
Effects of RIPC on the Metabolome in Patients Undergoing Vascular Surgery: A Randomized Controlled Trial

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility and Study Groups
2.2. Randomization
2.3. Intervention
2.4. Blinding
2.5. Outcomes
2.6. Statistical Analysis
3. Results
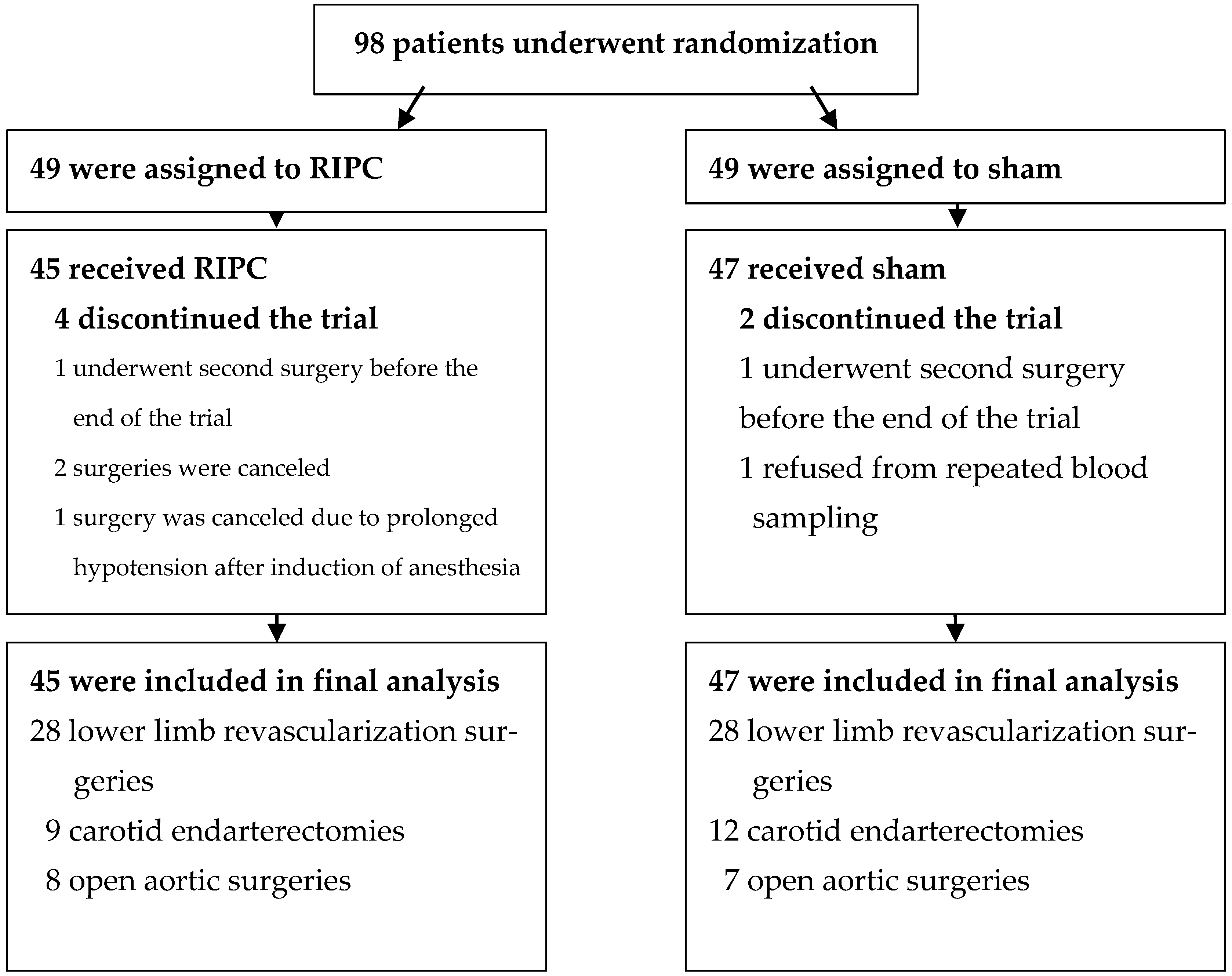
3.1. Overview of the Study Groups
3.2. Changes in the Metabolites 24 h Postoperatively
3.3. Correlations of the Metabolites with Cardiac and Kidney Markers in the RIPC Group
3.4. Correlations of the Metabolites with Heart and Kidney Markers in the Sham Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anttila, V.; Haapanen, H.; Yannopoulos, F.; Herajärvi, J.; Anttila, T.; Juvonen, T. Review of remote ischemic preconditioning: From laboratory studies to clinical trials. Scand. Cardiovasc. J. 2016, 50, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Stather, P.W.; Wych, J.; Boyle, J.R. A systematic review and meta-analysis of remote ischemic preconditioning for vascular surgery. J. Vasc. Surg. 2019, 70, 1353–1363.e3. [Google Scholar] [CrossRef] [PubMed]
- Kepler, T.; Kuusik, K.; Lepner, U.; Starkopf, J.; Zilmer, M.; Eha, J.; Vähi, M.; Kals, J. Remote ischaemic preconditioning attenuates cardiac biomarkers during vascular surgery: A randomised clinical trial. EJVES 2020, 59, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Kasepalu, T.; Kuusik, K.; Lepner, U.; Starkopf, J.; Zilmer, M.; Eha, J.; Vähi, M.; Kals, J. Remote ischaemic preconditioning reduces kidney injury biomarkers in patients undergoing open surgical lower limb revascularisation: A randomised trial. Oxid. Med. Cell. Longev. 2020, 2020, 7098505. [Google Scholar] [CrossRef]
- Kasepalu, T.; Kuusik, K.; Lepner, U.; Starkopf, J.; Zilmer, M.; Eha, J.; Vähi, M.; Kals, J. Remote ischaemic preconditioning influences the levels of acylcarnitines in vascular surgery: A randomised clinical trial. Nutr. Metab. 2020, 17, 76. [Google Scholar] [CrossRef]
- Shen, S.; Wang, J.F.; Wu, J.Q.; Zhou, J.X.; Meng, S.D.; Ma, J.; Zhu, C.L.; Deng, G.G.; Liu, D. GC/MS-based metabolomic analysis of alleviated renal ischemia-reperfusion injury induced by remote ischemic preconditioning. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 765–774. [Google Scholar]
