1. Introduction
Kidney segmentation algorithms are routinely used to extract regions of interest (ROIs) from entire medical images and help radiologists make clinical decisions [
1]. Given its advantages of being painless, noninvasive, and cost-efficient, ultrasound (US) imaging is a good option for evaluating kidney health [
2]. However, manually labeling US kidney images is tedious and complex. To reduce the workload of radiologists and increase the efficiency of annotation, there is a demand for an automatic US kidney segmentation algorithm for clinical applications [
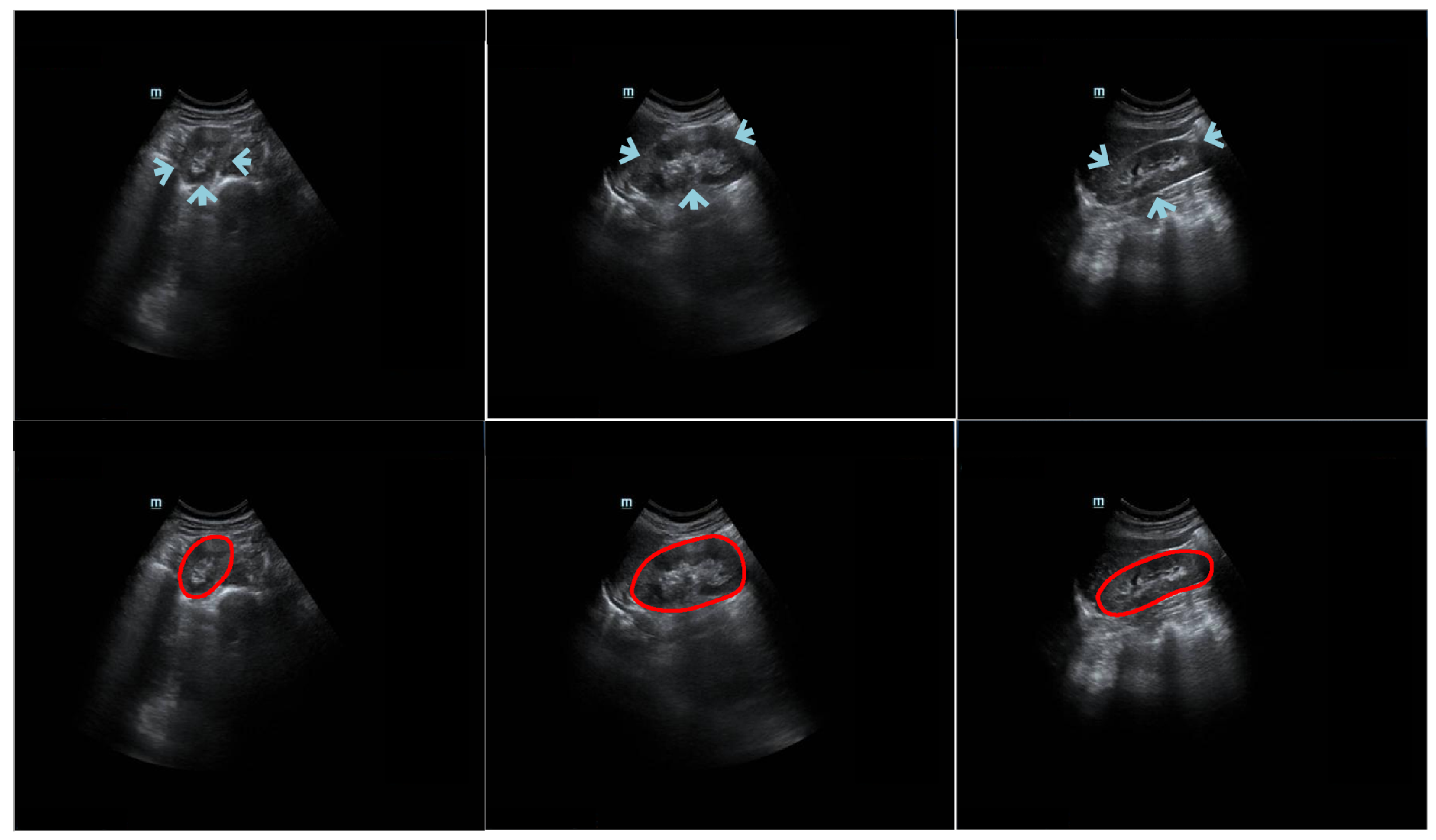
3]. It is challenging to develop such an algorithm because (1) the kidney boundary may not always be complete and prominent due to interference from neighboring tissues (e.g., intestinal gas) [
4]; (2) the kidney boundary may have low contrast; (3) the intensity of the kidney structure may follow different distributions; and (4) kidney shape varies across patients. The challenges of kidney segmentation in trans-abdominal US images are illustrated in
Figure 1.
