | type-IV sensitivities (4/6), history of atopy (3/6) | topical (6/6) and systemic (1/6) steroids, phototherapy (3/6), alitretinoin (4/6), MTX (5/6) | Topical tacrolimus (1/6). Allergen/irritant exposure was continued (4/6). | Dupilumab 600 mg s.c., then 300 mg q2w | total clearance of skin lesions (5/6), partial remission (1/6) | [49] |
| Contact dermatitis | case report (5) | 1 | M/44 | disseminated spongiotic dermatitis | type-IV sensitivities (nickel), nickel-containing stent, antiphospholipid syndrome, no AD or atopy | topical and systemic steroids, antihistamines, MMF (1.5 g/d) | systemic steroid, tapered | Dupilumab 600 mg s.c., then 300 mg q2w | significant improvement after 8 wk | [50] |
| Contact dermatitis | case series (4) | 3 | F/52, F/54, F/54 | disseminated eczema including body and face | type-IV sensitivities (neomycin, fragrance and perfume (1/3); budesonide, limonene (1/3); shampoo (1/3)) AD (2/2) | Dupilumab 600 mg s.c., then 300 mg q2w | 75%-improvement after 10 wk (1/3), full clearance after 8 wk (2/3) | [51] | ||
| Contact dermatitis | case report (5) | 1 | F/42 | eczema on hands and arms | type-IV sensitivity (colophonium), AD | topical and systemic steroids, MTX, ciclosporin | Dupilumab 300 mg q2w | flare-up at former patch-testing sites (recall dermatitis), partial control at 10 wk | [52] | |
| Contact dermatitis | case series (4) | 2 | F/83, F/69 | disseminated eczema including body and extremitites | type-IV sensitivities (fragrance, propylene glycol (1/2); balsam of peru, propylene glycol (1/2)) | topical and systemic steroids (2/2), MTX (15 mg/wk, 1/2), MMF (2 g/d, 1/2) | topical steroids and calcineurin inhibitors | Dupilumab 300 mg q2w | Significant improvement, BSA 2% after 4 mo (1/2) or 5% after 6 mo (1/2) | [53] |
| Contact dermatitis | retrospective study (4) | 15 | 44 (mean, 18 SD), females: 12/17 | AD (17/17) | 4 modalities on average | Dupilumab | BSA improvement in 82%, 71%-reduction (mean, 42 SD), pruritus improved in 100% | [54] | ||
| Contact dermatitis | case report (4) | 5 | 54 (median, 29–69 range), females: 2/5 | AD or history of atopy (4/5), type-IV sensitivities (5/5, miscellaneous) | topical (5/5) and systemic (3/5) steroid, ciclosporin (4/5), mycophenolic acid (4/3), MTX (1/5), phototherapy (1/5) | 80–100% improvement within 10–12 wk (5/5) | [55] | |||
| Contact dermatitis | retrospective study (4) | 6 | 55.3 (mean, 4.9 SD), females: 4/6 | generalized eczema | AD (6/6), type-IV sensitivities (multiple personal care products) | topical steroids, phototherapy (1/6) | Dupilumab 600 mg s.c., then 300 mg q2w | complete clearance of dermatitis (4/6), residual hand dermatitis (1/6), flares (1/6) | [56] | |
| Contact dermatitis | case report (5) | 1 | F/43 | pruritic rash on face and upper trunk after hair dyeing | type-IV sensitivity (p-phenylenediamine), dermatomyositis | topical steroids, antihistamines | Dupilumab 600 mg s.c., then 300 mg q2w | complete resolution after 6 wk | [57] | |
| Contact dermatitis | case report (5) | 1 | M/52 | facial eczema | no AD; type-IV sensitivities (sesquiterpene lactone, artichoke) | systemic steroids, ciclosporin | Dupilumab 600 mg s.c., then 300 mg q2w | partial response after 8 wk | [58] | |
| Contact dermatitis | case report (5) | 1 | F/45 | eczema of hands and arms | AD, allergic conjuncitivitis, type-IV sensitivity (rubber) | topical and systemic steroids, ciclosporin | Dupilumab 600 mg s.c. q2w | complete resolution of skin lesions at 18 wk, resolution of pruritus | [59] | |
| Contact dermatitis | case report (5) | 1 | F/48 | pruritic fissured hand eczema, eyelid eczema | asthma, no AD, type-IV sensitivities (p-phenylenediamine and others) | topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | no efficacy, discontinued | [60] | |
| Contact dermatitis | case report (5) | 1 | M/54 | vesiculobullous lesions of hands and feet | no AD; type-IV sensitivities (thiuram mix and others) | systemic steroids, ciclosporin | Dupilumab | no efficacy, discontinued after 12 mo | [61] | |
| Dyshidrotic eczema | case series (5) | 15 | 56 (mean, 32–76 range), females: 33% | no AD (15/15) | topical steroids (15/15), systemic immunosuppressive (7/15), phototherapy (3/15), psoriasis biologic (7/15) | ustekinumab (1/15, for concomitant psoriasis) | Dupilumab | Partial response (15/15) with reduced itch and skin lesions, complete clearance (6/15). | [63] | |
| CHE | case report (5) | 1 | M/12 | vesicular eczema of hands and feet with pruritus and painful lesions | AD | topical and systemic steroid, phototherapy, MTX (10 mg/m2/wk), ciclosporin (5 mg/kg biweekly) | topical mometasone and systemic prednisolone, tapered | Dupilumab 600 mg s.c., then 300 mg q2w | Gradual resolution of skin lesions at 4 wk, complete stable remission at 4 mo. | [64] |
| CHE | retrospective study (4) | 19 | 55.9 (mean, 13.0 SD), females: 16/19 | hyperkeratotic CHE (10/19), atopic CHE (4/19), allergic contact dermatitis (2/19), irritant contact dermatitis (1/19), pulpitis (1/19), vesicular hand eczema (1/19) | AD (6/19) | topical (19/19) and systemic (6/19) steroid, MTX (12/19), acitretin (6/19), alitretinoin (12/19), ciclosporin (5/19), azathioprin (11/19), MMF (7/19), psoriasis biologicals (7/19) | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of skin lesions and quality of life (14/19); no effect or deterioration (5/19). Effects were worse in hyperkeratotic CHE (p = 0.033 compared with all others) | [65] | |
| CHE | prospective observational study (3) | 72 | 45.2 (mean, 13.0 SD), females: 33.3% | chronic fissured HE (72.2%), recurrent vesicular HE (27.8%) | AD (100%), type-IV sensitivity (38.9%, patch testing performed), irritant contact dermatitis (22.2%), asthma (61.1%), allergic rhinitis (70.8%), allergic conjunctivitis (55.6%) | topical (100%) and systemic (81.9%) steroid, ciclosporin (93.1%), MTX (36.1%), azathioprin (26.4%), alitretinoin (13.9%), MMF (6.9%), systemic tacrolimus (2.8%) | Topical steroids or calcineurin inhibitors. No systemic immunosuppressive drugs (various washout intervals). | Dupilumab 600 mg s.c., then 300 mg q2w | HECSI −89% (95%-CI: −93.1 to −84.5) at wk 52, HECSI-90 met by 62.9%, no difference between HE-subtype or concomitant irritant contact dermatitis, improved quality of life | [66] |
| CHE | case series (4) | 3 | M/65, M/47, F/65 | hyperceratotic HE (3/3) | no AD (3/3) | topical steroids (3/3), alitretinoin (3/3) | no topical treatment (2 wk washout) | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in itch and quality of life (3/3), complete clearance of skin lesions (2/3) at 16 wk, no effect on skin lesions (1/3) | [67] |
| CHE | case report (5) | 1 | M/43 | occupational irritant hand dermatitis (compulsive hand washing, cleaning agents, steering wheel, handling coins) | no AD, no type-IV sensitvity (patch-testing performed) | topical and systemic steroids, phototherapy, acitretin (25 mg/d), MTX (15–20 mg/wk), antibiotics | topical steroid | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of HECSI (33 to 10 at 4 wk, 0 at 5 mo) | [68] |
| CHE | case report (5) | 1 | M/67 | recurrent vesicular HE | no AD, no atopy, no type-IV sensitivity (patch-testing performed) | topical and systemic steroids, tar, phototherapy, MTX (25 mg/wk), azathioprine (150 mg/d), ciclosporin (200 mg/d) | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of skin lesions at 2 wk, complete clearance at 4 wk, sustained response for 3 mo follow-up | [69] | |
| CHE | prospective observational study (3) | 47 | 45.2 (mean, 20–69 range), females: 31.9% | chronic fissured HE (74.5%), recurrent vesicular HE (25.5%) | AD (100%), type-IV sensitivity (29.8%, patch testing performed) | Topical steroids or calcineurin inhibitors. No systemic immunosuppressive drugs (various washout intervals). | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of HECSI (in 45/47), HECSI-90 met by 32%, HECSI mean change −74.6% (95%-CI −67.9 to −81.2) at 16 wk. No difference between HE-types. No response in 2/45 | [70] | |
| CHE | retrospective study (4) | 38 | 42.2 (mean, 18.4 SD), females: 23/38 | various subtypes of HE including dyshidrotic eczema, atopic HE, contact dermatitis | systemic steroid (42%), MMF (32%), ciclosporin (16%) | Topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in pruritus (96.7%, complete resolution in 26.7%), improvement in BSA (−15.9% mean) in ≥12 wk follow-up | [71] | |
| CHE | case report (5) | 1 | F/50s | atopic HE | AD, asthma, rhinitis, multiple type-IV sensitivities (including nickel, cobalt) | topical and systemic steroids, phototherapy, alitretinoin (10–30 mg/d), ciclosporin (5 mg/kg/d), azathioprin (2.5 mg/kg/d), mycophenolic acid (1140 mg/d), tacrolimus (0.1 mg/kg/d), MTX (10–20 mg/wk) | prednisolone (7.5 mg/d) | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in HECSI from 244 to 11 (“almost clear”) in 16 wk | [72] |
| CHE | case series (4) | 4 | F/72, F/65, M/48 | atopic HE (4/4) | AD (3/3), allergic rhinitis (2/3) multiple type-I sensitivities (1/3), no type-IV sensitvity (0/3, patch-testing performed) | topical (3/3) and systemic (2/3) steroids, topical (3/3) and systemic (1/3) calcineurin inhibitor, thalidomide (1/3), MTX (1/3), MMF (3/3), ciclosporin (2/3), apremilast (1/3), ustekinumab (1/3) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete clearance (1/3), partial improvement (2/3) after 6–12 wk, sustained response at 3–8 mo follow-up | [73] | |
| CHE | case series (4) | 2 | M/63, M38 | dyshidrotic hand and foot eczema | asthma (1/2), no AD (0/2) | topical and systemic steroids (2/2), phototherapy (2/2), excimer laser (1/2), apremilast (2/2), MTX (2/2), efalizumab (1/2), etanercept (1/2), adalimumab (1/2), ixekizumab (1/2), ciclosporin (1/2), MMF (1/2) | ciclosporin (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w | complete clearance after 8 wk (1/2) or 16 wk (1/2) | [74] |
| CHE | case report (5) | 1 | F/44 | dyshidrotic hand and foot eczema | asthma, no type-IV sensibilities (patch-testing performed) | topical and systemic steroids, topical calcineurin inhibitors, antihistamines, excimer laser therapy, | Dupilumab 600 mg s.c., then 300 mg q2w | complete clearance after 8 wk | [75] | |
| CHE | case report (5) | 1 | M/40s | dyshidrotic hand and foot eczema | no atopy | topical and systemic steroids, antifungals, ciclosporin | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution after 3 wk | [76] | |
| CHE | case series (4) | 2 | M/38 (2/2) | dyshidrotic hand (2/2) and foot (2/2) eczema | type IV-sensibilities (1/2; multiple) | topical and systemic steroids (2/2), apremilast (1/2), acitretin (1/2), phototherapy (1/2) | topical steroids (2/2), phototherapy (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Near complete resolution after 1 (1/2) or 6 wk (1/2) | [77] |
| CHF | case report (5) | 1 | F/29 | occupational irritant hand dermatitis | no atopy, no type-IV sensibilities (patch-testing performed) | topical seroids, topical calcineurin inhibitors, antihistamines | Dupilumab 600 mg s.c., then 300 mg q2w. Later q4w. | HECSI 116 to 15 after 4 wk | [78] | |
| Eczematous eruption (αIL17R-induced) | case report (5) | 1 | M/62 | generalized pruritic rash under brodalumab for psoriasis | psoriasis, AD, allergic rhinitis, latent tuberculosis infection | topical and systemic steroids, antihistamines | guselkumab; brodalumab discontinued | Dupilumab 600 mg s.c., then 300 mg q2w | Complete clearance of skin manifestations and itch at 8 wk | [79] |
| Eczematous eruption (αIL17 or -23 induced) | case series (4) | 3 | M/42, F/24, F/54 | localized AD-like eczema | psoriasis (2/3), Crohn’s disease (1/3) | topical (3/3) and systemic (1/3) steroids, topical calcineurin inhibitors (3/3) | ixekizumab (1/3), ustekinumab (1/3), tildrakizumab (1/3) (all continued) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution (EASI 0) after 4 wk (1/3), 6 (1/3) or 7 mo (1/3) | [80] |
| Eczematous eruption of aging | case series (4) | 15 | 75 (mean, SD: 8), females: 67% | no AD or atopy (15/15) | topical (15/15) and systemic steroids (11/15), topical calcineurin inhibitors (11/15), systemic immunosuppression (2/15), phototherapy (1/15) | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of skin lesions (15/15), BSA 20% (SD 15) to 2.6 (SD 4) in 2–8 wk. Sustained response in 7/15 after 8–12 mo follow-up | [81] | ||
| Eczematous eruption of aging | case report (5) | 1 | M/66 | 3-years history of generalized pruritic rash excluding head and neck | no atopy; type-IV allergy to ciprofloxacin | topical and systemic steroids, MTX (17.5 mg/wk), MMF (1 g/d), phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Complete clearance of skin manifestations and itch at 8 wk, sustained at 4 mo follow-up | [82] | |
| Eczematous eruption (CVID) | case report (5) | 1 | F/59 | Recurrent generalized pruritic rash | CVID, type-IV sensitivity (chrome, nickel, colophonium, mercapto-mix, thiomersal) | topical and systemic steroids, ciclosporin (150 mg/d), IVIg | Dupilumab 600 mg s.c., then 300 mg q2w | Control of itch in 4 wk. Complete resolution of skin manifestations (EASI 41.10 to 1.20) in 8 wk. | [83] | |
| Autoeczema-tization in chronic stasis dermatitis | case report (5) | 1 | M/80 | generalized pruritic papules and eczematous patches, venous stasis dermatitis of lower extremity | no type-IV sensitivity (patch-testing performed) | topical and systemic steroids, compression therapy | compression therapy | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of itch (-7 NRS) and reduced lower extremity edema at 10 wk. New psoriasiform dermatitis, dupilumab discontinued. | [84] |
3.2. Chronic Pruritus and Prurigo
3.3. Bullous and Acantholytic Dermatoses
| Disease | Study Type | n | Sex/Age | Medical History | Prior Systemic Therapies | Concomitant Systemic Medication | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|
| BP | case series (4) | 7 | 74 (median, 63–88 range) | hypertension (4/7), diabetes (2/7), MDS (1/7) | none (5/7), steroid + ciclosporin (1/7), tofacitinib + omalizumab (1/7) | none (1/7), methylprednisolone 0.5–0.6 mg/kg/d with reduction (5/7), prednisolone 0.5 mg/kg/d with reduction (1/7) | Dupilumab 600 mg s.c. initially, then 300 mg q2w for 16 wk | Total BPDAI reduced to 2 (median, IQR 6 to 0), p < 0.0001 at 16 wk, Reduction of BP180 and BP230 ab, also IgE. 4 stopped dupilumab, no relapse. 2 prolonged dosing with 300 mg q3-4w, no relapse. 1 relapse after taper of dupilumab, controlled again with 300 mg q2w. 1 relapse after glucocorticoid taper, controlled with dupilumab. | [105] |
| BP | case series (4) | 2 | F/53, M/78 | prednisolone 0.5–0.8 mg/kg/d | prednisolone 20 mg/d | Dupilumab 600 mg s.c. initially, then 300 mg q2w. Withdrawal after 2 months | Sustained clinical remission | [106] | |
| BP | case series (4) | 2 | M/72, M/88 | methylprednisolone (2/2), MTX (1/2) | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Relief of pruritus, improvement of lesions at 2 wk follow-up | [107] | ||
| BP | case series (4) | 3 | 2F, 1M | psychiatric disorders (1/3), Hepatitis B (2/3), gastric ulcers (1/3) | steroids (max. equivalent to 2.5 mg/kg/d prednisone, 2/3), IVIG (2/3), cyclophosphamide (1/3), MTX (1/3), ciclosporin (1/3), none (1/3) | prednisone (0.75 mg/kg/d) + cyclophosphamide (1/3), methylprednisolone + MTX + ciclosporin (1/3), none (1/3) | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Relief of pruritus (3/3), improvement of skin lesions (2/3), clinical remission (1/3) | [108] |
| Vesicular BP | case report (5) | 1 | M/32 | pulmonary tuberculosis | high-dose systemic steroids | prednisolone 30 mg/d, isoniazide, rifampicin, ethambutol | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Clinical remission, no relapse of tuberculosis | [109] |
| BP (non-bullous) | case report (5) | 1 | M/74 | diabetes mellitus, hypertension | high-dose systemic steroids | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission from 4 wk | [110] | |
| BP | case report (5) | 1 | F/61 | methylprednisolone (max. 0.5 mg/kg/d), azathioprine (100 mg/d) | methylprednisolone, azathioprine (100 mg/d) | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Resolution of pruritus and cessation of blister development within 1 month. Sustained clinical remission. | [111] | |
| BP | case report (5) | 1 | M/80 | prednisone 40 mg/d, doxycycline 200 mg/d, mycophenolate mofetil 1.000 mg/d, niacinamide 1.500 mg/d | prednisone, doxycycline | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission | [112] | |
| BP | case report (5) | 1 | M/70 | obesity, diabetes mellitus, hypertension | dapsone (150 mg/d), MTX (7.5 mg/wk s.c.), mycophenolate mofetil (2 g/d), omalizumab (300 mg s.c. q4w) | mycophenolate mofetil, omalizumab | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Reduced itch NRS (0/10) and cessation of new lesions after 3 months, sustained clinical remission | [113] |
| BP | case series (4) | 13 | 78 (median, 53–91 range) | none (1/13), steroids (9/13), MMF (2/13), rituximab (2/13), IVIG (3/13), azathioprine (1/13), nicotinamide (3/13), doxycycline (4/13), MTX (4/13) | none (7/13), MTX (3/13), prednisone with taper (3/13) | Dupilumab 600 mg s.c. initially, then 300 mg q2w or qw | Sustained clinical remission (7/13), relief of pruritus (12/13), no response (1/13) | [114] | |
| BP | case report (5) | 1 | M/89 | diabetes mellitus | doxycycline (200 mg/d), nicotinamide (1000 mg/d), MMF (2 g/d), prednisone (10 mg/d), omalizumab | prednisone (2.5 mg/d), MMF, doxycycline, nicotinamide | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Relief of pruritus at 2 wk, resolution of BP lesions at 7 wk. Sustained clinical remission at 1 year. | [115] |