- Baranovicova, E.; Kalenska, D.; Grendar, M.; Lehotsky, J. Metabolomic recovery as a result of ischemic preconditioning was more pronounced in hippocampus than in cortex that appeared more sensitive to metabolomic blood components. Metabolites 2021, 11, 516. [Google Scholar] [CrossRef]
- Chao de la Barca, J.M.; Bakhta, O.; Kalakech, H.; Simard, G.; Tamareille, S.; Catros, V.; Callebert, J.; Gadras, C.; Tessier, L.; Reynier, P.; et al. Metabolic signature of remote ischemic preconditioning involving a cocktail of amino acids and biogenic amines. JAHA 2016, 5, e003891. [Google Scholar] [CrossRef]
- Boldyrev, A.A.; Aldini, G.; Derave, W. Physiology and pathophysiology of carnosine. Physiol. Rev. 2013, 93, 1803–1845. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, H.; McKenzie, G.; Witting, P.K.; Stasch, J.P.; Hahn, M.; Changsirivathanathamrong, D.; Wu, B.J.; Ball, H.J.; Thomas, S.R.; et al. Kynurenine is an endothelium-derived relaxing factor produced during inflammation. Nat. Med. 2010, 16, 279–285. [Google Scholar] [CrossRef]
- Shi, H.; Kokoeva, M.V.; Inouye, K.; Tzameli, I.; Yin, H.; Flier, J.S. TLR4 links innate immunity and fatty acid–induced insulin resistance. J. Clin. Investig. 2006, 116, 3015–3025. [Google Scholar] [CrossRef] [PubMed]
- Bakhta, O.; Pascaud, A.; Dieu, X.; Beaumont, J.; Kouassi Nzoughet, J.; Kamel, R.; Croyal, M.; Tamareille, S.; Simard, G.; de la Barca, J.M.; et al. Tryptophane–kynurenine pathway in the remote ischemic conditioning mechanism. Basic Res. Cardiol. 2020, 115, 13. [Google Scholar] [CrossRef] [PubMed]
- Le Floc’h, N.; Otten, W.; Merlot, E. Tryptophan metabolism, from nutrition to potential therapeutic applications. J. Amino Acids 2011, 41, 1195–1205. [Google Scholar] [CrossRef]
- Höglund, E.; Øverli, Ø.; Winberg, S. Tryptophan metabolic pathways and brain serotonergic activity: A comparative review. Front. Endocrinol. 2019, 10, 158. [Google Scholar] [CrossRef]
- Changsiri, D.; Wang, Y.; dos Remedios, C.; Celermajer, D.; Stocker, R. Indoleamine 2,3-dioxygenase is induced in myocardium during inflammation. Heart Lung Circ. 2010, 19, S43–S44. [Google Scholar] [CrossRef]
