
Association of Aneurysm Tissue Neutrophil Mediator Levels with Intraluminal Thrombus Thickness in Patients with Abdominal Aortic Aneurysm

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Sampling
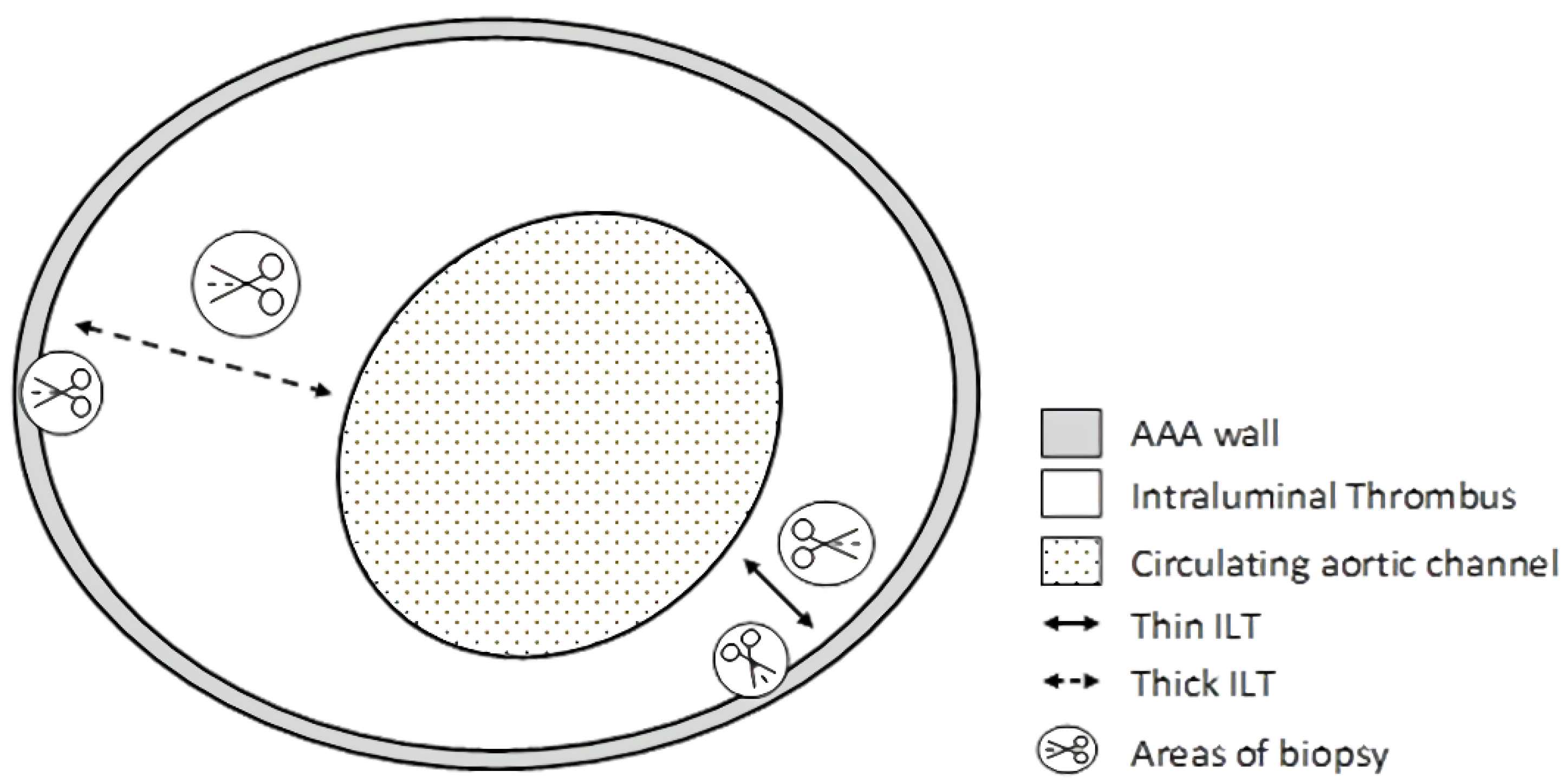
2.3. Tissue Samples
2.4. Tissue Homogenisation for Protein Analysis
2.5. ELISA Tests
2.6. Statistical Analyses
3. Results
3.1. Neutrophil Mediator Level Evaluation in Plasma/Serum
3.2. Neutrophil Mediator Distribution in Abdominal Aortic Aneurysm
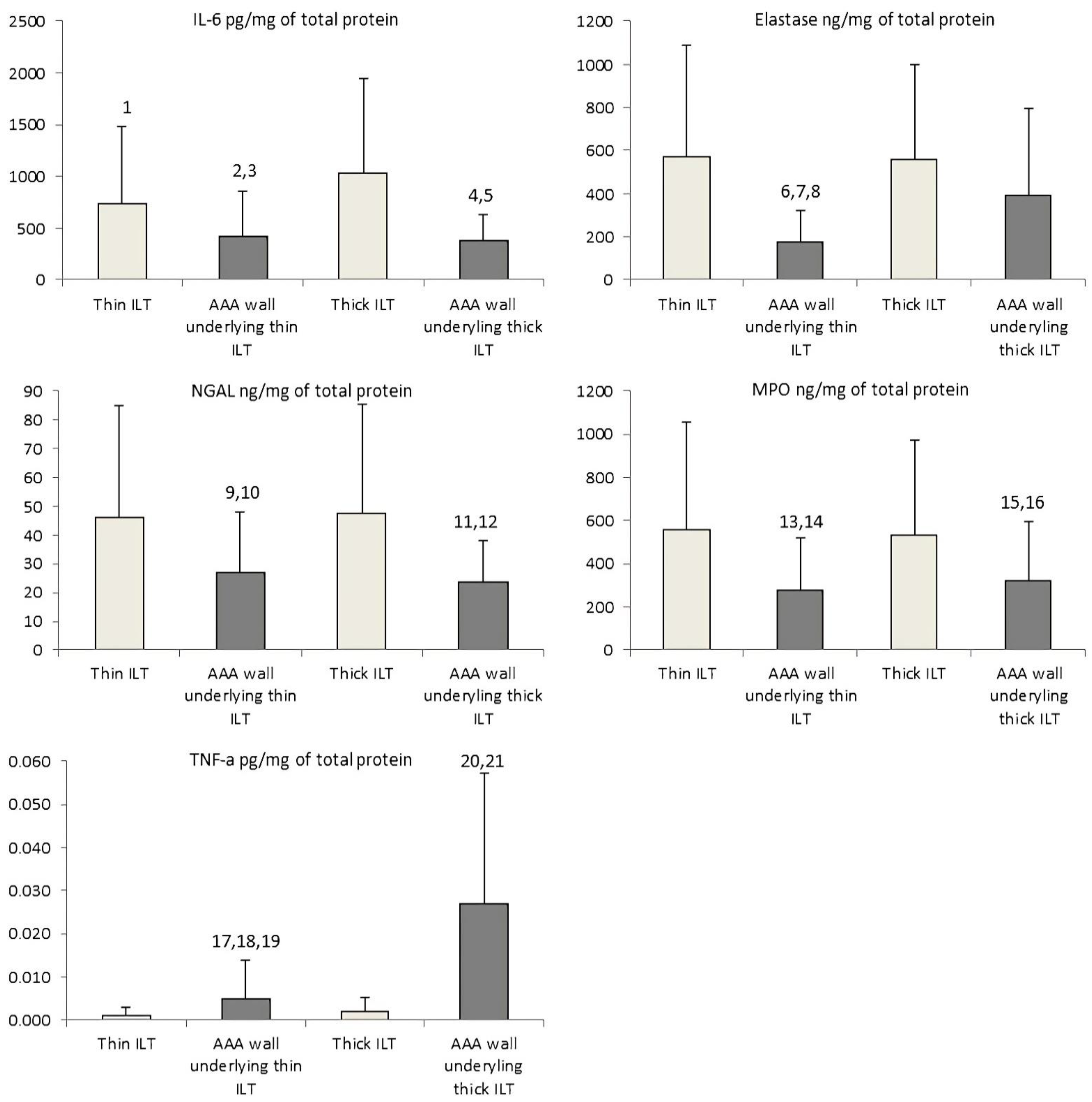
3.2.1. Interleukin 6
3.2.2. Neutrophil Elastase
3.2.3. Neutrophil Gelatinase-Associated Lipocalin
3.2.4. Myeloperoxidase
3.2.5. Tumour Necrosis Factor Alpha
3.3. Correlations between Neutrophil Mediator Levels within Thin and Thick ILT and AAA Wall Sections
3.4. Correlations of Neutrophil Mediator Levels between Thin and Thick ILT and AAA Wall Sections
3.5. Correlations of Tissue and Plasma/Serum Neutrophil Mediator Levels with ILT Thickness and AAA Diameter
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; Van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed]
- Kuivaniemi, H.; Ryer, E.J.; Elmore, J.R.; Tromp, G. Understanding the pathogenesis of abdominal aortic aneurysms. Expert. Rev. Cardiovasc. Ther. 2015, 13, 975–987. [Google Scholar] [CrossRef]
- Blassova, T.; Tonar, Z.; Tomasek, P.; Hosek, P.; Hollan, I.; Treska, V.; Molacek, J. Inflammatory cell infiltrates, hypoxia, vascularization, pentraxin 3 and osteoprotegerin in abdominal aortic aneurysms—A quantitative histological study. PLoS ONE 2019, 14, e0224818. [Google Scholar] [CrossRef] [PubMed]
- Bhagavan, D.; Di Achille, P.; Humphrey, J.D. Strongly Coupled Morphological Features of Aortic Aneurysms Drive Intraluminal Thrombus. Sci. Rep. 2018, 8, 13273. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.A.; Kavanagh, E.G.; Grace, P.A.; McGloughlin, T.M.; Doyle, B.J. The biaxial mechanical behaviour of abdominal aortic aneurysm intraluminal thrombus: Classification of morphology and the determination of layer and region specific properties. J. Biomech. 2014, 47, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.S.; Virag, L.; Di Achille, P.; Karsaj, I.; Humphrey, J.D. Biochemomechanics of intraluminal thrombus in abdominal aortic aneurysms. J. Biomech. Eng. 2013, 135, 021011. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Leach, J.R.; Wang, Y.; Gasper, W.; Saloner, D.; Hope, M.D. Intraluminal Thrombus Predicts Rapid Growth of Abdominal Aortic Aneurysms. Radiology 2020, 294, 707–713. [Google Scholar] [CrossRef]