Two main kinds of medical image segmentation algorithms are currently used: region-based [
5,
6] and contour-based [
7,
8]. Torres et al. [
9] proposed a fast phase-based method for US kidney segmentation and achieved a DSC of around 0.81. Nevertheless, when a phase-based feature detection algorithm was utilized to extract the initial contour around the external dark-to-bright transition, the refinement step, which used a B-spline active surface framework, was prone to becoming stuck at a local minimum. Chen et al. [
10] designed a deep convolutional neural architecture for segmenting US kidney slices. However, the outcome of the model was strongly influenced by the image quality, vagueness of the outline, and heterogeneous construction. This increased the potential of the method to wrongly detect and segment several slices. Yin et al. [
11] combined a boundary detection network with a transfer learning architecture for US kidney segmentation. Their method may have been restrained by the capability of the transfer learning architecture to capture kidney features. In other words, the capability of their proposed method relied on the performance of the pre-trained visual geometry group (VGG) model. Unlike region segmentation algorithms, contour segmentation algorithms have the merit of easily detecting the appearance of an anatomical structure.
Using the shape representation [
12] or the curve approximation method [
13,
14], contour-based segmentation algorithms can be used to delineate the contours of organs. Zheng et al. [
15] integrated image intensity information and texture information into a dynamic graph-cutting method to segment US kidney slices. Their method achieved good segmentation performance with reasonable initialization (i.e., intensity and texture information). Marsousi et al. [
16] proposed a new shape model to segment US kidney images using shape and anatomical knowledge as prior initialization. In Ref. [
17], a phase-based distance regularized evolution model was proposed for segmenting the ROI of the kidney, with the partial phase and feature used as priors to improve segmentation accuracy. However, their method required too many parameters to be initialized by humans. Using a parametric super-ellipse as a global shape initialization, Huang et al. [
12] designed a contour-based model for US kidney segmentation tasks with the aim of solving two problems: finding the segmented boundary of a fixed prior shape and determining the deformation parameters of the super-ellipse for the obtained segmented boundary. However, in practical scenarios, it was difficult for radiologists to manually determine an initialized shape-based ellipse’s central point that had the same location as the actual kidney contour’s central point.
We developed an automatic coarse-to-refinement segmentation network for kidney segmentation in US images. In the coarse segmentation stage, we used a deep fusion learning network (DFLN). In the DFLN, we integrated a deep parallel architecture consisting of an attention gate (AG) module [
18] and a squeeze and excitation (SE) module [
19] into the U-Net architecture [
20]. Furthermore, we used an automatic searching polygon tracking (ASPT) method coupled with an adaptive learning-rate backpropagation neural network (ABNN) [
21] to express a mathematical map function of a smooth kidney contour and optimize the coarse segmentation outcome. Compared with existing segmentation strategies, our new method has the following advantages:
Our fully automatic coarse-to-refinement segmentation method is more suitable for practical applications than manual and semi-automatic methods that require excessive human intervention.