- Torosyan, R.; Huang, S.; Bommi, P.V.; Tiwari, R.; An, S.Y.; Schonfeld, M.; Rajendran, G.; Kavanaugh, M.A.; Gibbs, B.; Truax, A.D.; et al. Hypoxic preconditioning protects against ischemic kidney injury through the IDO1/kynurenine pathway. Cell Rep. 2021, 36, 109547. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Zhang, A.; Binnie, M.; McGuire, K.; Webster, S.P.; Hughes, J.; Howie, S.E.M.; Mole, D.J. Kynurenine 3-monooxygenase is a critical regulator of renal ischemia–reperfusion injury. Exp. Mol. Med. 2019, 51, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Xiao, X.; Fogle, P.; Dong, Z. Changes in metabolic profiles during acute kidney injury and recovery following ischemia/reperfusion. PLoS ONE 2014, 9, e106647. [Google Scholar] [CrossRef]
- Wee, H.N.; Liu, J.J.; Ching, J.; Kovalik, J.P.; Lim, S.C. The kynurenine pathway in acute kidney injury and chronic kidney disease. Am. J. Nephrol. 2021, 52, 771–787. [Google Scholar] [CrossRef]
- Yun, J.H.; Kim, J.M.; Jeon, H.J.; Oh, T.; Choi, H.J.; Kim, B.J. Metabolomics profiles associated with diabetic retinopathy in type 2 diabetes patients. PLoS ONE 2020, 15, e0241365. [Google Scholar] [CrossRef]
- Chen, S.; Li, N.; Deb-Chatterji, M.; Dong, Q.; Kielstein, J.; Weissenborn, K.; Worthmann, H. Asymmetric dimethyarginine as marker and mediator in ischemic stroke. Int. J. Mol. Sci. 2012, 13, 15983–16004. [Google Scholar] [CrossRef] [PubMed]
- Ismaeel, A.; Franco, M.E.; Lavado, R.; Papoutsi, E.; Casale, G.P.; Fuglestad, M.; Mietus, C.J.; Haynatzki, G.R.; Smith, R.S.; Bohnnon, W.T.; et al. Altered metabolomic profile in patients with peripheral artery disease. J. Clin. Med. 2019, 8, 1463. [Google Scholar] [CrossRef] [PubMed]
- Behmenburg, F.; van Caster, P.; Bunte, S.; Brandenburger, T.; Heinen, A.; Hollmann, M.W.; Huhn, R. Impact of anesthetic regimen on remote ischemic preconditioning in the rat heart in vivo. Anesth. Analg. 2018, 126, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Moretti, C.; Cerrato, E.; Cavallero, E.; Lin, S.; Rossi, M.L.; Picchi, A.; Sanguineti, F.; Ugo, F.; Palazzuoli, A.; Bertaina, M.; et al. The EUROpean and Chinese cardiac and renal remote ischemic preconditioning study (EURO-CRIPS CardioGroup I): A randomized controlled trial. Int. J. Cardiol. 2018, 257, 1–6. [Google Scholar] [CrossRef]