| BP | case report (5) | 1 | M/86 | PN, type 2 diabetes mellitus | methylprednisolone, azathioprine, doxycycline | methylprednisolone, doxycycline; both discontinued after 4 mo | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Complete remission after 4 mo, sustained under dupilumab-monotherapy for 10 mo follow-up | [116] |
| BP | case report (5) | 1 | F/17 | doxycycline, methylprednisolone 75 mg/d, prednisolone, rituximab (q2w, later q4w), plasmapheresis (13 sessions total), IVIG (2g/kg q4w) | steroids, rituximab, IVIG | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Complete blister resolution, undetectable BP180 (initially 574 U/mL) | [117] | |
| BP | case report (5) | 1 | M/85 | suspected AD, asthma, ulcerative colitis | tofacitinib and omalizumab for suspected AD, ineffective | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission at 6 mo | [118] |
| BP | case report (5) | 1 | M/80 | prednisone | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission at 10 mo | [119] | |
| BP, COVID-vaccination induced | case report (5) | 1 | M/78 | diabetes mellitus, hypertension, hyperlipidemia | prednisone, doxycycline | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission | [120] |
| BP (ICI-induced) | case report (5) | 1 | M/76 | Melanoma St. IV (adjuvant Nivolumab 480 mg i.v. q4w for 6 mo) | methylprednisolone (0.6 mg/kg/d), doxycycline (200 mg/d), nivolumab discontinuation | methylprednisolone, tapered | Dupilumab 300 mg s.c. q2w | Sustained clinical remission | [121] |
| BP (ICI-induced) | case report (5) | 1 | F/59 | Cervical cancer St. IIB (adjuvant Pembrolizumab for 5 wk prior) | methylprednisolone (1 mg/kg/d), doxycycline (200 mg/d), niacinamide (1 g/d), dapsone (75 mg/d), pembrolizumab discontinuation | methylprednisolone (0.75 mg/kg/d), tapered | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Cessation of new blister formation at 2 mo, severe flare after discontinuation, sustained clinical remission after re-initiation of dupilumab | [122] |
| BP (ICI-induced) | case report (5) | 1 | F/79 | Melanoma St. II (adjuvant Nivolumab for 11 mo prior) | prednisone, doxycycline, dapsone | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission reached at 4 wk | [123] | |
| BP and GD (ICI-induced) | case report (5) | 1 | M/73 | Metastatic renal cell carinoma (ipilimumab/nivolumab treatment), autoimmune thyreoiditis | steroids, doxycycline, dapsone | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Complete resolution of skin lesions and pruritus of both BP and GD | [124] | |
| BP, COVID-vaccination induced | case report (5) | 1 | F/91 | hypertension, chronic kidney failure | prednisone, azathioprine, rituximab (1 cycle) | prednisone with tapering | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Resolution of pruritus and BP lesions after 2 months | [125] |
| BP | Retrospective cohort study (3) | 20 vs. 20 | 72 (median, 54–86 range) | hypertension (30%), cardiovascular disease (15%), diabetes mellitus (20%), chronic renal insufficiency (15%), neurologic disorder (25%), interstitial lung disease (25%), tumor (5%) | no prior therapy (17/20 cases, 20/20 controls) | methylprednisolone (<0.4 mg/kg/d) | Dupilumab 600 mg s.c. initially, then 300 mg q2w vs. 0.4 mg/kg/d methylprednisolone | Shorter median time to disease control (14 vs. 19 days, p = 0.043), lower cumulative dose of steroid (p < 0.01) | [126] |
| BP | Retro-spective cohort study (3) | 8 vs. 16 | 64.5 (median, 22–90 range) | cardiovascular disease (3/8), neurologic disorder (1/8), hyperlipidemia (3/8), tumor (2/8) | methylprednisolone (0.6 mg/kg/d) + azathioprine (2 mg/kg/d) with reduction | Dupilumab 600 mg s.c. initially, then 300 mg q2w vs. methylprednisolone (0.6 mg/kg/d) + azathioprine (2 mg/kg/d) with reduction | More rapid decline of itch NRS (p = 0.034) and BPDAI (p = 0.0308), shorter median time to cessation of new blisters (8 vs. 12 days, p = 0.028), lower cumulative dose of methylprednisolone (p = 0.036), lower cumulative dose of azathioprine (p = 0.0048) | [127] | |
| Pemphigoid gestationis | case report (5) | 1 | F/37 | 20 wk of gestation, g5, p4 | prednisone (0.5 mg/kg/d) | prednisone, tapered | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Decline of BP18 autoantibodies, clearance of skin lesions, sustained clinical remission postpartum. Newborn without skin lesions | [128] |
| LPP | case report (5) | 1 | M/69 | Lichen planus mucosae (20 years) | prednicolone (50 mg/d) | prednisolone, tapered | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission reached at 2 wk, normal BP180 ab | [129] |
| LPP | case report (5) | 1 | M/18 | AD | dexamethasone (8 mg/d), MMF (1 g/d) | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Partial remission at 4 wk, clinical remission reached at 15 wk and sustained after discontinuation of dupilumab | [130] |
| Brunsting-Perry Pemphigoid | case report (5) | 1 | M/71 | prednisone, MMF | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Partial clearance of bullae and erosions after 6 wk, persistent occasional bullae, mild pruritus, scarring | [131] | |
| Brunsting-Perry Pemphigoid | case report (5) | 1 | F/63 | AD, allergic rhinitis | rituximab, steroids, MMF, MTX, dapsone, doxycycline, nicotinamide | Dupilumab 300 mg s.c. q2w | Partial remission | [132] | |
| Pemphigoid nodularis | case report (5) | 1 | F/76 | hypertension, diabetes, obesity, and atrial fibrillation | none | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission reached at 4 mo | [133] |
| LAD | case report (5) | 1 | M/63 | AD, allergic rhino-conjunctivitis | methylprednisolone, azathioprine, dapsone (100 mg/d), colchicine (3 mg/d) | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Sustained clinical remission reached at 4 wk | [134] | |
| Pemphigus vulgaris | case report (5) | 1 | F/41 | steroids | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Clearance of oral lesions at 6 wk, sustained clinical remission | [136] | |
| Pemphigus vulgaris | case report (5) | 1 | M/35 | steroids, IVIG | steroids, IVIG | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Partial remission with PDAI -55 at 6 wk | [137] | |
| DEB-Pr (COL7A1 mutation) | case report (5) | 1 | F/52 | no AD | antihistamines, promethazine, cannabis, St. John’s wort | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Improvement of itch NAS and quality of life (measured by DLQI), improvement of skin lesions at 12 wk | [139] |
| DEB-Pr (COL7A1 mutation) | case series (4) | 2 | M/15, F/27 | asthma (1/2), ADHD (1/2) | steroids (1/2), antihistamines (2/2), ciclosporine (2/2), MMF (1/2), thalidomide (2/2), lenalidomide (1/2), omalizumab (1/2), tofacitinib (1/2), gabapentin (1/2), pregabalin (1/2), naltrexone (1/2), melatonine (1/2), clonidine (1/2), ondansetron (1/2), antidepressants (2/2), phototherapy (2/2), dermabrasio (1/2) | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w (1/2) or qw (1/2) | Sustained improvement of itch (-3.5 and -7 NRS), improvement of skin findings, improvement of sleep | [140] |
| DEB-Pr (COL7A1 mutation) | case report (5) | 1 | M/39 | dapsone, cyproheptadine | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Improvement of itch at 2 wk, cessation of new lesions at 4 wk, partial remission at 9 mo | [141] | |
| DEB-Pr (COL7A1 mutation) | case report (5) | 1 | F/10 | steroids | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Improvement of itch NAS and quality of life (measured by DLQI) | [142] | |
| DEB-Pr (COL7A1 mutation) | case report (5) | 1 | F/43 | frequent bacterial skin infections | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Improvement of itch, no more episodes of skin infections | [143] | |
| Hailey-Hailey | case report (5) | 1 | F/22 | ciclosporine (5 mg/kg/d) | none | Dupilumab 300 mg s.c. q2w | Resolution of skin lesions after 4 mo | [144] | |
| Hailey-Hailey | case series (4) | 3 | F/56, M/52, F/59 | antihistamines (3/3), acitretin (3/3), steroids (3/3), MTX (2/3), ciclosporine (2/3), hydroxychloroquine (2/3), naltrexone (2/3), apremilast (3/3), fluconazole (2/3), tetracyclines (3/3), dapsone (3/3), oxybutynin (2/3), MMF (1/3), local laser ablation (1/3) | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Improvement in affected body surface area (BSA) and quality of life (2/3), no improvement (1/3) | [145] | |
| Hailey-Hailey | case series (4) | 3 | F/50s, M/50s, M/70s | antihistamines (3/3), isotretinoin (1/3), etanercept (1/3), steroids (1/3), acitretin (2/3), naltrexone (2/3), antibiotics (1/3), ciclosporine (1/3), local botulinum toxin (1/3) | none | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Reduction of size and thickness of skin lesions | [146] | |
| GD | case report (5) | 1 | M/71 | Metastatic renal cell carinoma (ipilimumab/nivolumab treatment) | pulsed prednisone (60 mg/d max.), antihistamines, gabapentin, aprepitant, topical phototherapy | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Complete resolution of skin lesions and pruritus at 3 mo; sustained after restart of ipilimumab/nivolumab | [147] | |
| GD | case series (4) | 3 | M/70s, F/50s, M/70s | steroids (3/3), azathioprine (1/3), MTX (2/3), gabapentin (1/3), topical phototherapy (1/3), acitretin (1/3) | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Complete resolution of skin lesions and pruritus within 2 mo (3/3) | [148] | ||
| GD | case report (5) | 1 | M/77 | CRSwNP | steroids | pulsed steroid | Dupilumab 600 mg s.c. initially, then 300 mg q2w | Complete resolution of skin lesions and pruritus at 14 wk | [149] |
3.4. Alopecia Areata
3.5. Chronic Urticaria
3.6. Netherton Syndrome and Other Hereditary Skin Diseases
3.7. Eosinophilic Dermatoses
3.8. Connective Tissue Disorders
3.9. Other Inflammatory Skin Diseases
3.10. Cutaneous Lymphoma
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beck, L.A.; Thaçi, D.; Hamilton, J.D.; Graham, N.M.; Bieber, T.; Rocklin, R.; Ming, J.E.; Ren, H.; Kao, R.; Simpson, E.; et al. Dupilumab Treatment in Adults with Moderate-to-Severe Atopic Dermatitis. N. Engl. J. Med. 2014, 371, 130–139. [Google Scholar] [CrossRef]
- Deleuran, M.; Thaçi, D.; Beck, L.A.; de Bruin-Weller, M.; Blauvelt, A.; Forman, S.; Bissonnette, R.; Reich, K.; Soong, W.; Hussain, I.; et al. Dupilumab shows long-term safety and efficacy in patients with moderate to severe atopic dermatitis enrolled in a phase 3 open-label extension study. J. Am. Acad. Dermatol. 2020, 82, 377–388. [Google Scholar] [CrossRef]
- Beck, L.A.; Thaçi, D.; Deleuran, M.; Blauvelt, A.; Bissonnette, R.; De Bruin-Weller, M.; Hide, M.; Sher, L.; Hussain, I.; Chen, Z.; et al. Dupilumab Provides Favorable Safety and Sustained Efficacy for up to 3 Years in an Open-Label Study of Adults with Moderate-to-Severe Atopic Dermatitis. Am. J. Clin. Dermatol. 2020, 21, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Bissonnette, R.; Ungar, B.; Suárez-Fariñas, M.; Ardeleanu, M.; Esaki, H.; Suprun, M.; Estrada, Y.; Xu, H.; Peng, X.; et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 143, 155–172. [Google Scholar] [CrossRef] [PubMed]
- Berdyshev, E.; Goleva, E.; Bissonnette, R.; Bronova, I.; Bronoff, A.S.; Richers, B.N.; Garcia, S.; Ramirez-Gama, M.; Taylor, P.; Praestgaard, A.; et al. Dupilumab significantly improves skin barrier function in patients with moderate-to-severe atopic dermatitis. Allergy 2022, 77, 3388–3397. [Google Scholar] [CrossRef]
- Napolitano, M.; Maffei, M.; Patruno, C.; Leone, C.A.; Di Guida, A.; Potestio, L.; Scalvenzi, M.; Fabbrocini, G. Dupilumab effectiveness for the treatment of patients with concomitant atopic dermatitis and chronic rhinosinusitis with nasal polyposis. Dermatol. Ther. 2021, 34, e15120. [Google Scholar] [CrossRef]
- Rambhia, P.H.; Levitt, J.O. Recalcitrant prurigo nodularis treated successfully with dupilumab. JAAD Case Rep. 2019, 5, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.L.; Savage, K.T.; Qiu, C.C.; Jin, A.; Valdes-Rodriguez, R.; Mollanazar, N.K. Chronic Pruritus Responding to Dupilumab—A Case Series. Medicines 2019, 6, 72. [Google Scholar] [CrossRef] [PubMed]
- Calugareanu, A.; Jachiet, M.; Lepelletier, C.; De Masson, A.; Rybojad, M.; Bagot, M.; Bouaziz, J. Dramatic improvement of generalized prurigo nodularis with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e303–e304. [Google Scholar] [CrossRef]
- Almustafa, Z.; Weller, K.; Autenrieth, J.; Maurer, M.; Metz, M. Dupilumab in Treatment of Chronic Prurigo: A Case Series and Literature Review. Acta Derm.-Venereol. 2019, 99, 905–906. [Google Scholar] [CrossRef]
- Beck, K.M.; Yang, E.J.; Sekhon, S.; Bhutani, T.; Liao, W. Dupilumab Treatment for Generalized Prurigo Nodularis. JAMA Dermatol. 2019, 155, 118. [Google Scholar] [CrossRef]
- Tanis, R.; Ferenczi, K.; Payette, M. Dupilumab Treatment for Prurigo Nodularis and Pruritis. J. Drugs Dermatol. 2019, 18, 940–942. [Google Scholar] [PubMed]
- Mollanazar, N.K.; Elgash, M.; Weaver, L.; Valdes-Rodriguez, R.; Hsu, S. Reduced Itch Associated with Dupilumab Treatment In 4 Patients with Prurigo Nodularis. JAMA Dermatol. 2019, 155, 121–122. [Google Scholar] [CrossRef]
- Wieser, J.K.; Mercurio, M.G.; Somers, K. Resolution of Treatment-Refractory Prurigo Nodularis with Dupilumab: A Case Series. Cureus 2020, 12, e8737. [Google Scholar] [CrossRef]
- Calugareanu, A.; Jachiet, M.; Tauber, M.; Nosbaum, A.; Aubin, F.; Misery, L.; Droitcourt, C.; Barbarot, S.; Debarbieux, S.; Saussine, A.; et al. Effectiveness and safety of dupilumab for the treatment of prurigo nodularis in a French multicenter adult cohort of 16 patients. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e74–e76. [Google Scholar] [CrossRef]
- Napolitano, M.; Fabbrocini, G.; Scalvenzi, M.; Nisticò, S.P.; Dastoli, S.; Patruno, C. Effectiveness of Dupilumab for the Treatment of Generalized Prurigo Nodularis Phenotype of Adult Atopic Dermatitis. Dermatitis 2020, 31, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Kovács, B.; Rose, E.; Kuznik, N.; Shimanovich, I.; Zillikens, D.; Ludwig, R.J.; Thaçi, D. Dupilumab for treatment-refractory prurigo nodularis. JDDG J. Dtsch. Dermatol. Ges. 2020, 18, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Criado, P.; Pincelli, T.P.; Criado, R.F.J. Dupilumab as a useful treatment option for prurigo nodularis in an elderly patient with atopic diathesis. Int. J. Dermatol. 2020, 59, e358–e361. [Google Scholar] [CrossRef]
- Giura, M.T.; Viola, R.; Fierro, M.T.; Ribero, S.; Ortoncelli, M. Efficacy of dupilumab in prurigo nodularis in elderly patient. Dermatol. Ther. 2020, 33, e13201. [Google Scholar] [CrossRef]
- Reynolds, M.T.; Dinehart, S.M.; Anderson, K.R.; Gorelick, J. Treatment of Recalcitrant Prurigo Nodularis with Dupilumab. Ski. J. Cutan. Med. 2020, 4, 279–283. [Google Scholar] [CrossRef]
- Holm, J.G.; Agner, T.; Sand, C.; Thomsen, S.F. Dupilumab for prurigo nodularis: Case series and review of the literature. Dermatol. Ther. 2020, 33, e13222. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Maurelli, M.; Gori, N.; Argenziano, G.; De Simone, C.; Calabrese, G.; Girolomoni, G.; Peris, K. Dupilumab improves clinical manifestations, symptoms, and quality of life in adult patients with chronic nodular prurigo. J. Am. Acad. Dermatol. 2020, 83, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Bloomstein, J.D.; Hawkes, J.E. Simultaneous treatment of Samter triad and prurigo nodularis with dupilumab. JAAD Case Rep. 2021, 18, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Georgakopoulos, J.R.; Croitoru, D.; Felfeli, T.; Alhusayen, R.; Lansang, P.; Shear, N.H.; Yeung, J.; Walsh, S. Long-term dupilumab treatment for chronic refractory generalized prurigo nodularis: A retrospective cohort study. J. Am. Acad. Dermatol. 2021, 85, 1049–1051. [Google Scholar] [CrossRef]
- Ferrucci, S.; Tavecchio, S.; Berti, E.; Angileri, L. Dupilumab and prurigo nodularis-like phenotype in atopic dermatitis: Our experience of efficacy. J. Dermatol. Treat. 2019, 32, 453–454. [Google Scholar] [CrossRef]
- Liu, T.; Bai, J.; Wang, S.; Ying, S.; Li, S.; Qiao, J.; Fang, H. Effectiveness of Dupilumab for an Elderly Patient with Prurigo Nodularis Who Was Refractory and Contradicted to Traditional Therapy. J. Asthma Allergy 2021, 14, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Romano, C. Safety and Effectiveness of Dupilumab in Prurigo Nodularis. J. Investig. Allergol. Clin. Immunol. 2021, 31, 162–163. [Google Scholar] [CrossRef]
- Tilotta, G.; Pistone, G.; Caruso, P.; Gurreri, R.; Castelli, E.; Curiale, S.; Caputo, V.; Bongiorno, M. Our experience with prurigo nodularis treated with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e285–e287. [Google Scholar] [CrossRef]
- Winkler, J.K.; Haenssle, H.A.; Enk, A.; Toberer, F.; Hartmann, M. Erfolgreiche Behandlung einer chronischen Prurigo mit Dupilumab. Der Hautarzt 2020, 72, 528–532. [Google Scholar] [CrossRef]
- Luo, N.; Wang, Q.; Lei, M.; Li, T.; Hao, P. Dupilumab for Chronic Prurigo in Different Backgrounds: A Case Series. Clin. Cosmet. Investig. Dermatol. 2022, 15, 1863–1867. [Google Scholar] [CrossRef]
- Lönndahl, L.; Lundqvist, M.; Bradley, M.; Johansson, E.K. Dupilumab Significantly Reduces Symptoms of Prurigo Nodularis and Depression: A Case Series. Acta Derm. Venereol. 2022, 102, adv00754. [Google Scholar] [CrossRef] [PubMed]
- Mitsuyama, S.; Higuchi, T. Effectiveness of dupilumab for chronic prurigo in elderly patients with atopic dermatitis. An. Bras. Dermatol. 2022, 98, 86–89. [Google Scholar] [CrossRef]
- Gade, A.; Ghani, H.; Rubenstein, R. Dupilumab; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK585114/ (accessed on 6 December 2022).