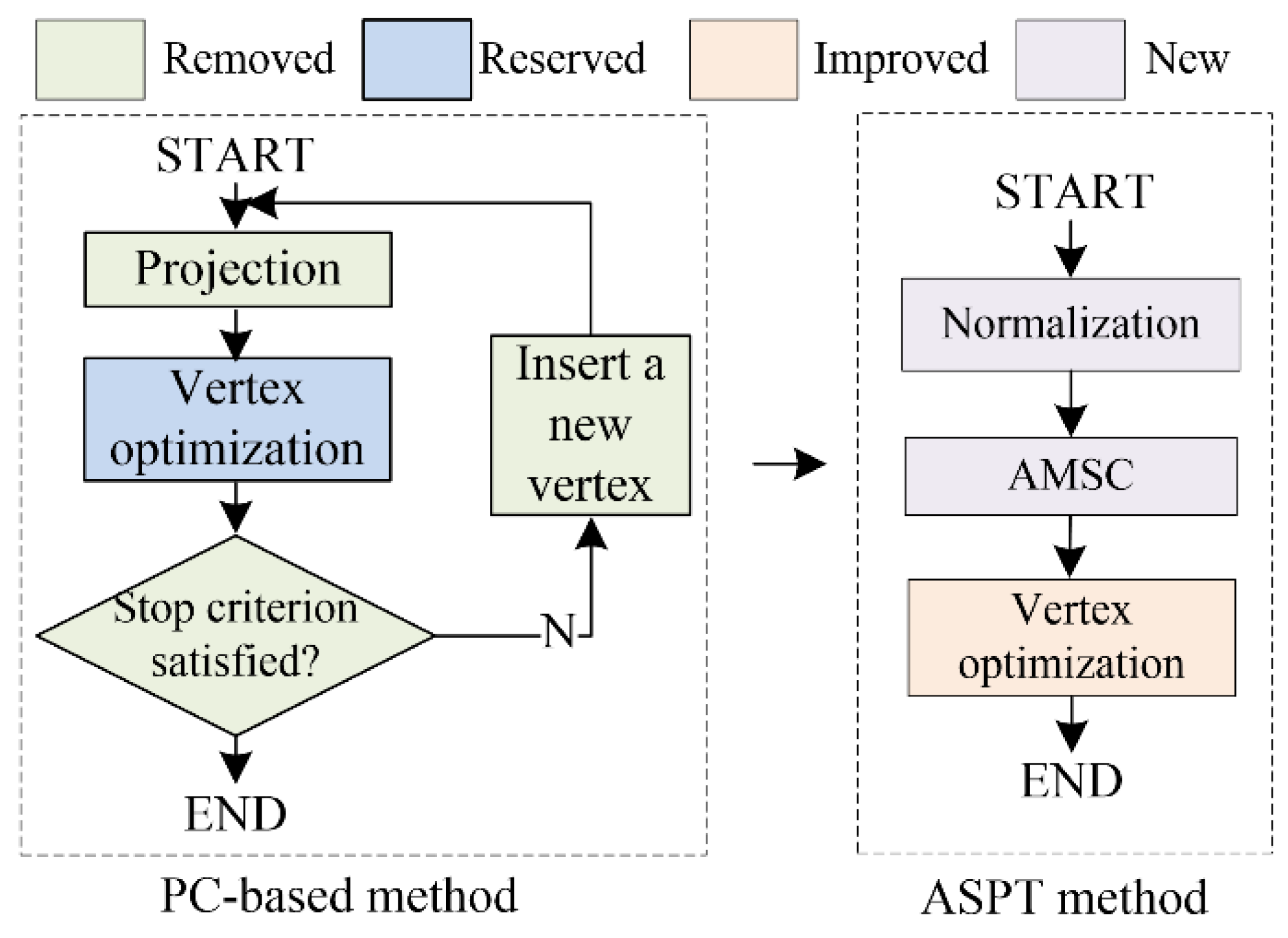
Our previous study proposed a closed polygonal segment method [
22] for the first time to address the drawbacks of the
K-segments polygonal segment algorithm [
23], which could not handle closed data well. Furthermore, we devised an enhanced polygonal segment algorithm [
24,
25] to minimize interference with the principal curve (PC) by abnormal data points. The above methods are standard PC-based methods. In this study, we devised an ASPT method to replace the standard PC-based methods for automatically determining vertices and clusters without prior knowledge.