- Wider, J.; Undyala, V.V.R.; Whittaker, P.; Woods, J.; Chen, X.; Przyklenk, K. Remote ischemic preconditioning fails to reduce infarct size in the Zucker fatty rat model of type-2 diabetes: Role of defective humoral communication. Basic Res. Cardiol. 2018, 113, 16. [Google Scholar] [CrossRef]
- Loukogeorgakis, S.P.; Panagiotidou, A.T.; Broadhead, M.W.; Donald, A.; Deanfield, J.E.; MacAllister, R.J. Remote ischemic preconditioning provides early and late protection against endothelial ischemia-reperfusion injury in humans. J. Am. Coll. Cardiol. 2005, 46, 450–456. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | RIPC (n = 45) | Sham (n = 47) | p-Value |
|---|---|---|---|
| Age, years (SD) | 67 (± 9) | 66 (± 10) | 0.577 |
| Male, n (%) | 36 (80) | 32 (68) | 0.288 |
| BMI, kg/m2 (SD) | 26.3 (± 6.4) | 26.5 (± 6.7) | 0.840 |
| ASA 2, n (%) | 18 (40) | 19 (40) | 1 |
| ASA 3, n (%) | 20 (44) | 22 (47) | 0.986 |
| ASA 4, n (%) | 7 (16) | 6 (13) | 0.933 |
| ACEI or ARB, n (%) | 21 (47) | 30 (64) | 0.148 |
| Calcium channel blockers, n (%) | 9 (20) | 17 (37) | 0.135 |
| Beta-blockers, n (%) | 11 (24) | 19 (40) | 0.158 |
| Statins, n (%) | 13 (29) | 14 (30) | 1 |
| Diabetes, n (%) | 5 (11) | 8 (17) | 0.607 |
| Myocardial infarction, n (%) | 8 (18) | 3 (6) | 0.172 |
| Stroke, n (%) | 10 (22) | 12 (26) | 0.899 |
| Smoker (current or ex-smoker), n (%) | 40 (89) | 42 (89) | 1 |
| MAP, mmHg (SD) | 99 (± 12) | 100 (± 11) | 0.678 |
| Heart rate, bpm (SD) | 66 (± 9) | 67 (± 11) | 0.754 |
| Cholesterol, mmol/L (IQR) | 5.0 (4.2–5.7) | 5.0 (3.9–5.6) | 0.793 |
| LDL, mmol/L (IQR) | 3.4 (8.1–10.4) | 3.3 (2.5–3.8) | 0.500 |
| HDL, mmol/L (IQR) | 1.1 (0.9–1.4) | 1.1 (1.0–1.3) | 0.311 |
| Triglycerides, mmol/L (IQR) | 1.6 (1.3–1.8) | 1.5 (1.2–2.0) | 0.787 |
| Administration on propofol, n (%) | 19 (42) | 26 (55) | 0.295 |
| Duration of surgery, min (IQR) | 108 (89–135) | 112 (84–156) | 0.827 |
| Metabolic Group and Metabolites | Baseline Comparison * | Change 24 h Postoperatively * |
|---|---|---|
| Amino acids (n = 19) Ala, Arg, Cit, Gln, Glu, Gly, His, Ile, Leu, Lys, Met, Orn, Phe, Pro, Ser, Thr, Trp, Tyr, Val | p ˃ 0.001 | p ˃ 0.001 |