- Fontaine, V.; Jacob, M.P.; Houard, X.; Rossignol, P.; Plissonnier, D.; Angles-Cano, E.; Michel, J.B. Involvement of the mural thrombus as a site of protease release and activation in human aortic aneurysms. Am. J. Pathol. 2002, 161, 1701–1710. [Google Scholar] [CrossRef]
- Napoli, C.; Paolisso, G.; Casamassimi, A.; Al-Omran, M.; Barbieri, M.; Sommese, L.; Infante, T.; Ignarro, L.J. Effects of nitric oxide on cell proliferation: Novel insights. J. Am. Coll. Cardiol. 2013, 62, 89–95. [Google Scholar] [CrossRef]
- Meyer, C.A.; Guivier-Curien, C.; Moore, J.E., Jr. Trans-thrombus blood pressure effects in abdominal aortic aneurysms. J. Biomech. Eng. 2010, 132, 071005:1–071005:7. [Google Scholar] [CrossRef]
- Sacks, M.S.; Vorp, D.A.; Raghavan, M.L.; Federle, M.P.; Webster, M.W. A noninvasive surface geometric analysis of in-vivo abdominal aortic aneurysms. Am. Soc. Mech. Eng. Proc. Bioeng. Conf. 1997, 35, 235–236. [Google Scholar]
- Dobrin, P.B. Pathophysiology and pathogenesis of aortic aneurysms: Current concepts. Surg. Clin. N. Am. 1989, 69, 687–703. [Google Scholar] [CrossRef]
- Siegel, C.L.; Cohan, R.H.; Korobkin, M.; Alpern, M.B.; Courneya, D.L.; Leder, R.A. Abdominal aortic aneurysm morphology: CT features in patients with ruptured and non ruptured aneurysms. AJR Am. J. Roentgenol. 1994, 163, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, T.A.; Garcia, G.N.; Dalio, M.B.; Bredarioli, M.; Bezerra, C.A.; Moriya, T. Morphological aspects of mural thrombi deposition residual lumen route in infrarenal abdominal aorta aneurisms. Acta Cir. Bras. 2008, 23, 151–156. [Google Scholar] [CrossRef][Green Version]
- Di Martino, E.S.; Bohra, A.; Vande Geest, J.P.; Gupta, N.; Makaroun, M.S.; Vorp, D.A. Biomechanical properties of ruptured versus electively repaired abdominal aortic aneurysm wall tissue. J. Vasc. Surg. 2006, 43, 570–576. [Google Scholar] [CrossRef]