- Muzumdar, S.; Skudalski, L.; Sharp, K.; Waldman, R.A. Dupilumab Facial Redness/Dupilumab Facial Dermatitis: A Guide for Clinicians. Am. J. Clin. Dermatol. 2022, 23, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, A.J.; Yosipovitch, G.; Shi, V.Y. Dupilumab use in dermatologic conditions beyond atopic dermatitis—A systematic review. J. Dermatol. Treat. 2021, 32, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Maloney, N.J.; Tegtmeyer, K.; Zhao, J.; Worswick, S. Dupilumab in Dermatology: Potential for Uses Beyond Atopic Dermatitis. J. Drugs Dermatol. 2019, 18, S1545961619P1053X. [Google Scholar]
- Jia, F.; Zhao, Q.; Shi, P.; Liu, H.; Zhang, F. Dupilumab: Advances in the off-label usage of IL4 / IL13 antagonist in dermatoses. Dermatol. Ther. 2022, 35, e15924. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- OCEBM Levels of Evidence Working Group. ‘The Oxford Levels of Evidence 2’. Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 28 March 2023).
- Patruno, C.; Stingeni, L.; Hansel, K.; Ferrucci, S.M.; Tavecchio, S.; Fabbrocini, G.; Nisticò, S.P.; Foti, C.; De Prezzo, S.; Napolitano, M. Effectiveness of dupilumab for the treatment of nummular eczema phenotype of atopic dermatitis in adults. Dermatol. Ther. 2020, 33, e13290. [Google Scholar] [CrossRef]
- Choi, S.; Zhu, G.A.; Lewis, M.A.; Honari, G.; Chiou, A.S.; Ko, J.; Chen, J.K. Dupilumab treatment of nummular dermatitis: A retrospective cohort study. J. Am. Acad. Dermatol. 2020, 82, 1252–1255. [Google Scholar] [CrossRef]
- Dhingra, N.; Shemer, A.; da Rosa, J.C.; Rozenblit, M.; Fuentes-Duculan, J.; Gittler, J.K.; Finney, R.; Czarnowicki, T.; Zheng, X.; Xu, H.; et al. Molecular profiling of contact dermatitis skin identifies allergen-dependent differences in immune response. J. Allergy Clin. Immunol. 2014, 134, 362–372. [Google Scholar] [CrossRef]
- Machler, B.C.; Sung, C.T.; Darwin, E.; Jacob, S.E. Dupilumab use in allergic contact dermatitis. J. Am. Acad. Dermatol. 2019, 80, 280–281.e1. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.; Balogh, E.; Rayhan, D.; Shitabata, P.; Yousefzadeh, D.; Feldman, S. Chromate-Induced Allergic Contact Dermatitis Treated with Dupilumab. J. Drugs Dermatol. 2021, 20, 1340–1342. [Google Scholar] [CrossRef] [PubMed]
- Arasu, A.; Ross, G. Treatment of generalised isobornyl acrylate contact allergy from diabetes pump with Dupilumab. Australas. J. Dermatol. 2022, 63, e91–e93. [Google Scholar] [CrossRef] [PubMed]
- Ruge, I.F.; Skov, L.; Zachariae, C.; Thyssen, J.P. Dupilumab treatment in two patients with severe allergic contact dermatitis caused by sesquiterpene lactones. Contact Dermat. 2020, 83, 137–139. [Google Scholar] [CrossRef]
- Zhu, G.A.; Chen, J.K.; Chiou, A.; Ko, J.; Honari, G. Repeat patch testing in a patient with allergic contact dermatitis improved on dupilumab. JAAD Case Rep. 2019, 5, 336–338. [Google Scholar] [CrossRef]
- Goldminz, A.M.; Scheinman, P.L. A case series of dupilumab-treated allergic contact dermatitis patients. Dermatol. Ther. 2018, 31, e12701. [Google Scholar] [CrossRef]
- Slodownik, D.; Levi, A.; Lapidoth, M.; Moshe, S. Occupational Chronic Contact Dermatitis Successfully Treated with Dupilumab: A Case Series. Dermatology 2022, 238, 1073–1075. [Google Scholar] [CrossRef]
- Joshi, S.R.; Khan, D.A. Effective Use of Dupilumab in Managing Systemic Allergic Contact Dermatitis. Dermatitis® 2018, 29, 282–284. [Google Scholar] [CrossRef]
- Suresh, R.; Murase, J.E. The role of expanded series patch testing in identifying causality of residual facial dermatitis following initiation of dupilumab therapy. JAAD Case Rep. 2018, 4, 899–904. [Google Scholar] [CrossRef]
- Collantes-Rodríguez, C.; Jiménez-Gallo, D.; García, L.O.; Villegas-Romero, I.; Linares-Barrios, M. Recall dermatitis at patch test sites in an atopic dermatitis patient treated with dupilumab. Contact Dermat. 2019, 80, 69–70. [Google Scholar] [CrossRef]
- Chipalkatti, N.; Lee, N.; Zancanaro, P.; Dumont, N.; Donovan, C.; Rosmarin, D. Dupilumab as a Treatment for Allergic Contact Dermatitis. Dermatitis® 2018, 29, 347–348. [Google Scholar] [CrossRef]
- Chipalkatti, N.; Lee, N.; Zancanaro, P.; Dumont, N.; Kachuk, C.; Rosmarin, D. A retrospective review of dupilumab for atopic dermatitis patients with allergic contact dermatitis. J. Am. Acad. Dermatol. 2019, 80, 1166–1167. [Google Scholar] [CrossRef]
- Jacob, S.E.; Sung, C.T.; Machler, B.C. Dupilumab for Systemic Allergy Syndrome with Dermatitis. Dermatitis 2019, 30, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Stout, M.; Silverberg, J.I. Variable impact of dupilumab on patch testing results and allergic contact dermatitis in adults with atopic dermatitis. J. Am. Acad. Dermatol. 2019, 81, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Jin, P.; Yang, C.; Bai, J.; Dong, L.; Zhi, L. Successfully treatment with Dupilumab for systemic contact dermatitis following hair dye in a patient with dermatomyositis. J. Cosmet. Dermatol. 2022, 21, 6468–6469. [Google Scholar] [CrossRef]
- Gallo, R.; Oddenino, G.; Trave, I.; Gasparini, G.; Guadagno, A.; Parodi, A. Contact sensitivity to sesquiterpene lactone mix and artichoke in a patient with severe recurrent dermatitis: A puzzling case. Contact Dermat. 2023, 88, 156–158. [Google Scholar] [CrossRef]
- Koh, Y.; Park, J.; Shin, S.; Kim, B.; Yoo, K. Dupilumab for the treatment of refractory allergic contact dermatitis from rubber/latex concomitant with atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e640–e643. [Google Scholar] [CrossRef] [PubMed]
- E Koblinski, J.; Hamann, D. Mixed occupational and iatrogenic allergic contact dermatitis in a hairdresser. Occup. Med. 2020, 70, 523–526. [Google Scholar] [CrossRef]
- Mainville, L.; Veillette, H.; Houle, M. Sequential patch testing in a patient treated with dupilumab then with upadacitinib: Differences in patch test results as well as in disease control. Contact Dermat. 2023, 1, 1–3. [Google Scholar] [CrossRef]
- Jo, C.E.; Mufti, A.; Sachdeva, M.; Pratt, M.; Yeung, J. Effect of dupilumab on allergic contact dermatitis and patch testing. J. Am. Acad. Dermatol. 2021, 84, 1772–1776. [Google Scholar] [CrossRef]
- Waldman, R.A.; DeWane, M.E.; Sloan, B.; Grant-Kels, J.M.; Lu, J. Dupilumab for the treatment of dyshidrotic eczema in 15 consecutive patients. J. Am. Acad. Dermatol. 2020, 82, 1251–1252. [Google Scholar] [CrossRef] [PubMed]
- Weins, A.B.; Biedermann, T.; Eyerich, K.; Moeckel, S.; Schnopp, C. Successful treatment of recalcitrant dyshidrotic eczema with dupilumab in a child. JDDG J. Dtsch. Dermatol. Ges. 2019, 17, 1165–1167. [Google Scholar] [CrossRef] [PubMed]
- Olesen, C.M.; Yüksel, Y.T.; Zachariae, C.; Lund, T.T.; Agner, T.; Petersen, T.S.; Thyssen, J.P. Treatment of chronic hand eczema with dupilumab—A retrospective follow-up study. J. Eur. Acad. Dermatol. Venereol. 2022, 37, e557–e559. [Google Scholar] [CrossRef] [PubMed]
- Voorberg, A.N.; Romeijn, G.L.E.; de Bruin-Weller, M.S.; Schuttelaar, M.L.A. The long-term effect of dupilumab on chronic hand eczema in patients with moderate to severe atopic dermatitis—52 week results from the Dutch BioDay Registry. Contact Dermat. 2022, 87, 185–191. [Google Scholar] [CrossRef]
- Loman, L.; Diercks, G.F.; Schuttelaar, M.L. Three cases of non-atopic hyperkeratotic hand eczema treated with dupilumab. Contact Dermat. 2021, 84, 124–127. [Google Scholar] [CrossRef]
- Zhu, G.A.; Honari, G.; Ko, J.M.; Chiou, A.S.; Chen, J.K. Dupilumab for occupational irritant hand dermatitis in a nonatopic individual: A case report. JAAD Case Rep. 2020, 6, 296–298. [Google Scholar] [CrossRef]
- Halling, A.; Zachariae, C.; Thyssen, J.P. Severe treatment-resistant acute and recurrent vesicular chronic hand eczema successfully treated with dupilumab. Contact Dermat. 2020, 83, 37–38. [Google Scholar] [CrossRef]
- Oosterhaven, J.A.; Voorberg, A.N.; Romeijn, G.L.; De Bruin-Weller, M.S.; Schuttelaar, M.L. Effect of dupilumab on hand eczema in patients with atopic dermatitis: An observational study. J. Dermatol. 2019, 46, 680–685. [Google Scholar] [CrossRef]
- Lee, N.; Chipalkatti, N.; Zancanaro, P.; Kachuk, C.; Dumont, N.; Rosmarin, D. A Retrospective Review of Dupilumab for Hand Dermatitis. Dermatology 2019, 235, 187–188. [Google Scholar] [CrossRef]
- Oosterhaven, J.A.F.; Romeijn, G.L.E.; Schuttelaar, M.L.A. Dupilumab Treatment of Very Severe Refractory Atopic Hand Eczema. JAMA Dermatol. 2018, 154, 969. [Google Scholar] [CrossRef]
- Zirwas, M.J. Dupilumab for hand eczema. J. Am. Acad. Dermatol. 2018, 79, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Weston, G.K.; Hooper, J.; E Strober, B. Dupilumab in the Treatment of Dyshidrosis: A Report of Two Cases. J. Drugs Dermatol. 2018, 17, 355–356. [Google Scholar]
- Nanda, S.; Nagrani, N.; MacQuhae, F.; Nichols, A. A Case of Complete Resolution of Severe Plantar Dyshidrotic Eczema With Dupilumab. J. Drugs Dermatol. 2019, 18, 211–212. [Google Scholar] [PubMed]
- Li, Y.; Xiao, J.; Sun, Y.; Fang, H.; Qiao, J. Quick Treatment of Very Severe Refractory Hand and Foot Eczema with Dupilumab: A Case Report and Literature Review. J. Asthma Allergy 2023, 16, 1–8. [Google Scholar] [CrossRef]
- A Gall, R.; Peters, J.D.; Brinker, A.J. Two Cases of Recalcitrant Dyshidrotic Eczema Treated with Dupilumab. J. Drugs Dermatol. 2021, 20, 558–559. [Google Scholar]
- Gan, H.; Gao, Y.-D. Occupational Chronic Hand Dermatitis in Hospital Environment Successfully Treated with Dupilumab: A Case Report. Iran. J. Allergy Asthma Immunol. 2022, 21, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Genco, L.; Noto, M.; Patruno, C.; Fabbrocini, G.; Napolitano, M. Eczematous eruption after brodalumab successfully treated with guselkumab and dupilumab. Dermatol. Ther. 2022, 35, e15839. [Google Scholar] [CrossRef]
- Koschitzky, M.; Tan, K.; Encarnacion, M.R.N.; Rivera-Oyola, R.; Khattri, S. Eczematous reactions to psoriasis biologics treated with dupilumab: A case series. JAAD Case Rep. 2021, 11, 29–32. [Google Scholar] [CrossRef]
- Shahriari, N.; Strober, B.; Shahriari, M. The role of dupilumab in the management of idiopathic chronic eczematous eruption of aging. J. Am. Acad. Dermatol. 2020, 83, 1533–1535. [Google Scholar] [CrossRef]
- Brummer, G.C.; Wang, L.T.; Sontheimer, R.D. A possible role for dupilumab (Dupixent) in the management of idiopathic chronic eczematous eruption of aging. Dermatol. Online J. 2018, 24. [Google Scholar] [CrossRef]
- Votquenne, N.; Dupire, G.; Michel, O.; Ben Said, B. Dupilumab for severe generalized eczematous eruption complicating common variable immunodeficiency. Eur. J. Dermatol. 2021, 31, 93–94. [Google Scholar] [CrossRef]
- Schrom, K.P.; Kobs, A.; Nedorost, S. Clinical Psoriasiform Dermatitis Following Dupilumab Use for Autoeczematization Secondary to Chronic Stasis Dermatitis. Cureus 2020, 12, e7831. [Google Scholar] [CrossRef] [PubMed]
- Oetjen, L.K.; Mack, M.R.; Feng, J.; Whelan, T.M.; Niu, H.; Guo, C.J.; Chen, S.; Trier, A.M.; Xu, A.Z.; Tripathi, S.V.; et al. Sensory Neurons Co-opt Classical Immune Signaling Pathways to Mediate Chronic Itch. Cell 2017, 171, 217–228.e13. [Google Scholar] [CrossRef] [PubMed]
- Fachler, T.; Faitataziadou, S.M.; Molho-Pessach, V. Dupilumab for pediatric prurigo nodularis: A case report. Pediatr. Dermatol. 2021, 38, 334–335. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Mori, F.; Oranges, T.; Ricci, S.; Barni, S.; Canessa, C.; Liccioli, G.; Lodi, L.; Sarti, L.; Novembre, E.; et al. Dupilumab treatment of prurigo nodularis in an adolescent. Eur. J. Dermatol. 2021, 31, 104–106. [Google Scholar] [CrossRef]
- Edmonds, N.; Noland, M.; Flowers, R.H. Six cases of refractory pruritus and histologic dermal hypersensitivity reaction successfully treated with dupilumab. JAAD Case Rep. 2022, 19, 28–33. [Google Scholar] [CrossRef]
- Jeon, J.; Wang, F.; Badic, A.; Kim, B.S. Treatment of patients with chronic pruritus of unknown origin with dupilumab. J. Dermatol. Treat. 2022, 33, 1754–1757. [Google Scholar] [CrossRef] [PubMed]
- Stanger, R.; Rivera-Oyola, R.; Lebwohl, M. Dupilumab as a treatment for generalized idiopathic pruritus: A report of two cases. Br. J. Dermatol. 2020, 182, 1494–1495. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Brieva, J. A successful case of dupilumab treatment for severe uremic pruritus. JAAD Case Rep. 2019, 5, 339–341. [Google Scholar] [CrossRef]
- Chovatiya, R.; Brieva, J.; Hung, A. Dupilumab treatment for cholestatic pruritus. Dermatol. Ther. 2022, 35, e15296. [Google Scholar] [CrossRef]
- Abel, M.K.; Ashbaugh, A.G.; Stone, H.F.; Murase, J.E. The use of dupilumab for the treatment of recalcitrant brachioradial pruritus. JAAD Case Rep. 2021, 10, 69–71. [Google Scholar] [CrossRef]
- Yang, E.; Murase, J. Recalcitrant anal and genital pruritus treated with dupilumab. Int. J. Womens Dermatol. 2018, 4, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Lee, J.H.; Choi, J.E.; Han, T.Y. Treatment of acquired reactive perforating collagenosis with dupilumab in a patient with end-stage renal disease. Dermatol. Ther. 2022, 35, e15926. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zeng, Y.; Jin, H. Reactive perforating collagenosis treated with dupilumab: A case report and literature review. Dermatol. Ther. 2022, 35, e15916. [Google Scholar] [CrossRef]
- Alsebayel, M.M.; Alzaid, T.; Alobaida, S.A. Dupilumab in acquired perforating dermatosis: A potential new treatment. JAAD Case Rep. 2022, 28, 34–36. [Google Scholar] [CrossRef]
- Gil-Lianes, J.; Loughlin, C.R.; Mascaró, J.M. Reactive perforating collagenosis successfully treated with dupilumab. Australas. J. Dermatol. 2022, 63, 398–400. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.; Shuang, C.; Zhen-Ying, Z. Dupilumab may be an alternative option in the treatment of acquired reactive perforating collagenosis combined with AD. Immunity Inflamm. Dis. 2022, 10, e574. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, R.J.; Vanhoorelbeke, K.; Leypoldt, F.; Kaya, Z.; Bieber, K.; McLachlan, S.M.; Komorowski, L.; Luo, J.; Cabral-Marques, O.; Hammers, C.M.; et al. Mechanisms of Autoantibody-Induced Pathology. Front. Immunol. 2017, 8, 603. [Google Scholar] [CrossRef]
- Has, C.; Bauer, J.W.; Bodemer, C.; Bolling, M.C.; Bruckner-Tuderman, L.; Diem, A.; Fine, J.-D.; Heagerty, A.; Hovnanian, A.; Marinkovich, M.P.; et al. Consensus reclassification of inherited epidermolysis bullosa and other disorders with skin fragility. Br. J. Dermatol. 2020, 183, 614–627. [Google Scholar] [CrossRef]
- Kridin, K.; Ludwig, R. The Growing Incidence of Bullous Pemphigoid: Overview and Potential Explanations. Front. Med. 2018, 5, 220. [Google Scholar] [CrossRef]
- Schmidt, E.; Zillikens, D. Pemphigoid diseases. Lancet 2013, 381, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Van Beek, N.; Lüttmann, N.; Huebner, F.; Recke, A.; Karl, I.; Schulze, F.S.; Zillikens, D.; Schmidt, E. Correlation of Serum Levels of IgE Autoantibodies Against BP180 With Bullous Pemphigoid Disease Activity. JAMA Dermatol. 2017, 153, 30–38. [Google Scholar] [CrossRef]
- Zhang, X.; Man, X.; Tang, Z.; Dai, R.; Shen, Y. Dupilumab as a novel therapy for bullous pemphigoid. Int. J. Dermatol. 2022, 62, e263–e266. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Song, W.; Cai, Y.; Huang, R.; Wei, J.; Liu, H.; Peng, X.; Zeng, K.; Li, C. Successful treatment of eczema-like bullous pemphigoid and typical bullous pemphigoid with dupilumab: Two case reports. Int. J. Dermatol. 2022, 62, e144–e146. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Wang, J.; Shi, B. Case report: Dupilumab for the treatment of bullous pemphigoid. Dermatol. Ther. 2022, 35, e15541. [Google Scholar] [CrossRef]
- Liu, X.; Ma, J.; Qiu, X.; Hong, D.; Wang, L.; Shi, Z. Dupilumab, an emerging therapeutic choice for recalcitrant subepidermal autoimmune bullous diseases: A case series of three patients. Eur. J. Dermatol. 2021, 31, 846–847. [Google Scholar] [CrossRef]
- Shan, Y.; Zuo, Y. A successful case of vesicular pemphigoid concurrent with pulmonary tuberculosis with dupilumab. Dermatol. Ther. 2022, 35, e15330. [Google Scholar] [CrossRef]
- Bal, A.; Sorensen, A.; Ondreyco, S.M. Nonbullous erythrodermic pemphigoid with florid lymphadenopathy, response to dupilumab. JAAD Case Rep. 2021, 17, 58–60. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Chen, J.; Lin, M.; Gong, T.; Cheng, B.; Ji, C. Dupilumab successfully treated refractory bullous pemphigoid with early clinical manifestations imitating atopic dermatitis: A case letter. Australas. J. Dermatol. 2021, 62, 525–527. [Google Scholar] [CrossRef]
- Saleh, M.; Reedy, M.; Torok, H.; Weaver, J. Successful treatment of bullous pemphigoid with dupilumab: A case and brief review of the literature. Dermatol. Online J. 2021, 27. [Google Scholar] [CrossRef]