| Biogenic amines (n = 7) ADMA, Creatinine, Kynurenine, Serotonine, Spermine, Taurine, total DMA | p ˃ 0.001 | p ˃ 0.001 |
| Glycerophospholipids (n = 62) lysoPCaC16:0, lysoPCaC16:1, lysoPCaC17:0, lysoPCaC18:0, lysoPCaC18:1, lysoPCaC18:2, lysoPCaC20:3, lysoPCaC20:4, lysoPCaC26:1, PCaaC28:1, PCaaC30:0, PCaaC32:0, PCaaC32:1, PCaaC32:2, PCaaC32:3, PCaaC34:1, PCaaC34:2, PCaaC34:4, PCaaC36:0, PCaaC36:1, PCaaC36:2, PCaaC36:3, PCaaC36:4, PCaaC36:5, PCaaC38:0, PCaaC38:3, PCaaC38:4, PCaaC38:5, PCaaC38:6, PCaaC40:4, PCaaC40:5, PCaaC40:6, PCaaC42:4, PCaaC42:5, PCaaC42:6, PCaeC30:1, PCaeC32:1, PCaeC32:2, PCaeC34:0, PCaeC34:1, PCaeC34:2, PCaeC34:3, PCaeC36:0, PCaeC36:1, PCaeC36:2, PCaeC36:3, PCaeC36:4, PCaeC36:5, PCaeC38:0, PCaeC38:3, PCaeC38:4, PCaeC38:5, PCaeC38:6, PCaeC40:1, PCaeC40:2, PCaeC40:4, PCaeC40:5, PCaeC40:6, PCaeC42:4, PCaeC44:4, PCaeC44:5, PCaeC44:6 | p ˃ 0.001 | p ˃ 0.001 |
| Sphingolipids (n = 14) SM(OH)C14:1, SM(OH)C16:1, SM(OH)C22:1, SM(OH)C22:2, SM(OH)C24:1, SMC16:0, SMC16:1, SMC18:0, SMC18:1, SMC20:2, SMC24:0, SMC24:1, SMC26:0, SMC26:1 | p ˃ 0.001 | p ˃ 0.001 |
| Hexoses (n = 1) H1 | p ˃ 0.001 | p ˃ 0.001 |
| Metabolic ratios (n = 20) (C2 + C3)/C0, AAA, ADMA/Arg, BCAA, C2/C0, Cit/Arg, Cit/Orn, Essential AA, Fisher ratio, Glucogenic AA, Kynurenine/Trp, Nonessential AA, Orn/Arg, Putrescine/Orn, Serotonin/Trp, Total SM, Total SM-nonOH, Total SM-OH, Total SM-OH/Total SM-nonOH, Tyr/Phe | p ˃ 0.001 | p ˃ 0.001 |
| Baseline | Change 24 h Postoperatively | |||||
|---|---|---|---|---|---|---|
| Sham | RIPC | Sham | RIPC | |||
| Metabolite | Mean (±SD)/Median (IQR) | Mean (±SD)/Median (IQR) | p-Value | Mean (±SD)/Median (IQR) | Mean (±SD)/Median (IQR) | p-Value |
| Ala | 392.5 (±91.4) | 385.5 (±89.9) | 0.715 | −25.3 (±120.7) | −11.6 (±123.7) | 0.592 |
| Arg | 114.3 (±29.6) | 120.4 (±35.4) | 0.365 | −20.0 (±38.7) | −21.0 (−35.8–(−2.0)) | 0.591 |
| Cit | 35.9 (±8.2) | 34.2 (±9.8) | 0.384 | -8.8 (±8.9) | −7.6 (±7.8) | 0.496 |
| Gln | 812.0 (±132.5) | 836.5 (±186.1) | 0.470 | −150.5 (±170.0) | −161.5 (±189.4) | 0.770 |
| Glu | 72.9 (55.4–95.9) | 57.1 (46.4–74.8) | 0.036 | −0.7 (−15.5–14.6) | −12.7 (−24.0–14.0) | 0.128 |
| Gly | 240.0 (189.0–286.0) | 247.0 (202.0–288.0) | 0.885 | −26.3 (±53.4) | −22.4 (±52.7) | 0.723 |