- Khan, J.A.; Abdul Rahman, M.N.; Mazari, F.A.; Shahin, Y.; Smith, G.; Madden, L.; Fagan, M.J.; Greenman, J.; McCollum, P.T.; Chetter, I.C. Intraluminal thrombus has a selective influence on matrix metalloproteinases and their inhibitors (tissue inhibitors of matrix metalloproteinases) in the wall of abdominal aortic aneurysms. Ann. Vasc. Surg. 2012, 26, 322–329. [Google Scholar] [CrossRef]
- Wiernicki, I.; Stachowska, E.; Safranow, K.; Cnotliwy, M.; Rybicka, M.; Kaczmarczyk, M.; Gutowski, P. Enhanced matrix-degrading proteolytic activity within the thin thrombus-covered wall of human abdominal aortic aneurysms. Atherosclerosis 2010, 212, 161–165. [Google Scholar] [CrossRef]
- Folkesson, M.; Silveira, A.; Eriksson, P.; Swedenborg, J. Protease activity in the multi-layered intra-luminal thrombus of abdominal aortic aneurysms. Atherosclerosis 2011, 218, 294–299. [Google Scholar] [CrossRef]
- Swedenborg, J.; Eriksson, P. The intraluminal thrombus as a aource of proteolytic activity. Ann. N. Y. Acad. Sci. 2006, 1085, 133–138. [Google Scholar] [CrossRef]
- Eliason, J.L.; Hannawa, K.K.; Ailawadi, G.; Sinha, I.; Ford, J.W.; Deogracias, M.P.; Roelofs, K.J.; Woodrum, D.T.; Ennis, T.L.; Henke, P.K.; et al. Neutrophil depletion inhibits experimental abdominal aortic aneurysm formation. Circulation 2005, 112, 232–240. [Google Scholar] [CrossRef]
- Dale, M.A.; Ruhlman, M.K.; Baxter, B.T. Inflammatory cell phenotypes in AAAs: Their role and potential as targets for therapy. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1746–1755. [Google Scholar] [CrossRef] [PubMed]
- De Franciscis, S.; Mastroroberto, P.; Gallelli, L.; Buffone, G.; Montemurro, R.; Serra, R. Increased plasma levels of metalloproteinase-9 and neutrophil gelatinase-associated lipocalin in a rare case of multiple aneurysms. Ann. Vasc. Surg. 2013, 27, 1185.e5–1185.e7. [Google Scholar] [CrossRef] [PubMed]
- Pearce, S.; Xiao, Q.; Wu, W.; An, W.; Yang, M. BS38 Role of neutrophil elastase in abdominal aortic aneurysms and thoracic aortic dissection. Heart 2019, 105, A164. [Google Scholar] [CrossRef]
- Shah, A.D.; Denaxas, S.; Nicholas, O.; Hingorani, A.D.; Hemingway, H. Neutrophil Counts and Initial Presentation of 12 Cardiovascular Diseases: A CALIBER Cohort Study. J. Am. Coll. Cardiol. 