- Jafari, S.M.S.; Feldmeyer, L.; Bossart, S.; Simon, D.; Schlapbach, C.; Borradori, L. Case Report: Combination of Omalizumab and Dupilumab for Recalcitrant Bullous Pemphigoid. Front. Immunol. 2020, 11, 611549. [Google Scholar] [CrossRef] [PubMed]
- Abdat, R.; Waldman, R.A.; de Bedout, V.; Czernik, A.; Mcleod, M.; King, B.; Gordon, S.; Ahmed, R.; Nichols, A.; Rothe, M.; et al. Dupilumab as a novel therapy for bullous pemphigoid: A multicenter case series. J. Am. Acad. Dermatol. 2020, 83, 46–52. [Google Scholar] [CrossRef]
- Seidman, J.S.; Eichenfield, D.Z.; Orme, C.M. Dupilumab for bullous pemphigoid with intractable pruritus. Dermatol. Online J. 2019, 25. [Google Scholar] [CrossRef]
- Tseng, H.-C.; Lai, P.-T. Refractory bullous pemphigoid with prurigo nodularis successfully treated with dupilumab monotherapy. Dermatol. Sin. 2022, 40, 237. [Google Scholar] [CrossRef]
- Zhou, A.E.; Shao, K.; Ferenczi, K.; Adalsteinsson, J.A. Recalcitrant bullous pemphigoid responsive to dupilumab in an adolescent patient. JAAD Case Rep. 2022, 29, 149–151. [Google Scholar] [CrossRef]
- Li, W.; Cai, S.; Man, X. The treatment of refractory atypical bullous pemphigoid with generalized eczema and intense pruritus with dupilumab. Dermatol. Ther. 2022, 35, e15243. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.; Gordon, S.C.; Deverapalli, S.C.; Her, M.J.; Rosmarin, D. Dupilumab for the Treatment of Recalcitrant Bullous Pemphigoid. JAMA Dermatol. 2018, 154, 1225. [Google Scholar] [CrossRef]
- Savoldy, M.A.; Tadicherla, T.; Moureiden, Z.; Ayoubi, N.; Baldwin, B.T. The Successful Treatment of COVID-19-Induced Bullous Pemphigoid With Dupilumab. Cureus 2022, 14, e30541. [Google Scholar] [CrossRef]
- Bruni, M.; Moar, A.; Schena, D.; Girolomoni, G. A case of nivolumab-induced bullous pemphigoid successfully treated with dupilumab. Dermatol. Online J. 2022, 28, 1–5. [Google Scholar] [CrossRef]
- Pop, S.R.; Strock, D.; Smith, R.J. Dupilumab for the treatment of pembrolizumab-induced bullous pemphigoid: A case report. Dermatol. Ther. 2022, 35, e15623. [Google Scholar] [CrossRef]
- Klepper, E.M.; Robinson, H.N. Dupilumab for the treatment of nivolumab-induced bullous pemphigoid: A case report and review of the literature. Dermatol. Online J. 2021, 27. [Google Scholar] [CrossRef] [PubMed]
- Khazaeli, M.; Grover, R.; Pei, S. Concomitant nivolumab associated Grover disease and bullous pemphigoid in a patient with metastatic renal cell carcinoma. J. Cutan. Pathol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Baffa, M.E.; Maglie, R.; Montefusco, F.; Pipitò, C.; Senatore, S.; Antiga, E. Severe bullous pemphigoid following COVID-19 vaccination resistant to rituximab and successfully treated with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2022, 37, e135–e137. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Gao, H.; Zhang, Z.; Tang, C.; Chen, Z.; Wang, L.; Yang, F.; Chen, S.; He, S.; Liu, S.; et al. Dupilumab combined with low-dose systemic steroid therapy improves efficacy and safety for bullous pemphigoid. Dermatol. Ther. 2022, 35, e15648. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, Q.; Chen, L.; Chen, J.; Zhang, J.; Zou, Y.; Gong, T.; Ji, C. Efficacy and Safety of Dupilumab in Moderate-to-Severe Bullous Pemphigoid. Front. Immunol. 2021, 12, 4144. [Google Scholar] [CrossRef] [PubMed]
- Loughlin, C.R.; Mascaró, J.M. Treatment of pemphigoid gestationis with dupilumab. Clin. Exp. Dermatol. 2021, 46, 1578–1579. [Google Scholar] [CrossRef]
- Li, S.-Z.; Xie, Y.-H.; Wang, S.-H.; Fang, R.-Y.; Jin, H.-Z.; Zuo, Y.-G. Case report: Successful treatment of non-bullous lichen planus pemphigoides with dupilumab. Front. Med. 2022, 9, 3735. [Google Scholar] [CrossRef]
- Ch’en, P.Y.; Song, E.J. Lichen planus pemphigoides successfully treated with dupilumab. JAAD Case Rep. 2023, 31, 56–58. [Google Scholar] [CrossRef]
- Blum, F.R.; Sigmon, J.R. Successful treatment of Brunsting-Perry pemphigoid with dupilumab. JAAD Case Rep. 2021, 10, 107–109. [Google Scholar] [CrossRef]
- Raef, H.S.; Elmariah, S.B. Successful Treatment of Brunsting-Perry Cicatricial Pemphigoid With Dupilumab. J. Drugs Dermatol. JDD 2021, 20, 1113–1115. [Google Scholar] [CrossRef]
- Jendoubi, F.; Bost, C.; Tournier, E.; Paul, C.; Konstantinou, M.P. Severe pemphigoid nodularis successfully treated with dupilumab. Dermatol. Ther. 2022, 35, e15727. [Google Scholar] [CrossRef] [PubMed]
- Valenti, M.; De Giacomo, P.; Lavecchia, A.; Valenti, G. A severe case of IgA bullous pemphigoid successfully treated with dupilumab. Dermatol. Ther. 2022, 35, e15890. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, E.; Kasperkiewicz, M.; Joly, P. Pemphigus. Lancet 2019, 394, 882–894. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.Y.; Hurley, K. Dupilumab monotherapy suppresses recalcitrant pemphigus vulgaris. JAAD Case Rep. 2023, 31, 16–18. [Google Scholar] [CrossRef]
- Chen, S.; Zhan, S.; Hua, C.; Tang, Y.; Cheng, H. A Novel Combined Use of Dupilumab for Treatment of Aggressive Refractory Pemphigus Vulgaris Complicated with Pulmonary Tuberculosis: A Case Report and the RNA-seq Analysis. Front. Immunol. 2022, 13, 234. [Google Scholar] [CrossRef]
- Kasperkiewicz, M.; Ellebrecht, C.T.; Takahashi, H.; Yamagami, J.; Zillikens, D.; Payne, A.S.; Amagai, M. Pemphigus. Nat. Rev. Dis. Primers. 2017, 3, 1–18. [Google Scholar] [CrossRef]
- Shehadeh, W.; Sarig, O.; Bar, J.; Sprecher, E.; Samuelov, L. Treatment of epidermolysis bullosa pruriginosa-associated pruritus with dupilumab. Br. J. Dermatol. 2020, 182, 1495–1497. [Google Scholar] [CrossRef]
- Bs, A.G.Z.; Little, A.J.; Antaya, R.J. Epidermolysis bullosa pruriginosa treated with dupilumab. Pediatr. Dermatol. 2021, 38, 526–527. [Google Scholar] [CrossRef]
- Clawson, R.C.; Duran, S.F.; Pariser, R.J. Epidermolysis bullosa pruriginosa responding to dupilumab. JAAD Case Rep. 2021, 16, 69–71. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, M.; Zhang, L.; Zheng, S.; Hong, Y.; Gao, X. Amelioration of dystrophic epidermolysis bullosa pruriginosa symptoms with dupilumab: A case report. Dermatol. Ther. 2021, 34, e15130. [Google Scholar] [CrossRef]
- Caroppo, F.; Milan, E.; Giulioni, E.; Fortina, A.B. A case of dystrophic epidermolysis bullosa pruriginosa treated with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e365–e367. [Google Scholar] [CrossRef] [PubMed]
- Licata, G.; Buononato, D.; Calabrese, G.; Gambardella, A.; Briatico, G.; Pagliuca, F.; Argenziano, G. A case of Hailey-Hailey disease successfully treated with dupilumab. Int. J. Dermatol. 2022, 61, 1427–1428. [Google Scholar] [CrossRef] [PubMed]
- Alamon-Reig, F.; Serra-García, L.; Bosch-Amate, X.; Loughlin, C.R.; Mascaró, J. Dupilumab in Hailey-Hailey disease: A case series. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e776–e779. [Google Scholar] [CrossRef]
- Alzahrani, N.; Grossman-Kranseler, J.; Swali, R.; Fiumara, K.; Zancanaro, P.; Tyring, S.; Rosmarin, D. Hailey–Hailey disease treated with dupilumab: A case series. Br. J. Dermatol. 2021, 185, 680–682. [Google Scholar] [CrossRef] [PubMed]
- Shelton, E.; Doolittle, C.; Shinohara, M.M.; Thompson, J.A.; Moshiri, A.S. Can’t handle the itch? Refractory immunotherapy-related transient acantholytic dermatosis: Prompt resolution with dupilumab. JAAD Case Rep. 2022, 22, 31–33. [Google Scholar] [CrossRef]
- Butler, D.C.; Kollhoff, A.; Berger, T. Treatment of Grover Disease with Dupilumab. JAMA Dermatol. 2021, 157, 353. [Google Scholar] [CrossRef]
- Barei, F.; Torretta, S.; Morini, N.; Ferrucci, S. A case of Grover disease treated with Dupilumab: Just serendipity or a future perspective? Dermatol. Ther. 2022, 35, e15429. [Google Scholar] [CrossRef]
- Ito, T.; Kageyama, R.; Nakazawa, S.; Honda, T. Understanding the significance of cytokines and chemokines in the pathogenesis of alopecia areata. Exp. Dermatol. 2020, 29, 726–732. [Google Scholar] [CrossRef]
- Andersen, Y.M.; Egeberg, A.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Autoimmune diseases in adults with atopic dermatitis. J. Am. Acad. Dermatol. 2017, 76, 274–280.e1. [Google Scholar] [CrossRef]
- Alotaibi, L.; Alfawzan, A.; Alharthi, R.; Al Sheikh, A. Improvement of atopic dermatitis and alopecia universalis with dupilumab: A case report. Dermatol. Rep. 2022, 14, 9359. [Google Scholar] [CrossRef]
- Romagnuolo, M.; Barbareschi, M.; Tavecchio, S.; Angileri, L.; Ferrucci, S.M. Remission of Alopecia Universalis after 1 Year of Treatment with Dupilumab in a Patient with Severe Atopic Dermatitis. Ski. Appendage Disord. 2022, 8, 38–41. [Google Scholar] [CrossRef]
- Call, J.E.; Sahni, S.; Zug, K.A. Effectiveness of Dupilumab in the treatment of both atopic dermatitis and alopecia universalis. Clin. Case Rep. 2020, 8, 1337–1339. [Google Scholar] [CrossRef] [PubMed]
- Szekely, S.; Vaccari, D.; Salmaso, R.; Belloni-Fortina, A.; Alaibac, M. Onset of Schamberg Disease and Resolution of Alopecia Areata During Treatment of Atopic Dermatitis with Dupilumab. J. Investig. Allergol. Clin. Immunol. 2021, 31, 65–66. [Google Scholar] [CrossRef] [PubMed]
- Babino, G.; Fulgione, E.; D’Ambra, I.; Calabrese, G.; Alfano, R.; Argenziano, G. Rapid hair regrowth induced by dupilumab in a patient affected by alopecia totalis of 28 years’ duration: Clinical and dermoscopic features. Dermatol. Ther. 2020, 33, e13582. [Google Scholar] [CrossRef] [PubMed]
- Ushida, M.; Ohshita, A.; Arakawa, Y.; Kanehisa, F.; Katoh, N.; Asai, J. Dupilumab therapy rapidly improved alopecia areata associated with trichotillomania in an atopic dermatitis patient. Allergol. Int. 2020, 69, 480–482. [Google Scholar] [CrossRef]
- Harada, K.; Irisawa, R.; Ito, T.; Uchiyama, M.; Tsuboi, R. The effectiveness of dupilumab in patients with alopecia areata who have atopic dermatitis: A case series of seven patients. Br. J. Dermatol. 2020, 183, 396–397. [Google Scholar] [CrossRef]
- Ludriksone, L.; Elsner, P.; Schliemann, S. Simultaneous effectiveness of dupilumab in atopic dermatitis and alopecia areata in two patients. JDDG J. Dtsch. Dermatol. Ges. 2019, 17, 1278–1280. [Google Scholar] [CrossRef]
- Magdaleno-Tapial, J.; Valenzuela-Oñate, C.; García-Legaz-Martínez, M.; Martínez-Domenech, Á.; Pérez-Ferriols, A. Improvement of alopecia areata with Dupilumab in a patient with severe atopic dermatitis and review the literature. Australas. J. Dermatol. 2020, 61, e223–e225. [Google Scholar] [CrossRef]
- Uchida, H.; Kamata, M.; Watanabe, A.; Agematsu, A.; Nagata, M.; Fukaya, S.; Hayashi, K.; Fukuyasu, A.; Tanaka, T.; Ishikawa, T.; et al. Dupilumab Improved Alopecia Areata in a Patient with Atopic Dermatitis: A Case Report. Acta Derm. Venereol. 2019, 99, 675–676. [Google Scholar] [CrossRef]
- Smogorzewski, J.; Sierro, T.; Compoginis, G.; Kim, G. Remission of alopecia universalis in a patient with atopic dermatitis treated with dupilumab. JAAD Case Rep. 2019, 5, 116–117. [Google Scholar] [CrossRef]
- Darrigade, A.-S.; Legrand, A.; Andreu, N.; Jacquemin, C.; Boniface, K.; Taïeb, A.; Seneschal, J. Dual efficacy of dupilumab in a patient with concomitant atopic dermatitis and alopecia areata. Br. J. Dermatol. 2018, 179, 534–536. [Google Scholar] [CrossRef]
- Patruno, C.; Napolitano, M.; Ferrillo, M.; Fabbrocini, G. Dupilumab and alopecia: A Janus effect. Dermatol. Ther. 2019, 32, e13023. [Google Scholar] [CrossRef]
- Alniemi, D.T.; McGevna, L. Dupilumab treatment for atopic dermatitis leading to unexpected treatment for alopecia universalis. JAAD Case Rep. 2019, 5, 111–112. [Google Scholar] [CrossRef]
- Flanagan, K.E.; Bs, I.M.P.W.; Ba, J.T.P.; Walker, C.J.; Senna, M.M. Dupilumab-induced psoriasis in a patient with atopic dermatitis and alopecia totalis: A case report and literature review. Dermatol. Ther. 2022, 35, e15255. [Google Scholar] [CrossRef]
- Muto, J.; Yoshida, S.; Doi, C.; Habu, M.; Sayama, K. Dupilumab treatment of atopic dermatitis leading to successful treatment of alopecia universalis: A Japanese case report. J. Dermatol. 2021, 48, e72–e73. [Google Scholar] [CrossRef]
- Sevray, M.; Dupré, D.; Misery, L.; Abasq-Thomas, C. Hair regrowth and dissemination of molluscum contagiosum: Two unexpected effects with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e296–e298. [Google Scholar] [CrossRef] [PubMed]
- Visconti, M.J.; Richardson, A.; LaFond, A.A. Visconti Dupilumab as a Therapeutic Approach in Alopecia Universalis. Cutis 2022, 110, E7–E8. [Google Scholar] [CrossRef] [PubMed]
- Fukuyama, M.; Kinoshita-Ise, M.; Mizukawa, Y.; Ohyama, M. Two-sided influence of dupilumab on alopecia areata co-existing with severe atopic dermatitis: A case series and literature review. J. Cutan. Immunol. Allergy 2023, 6, 13–17. [Google Scholar] [CrossRef]
- Choe, S.; Newman, E.M. Time to loss of response for dupilumab in ophiasis-pattern alopecia areata. JAAD Case Rep. 2021, 15, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Zilberstein, A.T.; Teng, E.L.; Mancini, A.J. Dupilumab, incontinentia pigmenti, and alopecia: A serendipitous observation. JAAD Case Rep. 2022, 29, 121–122. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, M.; Rohan, C.A.; Travers, J.B.; Serrao, R. Long-Term Efficacy of Dupilumab in Alopecia Areata. Am. J. Case Rep. 2022, 23, e936488. [Google Scholar] [CrossRef]
- Cho, S.K.; Craiglow, B.G. Dupilumab for the treatment of alopecia areata in children with atopic dermatitis. JAAD Case Rep. 2021, 16, 82–85. [Google Scholar] [CrossRef]
- McKenzie, P.L.; Castelo-Soccio, L. Dupilumab therapy for alopecia areata in pediatric patients with concomitant atopic dermatitis. J. Am. Acad. Dermatol. 2021, 84, 1691–1694. [Google Scholar] [CrossRef]
- Gruenstein, D.; Malik, K.; Levitt, J. Full scalp hair regrowth in a 4-year-old girl with alopecia areata and atopic dermatitis treated with dupilumab. JAAD Case Rep. 2020, 6, 1286–1287. [Google Scholar] [CrossRef]
- Penzi, L.R.; Yasuda, M.; Manatis-Lornell, A.; Hagigeorges, D.; Senna, M.M. Hair Regrowth in a Patient With Long-standing Alopecia Totalis and Atopic Dermatitis Treated With Dupilumab. JAMA Dermatol. 2018, 154, 1358–1360. [Google Scholar] [CrossRef]
- Napolitano, M.; Cantelli, M.; Potestio, L.; Ocampo-Garza, S.; Vastarella, M.; Nappa, P.; Scalvenzi, M.; Fabbrocini, G.; Patruno, C. Clinical, trichoscopic and in vivo reflectance confocal microscopy evaluation of alopecia areata in atopic dermatitis patients treated with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e561–e563. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Renert-Yuval, Y.; Bares, J.; Chima, M.; Hawkes, J.E.; Gilleaudeau, P.; Sullivan-Whalen, M.; Singer, G.K.; Garcet, S.; Pavel, A.B.; et al. Phase 2a randomized clinical trial of dupilumab (anti-IL-4Rα) for alopecia areata patients. Allergy 2022, 77, 897–906. [Google Scholar] [CrossRef]
- Ständer, S.; Trense, Y.; Thaçi, D.; Ludwig, R.J. Alopecia areata development in atopic dermatitis patients treated with dupilumab. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e612–e613. [Google Scholar] [CrossRef]
- McLeod, J.J.; Baker, B.; Ryan, J.J. Mast cell production and response to IL-4 and IL-13. Cytokine 2015, 75, 57–61. [Google Scholar] [CrossRef]
- Puxkandl, V.; Hoetzenecker, W.; Altrichter, S. Case report: Severe chronic spontaneous urticaria successfully treated with omalizumab and dupilumab. Allergol. Sel. 2023, 7, 17–19. [Google Scholar] [CrossRef]
- Sun, Y.; Lin, S.Y.; Lan, C.E. Dupilumab as a rescue therapy for a chronic urticaria patient who showed secondary failure to omalizumab. Kaohsiung J. Med. Sci. 2022, 38, 610–611. [Google Scholar] [CrossRef]
- Holm, J.G.; Sørensen, J.A.; Thomsen, S.F. Concurrent use of omalizumab and dupilumab in a 47-year-old woman with chronic spontaneous urticaria and atopic dermatitis. Int. J. Dermatol. 2022, 61, e173–e174. [Google Scholar] [CrossRef]
- Errichetti, E.; Stinco, G. Recalcitrant chronic urticaria treated with dupilumab: Report of two instances refractory to H1-antihistamines, omalizumab and cyclosporine and brief literature review. Dermatol. Ther. 2021, 34, e14821. [Google Scholar] [CrossRef]
- Lee, J.K.; Simpson, R.S. Dupilumab as a novel therapy for difficult to treat chronic spontaneous urticaria. J. Allergy Clin. Immunol. Pract. 2019, 7, 1659–1661.e1. [Google Scholar] [CrossRef]
- Abadeh, A.; Lee, J.K. Long-term follow-up of patients treated with dupilumab for chronic spontaneous urticaria: A case report. SAGE Open Med. Case Rep. 2022, 10, 2050313X221117702. [Google Scholar] [CrossRef]
- Staubach, P.; Peveling-Oberhag, A.; Lang, B.M.; Zimmer, S.; Sohn, A.; Mann, C. Severe chronic spontaneous urticaria in children—Treatment options according to the guidelines and beyond—A 10 years review. J. Dermatol. Treat. 2022, 33, 1–4. [Google Scholar] [CrossRef]
- Zhu, C.; Fok, J.S.; Lin, L.; Su, H.; Maurer, M. Complete response to dupilumab in a patient with chronic spontaneous urticaria who did not tolerate omalizumab. JAAD Case Rep. 2023, 32, 109–112. [Google Scholar] [CrossRef]