In our method, an explainable mathematical mapping function of the kidney boundary is represented by the parameters of the ABNN. During ABNN training, model deviation is reduced to yield a precise outcome.
Work related to the current study was accepted at the 2021 IEEE International Conference on Bioinformatics and Biomedicine (BIBM) conference [
14]. There are some differences between the conference paper and the current study:
4. Discussion
This paper presents a novel mechanism to segment kidneys in US images. The proposed method has three attributes: (1) an automatic deep fusion learning network; (2) an automatic searching polygon tracking method; and (3) an interpretable mathematical formula for the kidney boundary. To assess the capability of our method for kidneys with inconsistent appearances, kidney images of 115 patients were used for a detailed qualitative and quantitative evaluation. Our work demonstrated that (1) our model exhibited good outcomes for different patients and evaluation metrics (DSC and Ω); and (2) our model outperformed other existing models. We discuss more details of the overall work below.
We collected trans-abdominal US scanning-based data from 115 patients, with left and right kidney images for each patient. The left and right kidneys could not be acquired in the same image because (1) there is a long distance between them, (2) they are separated by the spine, and (3) the probe scan range is limited.
As shown in
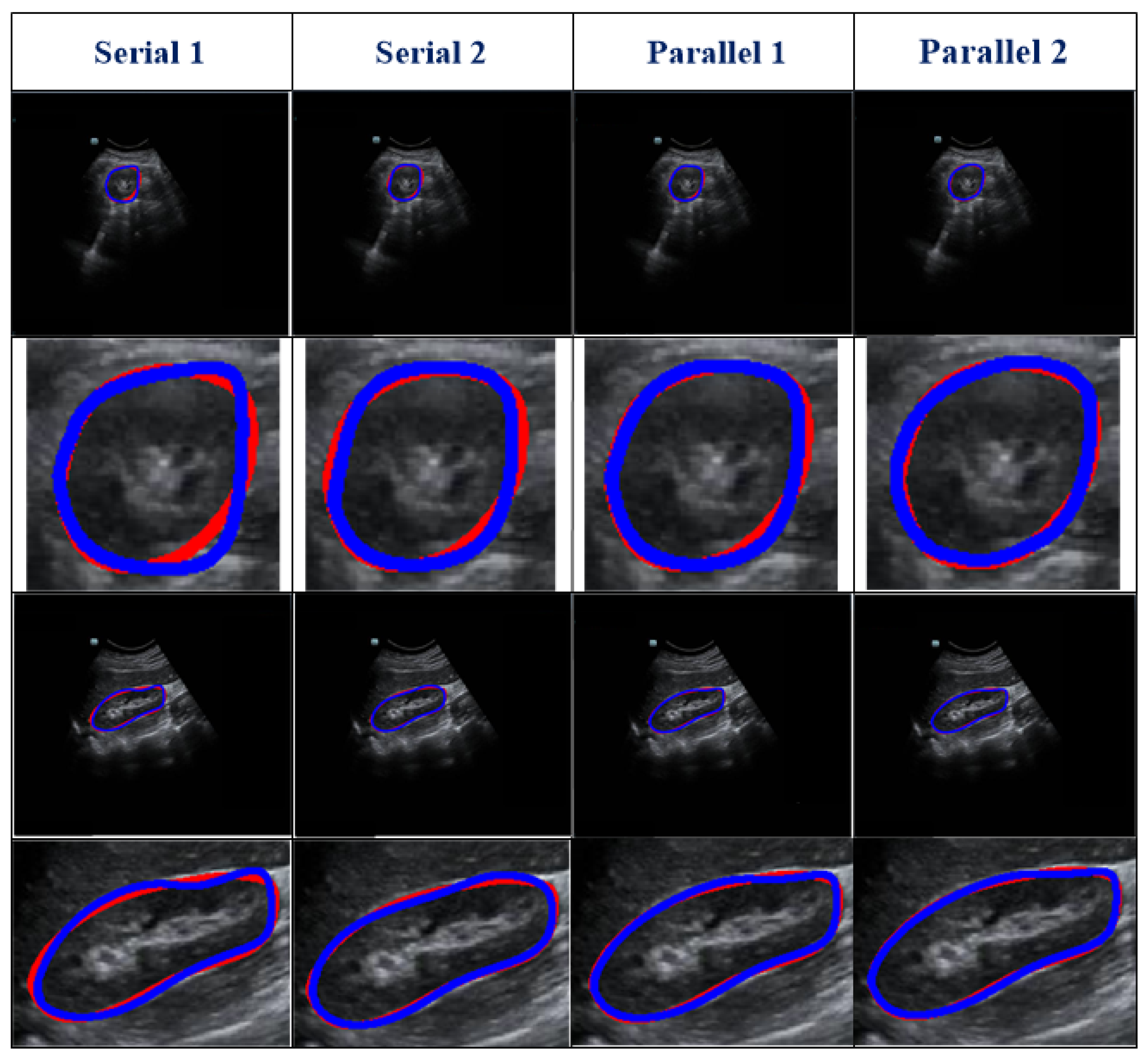
Table 2, different serial and parallel architectures resulted in different levels of performance for the coarse segmentation strategy. There are three aspects of the outcomes presented in
Table 2 to be discussed.
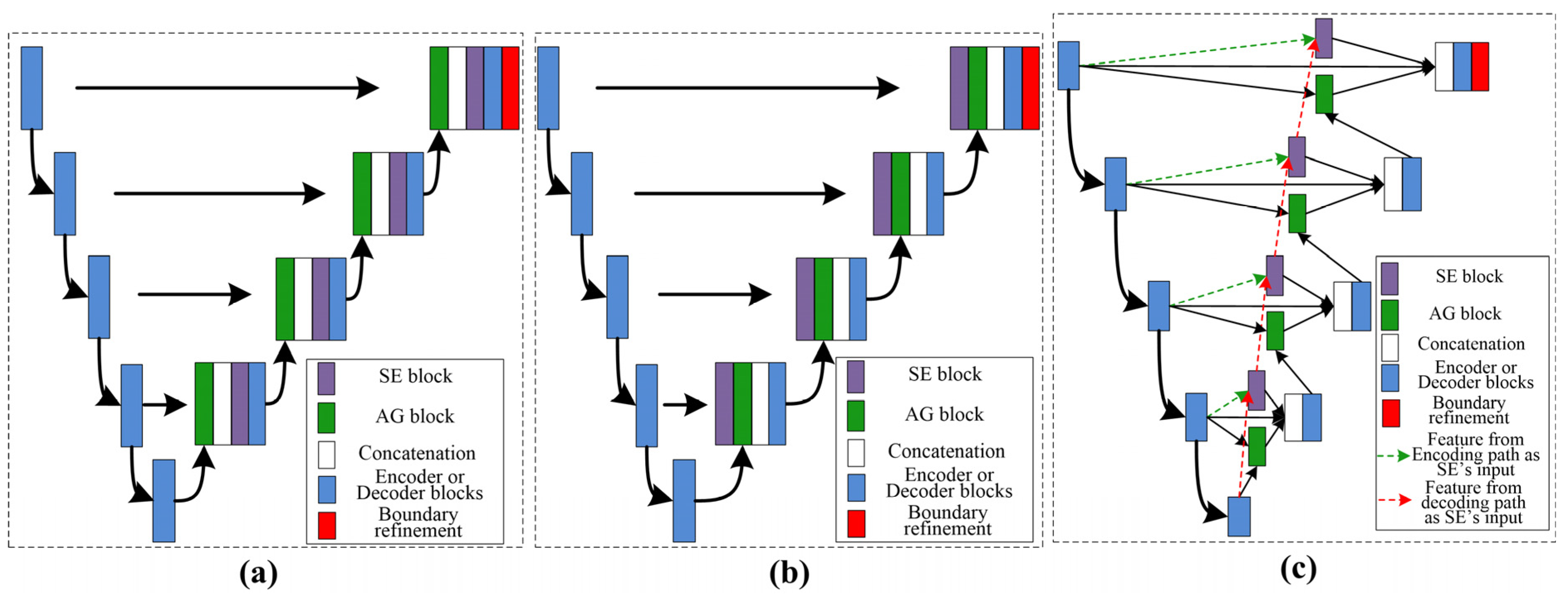
First, overall, the parallel architecture showed better capability than the serial architecture. Both the AG [
18] and SE [
19] modules are known to have a good ability to boost relevant features and remove irrelevant features. However, using serial AG and SE modules may cause the deletion of a large amount of information, some of which may be useful.
Second, of the serial architectures evaluated, SE-AG (
Figure 3b) showed better performance than AG-SE (
Figure 3a). The main reason for this is that the AG module has a more complex structure than the SE module (as shown in
Section 2.3), which makes it difficult to train the AG module and avoid the loss of meaningful information.
Third, as illustrated in