2017, 7, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Mozo, P.; Madrigal-Matute, J.; Martinez-Pinna, R.; Blanco-Colio, L.M.; Lopez, J.A.; Camafeita, E.; Meilhac, O.; Michel, J.B.; Aparicio, C.; Vega de Ceniga, M.; et al. Proteomic analysis of polymorphonuclear neutrophils identifies catalase as a novel biomarker of abdominal aortic aneurysm: Potential implication of oxidative stress in abdominal aortic aneurysm progression. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 3011–3019. [Google Scholar] [CrossRef]
- Kim, H.W.; Blomkalns, A.L.; Ogbi, M.; Thomas, M.; Gavrila, D.; Neltner, B.S.; Cassis, L.A.; Thompson, R.W.; Weiss, R.M.; Lindower, P.D.; et al. Role of myeloperoxidase in abdominal aortic aneurysm formation: Mitigation by taurine. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H1168–H1179. [Google Scholar] [CrossRef]
- Kaneko, H.; Anzai, T.; Horiuchi, K.; Kohno, T.; Nagai, T.; Anzai, A.; Takahashi, T.; Sasaki, A.; Shimoda, M.; Maekawa, Y.; et al. Tumor necrosis factor-α converting enzyme is a key mediator of abdominal aortic aneurysm development. Atherosclerosis 2011, 218, 470–478. [Google Scholar] [CrossRef]
- Kolaczkowska, E.; Kubes, P. Neutrophil recruitment and function in health and inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef]
- Ijaz, T.; Tilton, R.G.; Brasier, A.R. Cytokine amplification and macrophage effector functions in aortic inflammation and abdominal aortic aneurysm formation. J. Thorac. Dis. 2016, 8, E746–E754. [Google Scholar] [CrossRef]
- Dawson, J.; Cockerill, G.W.; Choke, E.; Belli, A.M.; Loftus, I.; Thompson, M.M. Aortic aneurysms secrete interleukin-6 into the circulation. J. Vasc. Surg. 2007, 45, 350–356. [Google Scholar] [CrossRef]
- Wallinder, J.; Bergqvist, D.; Henriksson, A.E. Proinflammatory and anti-inflammatory cytokine balance in patients with abdominal aortic aneurysm and the impact of aneurysm size. Vasc. Endovascular Surg. 2009, 43, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Kokje, V.B.C.; Gäbel, G.; Koole, D.; Northoff, B.H.; Holdt, L.M.; Hamming, J.F.; Lindeman, J.H.N. IL-6: A Janus-like factor in abdominal aortic aneurysm disease. Atherosclerosis 2016, 251, 139–146. [Google Scholar] [CrossRef] [PubMed]