- Maurer, M.; Casale, T.; Saini, S.; Ben-Shoshan, M.; Amin, N.; Radin, A.; Akinlade, B.; Fan, C.; Bauer, D.; Laws, E.; et al. Dupilumab Significantly Reduces Itch and Hives in Patients with Chronic Spontaneous Urticaria: Results From a Phase 3 Trial (LIBERTY-CSU CUPID Study A). J. Allergy Clin. Immunol. 2022, 149, AB312. [Google Scholar] [CrossRef]
- Maurer, M.; Casale, T.; Saini, S.; Ben-Shoshan, M.; Radin, A.; Akinlade, B.; Laws, E.; Mannent, L. DUPILUMAB EFFICACY IN PATIENTS WITH CHRONIC SPONTANEOUS URTICARIA BY IGE LEVEL: LIBERTY-CSU CUPID STUDY A. Ann. Allergy Asthma Immunol. 2022, 129, S11. [Google Scholar] [CrossRef]
- Ferrucci, S.; Benzecry, V.; Berti, E.; Asero, R. Rapid disappearance of both severe atopic dermatitis and cold urticaria following dupilumab treatment. Clin. Exp. Dermatol. 2020, 45, 345–346. [Google Scholar] [CrossRef]
- Sirufo, M.N.; Catalogna, A.; Raggiunti, M.; De Pietro, F.; Ginaldi, L.; De Martinis, M. Cholinergic Urticaria, an Effective and Safe “Off Label” Use of Dupilumab: A Case Report with Literature Review. Clin. Cosmet. Investig. Dermatol. 2022, 15, 253–260. [Google Scholar] [CrossRef]
- Goodman, B.; Jariwala, S. Dupilumab as a novel therapy to treat adrenergic urticaria. Ann. Allergy Asthma Immunol. 2021, 126, 205–206. [Google Scholar] [CrossRef]
- Yan, S.; Wu, X.; Jiang, J.; Yu, S.; Fang, X.; Yang, H.; Bai, X.; Wang, H.; Luo, X. Dupilumab improves clinical symptoms in children with Netherton syndrome by suppressing Th2-mediated inflammation. Front. Immunol. 2022, 13, 1054422. [Google Scholar] [CrossRef]
- Odorici, G.; Schenetti, C.; Marzola, E.; Monti, A.; Borghi, A.; Corazza, M. Treatment of Netherton syndrome with dupilumab. JDDG J. Dtsch. Dermatol. Ges. 2022, 20, 1636–1640. [Google Scholar] [CrossRef]
- Galdo, G.; Fania, L. A Netherton syndrome case report: Response to dupilumab treatment. Dermatol. Ther. 2022, 35, e15862. [Google Scholar] [CrossRef]
- Ragamin, A.; Nouwen, A.E.; Dalm, V.A.; van Mierlo, M.M.; Lincke, C.R.; Pasmans, S.G. Treatment Experiences with Intravenous Immunoglobulins, Ixekizumab, Dupilumab, and Anakinra in Netherton Syndrome: A Case Series. Dermatology 2022, 239, 72–80. [Google Scholar] [CrossRef]
- Inaba, Y.; Kanazawa, N.; Muraoka, K.; Yariyama, A.; Kawaguchi, A.; Kunimoto, K.; Kaminaka, C.; Yamamoto, Y.; Tsujioka, K.; Yoshida, A.; et al. Dupilumab Improves Pruritus in Netherton Syndrome: A Case Study. Children 2022, 9, 310. [Google Scholar] [CrossRef]
- Wang, J.; Yu, L.; Zhang, S.; Wang, C.; Li, Z.; Li, M.; Zhang, S. Successful treatment of Netherton syndrome with dupilumab: A case report and review of the literature. J. Dermatol. 2022, 49, 165–167. [Google Scholar] [CrossRef]
- Murase, C.; Takeichi, T.; Taki, T.; Yoshikawa, T.; Suzuki, A.; Ogi, T.; Suga, Y.; Akiyama, M. Successful dupilumab treatment for ichthyotic and atopic features of Netherton syndrome. J. Dermatol. Sci. 2021, 102, 126–129. [Google Scholar] [CrossRef]
- Aktas, M.; Salman, A.; Sengun, O.A.; Ozer, E.C.; Tekin, S.H.; Cakici, O.A.; Demir, G.; Ergun, T. Netherton syndrome: Temporary response to dupilumab. Pediatr. Dermatol. 2020, 37, 1210–1211. [Google Scholar] [CrossRef]
- Süßmuth, K.; Traupe, H.; Loser, K.; Ständer, S.; Kessel, C.; Wittkowski, H.; Oji, V. Response to dupilumab in two children with Netherton syndrome: Improvement of pruritus and scaling. J. Eur. Acad. Dermatol. Venereol. 2020, 35, e152–e155. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, T.H.; Karstensen, H.G.; Duno, M.; Lei, U.; Zachariae, C.; Thyssen, J.P. Successful treatment with dupilumab of an adult with Netherton syndrome. Clin. Exp. Dermatol. 2020, 45, 915–917. [Google Scholar] [CrossRef]
- Steuer, A.B.; Cohen, D.E. Treatment of Netherton Syndrome With Dupilumab. JAMA Dermatol. 2020, 156, 350–351. [Google Scholar] [CrossRef]
- Binkhonain, F.K.; Aldokhayel, S.; BinJadeed, H.; Madani, A. Successful Treatment of an Adult with Atopic Dermatitis and Lamellar Ichthyosis Using Dupilumab. Biol. Targets Ther. 2022, 16, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Steinhoff, M.; Al-Marri, F.; Al Chalabi, R.; Gieler, U.; Buddenkotte, J. Recalcitrant erythrodermic ichthyosis with atopic dermatitis successfully treated with Dupilumab in combination with Guselkumab. Ski. Health Dis. 2022, 2, e87. [Google Scholar] [CrossRef] [PubMed]
- Alexis, B.; Nathalie, J.; Audrey, M.-B.; Pol-André, A.; Juliette, M.-H. Peeling Skin Syndrome Type 1: Dupilumab Reduces IgE, But Not Skin Anomalies. J. Clin. Immunol. 2022, 42, 873–875. [Google Scholar] [CrossRef]
- Gruber, R.; Zschocke, A.; Zellner, H.; Schmuth, M. Successful treatment of trichothiodystrophy with dupilumab. Clin. Exp. Dermatol. 2021, 46, 1381–1383. [Google Scholar] [CrossRef]
- Chello, C.; Sernicola, A.; Paolino, G.; Grieco, T. Effects of dupilumab in type 1 neurofibromatosis coexisting with severe atopic dermatitis. An. Bras. Dermatol. 2021, 96, 638–640. [Google Scholar] [CrossRef]
- Tehrany, Y.A.; Marois, L.; Colmant, C.; Marchand, V.; Kokta, V.; Coulombe, J.; Marcoux, D.; Haddad, E.; McCuaig, C. Refractory pruritus responds to dupilumab in a patient with TTC7A mutation. JAAD Case Rep. 2021, 8, 9–12. [Google Scholar] [CrossRef]
- Maher, M.C.; Hall, E.M.; Horii, K.A.; Maher, M.C. Generalized eczematous dermatitis and pruritus responsive to dupilumab in a patient with immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome. Pediatr. Dermatol. 2021, 38, 1370–1371. [Google Scholar] [CrossRef]
- Atwal, S.; Ong, P.Y. Successful use of dupilumab to treat eczema in a child with X-linked agammaglobulinemia. Ann. Allergy Asthma Immunol. 2022, 129, 384–386. [Google Scholar] [CrossRef]
- Gandhi, N.A.; Bennett, B.L.; Graham, N.M.H.; Pirozzi, G.; Stahl, N.; Yancopoulos, G.D. Targeting key proximal drivers of type 2 inflammation in disease. Nat. Rev. Drug Discov. 2016, 15, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Wieser, J.K.; Kuehn, G.J.; Prezzano, J.C.; Cusick, E.H.; Stiegler, J.D.; Scott, G.A.; Liesveld, J.L.; Beck, L.A. Improvement in a patient with hypereosinophilic syndrome after initiation of dupilumab treatment. JAAD Case Rep. 2020, 6, 292–295. [Google Scholar] [CrossRef]
- Chen, M.M.; Roufosse, F.; Wang, S.A.; Verstovsek, S.; Durrani, S.R.; Rothenberg, M.E.; Pongdee, T.; Butterfield, J.; Lax, T.; Wechsler, M.E.; et al. An International, Retrospective Study of Off-Label Biologic Use in the Treatment of Hypereosinophilic Syndromes. J. Allergy Clin. Immunol. Pract. 2022, 10, 1217–1228.e3. [Google Scholar] [CrossRef]
- Du, X.; Chen, Y.; Chang, J.; Sun, X.; Zhang, Y.; Zhang, M.; Maurer, M.; Li, Y.; Zhao, Z.; Tong, X. Dupilumab as a novel steroid-sparing treatment for hypereosinophilic syndrome. JAAD Case Rep. 2022, 29, 106–109. [Google Scholar] [CrossRef]
- Jin, A.; Pousti, B.T.; Savage, K.T.; Mollanazar, N.K.; Lee, J.B.; Hsu, S. Eosinophilic dermatosis of hematologic malignancy responding to dupilumab in a patient with chronic lymphocytic leukemia. JAAD Case Rep. 2019, 5, 815–817. [Google Scholar] [CrossRef]
- Goyal, A.; Lofgreen, S.; Mariash, E.; Bershow, A.; Gaddis, K.J. Targeted inhibition of IL -4/13 with dupilumab is an effective treatment for eosinophilic dermatosis of hematologic malignancy. Dermatol. Ther. 2020, 33, e13725. [Google Scholar] [CrossRef]
- Maglie, R.; Ugolini, F.; De Logu, F.; Simi, S.; Senatore, S.; Montefusco, F.; Nassini, R.; Massi, D.; Antiga, E. Dupilumab for the treatment of recalcitrant eosinophilic dermatosis of haematologic malignancy. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e501–e503. [Google Scholar] [CrossRef] [PubMed]
- Lévy, R.; Béziat, V.; Barbieux, C.; Puel, A.; Bourrat, E.; Casanova, J.-L.; Hovnanian, A. Efficacy of Dupilumab for Controlling Severe Atopic Dermatitis in a Patient with Hyper-IgE Syndrome. J. Clin. Immunol. 2020, 40, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Nihal, A.; Comstock, J.R.; Holland, K.E.; Singh, A.M.; Seroogy, C.M.; Arkin, L.M. Clearance of atypical cutaneous manifestations of hyper-IgE syndrome with dupilumab. Pediatr. Dermatol. 2022, 39, 940–942. [Google Scholar] [CrossRef]
- Matucci-Cerinic, C.; Viglizzo, G.; Pastorino, C.; Corcione, A.; Prigione, I.; Bocca, P.; Bustaffa, M.; Cecconi, M.; Gattorno, M.; Volpi, S. Remission of eczema and recovery of Th1 polarization following treatment with Dupilumab in STAT3 hyper IgE syndrome. Pediatr. Allergy Immunol. 2022, 33, e13770. [Google Scholar] [CrossRef]
- Wang, H.; Yang, T.; Lan, C. Dupilumab treatment of eczema in a child with STAT3 hyper-immunoglobulin E syndrome. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e367–e369. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Darder, I.; De Ves, J.P.; Cortina, M.R.; Martín-Santiago, A. Patient with atopic dermatitis, hyper IgE syndrome and ulcerative colitis, treated successfully with dupilumab during pregnancy. Dermatol. Ther. 2021, 35, e15237. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-W.; Lee, W.-I.; Chung, W.-H. Dupilumab for STAT3-Hyper-IgE Syndrome with Refractory Intestinal Complication. Pediatrics 2021, 148, e2021050351. [Google Scholar] [CrossRef]
- Dixit, C.; Thatayatikom, A.; Pappa, H.; Knutsen, A.P. Treatment of severe atopic dermatitis and eosinophilic esophagitis with dupilumab in a 14-year-old boy with autosomal dominant hyper-IgE syndrome. J. Allergy Clin. Immunol. Pract. 2021, 9, 4167–4169. [Google Scholar] [CrossRef]
- Su, C.-J.; Tseng, H.-C. Treatment efficacy of dupilumab in a hyper-immunoglobulin E syndrome patient with severe atopic dermatitis. JAAD Case Rep. 2021, 11, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Sogkas, G.; Hirsch, S.; Jablonka, A.; Witte, T.; Schmidt, R.E.; Atschekzei, F. Dupilumab to treat severe atopic dermatitis in autosomal dominant hyper-IgE syndrome. Clin. Immunol. 2020, 215, 108452. [Google Scholar] [CrossRef] [PubMed]
- Joshi, T.P.; Anvari, S.; Gupta, M.R.; Davis, C.M.; Hajjar, J. Case Report: Dupilumab Successfully Controls Severe Eczema in a Child with Elevated IgE Levels and Recurrent Skin Infections. Front. Pediatr. 2021, 9, 646997. [Google Scholar] [CrossRef]
- Ollech, A.; Mashiah, J.; Lev, A.; Simon, A.J.; Somech, R.; Adam, E.; Barzilai, A.; Hagin, D.; Greenberger, S. Treatment options for DOCK8 deficiency-related severe dermatitis. J. Dermatol. 2021, 48, 1386–1393. [Google Scholar] [CrossRef]
- Teraki, Y.; Terao, A. Treatment of Kimura Disease with Dupilumab. JAMA Dermatol. 2022, 158, 329–330. [Google Scholar] [CrossRef]
- Huang, H.-Y.; Yang, C.-Y.; Yao, W.-T.; Chen, Y.-F.; Yu, C.-M.; Tung, K.-Y.; Tsai, M.-F. Kimura Disease of the Thigh Treated with Surgical Excision and Dupilumab. Ann. Plast. Surg. 2022, 88, S110–S113. [Google Scholar] [CrossRef] [PubMed]
- Bellinato, F.; Mastrosimini, M.G.; Querzoli, G.; Gisondi, P.; Girolomoni, G. Dupilumab for recalcitrant Kimura disease. Dermatol. Ther. 2022, 35, e15674. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Yu, H.; Jia, M.; Yao, W.; Diao, R.; Li, B.; Wang, Y.; Li, T.; Ge, L.; Wang, H. Successful treatment of dupilumab in Kimura disease independent of IgE: A case report with literature review. Front. Immunol. 2022, 13, 1084879. [Google Scholar] [CrossRef] [PubMed]
- Teraki, Y.; Taguchi, R.; Takamura, S.; Fukuda, T. Use of Dupilumab in the Treatment of Papuloerythroderma of Ofuji. JAMA Dermatol. 2019, 155, 979–980. [Google Scholar] [CrossRef] [PubMed]
- Komatsu-Fujii, T.; Nonoyama, S.; Ogawa, M.; Fukumoto, T.; Tanabe, H. Rapid effects of dupilumab treatment on papuloerythroderma of Ofuji. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e739–e741. [Google Scholar] [CrossRef]
- Mizuno, A.; Habe, K.; Matsushima, Y.; Kondo, M.; Yamanaka, K. A Case of Papuloerythroderma Successfully Treated with Dupilumab. Case Rep. Dermatol. 2022, 14, 117–122. [Google Scholar] [CrossRef]
- Traidl, S.; Angela, Y.; Kapp, A.; Suhling, H.; Schacht, V.; Werfel, T. Dupilumab in eosinophilic cellulitis (Wells’ syndrome)—Case report of a potential new treatment option. JDDG J. Dtsch. Dermatol. Ges. 2021, 19, 1653–1655. [Google Scholar] [CrossRef]
- Kirven, R.M.; Plotner, A.N. Wells syndrome successfully treated with dupilumab. Int. J. Dermatol. 2022, 36349453. [Google Scholar] [CrossRef]
- Gordon, S.C.; Robinson, S.N.; Abudu, M.; Her, M.; Deverapalli, S.; Levin, A.; Schmidt, B.A.R.; Gellis, S.E.; Rosmarin, D. Eosinophilic annular erythema treated with dupilumab. Pediatr. Dermatol. 2018, 35, e255–e256. [Google Scholar] [CrossRef]
- Maione, V.; Caravello, S.; Cozzi, C.; Venturini, M.; Incardona, P.; Frassi, M.; Pinton, P.C. Refractory eosinophilic annular erythema treated successfully with dupilumab. JDDG J. Dtsch. Dermatol. Ges. 2020, 18, 1031–1032. [Google Scholar] [CrossRef]
- Xia, R.; Liu, J.; Su, T.; Xia, J.; Yin, Z. Dupilumab for treatment of eosinophilic fasciitis. Clin. Exp. Dermatol. 2022, 47, 2298–2300. [Google Scholar] [CrossRef]
- Franke, K.; Notaro, E.; Moshiri, A.S.; Ayars, A.; Kalus, A. Use of Dupilumab and Eosinophil Targeted Therapy in Treating Angiolymphoid Hyperplasia with Eosinophilia. JAMA Dermatol. 2022, 158, 960–962. [Google Scholar] [CrossRef]
- Peterson, D.M.; Damsky, W.E.; Vesely, M.D. Treatment of lichen sclerosus and hypertrophic scars with dupilumab. JAAD Case Rep. 2022, 23, 76–78. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.A.; Hsu, S.; Shevchenko, A.; Quartey, A. Dupilumab Failure in Treating Dermatomyositis-Associated Pruritus. Cureus 2022, 14, e28270. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.S.; Lau, S.; Lee, J.K. Dupilumab as a novel steroid-sparing treatment for IgG4-related disease. Ann. Rheum. Dis. 2020, 79, 549–550. [Google Scholar] [CrossRef] [PubMed]
- Diaz, A.; Tan, K.; He, H.; Xu, H.; Cueto, I.; Pavel, A.B.; Krueger, J.G.; Guttman-Yassky, E. Keloid lesions show increased IL -4/ IL -13 signaling and respond to Th2-targeting dupilumab therapy. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e161–e164. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.J.S.; Song, E.J. Dupilumab as an adjuvant treatment for keloid-associated symptoms. JAAD Case Rep. 2021, 13, 73–74. [Google Scholar] [CrossRef]
- Tirgan, M.; Uitto, J. Lack of efficacy of dupilumab in the treatment of keloid disorder. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e120–e122. [Google Scholar] [CrossRef]
- Luk, K.; Fakhoury, J.; Ozog, D. Nonresponse and Progression of Diffuse Keloids to Dupilumab Therapy. J. Drugs Dermatol. 2022, 21, 197–199. [Google Scholar] [CrossRef]
- Smith, M.P.; Ly, K.; Thibodeaux, Q.; Beck, K.; Berger, T.; Khodosh, R.; Liao, W.; Bhutani, T. Dupilumab for the treatment of severe photodermatitis. JAAD Case Rep. 2019, 5, 614–616. [Google Scholar] [CrossRef]
- Patel, N.; Konda, S.; Lim, H.W. Dupilumab for the treatment of chronic actinic dermatitis. Photodermatol. Photoimmunol. Photomed. 2020, 36, 398–400. [Google Scholar] [CrossRef]
- Chen, J.; Li, H.; Zhu, H. Successful Treatment of Chronic Actinic Dermatitis with Dupilumab: A Case Report and Review of the Literature. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1913–1917. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lian, C. Chronic actinic dermatitis in an old adult significantly improved by dupilumab. Photodermatol. Photoimmunol. Photomed. 2022, 38, 176–177. [Google Scholar] [CrossRef] [PubMed]
- McFeely, O.; Doyle, C.; Blasco, M.C.; Beatty, P.; Murphy, L.; O’Mahony, S.; Andrawis, M.; Salim, A. Chronic actinic dermatitis successfully treated with methotrexate and dupilumab. Photodermatol. Photoimmunol. Photomed. 2023, 39, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.; Wu, L.; Lou, H.; Zhong, J.; Qiu, Y.; Da, J.; Shan, J.; Lu, K. Clearance of Chronic Actinic Dermatitis With Dupilumab Therapy in Chinese Patients: A Case Series. Front. Med. 2022, 9, 803692. [Google Scholar] [CrossRef]
- Verma, L.; Pratt, M. A case report of therapeutically challenging chronic actinic dermatitis. SAGE Open Med. Case Rep. 2019, 7, 2050313X19845235. [Google Scholar] [CrossRef]
- Eickstaedt, J.B.; Starke, S.; Krakora, D.; Hinshaw, M.; Arkin, L.M. Clearance of pediatric actinic prurigo with dupilumab. Pediatr. Dermatol. 2020, 37, 1176–1178. [Google Scholar] [CrossRef]
- Larijani, M.; Zarowin, D.; Wohlschlaeger, A.; Perman, M.J.; Treat, J.R. Atopic dermatitis-like graft-versus-host disease treated with dupilumab. Pediatr. Dermatol. 2022, 40, 320–322. [Google Scholar] [CrossRef]
- Zheng, Y.; Zheng, M.; Cai, S. Successful treatment of secukinumab-resistant palmoplantar pustulosis by Dupilumab: A case report. Dermatol. Ther. 2022, 35, e15781. [Google Scholar] [CrossRef]
- Kazemi, S.; Murphrey, M.; Hawkes, J.E. Rapid resolution of widespread cutaneous lichen planus and generalized pruritus in an elderly patient following treatment with dupilumab. JAAD Case Rep. 2022, 30, 108–110. [Google Scholar] [CrossRef]