Table 2, the Parallel 2 model performed better than the Parallel 1 model. The main difference between these two parallel architectures is in the input for the SE module, with one using features from the decoding path (Parallel 1) and the other using features from the encoding path (Parallel 2). Parallel 2 may perform better because using encoding features as the input for the SE module carries the merit of the SE module to emphasize meaningful features and suppress less useful features.
As shown in
Figure 6, we used an ablation comparison to demonstrate the capability of our method. The regions indicated by arrows are missing or ambiguous due to different factors. The white and green arrows indicate the blurry boundary of the kidney caused by intestinal gas and the spleen, respectively. The orange arrow indicates the ambiguous boundary of the kidney due to the kidney’s thickness and internal structure (i.e., renal pelvis, calyces, blood vessels, and adipose tissue). However, the model with a refinement step still obtained highly accurate results.
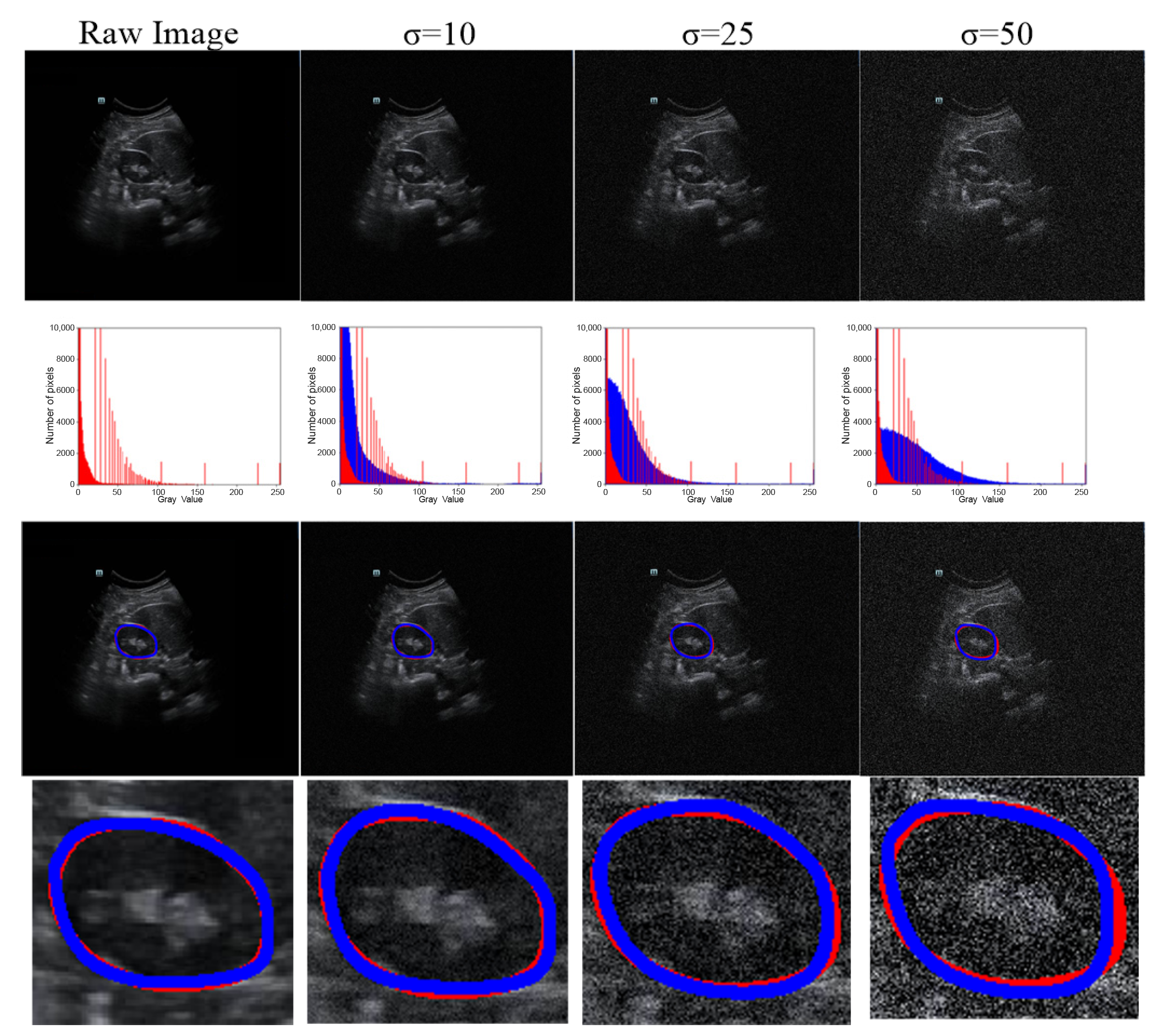
As US images are grayscale, most of the pixels are black and have a gray value of zero. To better distinguish the effect of other pixel points (gray value > 0), we only selected the number of pixels within the range [0, 10,000] in the image to show the distribution of pixel points with different gray values (
Table 4 and
Figure 7). When we added more Gaussian noise (σ increases), the number of pixels with gray values greater than 0 increased. This illustrates that the degree of damage to the original images increased. However, the DSC values were greater than 90% even for images with a severe level of noise (σ = 50). This indicates that the blurry boundaries were efficiently detected (
Table 3 and
Figure 7).
Figure 8 shows zoomed-in images corresponding to those in
Figure 7.
Although our method yielded promising results, several aspects require improvement. First, we want to further evaluate our method on multiple modalities (i.e., computed tomography and magnetic resonance slices) and multi-site data. Second, to achieve the goal of real-time clinical applications, model compression of our coarse-to-refinement method may be necessary to reduce the memory burden during the execution process. Third, we wish to evaluate our method on different organs or multi-organs such as the prostate, bladder, and fetal head. Finally, chronic nephritis, renal vascular disease, kidney transplantation, hydronephrosis, kidney tumors, and other diseases require highly accurate measurements of kidney volume. This plays a crucial role in the selection of treatment methods and postoperative evaluation. In the future, we will discuss the performance of our method in these directions.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}