- De Ceniga, M.V.; Esteban, M.; Barba, A.; Estallo, L.; Blanco-Colio, L.M.; Martin-Ventura, J.L. Assessment of biomarkers and predictive model for short-term prospective abdominal aortic aneurysm growth—A pilot study. Ann. Vasc. Surg. 2014, 28, 1642–1648. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Watanabe, T.; Mizuno, Y.; Kawai, N.; Umemoto, T. Circulating interleukin-6 levels are associated with abdominal aortic aneurysm presence: A meta-analysis and meta-regression of case-control studies. Ann. Vasc. Surg. 2014, 28, 1913–1922. [Google Scholar] [CrossRef]
- Serra, R.; Grande, R.; Montemurro, R.; Butrico, L.; Caliò, F.G.; Mastrangelo, D.; Scarcello, E.; Gallelli, L.; Buffone, G.; De Franciscis, S. The role of matrix metalloproteinases and neutrophil gelatinase-associated lipocalin in central and peripheral arterial aneurysms. Surgery 2015, 157, 155–162. [Google Scholar] [CrossRef]
- Lindeman, J.H.; Abdul-Hussien, H.; Van Bockel, J.H.; Wolterbeek, R.; Kleemann, R. Clinical trial of doxycycline for matrix metalloproteinase-9 inhibition in patients with an abdominal aneurysm: Doxycycline selec tively depletes aortic wall neutrophils and cytotoxic T cells. Circulation 2009, 119, 2209–2216. [Google Scholar] [CrossRef]
- Houard, X.; Touat, Z.; Ollivier, V.; Louedec, L.; Philippe, M.; Sebbag, U.; Meilhac, O.; Rossignol, P.; Michel, J.B. Mediators of neutrophil recruitment in human abdominal aortic aneurysms. Cardiovasc. Res. 2009, 82, 532–541. [Google Scholar] [CrossRef]
- Coutard, M.; Touat, Z.; Houard, X.; Leclercq, A.; Michel, J.B. Thrombus versus wall biological activities in experimental aortic aneurysms. J. Vasc. Res. 2010, 47, 355–366. [Google Scholar] [CrossRef]
- Ducas, A.A. Increased matrix metalloproteinase 9 activity correlates with flow-mediated intraluminal thrombus deposition and wall degeneration in human abdominal aortic aneurysm. JVS Vasc. Sci. 2020, 1, 190–199. [Google Scholar] [CrossRef]
- Zambrano, B.A.; Gharahi, H.; Lim, C.; Jaberi, F.A.; Choi, J.; Lee, W.; Baek, S. Association of Intraluminal Thrombus, Hemodynamic Forces, and Abdominal Aortic Aneurysm Expansion Using Longitudinal CT Images. Ann. Biomed. Eng. 2016, 44, 1502–1514. [Google Scholar] [CrossRef]
- Fontaine, V.; Touat, Z.; Mtairag, E.M.; Vranckx, R.; Louedec, L.; Houard, X.; Andreassian, B.; Sebbag, U.; Palombi, T.; Jacob, M.P.; et al. Role of leukocyte elastase in preventing cellular re-colonization of the mural thrombus. Am. J. Pathol. 2004, 164, 2077–2087. [Google Scholar] [CrossRef]