- Pousti, B. Dupilumab for the Treatment of Lichen Planus. Cutis 2021, 107, E8–E10. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.K.; Shin, J.U.; Kim, D.H.; Lee, H.J. Severe atopic dermatitis and concurrent severe hidradenitis suppurativa successfully treated with dupilumab. Clin. Exp. Dermatol. 2022, 47, 2303–2305. [Google Scholar] [CrossRef] [PubMed]
- Molinelli, E.; Sapigni, C.; Simonetti, O.; Radi, G.; Gambini, D.; Maurizi, A.; Rizzetto, G.; D’Agostino, G.M.; Offidani, A. Successfully and safety use of dupilumab in the management of severe atopic dermatitis and concomitant moderate-to-severe hidradenitis suppurativa. Dermatol. Ther. 2022, 35, e15645. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, A.; Calabrese, G.; Di Brizzi, E.V.; Alfano, R.; Argenziano, G. A case of Atopic dermatitis and Hidradenitis Suppurativa successfully treated with Dupilumab. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e284–e286. [Google Scholar] [CrossRef] [PubMed]
- Song, E.J.; Bezecny, J.; Farrer, S. Recalcitrant generalized granuloma annulare treated successfully with dupilumab. JAAD Case Rep. 2021, 7, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.; Ohyama, M.; Mizukawa, Y. A case of lichen amyloidosis associated with atopic dermatitis successfully treated with dupilumab: A case report and literature review. Dermatol. Ther. 2021, 34, e15005. [Google Scholar] [CrossRef] [PubMed]
- Zahid, S.; Saussine, A.; Calugareanu, A.; Jachiet, M.; Vignon-Pennamen, M.; Rybojad, M.; Bagot, M.; Bouaziz, J.; Mahévas, T. Dramatic response to dupilumab in papular amyloidosis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e1071–e1072. [Google Scholar] [CrossRef]
- Humeda, Y.; Beasley, J.; Calder, K. Clinical resolution of generalized lichen amyloidosis with dupilumab: A new alternative therapy. Dermatol. Online J. 2020, 26, 0513030. [Google Scholar] [CrossRef]
- Rial, M.J.; Barroso, B.; Sastre, J. Dupilumab for treatment of food allergy. J. Allergy Clin. Immunol. Pract. 2019, 7, 673–674. [Google Scholar] [CrossRef]
- Mollanazar, N.K.; Savage, K.T.; Pousti, B.T.; Jariwala, N.; Del Guzzo, C.; Haun, P.; Vittorio, C.C.; Rook, A.H.; Kim, E.J. Cutaneous T-cell Lymphoma and Concomitant Atopic Dermatitis Responding to Dupilumab. Cutis 2020, 106, 131–132. [Google Scholar] [CrossRef]
- Steck, O.; Bertschi, N.L.; Luther, F.; Berg, J.V.D.; Winkel, D.J.; Holbro, A.; Schlapbach, C. Rapid and sustained control of itch and reduction in Th2 bias by dupilumab in a patient with Sézary syndrome. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Lazaridou, I.; Ram-Wolff, C.; Bouaziz, J.; Bégon, E.; Battistella, M.; Rivet, J.; Jachiet, M.; Bagot, M.; Masson, A. Dupilumab Treatment in Two Patients with Cutaneous T-cell Lymphomas. Acta Derm. Venereol. 2020, 100, adv00271. [Google Scholar] [CrossRef] [PubMed]
- Miyashiro, D.; Vivarelli, A.G.; Gonçalves, F.; Cury-Martins, J.; Sanches, J.A. Progression of mycosis fungoides after treatment with dupilumab: A case report. Dermatol. Ther. 2020, 33, e13880. [Google Scholar] [CrossRef]
- Espinosa, M.L.; Nguyen, M.T.; Aguirre, A.S.; Martinez-Escala, M.E.; Kim, J.; Walker, C.J.; Pontes, D.S.; Silverberg, J.I.; Choi, J.; Pro, B.; et al. Progression of cutaneous T-cell lymphoma after dupilumab: Case review of 7 patients. J. Am. Acad. Dermatol. 2020, 83, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Umemoto, N.; Demitsu, T.; Otaki, K.; Matsumoto, T.; Takazawa, M.; Yamada, A.; Kimura, S.; Kakurai, M. Dupilumab therapy in Sézary syndrome misdiagnosed as atopic dermatitis: A case report. J. Dermatol. 2020, 47, e356–e357. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, M.; Miyagaki, T.; Komaki, R.; Takeuchi, S.; Kadono, T. Development of Nodular Lesions after Dupilumab Therapy in Erythrodermic Mycosis Fungoides with Interleukin-13 Receptor alpha2 Expression. Acta Derm. Venereol. 2022, 102, adv00766. [Google Scholar] [CrossRef] [PubMed]
- Chiba, T.; Nagai, T.; Osada, S.; Manabe, M. Diagnosis of Mycosis Fungoides Following Administration of Dupilumab for Misdiagnosed Atopic Dermatitis. Acta Derm.-Venereol. 2019, 99, 818–819. [Google Scholar] [CrossRef]
- Park, A.; Wong, L.; Lang, A.; Kraus, C.; Anderson, N.; Elsensohn, A. Dupilumab-Associated Mycosis Fungoides with a CD8+ Immunophenotype. Dermatopathology 2022, 9, 385–391. [Google Scholar] [CrossRef]
- Newsom, M.; Hrin, M.L.; Hamid, R.N.; Strowd, L.C.; Ahn, C.; Jorizzo, J.L.; Feldman, S.R. Two cases of mycosis fungoides diagnosed after treatment non-response to dupilumab. Dermatol. Online J. 2021, 27. [Google Scholar] [CrossRef]
- Tran, J.; Morris, L.; Vu, A.; Duvic, M. Development of Sézary syndrome following the administration of dupilumab. Dermatol. Online J. 2020, 26. [Google Scholar] [CrossRef]
- Joshi, T.P.; Duvicy, M.; Torres-Cabala, C.A.; Tschen, J. Treatment with Dupilumab for Refractory Cutaneous B-Cell Pseudolymphoma. JAMA Dermatol. 2022, 158, 697–699. [Google Scholar] [CrossRef] [PubMed]
- Trum, N.A.; Zain, J.; Abad, C.; Rosen, S.T.; Querfeld, C. Dupilumab as a therapy option for treatment refractory mogamulizumab-associated rash. JAAD Case Rep. 2021, 14, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Patruno, C.; Potestio, L.; Scalvenzi, M.; Battista, T.; Raia, F.; Picone, V.; Fabbrocini, G.; Napolitano, M. Dupilumab for the treatment of adult atopic dermatitis in special populations. J. Dermatol. Treat. 2022, 33, 3028–3033. [Google Scholar] [CrossRef] [PubMed]


| Disease | Study Type | n | Sex/Age | Medical History | Prior Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|
| PN | case report (5) | 1 | F/9 | no AD, normal IgE | topical steroids, antihistamines, phototherapy, ciclosporin (4 mg/kg/d), MTX (7.5–10 mg/wk), psychiatric interventions | Dupilumab 200 mg s.c., then 100 mg q2w | Decreased pruritus at 4 wk, resolution of skin lesions at 3 mo | [86] | |
| PN | case report (5) | 1 | M/16 | no AD, no family history of atopy | antihistamines, topical steroids, ciclosporin (5 mg/kg/d) | ciclosporin, tapered | Dupilumab 600 mg s.c., then 300 mg q2w | Resolution of skin lesions at 3 mo, reduction of itch NRS, improved quality of life (by DLQI) | [87] |
| CPUO | case series (4) | 6 | 60.5 (median, 43–78 range), female: 2/6 | asthma (1/6), hypereosinophilia (2/6), type-IV sensitivity (3/6), cardiovascular disease (4/6), nephrotic syndrome (1/6), tumor (1/6), depression (1/6), diabetes mellitus (1/6), sarcoidosis (1/6) | antihistamines (5/6), topical (6/6) and systemic (6/6) steroids, MMF (4/6), topical calcineurin inhibitor (3/6), phototherapy (1/6), mirtazapine (1/6), gabapentin (1/6), aprepitant (1/6), azathioprin (1/6) | Dupilumab 600 mg s.c., then 300 mg q2w (5/6) or q4w (1/6) | Improvement in pruritus and skin lesions (6/6) | [88] | |
| CPUO | case series (4) | 15 | 68.7 (mean, SD 12.6), female: 67% | Exclusion of patients with AD or atopy, other primary dermatologic disorder or systemic disease-causing itch | topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of itch NRS mean -7.0 (SD 1.9) at various follow-up intervals (mean 19 mo, interquartile range 10–26) | [89] | |
| CPUO | case series (4) | 2 | F/68, M/86 | no AD or atopy (2/2), hypereosinophilia (1/2), cardiovascular disease (1/2) | topical steroids (2/2), antihistamines (2/2), phototherapy (1/2), MMF (1/2), gabapentin (1/2), pregabalin (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Resolution of pruritus at 4 or 5 mo (2/2) measured by worst itch-NRS | [90] | |
| CPUO | case series (4) | 4 | 65 (median, 56–66 range), female: 3/4 | AD (1/4) | topical steroids, topical calcineurin inhibitors | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of itch NRS -8.75 (mean, SD 1.26) at wk 12; withdrawal of dupilumab at 4 wk with sustained response at wk 20 (2/4) | [8] | |
| Uremic pruritus | case series (4) | 5 | 64 (median, 57–78 range), female: 2/5 | no AD or atopy (5/5) | topical steroids, topical calcineurin inhibitors | hemodialysis (1/5) | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of itch NRS -6.4 (mean, SD 3.51) at 12 wk | [8] |
| Uremic pruritus | case report (5) | 1 | F/61 | Allergic rhinitis, hypertension, polycystic kidney disease, renal transplant (aged 53) | phototherapy, doxepin, aprepitant, pregabalin, naltrexone, mirtazapin, topical steroid, topical anesthetic | phototherapy, gabapentin (tapered) | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of itch NRS to 0 at 6 mo, improvement in quality of life (DLQI 1 at 6 mo) | [91] |
| Cholestatic pruritus | case report (5) | 1 | M/44 | Primary sclerosing cholangitis and autoimmune hepatitis | topical steroids, topical retinoids, bile acid sequestrants, anticonvulsants, antihistamines, doxepin, phototherapy | phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in pruritus (-8 NRS), resolution of skin lesions, improvement in quality of life (DLQI) | [92] |
| Brachioradial pruritus | case report (5) | 1 | F/53 | fibromyalgia, cervical disc protrusion, scoliosis | topical steroid, topical doxepin, antihistamines, gabapentin, pregabalin | topical steroid, topical anesthetic, amitriptyline (discontinued after 4 wk) | Dupilumab 600 mg s.c., then 300 mg q2w | 95% improvement of pruritus at 12 wk, sustained response for 8 mo | [93] |
| Anal and genital pruritus | case report (5) | 1 | M/62 | ADHD, depression, asthma, lumbal spine degeneration, multiple food allergies and type-IV sensitivity | topical antiinfectives, topical and systemic steroids, topical calcineurin inhibitors, topical doxepin, topical capsaicin, antihistamines, gabapentin, MMF (3 g/d) | Dupilumab 600 mg s.c., then 300 mg q2w | 95% resolution of itch and resolution of skin lesions at 4 wk, sustained response at 12 mo | [94] | |
| RPC | case report (5) | 1 | M/66 | no AD or atopy; chronic kidney disease, hypertension, diabetes mellitus | phototherapy, nalfurafine | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of itch NRS from 10 to 2 at 4 wk, resolution of skin lesions | [95] | |
| RPC | case report (5) | 1 | M/59 | diabetes mellitus, pulmonary tuberculosis | systemic steroids, hydroxychloroquine | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of itch and skin lesions after 2 wk | [96] | |
| RPC | case report (5) | 1 | F/20 | Wilson’s disease, liver transplant (aged 15) | systemic steroids (20 mg/d), systemic tacrolimus (5 mg/d) due to transplant | Immune-suppressive therapy after transplant was continued | Dupilumab 600 mg s.c., then 300 mg q2w | Clearance of pruritus within 2 wk, clearance of active skin lesions at 10 wk | [97] |
| RPC | case report (5) | 1 | F/40s | AD | topical and systemic steroids, phototherapy, antihistamines, ciclosporin | phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in pruritus after 2 mo, resolution of skin lesions afer 12 mo | [98] |
| RPC | case series (4) | 2 | M/71, M/70 | AD (2/2), cardiovascular disease (2/2), diabetes mellitus (2/2) | antihistamines (2/2), topical steroids (2/2), phototherapy (1/2) | none (2/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Partial reduction of pruritus and reduction of skin lesions at 6 or 12 wk | [99] |
| Disease | Study Type | n | Sex/Age | Medical History | Prior Systemic Therapies | Prior Topical Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| AU | case report (5) | 1 | F/21 | AD | UVB phototherapy, tofacitinib | Dupilumab 300 mg q2w | Regrowth of hair on scalp, eyebrowes and eyelashes at 2 mo. Only one alopecic patch left at 4 mo | [152] | ||
| AU | case report (5) | 1 | F/49 | AD, allergic rhinitis, asthma, polysensitization | betamethasone (0.5 mg/d), ciclosporin | Dupilumab 600 mg s.c., then 300 mg q2w | Partial regrowth of terminal hairs and body hairs, regrowth of eyebrows, sustained for 1, 5 years | [153] | ||
| AA (AU) | case report (5) | 1 | F/34 | AD, asthma | steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth within 10 mo | [154] | ||
| AA (AT) | case report (5) | 1 | M/30 | AD | steroids, MTX, ciclosporine | steroids, phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth within 3 mo | [155] | |
| AA (AT) | case report (5) | 1 | F/68 | no AD, no family history of AD | steroids, ciclosporine | photodynamic therapy, steroids, squaric acid | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement in SALT at wk 2 (-92), complete regrowth within 3 mo | [156] | |
| AA | case report (5) | 1 | F/33 | AD, trichotillomania | Dupilumab 600 mg s.c., then 300 mg q2w | Partial regrowth within 3 wk, complete regrowth within 19 wk | [157] | |||
| AA (AT 3/7, AU 1/7) | case series (4) | 7 | 40.0 (mean, 33–52 range), females: 2/7 | AD | steroids (5/7) | steroids (5/7), diphenylcyclopropenon (4/7), squaric acid (1/7), phototherapy (2/7) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth (SALT < 10, 2/7), partial response (4/7), no response (1/7) | [158] | |
| AA | case series (4) | 2 | M/38, M/32 | AD (2/2), allergic rhinoconjuncitivis (2/2), asthma (2/2) | ciclosporine (2/2), azathioprine (1/2) | phototherapy (2/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth at wk 21 or 22 (2/2) | [159] | |
| AA | case report (5) | 1 | M/49 | AD | steroids, azathioprine, ciclosporine, MTX | phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth at 3 mo | [160] | |
| AA | case report (5) | 1 | M/44 | AD | steroids | steroids | steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth at 3 mo (SALT -53) | [161] |
| AA (AU) | case report (5) | 1 | F/35 | AD, chronic urticaria | steroids, omalizumab, ciclosporin | steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth at 12 mo | [162] | |
| AA (AU) | case report (5) | 1 | M/28 | AD, asthma | ciclosporin (5 mg/kg/d), MTX (20 mg/wk) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth (SALT -80.4) | [163] | ||
| AA | case report (5) | 1 | M/21 | AD | ciclosporin (5 mg/kg/d) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth (SALT 8.2) at 16 wk. Report also includes another case of AA developed as an adverse effect of dupilumab | [164] | ||
| AA (AU) | case report (5) | 1 | F/49 | AD | pulsed prednisone, MTX (20 mg/wk) | steroids, calcineurin inhibitors, phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth at 8 mo | [165] | |
| AA (AT) | case report (5) | 1 | F/28 | AD | steroids, phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Nearly complete regrowth at 2–3 mo | [166] | ||
| AA (AU) | case report (5) | 1 | F/44 | AD | pulsed methylprednisolone (500 mg/d max.) | steroids, phototherapy | topical steroid | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth at 10 m. Patient developed psoriasis as uncommon adverse effect of dupilumab. | [167] |
| AA (AT) | case report (5) | 1 | M/47 | AD | ciclosporin, MTX | Dupilumab 600 mg s.c., then 300 mg q2w | partial regrowth at 8 wk | [168] | ||
| AA (AU) | case report (5) | 1 | M/65 | AD | steroids and calcineurin inhibitors | Dupilumab 600 mg s.c., then 300 mg q2w | partial regrowth at 10 mo | [169] | ||
| AA (3/4) | case series (4) | 4 | F/40, F/51, F/54, F/42 | AD (4/4), asthma (2/4), allergic rhinitis (1/4), Basedow’s disease (1/4) | steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth within 4 mo (3/4), novel development of AA (1/4) after 8 mo | [170] | ||
| AA | case report (5) | 1 | F/33 | no AD | steroids | steroids, calcineurin inhibitors, minoxidil, squaric acid, calcipotriene, platelet-rich plasma, tofacitinib cream | Dupilumab 600 mg s.c., then 300 mg q2w | Near complete regrowth of hairs within 6 mo, SALT reduction (81.3 to 2.4). Relapse at 6 mo after discontinuation of dupilumab | [171] | |
| Inconti-nentia pigmenti with curvi-linear scalp alopecia | case report (5) | 1 | F/6 | Incontinentia pigmenti, AD | antihistamines | Dupilumab | Regrowth of terminal hairs at 10 wk | [172] | ||
| AT | case report (5) | 1 | M/16 | AD, asthma, Type-I allergy to eggs | montelukast | Dupilumab 600 mg s.c., then 300 mg q2w | Complete regrowth of hairs within 8 mo, sustained for 3 years | [173] | ||
| AA | case series (4) | 6 | M/12, M/7, F/7, F/8, F/7, F/12 | AD (6/6), asthma (2/6), food allergies (3/6) | steroids (2/6), minoxidil (1/6) | steroids (6/6), minoxidil (2/6), anthralin (1/6), tofacitinib (1/6) | none (2/6), topical (1/6) or systemic (3/6) minoxidil, topical tofacitinib (2/6), topical (1/6) or systemic (1/6) steroids | Dupilumab | Complete regrowth (4/6) with reduction of SALT to 0, partial regrowth (1/6) with 73% SALT reduction after 2 years, no response (1/6) | [174] |
| AA (7/14 AU) | case series (4) | 16 | 13.5 (median, 8–19 range) | AD (14/14), | steroids (12/14), MTX (9/14), tofacitinib (3/14) | steroids (14/14), anthralin (5/14), retinoid (7/14), tofacitinib (4/14), squaric acid (2/14), minoxidil (3/14) | none (8/14), topical (2/14) or systemic (2/14) tofacitinib, oral MTX (1/14), topical steroids (3/14), topical minoxidil (2/14), spironolactone (1/14) | Dupilumab 300 mg s.c. q2w | Initial worsening (4/14, SALT average worsening of 11.3), complete regrowth (3/14), partial response (1/4; SALT average reduction of 33.3 after 12 mo), no response (2/14), 8/14 had no active disease at baseline | [175] |