| His | 91.8 (±19.4) | 94.7 (±18.7) | 0.479 | −12.7 (±13.4) | −14.7 (±18.6) | 0.550 |
| Ile | 85.0 (72.8–103.0) | 85.5 (70.6–108.0) | 0.867 | −16.4 (±28.9) | −25.0 (±32.7) | 0.188 |
| Leu | 180.0 (147.0–203.0) | 168.0 (144.0–205.0) | 0.680 | −28.2 (±54.6) | −46.1 (±52.3) | 0.112 |
| Lys | 251.9 (±62.3) | 271.0 (±71.0) | 0.171 | −50.3 (±65.5) | −56.5 (±63.2) | 0.645 |
| Met | 23.0 (±5.6) | 24.5 (±6.4) | 0.232 | −1.6 (±7.3) | −1.2 (±9.6) | 0.822 |
| Orn | 96.3 (±26.0) | 97.4 (±23.5) | 0.826 | −25.2 (±30.6) | −26.0 (±24.8) | 0.894 |
| Phe | 70.5 (63.7–83.3) | 72.1 (65.8–78.3) | 0.697 | 2.2 (±12.7) | −1.1 (±14.8) | 0.255 |
| Pro | 204.7 (±49.7) | 206.6 (±63.3) | 0.877 | −13.0 (±55.0) | −17.0 (−42.0–21.0) | 0.666 |
| Ser | 134.0 (±34.9) | 133.1 (±31.4) | 0.893 | −27.1 (±37.9) | −32.0 (−53.8–(−10.0)) | 0.222 |
| Thr | 147.0 (109.0–251.0) | 111.0 (92.5–161.0) | 0.072 | −21.6 (±49.1) | −20.9 (−81.0–12.0) | 0.516 |
| Trp | 64.9 (54.3–76.4) | 66.0 (53.9–74.4) | 0.885 | −8.8 (±17.4) | −10.0 (±15.2) | 0.725 |
| Tyr | 64.5 (±12.7) | 70.9 (±15.1) | 0.028 | −3.9 (±16.1) | −5.3 (±18.9) | 0.692 |
| Val | 266.5 (±53.0) | 265.5 (±71.7) | 0.941 | −22.2 (±74.6) | −37.8 (±72.9) | 0.315 |
| ADMA | 0.6 (±0.2) | 0.6 (±0.1) | 0.741 | −0.1 (±0.2) | −0.1 (±0.2) | 0.833 |
| Creatinine | 105.0 (81.3–151.0) | 108.0 (76.4–143.0) | 0.640 | 1.0 (−9.0–20.0) | -3.7 (−15.0–22.0) | 0.322 |
| Kynurenine | 0.04 (0.03–0.05) | 0.04 (0.03–0.05) | 0.353 | 0.1 (±0.7) | 0.1 (±1.0) | 0.842 |
| Serotonine | 0.4 (0.3–0.6) | 0.5 (0.03–0.7) | 0.421 | −0.1 (±0.1) | −0.1 (±0.1) | 0.717 |
| Spermine | 0.0 (0.0–3.8) | 0.0 (0.0–3.8) | 0.711 | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.030 |
| Taurine | 107.0 (±30.0) | 105.6 (±32.0) | 0.827 | −14.9 (±30.1) | −10.3 (±31.4) | 0.475 |
| Total DMA | 1.1 (±0.3) | 1.1 (±0.3) | 0.330 | −0.08 (±0.3) | −0.09 (±0.4) | 0.932 |
| H1 | 4825.0 (4245.0–5231.0) | 4505.0 (4207.0–5013.0) | 0.128 | 1231.6 (±1798.1) | 1157.7 (±1431.5) | 0.828 |
| AAA | 204.2 (±35.7) | 211.7 (±36.8) | 0.325 | −10.4 (±37.0) | −16.3 (±38.5) | 0.453 |
| ADMA/ Arg | 0.01 (0.00–0.01) | 0.01 (0.00–0.01) | 0.841 | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.776 |