| AA (AT) | case report (5) | 1 | F/4 | AD | antihistamines | steroids, calcineurin inhibitors | Dupilumab 200 mg s.c. q2w | Complete regrowth within 4 mo | [176] | |
| AA (AT) | case report (5) | 1 | F/13 | AD | pulsed prednisone (50 mg/d max.), MTX (15 mg/wk max.) | squaric acid, anthralin | Dupilumab 600 mg s.c., then 300 mg q2w | Partial regrowth at 11 mo | [177] | |
| AA (AT 5/10, AU 3/10) | case series (4) | 10 | 43.71 (mean, SD 8.22), females: 4/10 | AD (10/10) | ciclosporin (7/10) | steroids (10/10), diphenylcyclo-propenone or squaric acid (7/10), | Dupilumab 600 mg s.c., then 300 mg q2w | Non-significant improvement of SALT (SALT30 32.5%, with elevated IgE 53.8%) at wk 48, no complete responses | [178] | |
| AA (AT/AU in 32.5%) | RCT (2) | 40 vs. 20 | 41.6 (mean, SD 13.8), females: 75% | AD (42.5%, active AD 12.5%), family history of atopy (45%). Other severe, progressive or uncontrolled disease was excluded | none; use of systemic immunosuppression, topical steroids or topical calcineurin inhibitors was excluded | Dupilumab 300 mg qw vs. Placebo | Improvement in SALT at wk 24 (p = 0.049) and wk 48 (p < 0.0001), 30%-improvement in SALT at wk 48 in 32.5% vs. 20% (p = 0.067), 50%-improvement in SALT at wk 48 in 22.5% vs. 15% (p = 0.02), high IgE levels (>200 U/mL) or AD/family history of atopy predicted better outcome | [179] |
| Disease | Study Type | n | Sex/Age | Presentation | Medical History | Prior Therapies | Concomitant Medication | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| Adrenergic urticaria | case report (5) | 1 | M/18 | Papules surrounded by vasoconstricted halos, triggered by heat, stress and exercise | POTS | antihistamines, montelukast, dapsone, omalizumab | propranolol (120 mg/d) | Dupilumab q4w | Complete resolution | [169] |
| CSU | case report (5) | 1 | F/68 | recurrent wheals and episodes of facial angioedema, onset 6 mo prior | chronic renal insufficiency | antihistamines, omalizumab, systemic steroids | systemic steroids (discontinued), antihistamines (tapered), omalizumab (450 mg q4w, later reduced to 300 mg q4w) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete disease control after 6 wk (no new wheals or angioedema, UCT 16) | [182] |
| CSU | case report (5) | 1 | M/44 | pruritic wheals and papules, angioedema | antihistamines, ciclosporin, phototherapy, systemic steroids, omalizumab | Dupilumab 600 mg s.c., then 300 mg q2w | Complete disease control after first application (UAS7 0, no more pruritus, wheals or angioedema), stable for 2 years | [183] | ||
| CSU | case report (5) | 1 | F/47 | 4-month history of hives | AD, multiple type-I allergies | antihistamines, topical and systemic steroid, omalizumab (450 mg q4w) | omalizumab 450 mg q4w, fexofenadine 720 mg/d, prednisolone 12.5 mg/d (tapered) | Dupilumab 600 mg s.c., then 300 mg q2w | Partial control of CSU with UAS7 21 improved to 7, remission of AD with EASI 2.6, improved quality of life (DLQI 3) at 12 mo | [184] |
| CSU | case series (4) | 2 | F/63, F/52 | wheals and lip angioedema for 3 (1/2) and 11 (1/2) years | AD (1/2) | antihistamines (2/2), omalizumab (2/2), ciclosporin (2/2), montelukast (1/2), MTX (1/2) | none (1/2), antihistamines (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete remission (2/2) after 8 wk, sustained at latest follow-up (5 or 23 mo) | [185] |
| CSU | case series (4) | 6 | 35.5 (median, 18–50 range), females: 3/6 | AD (6/6), asthma (2/6), autoimmune thyroiditis (1/6), | antihistamines, omalizumab | antihistamines (6/6), topical steroid or calcineurin inhibitor (5/6), montelukast (1/6), gabapentin (1/6), dapsone (1/6) | Dupilumab 600 mg s.c., then 300 mg q2w | Follow-up for to 34 mo. Complete remission with UAS7 = 0 (4/6). Uncontrolled disease under dupilumab, omalizumab added (1/6), dupilumab discontinued for financial reasons and relapse (1/6) | [186,187] | |
| Cold urticaria | case report (5) | 1 | M/28 | cold urticaria since childhood (positive ice-cube skin test) | severe AD, multiple type-I sensitizations, type-IV sensitization to nickel | antihistamines, systemic steroid, omalizumab, ciclosporin | Dupilumab 600 mg s.c., then 300 mg q2w | 85% reduction of EASI, 86% reduction of itch NRS, DLQI 0, ice-cube test negative, no wheals after cold-water exposure | [192] | |
| Cholinergic urticaria | case report (5) | 1 | M/26 | pruritic wheals after physical exercise | no atopy | antihistamines, systemic steroid, montelukast, omalizumab q4w | antihistamines, discontinued after 8 wk | Dupilumab 600 mg s.c., then 300 mg q2w | Complete remission after 8 wk | [193] |
| CSU | case series (4) | 2 | 6–17 years | atopy (1/2) | antihistamines, omalizumab, ciclosporin | Dupilumab 300 mg s.c. q2w | UAS7 = 0 after 4 wk (1/2), significant improvement of symptoms after 12 wk (1/2) | [188] | ||
| CSU | case report | 1 | M/31 | 3-year history of recurrent itchy wheals | antihistamines, omalizumab | Dupilumab 600 mg s.c., then 300 mg q2w | UAS7 = 0 at wk 16, sustained for 42 wk follow-up | [189] |
| Disease | Study Type | n | Sex/Age | Medical History | Prior Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Lamellar ichthyosis | case report (5) | 1 | M/22 | AD, asthma, Stargardt’s syndrome | Acitretin (10 mg/d), MTX (10 mg/wk) | Dupilumab 300 mg s.c. q2w | Clinical improvement of ichthyosis and AD after 3 mo | [188] | |
| Netherton syndrome | case series (4) | 4 | 3.25 (median, 2–4.5 range), females: 2/4 | ichthyosis linearis circumflexa (4/4), trichorrhexis invaginata (4/4) growth delay (4/4), food allergies (1/4) | topical steroid or topical caldineurin inhibitor | Dupilumab 400 mg s.c., then 200 mg q2w | Temporary response with improvement in pruritus and skin lesions at 6 wk. Deterioration after 8 wk, itch and skin findings worse than at baseline by wk 10. | [195] | |
| Netherton syndrome | case report (5) | 1 | F/29 | asthma, ichthyosis, hair abnormalities, polycystic ovary syndrome | topical and systemic steroids, antihistamines, phototherapy, antibiotics | none | Dupilumab 300 mg s.c. q2w | Reduced itch (NRS -8), resolution of skin lesions (EASI –16), higher quality of life (DLQI –15) in 12 wk. Hair anomalities remained. | [196] |
| Netherton syndrome | case report (5) | 1 | F/42 | Ichthyosis linearis circumflexa, trichorrhexis invaginata | topical steroids, antihistamines | Dupilumab 600 mg s.c., then 300 mg q2w | Reduced itch (NRS -10), resolution of skin lesions (EASI –21), higher quality of life (DLQI –24) in 8 wk. Improvement of ichthyosis. Hair regrowth. | [197] | |
| Netherton syndrome | case report (5) | 1 | F/41 | Ichthyosis linearis circumflexa with erythroderma | topical and systemic steroids, antibiotics, ciclosporin | topical steroid | Dupilumab 600 mg s.c., then 300 mg q2w, later qw | Reduced erythema and scaling, relapse after 5 mo and insufficient control at dose-increase to 300 mg qw, withdrawn after 6 mo | [198] |
| Netherton syndrome | case report (5) | 1 | M/26 | ichthyosis and erythroderma, sleeping disorder | antihistamines | Dupilumab 600 mg s.c., then 300 mg q2w | Cessation of itch (NRS 0), partial resolution of skin lesions (EASI 20) at 12 wk, sustained for 12 mo follow-up | [199] | |
| Netherton syndrome | case report (5) | 1 | F/20 | Ichthyosis linearis circumflexa, trichorrhexis invaginata | topical steroids, antihistamines, acitretin, antibiotics | Dupilumab 600 mg s.c., then 300 mg q2w | Control of itch after 2 days, complete resolution of skin lesions (EASI 2.7) in 4 wk, improved quality of life (DLQI –20 in 6 wk). Hair regrowth after 3 mo. | [200] | |
| Netherton syndrome | case series (4) | 2 | F/32, F/17 | Ichthyosis linearis circumflexa (2/2), trichorrhexis invaginata (2/2), food allergies (2/2), optic nerve inflammation (1/2) | topical and systemic steroids (2/2), omalizumab (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of itch within one day (2/2), itch NRS –4 (1/2) or –2 (1/2) sustained for 6 mo. Partial resolution of skin lesions (EASI 12–13 at 6 mo, 2/2). Hair regrowth (1/2). | [201] | |
| Netherton syndrome | case report (5) | 1 | F/40 | Ichthyosis linearis circumflexa, trichorrhexis invaginata, AD, asthma | topical steroids, topical retinoid, topical tacrolimus, acitretin, azathioprin, ciclosporin, IVIg | Dupilumab 600 mg s.c., then 300 mg q2w | Temporary response with improvement in pruritus and skin lesions at 6 wk. Deterioration after 8 wk, itch and skin findings worse than at baseline by wk 10. | [202] | |
| Netherton syndrome | case series (4) | 2 | F/12, M/8 | IVIG (1/2) | IVIG (1/2), dose reduction | Dupilumab 600 mg s.c., then 300 mg q4w and later 200 mg q2w (1/2). Dupilumab 300 mg q4w (1/2) | Reduction of itch (NRS –5 or –4 in 4 wk), sustained for 10 wk follow up. Sustained improvement of skin lesions. | [203] | |
| Netherton syndrome | case report (5) | 1 | M/43 | asthma, adrenal insufficiency, squamous cell carcinoma | topical and systemic steroids, MTX, MMF, azathioprin, phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Resolution of skin manifestations (EASI –76% of baseline at wk 4), improved quality of life (DLQI 2 at wk 4) | [204] | |
| Netherton syndrome | case report (5) | 1 | F/32 | Ichthyosis linearis circumflexa, trichorrhexis invaginata | topical steroids, topical retinoid, topical tacrolimus, ciclosporin | Dupilumab 600 mg s.c., then 300 mg q2w | Resolution of itch (NRS –7 in 4 wk), improvement of skin lesions (BSA –50% in 4 wk) | [205] | |
| Erythrodermic ichthyosis | case report (5) | 1 | M/38 | AD, frequent bacterial and fungal skin infections | topical steroids, ciclosporin, MTX, acitretin | Guselkumab | Dupilumab 300 mg s.c. q2w | Improvement of ichthyosis and AD after 10 wk | [207] |
| Peeling skin syndrome Type 1 | case report (5) | 1 | F/17 | growth delay | Dupilumab 400 mg s.c., then 200 mg q2w | Mild reduction of erythroderma; pruritus and quality of life not affected. Reduced serum IgE | [208] | ||
| Trichothio-dystrophy (ERCC2-mutation) | case report (5) | 1 | M/8 | ichthyosiform erythroderma, nail dystrophy, allergic rhinoconjuncitivitis, asthma, trichorrhexis nodosa | topical steroids and calcineurin inhibitors, antihistamines | Dupilumab 200 mg s.c. q2w | Complete remission of skin lesions, less pruritus, remission of asthma afer 12 mo | [209] | |
| Neurofibromatosis type 1 | case report (5) | 1 | F/30 | AD | systemic steroids, ciclosporin | Dupilumab 600 mg s.c., then 300 mg q2w | Size reduction of neurofibromas at 4 wk, number and size of neurofibromas stable for 1.5 years. Remission of AD. | [210] | |
| TTC7A-deficiency | case report (5) | 1 | F/5 | multiple intestinal atresia, combined immunodeficiency, linear IgA-dermatosis elevated IgE and hypereosinophilia | topical and systemic steroids, antihistamines, gabapentin, clonidine, mirtazapine, amitriptyline, mepolizumab (50 mg q4w) | methylprednisolone (1 mg/kg/d max.), tapered | Dupilumab 100 mg s.c. q2w | Improvement of itch within few days, complete resolution of pruritus and skin lesions at 6 mo, sustained after withdrawal of steroid | [211] |
| IPEX syndrome | case report (5) | 1 | M/2 | Vitiligo, milk protein allergy, neurofibromatosis, growth delay | bone marrow transplant, systemic steroids, sirolimus, ciclosporin, rituximab, abatacept | Dupilumab 200 mg s.c. q4w | Complete remission of skin findings at 12 wk, improved pruritus | [212] | |
| X-linked agamma-globulinemia with AD-like eczema | case report | 1 | M/11 | multiple episodes of skin infections | topical steroids, intravenous antibiotics, intravenous immunoglobulins | Dupilumab 300 mg s.c. q2w | Complete resolution of skin findings and pruritus, no subsequent skin infections after 3 mo | [213] |
| Disease | Study Type | n | Sex/Age | Presentation | Medical History | Eosinophilia? | Prior Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|
| HES | case report (5) | 1 | M/57 | pruritic hyperpigmentated papules on head and neck. Pulmonary opacities | obesity, diabetes mellitus | Yes (1900/µL) | topical and systemic steroids, phototherapy, pegylated interferon a-2a (180 µg/wk s.c.), mepolizumab, hydroxyurea, gabapentin, antihistamines | Hydroxyurea, gabapentin, hydroxycine (doses reduced) | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of pruritus (NRS 10 to 3) and resolution of skin lesions at wk 4, improvement of pulmonary findings at 23 wk | [215] |
| HES | retrospective study (4) | 9 | 42 (median, 11–85 range), females: 67% | 5/9 with skin findings | AD (1/9) | Yes (>1500/µL) | Systemic steroids; Benralizumab (1/6), Omalizumab (2/9), Mepolizumab (2/9); Dupilumab was first-line biological in 4/9 | Systemic steroid (5/9), tapered | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of skin lesions (3/5), no hematologic remissions (normal eosinophil count, 0/9) | [216] |
| HES | case report (5) | 1 | F/51 | Generalized eczema on trunk and extremities, urticaria-like rashes, severe pruritus. Abdominal cramping pain, uncontrolled asthma. | Allergic asthma, chronic sinusitis, allergic rhinitis. | Yes (2100/µL) | Topical and systemic steroids | Systemic steroid, tapered | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of pruritus (NRS 8 to 4), increased quality of life (DLQI 25 to 9), increased FEV1 | [217] |
| EDHM | case report (5) | 1 | M/82 | CLL (chemotherapy) | systemic steroids | Improvement of itch (NRS 6 to 0 in 4 wk) | [8] | ||||
| EDHM | case report (5) | 1 | M/81 | erosions and pink dermal nodules on chest and face | CLL with leukemia cutis (treated with rituximab and chlorambucil) | topical and systemic steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution of skin lesions after 4 wk | [218] | ||
| EDHM | case report (5) | 1 | M/59 | prurituc urticarial targetoid plaques on trunk and extremities with erosion and impetiginization | CLL (treated with ibrutinib) | No | topical and systemic steroid, antibiotic | Dupilumab 600 mg s.c., then 300 mg q2w | Complete clearance after 6 wk, sustained for 6 mo follow-up | [219] | |
| EDHM | case report (5) | 1 | F/50s | pruritic rash on extremities with indurated papules and blisters | small lymphocytic lymphoma (treated with rituximab + bendamustine) | No | topical and systemic steroid | none | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of pruritus and complete clearance of skin lesions at wk 6 | [220] |
| Hyper-IgE syndrome (ZNF341 deficiency) | case report (5) | 1 | F/48 | severe pruritus, disseminated excoriated papules and scars | topical steroids | topical steroids, discontinued | Dupilumab 600 mg s.c., then 300 mg q2w | Complete remission of skin findings (SCORAD < 10) at wk 4, improved quality of life (DLQI < 5 at wk 6) | [221] | ||
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | F/2 | pruritic disseminated papules and pustules | recurrent pulmonary and skin infections | Yes (1700/µL) | topical and systemic steroids, topical tacrolimus, antibiotics, antihistamines | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution of itch and skin lesions, sustained at 6 mo follow-up | [222] | |
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | M/17 | generalized AD-like eczema | recurrent skin and respiratory tract infections, multiple type-I allergies | Yes (>20% of leukocytes) | topical and systemic steroids, antihistamines, ciclosporin (5 mg/kg/d) | topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Partial remission of skin findings and better quality of life (DLQI 2) after 12 mo | [223] |
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | M/9 | generalized eczema with papules and xerosis | recurrent pneumonia, skin infections, liver abscess | topical steroids, antibiotics, antihistamines | Dupilumab 200 mg s.c., then 100 mg q2w, later q3–4w | Complete remission at wk 20 (SCORAD and EASI 0) | [224] | ||
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | F/28 | Recurrent flares of eczema with severe pruritus | recurrent skin infections and pneumonia, asthma, allergic rhinoconjuncititis, multiple type-I allergies, depression, ulcerative colitis (total colectomy 4 years prior) | Yes (1910/µL) | topical and systemic steroids, topical calcineurin inhibitors, antihistamines, IVIg, ciclosporin, infliximab | IVIG | Dupilumab | Complete clearance of skin lesions | [225] |
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | M/21 | generalized eczema | refractory diarrhea, perforated colon | Yes (6000/µL) | IVIg, systemic steroid | IVIG | Dupilumab 300 mg s.c. q3w | Complete remission of skin findings (EASI 0), cessation of diarrhea after 6 mo | [226] |
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | M/14 | AD-like eczema | recurrent skin infections, pneumonia; eosinophilic esophagitis | Yes (800/µL) | topical steroids and calcineurin inhibitors | Dupilumab 600 mg s.c., then 300 mg q2w | Remission of skin findings (SCORAD 10) after 4 wk | [227] | |
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | M/18 | generalized eczema with lichenification | recurrent skin and respiratory tract infections | topical steroids, topical tacrolimus | Dupilumab 600 mg s.c., then 300 mg q2w, later q4w | Resolution of skin findings (EASI 60 to 9.3) and itch (NRS 9 to 2) | [228] | ||
| Hyper-IgE syndrome (STAT3-mutation) | case report (5) | 1 | F/33 | generalized pruritic eczema | recurrent infections | topical steroids, topical pimecrolimus, phototherapy | Dupilumab 600 mg s.c., then 300 mg q2w | Complete remission of skin findings (SCORAD < 10) and pruritus at wk 4 | [229] | ||
| Hyper-IgE syndrome (DOCK8-mutation) | case report (5) | 1 | M/13 | severe generalized eczema | recurrent skin infections, asthma, allergic rhinigis, multiple type-I allergies, drug allergies | topical and systemic steroids, omalizumab, MTX, IVIG, ciclosporin | ciclosporin; IVIG (discontinued); topical and systemic steroids (discontinued) | Dupilumab 200 mg s.c. q2w | Partial sustained remission of skin findings and pruritus | [230] | |
| Hyper-IgE syndrome (DOCK8-mutation) | case series (4) | 2 | F/11, F/10 | Severe pruritic eczema on extremities and trunk | recurrent skin infections and pneumonia (2/2), type-I allergies (1/2) | Yes (>2000/µL) | topical (2/2) and systemic steroids (1/2), antihistamines, antibiotics | topical (2/2) and systemic steroids (1/2) | Dupilumab 600 mg s.c., then 300 mg q2w (1/2) or 400 mg s.c., then 200 mg q2w (1/2) | Significant improvement of pruritus and skin lesions at 4 wk, less frequent skin infections (2/2) | [231] |
| Kimura disease | case report (5) | 1 | M/57 | itchy subcutaneous nodule on left arm | Yes (3520/µL) | none | Dupilumab 600 mg s.c., then 300 mg q2w, later q4w | Complete resolution at 4 wk, sustained at 10 mo | [232] | ||
| Kimura disease | case report (5) | 1 | M/36 | subcutaneous nodule on left thigh | surgical excision | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution, sustained at 12 mo follow-up | [233] | |||
| Kimura disease | case report (5) | 1 | M/59 | itchy and painful subcutaneous nodules in the face | schistosomiasis (7 years prior) | Yes (15% of leukocytes) | systemic steroids, antibiotics, dapsone, indomethacin | Dupilumab 300 mg s.c. q2w | Complete resolution of skin findings at 4 wk, sustained for 6 mo follow-up | [234] | |
| Kimura disease | case report (5) | 1 | M/57 | bilateral auricular subcutaneous masses | Yes (1640/µL, 22.8% of leukocytes) | systemic steroid, omalizumab | Dupilumab 600 mg s.c., then 300 mg q2w | Size reduction at 16 wk follow-up | [235] | ||
| Papulo-erythro-derma Ofuji | case series (4) | 2 | M/80s, M/90s | pruritic confluent papules, erythroderma, deck-chair sign | Yes | topical and systemic steroids | Dupilumab 600 mg s.c., then 300 mg q2w, later q4w (1/2) or q6w (1/2) | Complete resolution of skin lesions and pruritus (NRS 10 to 0) at 16 wk (2/2) | [236] | ||
| Papulo-erythro-derma Ofuji | case report (5) | 1 | M/65 | disseminated pruritic papules | no AD or atopy | Yes (1000/µL) | topical and systemic steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution of skin lesions and pruritus (NRS 0) at 14 wk | [237] | |
| Papulo-erythro-derma Ofuji | case report (5) | 1 | M/80s | disseminated pruritic papules | Yes (24.8% of leukocytes) | antihistamines, topical steroids, minocycline, antibiotics, ciclosporin | Dupilumab | Complete resolution of skin lesions and pruritus at 6 mo | [238] | ||
| Wells syndrome | case report (5) | 1 | F/52 | pruritic morphea-like indurated plaques | eosinophilic asthma, nasal polyps | dapsone, systemic steroids, benralizumab | systemic steroids, tapered | Dupilumab | Complete resolution after 6 mo, improvement of asthma | [239] | |
| Wells syndrome | case report (5) | 1 | F/80 | relapsing painful arcuate patches and plaques | systemic steroids, dapsone, hydroxychloroquine, doxycycline, ciclosporin | dapsone 100 mg/d | Dupilumab 400 mg s.c., then 200 mg q2w | Resolution of skin lesions after 5 wk | [240] | ||
| EAE | case report (5) | 1 | F/14 | annular urticarial plaques on trunk, arms and forehead with severe pruritus with central hyperpigmentation | none | Yes (700/µL, 11.3% of leukocytes) | topical and systemic steroids, dapsone, tofacitinib | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution of skin lesions and pruritus after 4 wk | [241] | |
| EAE | case report (5) | 1 | F/56 | annular plaques on trunk and arms with polycyclic margins and central hyperpigmentation, intense pruritus | none | No | topical and systemic steroids, ciclosporin, hydroxychloroquine, dapsone, MTX, thalidomide, indomethacin | systemic steroid, tapered | Dupilumab 600 mg s.c., then 300 mg q2w | Complete remission after 4 wk | [242] |
| Eosino-philic fasciitis | case report (5) | 1 | M/46 | Swelling and induration of skin on abdomen and arms, groove sign of superficial veins | Yes (1110/µL) | Systemic steroid | Systemic steroid, tapered | Dupilumab 300 mg s.c. q2w | Resolution of skin findings (clinically and in MRI) after 10 wk | [243] | |
| Angiolym-phoid hyperplasia with eosino-philia | case report (5) | 1 | F/68 | diffuse pruritic dermal nodules on face, arms and trunk | Yes (1200/µL) | Mepolizumab, benralizumab | Dupilumab 300 mg s.c. q2w | Resolution of skin findings after 4 wk. Dupilumab discontinued after 6 mo with sustained response. | [244] |
| Disease | Study Type | n | Sex/Age | Medical History | Prior Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Lichen sclerosus | case report (5) | 1 | F/80 | topical steroids, MMF (2 g/d), phototherapy, MTX (15 mg/wk) | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of itch and skin lesions after 12 wk, complete resolution after 10 mo | [245] | ||
| Dermatomyositis | case report (5) | 1 | F/28 | topical and systemic steroids, dapsone, MTX, azathioprin, hydroxychloroquine, thalidomide | Dupilumab 600 mg s.c., then 300 mg q2w | No improvement of pruritus, discontinued | [246] | ||
| IgG4-related disease | case report (5) | 1 | M/67 | AD, allergic rhinoconjunctivitis, asthma, obstructive sleep apnea | systemic steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Resolution of retroperitoneal fibrosis and skin lesions after 12 mo | [247] | |
| Keloid | case report (5) | 1 | M/53 | Severe AD | intralesional steroids | Dupilumab 300 mg s.c. q2w | Drastic size reduction | [248] | |
| Keloid | case report (5) | 1 | F/37 | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of pain, no size reduction of keloid | [249] | |||
| Keloid | case series (4) | 8 | 32.5 (median, 23–52 range), females: 2/8 | Dupilumab 300 mg s.c. q2w | No effects or deterioration | [250] | |||
| Keloid | case series (4) | 2 | F/17, M/17 | acne vulgaris, folliculitis | intralesional steroids (2/2), isotretinoin (1/2), doxycycline (1/2) | Dupilumab 300 mg s.c. q2w | No improvement of pain, itch or size of keloid | [251] | |
| CAD | case series (4) | 4 | 42.6 (median, 25–59 range), females: 2/4 | topical (4/4) or systemic (2/4) steroids, topical calcineurin inhibitors (1/4) antihistamines (1/4), azathioprine (2/4), ciclosporine (3/4), hydroxychloroquine (3/4), MTX (2/4), thalidomide (1/4), MMF (1/4) | photoprotection (4/4), topical steroids (2/4), azathioprine (1/4, tapered), hydroxychloroquine (1/4), MTX (1/4, tapered), ciclosporin (1/4, tapered), thalidomide (1/4) | Dupilumab 600 mg s.c., then 300 mg q2w | Reduced itch and skin lesions by week 2–8 (4/4) | [252] | |
| CAD | case series (4) | 5 | 66 (median, 49–79 range), females: 1/5 | topical (5/5) or systemic (2/5) steroids, hydroxychloroquine (1/5), MMF (5/5), MTX (1/5), azathioprine (1/5) | none | Dupilumab 600 mg s.c., then 300 mg q2w | Significant improvement of itch and skin lesions (5/5); dupilumab discontinued due to facial erythema (1/5) | [253] | |
| CAD | case report (5) | 1 | M/45 | AD | topical and systemic steroids, MTX, antihistamines, ciclosporine (75 mg/d), hydroxychloroquine (0.2 g/d) | ciclosporine (75 mg/d, tapered) | Dupilumab 600 mg s.c., then 300 mg q2w | Resolution of pruritus at 8 wk, reduction in skin lesions, improved quality of life (DLQI 17 to 2) | [254] |
| CAD | case report (5) | 1 | M/82 | topical steroids, antihistamines, hydroxychloroquine | topical steroids, hydroxychloroquine (400 mg/d) | Dupilumab 600 mg s.c., then 300 mg q2w | Clearance of skin lesions at 16 wk | [255] | |
| CAD | case report (5) | 1 | M/60 | no atopy | topical and systemic steroids, MTX (25 mg/wk), ciclosporin (5 mg/kg/d), azathioprine (100 mg/d) | MTX (15 mg/wk) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete remission after 5 mo | [256] |
| CAD | case series (4) | 3 | M/58, M/77, M/69 | AD (1/3) | topical (3/3) and systemic (2/3) steroid, MTX (2/3), antihistamines (2/3), hydroxychloroquine (3/3), azathioprine (1/3), MMF (1/3) | hydroxychloro-quine 200 mg/d (3/3) | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution (3/3) | [257] |
| CAD | case report (5) | 1 | M/54 | AD, allergic rhinitis, alopecia universalis | topical and systemic steroids, MTX (15 mg/wk), MMF (1 g/d), azathioprine (50 mg/d), hydroxychloroquine (400 mg/d), apremilast (60 mg/d), ciclosporine (200 mg/d) | pulsed prednisone, topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Partial response at 9 mo | [258] |
| Actinic prurigo | case report (5) | 1 | F/7 | cheilitis | antihistamines, topical steroids, ciclosporin (5 mg/kg/d), MTX (0.4 mg/kg/wk) | MTX, discontinued after 8 wk | Dupilumab 400 mg s.c., then 200 mg q2w | 50% improvement in pruritus at 4 wk, resolution of skin lesions at 8 wk | [259] |
| GVHD | case series (4) | 4 | 6.5 (median, 4–17 range), females: 3/4 | cord blood transplantation (3/4), peripheral stem cell transplantation (1/4) | topical (4/4) and systemic (1/4) steroids, topical calcineurin inhibitors (3/4), phototherapy (1/4), systemic tacrolimus (3/4), MMF 3/4), ruxolitinib (2/4) | Dupilumab 400 mg s.c., then 200 mg q4w (2/4), 200 mg s.c. q2w (1/4), 600 mg s.c., then 300 mg q3w (1/2) | Complete resolution (IGA 0; 3/4), no response (1/4) | [260] | |
| Palmoplantar pustulosis | case report (5) | 1 | M/52 | non-atopic | topical steroids, topical vitamin D-derivatives, secukinumab (300 mg qw) | Dupilumab 300 mg s.c. q2w | Complete resolution after 4 wk | [261] | |
| Lichen planus | case report (5) | 1 | M/52 | no atopy | topical and systemic steroids, acitretin | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of pruritus (NRS 9 to 1), improvement of skin lesions | [8] | |
| Lichen planus | case report (5) | 1 | F/92 | topical and systemic steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Ccomplete clearance of skin lesions and pruritus after 4 wk | [262] | ||
| Lichen planus | case report (5) | 1 | M/52 | AD | topical and systemic steroids, acitretin | Dupilumab 600 mg s.c., then 300 mg q2w | Partial resolution of skin lesions, resolution of itch (NRS 1/10) after 12 wk | [263] | |
| HS | case report (5) | 1 | M/25 | severe AD | ciclosporin (200 mg/d), minocycline (100 mg/d) | systemic clindamycin | Dupilumab 600 mg s.c., then 300 mg q2w | IHS4 < 3 after 12 mo | [264] |
| HS | case report (5) | 1 | M/43 | AD | ciclosporin, lymecycline | Dupilumab 600 mg s.c., then 300 mg q2w | No flare of HS in 6 mo | [265] | |
| HS | case report (5) | 1 | M/50 | AD | adalimumab | Dupilumab 600 mg s.c., then 300 mg q2w | HiSCR achieved after 16 wk | [266] | |
| Granuloma anulare | case report (5) | 1 | F/74 | topical steroids, hydroxychloroquine, MTX, niacinamide, adalimumab, antibiotics | Dupilumab 600 mg s.c., then 300 mg q2w | Nearly complete clearance of skin lesions after 4 wk | [267] | ||
| Lichen amyloido-sus | case report (5) | 1 | F/49 | AD | topical steroids, antihistamines | Dupilumab | Flattening of LA papules and reduction of itch | [268] | |
| Lichen amyloido-sus | case series (4) | 2 | F/28, F/30 | AD | topical steroids, topical calcineurin inhibitors, phototherapy, ciclosporin (all: 1/2) | Dupilumab | Complete resolution of skin lesions and pruritus (NRS 2) after 5 or 6 mo | [269] | |
| Lichen amyloido-sus | case report (5) | 1 | M/76 | no atopy | phototherapy, amitriptyline, antihistamines, acitretin, benralizumab | Dupilumab 600 mg s.c., then 300 mg q2w | Flattening of papules, resolution of pruritus after 12 wk | [270] | |
| Food allergy | case report (5) | 1 | F/30 | AD, allergic rhinitis, anaphylactic shock after ingestion of corn, several food type-I sensitivities | Dupilumab 600 mg s.c., then 300 mg q2w | Oral provocation with peanuts and corn with no reaction after 3 mo | [271] | ||
| Peanut allergy | interventional study (3) | 24 | 11.7 (mean, 3.28 SD), females: 6/24 | Dupilumab | Double-blind placebo-controlled food challenge (DBPCFC) passed by 8.3% | NCT 03793608 |
| Disease | Study Type | n | Sex/Age | Medical History | Prior Therapies | Concomitant Therapy | Therapy | Response | Reference |
|---|---|---|---|---|---|---|---|---|---|
| CTCL (Sézary), St. IVA1 (T4, N0, M0, B2) | case report (5) | 1 | M/68 | AD | phototherapy, ECP, bexarotene, interferon a-2b, topical steroids | phototherapy, ECP, bexarotene, interferon a-2b, topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Reduction of blood involvement, partial resolution of skin findings, improvement of itch after 12 wk | [272] |
| CTCL (Sézary), St. IVA1 (pT4, N1, B2, M0) | case report (5) | 1 | F/74 | phototherapy, topical and systemic steroids, ciclosporin, ECP, interferon a-2a | ECP | Dupilumab 600 mg s.c., then 300 mg q2w | Improvement of pruritus (NRS 2) and quality of life (DLQI) within days | [273] | |
| CTCL (MF) (1/2), Sézary (1/2) | case series (4) | 2 | F/37, M/55 | AD (1/2) | topical steroids, phototherapy, ciclosporin (1/2) | Dupilumab | MF (1/2): improvement of pruritus and partial remission of MF after 16 wk, Sézary (1/2): no effect | [274] | |
| CTCL (MF) St. IIB (T3 N0 M0 B0) | case report (5) | 1 | F/51 | no AD | azathioprin, topical and systemic steroids | Dupilumab | Relief of pruritus but spreading of plaques and new skin tumors. | [275] | |
| CTCL (MF) St. IB-IIIB | case series (4) | 7 | 65.6 (median, 40–77 range), females: 3/7 | Dupilumab | Initial improvement (median duration 2 mo, 6/7). Subsequent progression (7/7), progression into Sézary syndrome (3/7), death (2/7) | [276] | |||
| CTCL (Sézary), St. IVA1 (T4, N2, M0, B2) | case report (5) | 1 | F/48 | AD | Dupilumab | CTCL developed under therapy with dupilumab. Therapy was discontinued. | [277] | ||
| CTCL (MF) St. ≥ III (T4 Nx M0 Bx) | case report (5) | 1 | F/47 | AD | CTCL developed under therapy with dupilumab. Therapy was discontinued. | [278] | |||
| CTCL (MF) St. IB (T2 N0 M0 B0) | case report (5) | 1 | M/58 | AD, allergic rhinitis, conjunctivitis, asthma | topical steroids | Dupilumab 600 mg s.c., then 300 mg q2w | Exacerbation under dupilumab | [279] | |
| CTCL (MF) St. IIA (T2 N1 M0 B0) | case report (5) | 1 | M/72 | topical steroids and calcineurin inhibitors | Progression under dupilumab | [280] | |||
| CTCL (MF) St. IB (2/2) | case series (4) | 2 | F/48, M/55 | AD (2/2) | topical steroids (2/2), MTX (1/2), phototherapy (2/2) | Dupilumab | No effect, discontinued after 5 or 6 mo | [281] | |
| CTCL (Sézary), St. IVA1 (T4 N0 M0 B2) | case report (5) | 1 | M/64 | AD | topical steroids, phototherapy | Dupilumab 600 mg s.c. single dose | CTCL developed under dupilumab for AD | [282] | |
| Cutaneous B cell pseudolymphoma | case report (5) | 1 | M/76 | topical steroids, rituximab, hydroxychloroquine, MTX | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution of skin findings at 6 wk | [283] | ||
| CTCL (MF) St. IB (T2b N0 M0 B0), lichenoid drug eruption associated with mogamulizumab | case report (5) | 1 | F/26 | topical and systemic steroids, antihistamines | Mogamulizumab discontinued | Dupilumab 600 mg s.c., then 300 mg q2w | Complete resolution of drug eruption and improvement of itch after 4 mo | [284] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olbrich, H.; Sadik, C.D.; Ludwig, R.J.; Thaçi, D.; Boch, K. Dupilumab in Inflammatory Skin Diseases: A Systematic Review. Biomolecules 2023, 13, 634. https://doi.org/10.3390/biom13040634
Olbrich H, Sadik CD, Ludwig RJ, Thaçi D, Boch K. Dupilumab in Inflammatory Skin Diseases: A Systematic Review. Biomolecules. 2023; 13(4):634. https://doi.org/10.3390/biom13040634
Chicago/Turabian StyleOlbrich, Henning, Christian D. Sadik, Ralf J. Ludwig, Diamant Thaçi, and Katharina Boch. 2023. "Dupilumab in Inflammatory Skin Diseases: A Systematic Review" Biomolecules 13, no. 4: 634. https://doi.org/10.3390/biom13040634
APA StyleOlbrich, H., Sadik, C. D., Ludwig, R. J., Thaçi, D., & Boch, K. (2023). Dupilumab in Inflammatory Skin Diseases: A Systematic Review. Biomolecules, 13(4), 634. https://doi.org/10.3390/biom13040634