| BCAA | 532.2 (±96.7) | 537.9 (±143.3) | 0.825 | −104.0 (−183.0–(−29.0)) | −81.0 (−159.0–53.0) | 0.238 |
| Cit/Arg | 0.3 (±0.1) | 0.3 (±0.1) | 0.276 | −0.02 (±0.11) | 0.00 (±0.11) | 0.422 |
| Cit/Orn | 0.4 (±0.1) | 0.4 (±0.1) | 0.342 | 0.04 (−0.07–0.09) | 0.00 (−0.12–0.14) | 0.474 |
| Essential AA | 1087.5 (±208.4) | 1081.5 (±212.4) | 0.893 | −160.0 (±254.7) | −185.4 (±241.4) | 0.625 |
| Fisher ratio | 2.6 (±0.4) | 2.5 (±0.5) | 0.326 | −0.3 (±0.6) | −0.3 (±0.6) | 0.456 |
| Glucogenic AA | 740.0 (690.0–872.0) | 765.0 (701.0–839.0) | 0.770 | −84.8 (±162.9) | −57.8 (±175.6) | 0.445 |
| Kynurenine/Trp | 0.04 (±0.02) | 0.04 (±0.01) | 0.654 | 0.01 (0.00–0.01) | 0.01 (0.00–0.02) | 0.741 |
| Nonessential AA | 2319.6 (±252.8) | 2346.0 (±338.1) | 0.671 | −339.9 (±362.3) | −324.0 (±413.2) | 0.845 |
| Orn/Arg | 0.8 (0.7–1.1) | 0.8 (0.6–1.0) | 0.741 | −0.1 (−0.2–0.1) | −0.1 (−0.3–0.1) | 0.901 |
| Serotonin/Trp | 0.01 (0.01–0.01) | 0.01 (0.01–0.01) | 0.391 | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.991 |
| Tyr/Phe | 0.9 (±0.2) | 1.0 (±0.2) | 0.115 | −0.1 (±0.2) | −0.1 (±0.2) | 0.692 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eerik, K.; Kasepalu, T.; Kuusik, K.; Eha, J.; Vähi, M.; Kilk, K.; Zilmer, M.; Kals, J. Effects of RIPC on the Metabolome in Patients Undergoing Vascular Surgery: A Randomized Controlled Trial. Biomolecules 2022, 12, 1312. https://doi.org/10.3390/biom12091312
Eerik K, Kasepalu T, Kuusik K, Eha J, Vähi M, Kilk K, Zilmer M, Kals J. Effects of RIPC on the Metabolome in Patients Undergoing Vascular Surgery: A Randomized Controlled Trial. Biomolecules. 2022; 12(9):1312. https://doi.org/10.3390/biom12091312
Chicago/Turabian StyleEerik, Kadri, Teele Kasepalu, Karl Kuusik, Jaan Eha, Mare Vähi, Kalle Kilk, Mihkel Zilmer, and Jaak Kals. 2022. "Effects of RIPC on the Metabolome in Patients Undergoing Vascular Surgery: A Randomized Controlled Trial" Biomolecules 12, no. 9: 1312. https://doi.org/10.3390/biom12091312
APA StyleEerik, K., Kasepalu, T., Kuusik, K., Eha, J., Vähi, M., Kilk, K., Zilmer, M., & Kals, J. (2022). Effects of RIPC on the Metabolome in Patients Undergoing Vascular Surgery: A Randomized Controlled Trial. Biomolecules, 12(9), 1312. https://doi.org/10.3390/biom12091312