- Shimizu, K.; Mitchell, R.N.; Libby, P. Inflammation and cellular immune responses in abdominal aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Moris, D.; Mantonakis, E.; Avgerinos, E.; Makris, M.; Bakoyiannis, C.; Pikoulis, E.; Georgopoulos, S. Novel biomarkers of abdominal aortic aneurysm disease: Identifying gaps and dispelling misperceptions. Biomed. Res. Int. 2014, 2014, 925840. [Google Scholar] [CrossRef]
- Maurice, P.; Blaise, S.; Gayral, S.; Debelle, L.; Laffargue, M.; Hornebeck, W.; Duca, L. Elastin fragmentation and atherosclerosis progression: The elastokine concept. Trends Cardiovasc. Med. 2013, 23, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Teng, Z.; Elkhawad, M.; Tarkin, J.M.; Joshi, N.; Boyle, J.R.; Buscombe, J.R.; Fryer, T.D.; Zhang, Y.; Park, A.Y.; et al. High Structural Stress and Presence of Intraluminal Thrombus Predict Abdominal Aortic Aneurysm 18F-FDG Uptake: Insights From Biomechanics. Circ. Cardiovasc. Imaging 2016, 9, e004656. [Google Scholar] [CrossRef]
- Vorp, D.A.; Lee, P.C.; Wang, D.H.; Makaroun, M.S.; Nemoto, E.M.; Ogawa, S.; Webster, M.W. Association of intraluminal thrombus in abdominal aortic aneurysm with local hypoxia and wall weakening. J. Vasc. Surg. 2001, 34, 291–299. [Google Scholar] [CrossRef]
- Hartney, T.; Birari, R.; Venkataraman, S.; Villegas, L.; Martinez, M.; Black, S.M.; Stenmark, K.R.; Nozik-Grayck, E. Xanthine oxidase-derived ROS upregulate Egr-1 via ERK1/2 in PA smooth muscle cells; model to test impact of extracellular ROS in chronic hypoxia. PLoS ONE 2011, 6, e27531. [Google Scholar] [CrossRef]
- Wiernicki, I.; Parafiniuk, M.; Kolasa-Wołosiuk, A.; Gutowska, I.; Kazimierczak, A.; Clark, J.; Baranowska-Bosiacka, I.; Szumilowicz, P.; Gutowski, P. Relationship between aortic wall oxidative stress/proteolytic enzyme expression and intraluminal thrombus thickness indicates a novel pathomechanism in the progression of human abdominal aortic aneurysm. FASEB J. 2019, 33, 885–895. [Google Scholar] [CrossRef]
- Koole, D.; Zandvoort, H.J.; Schoneveld, A.; Vink, A.; Vos, J.A.; van den Hoogen, L.L.; de Vries, J.P.; Pasterkamp, G.; Moll, F.L.; van Herwaarden, J.A. Intraluminal abdominal aortic aneurysm thrombus is associated with disruption of wall integrity. J. Vasc. Surg. 2013, 57, 77–83. [Google Scholar] [CrossRef]
- Folkesson, M.; Kazi, M.; Zhu, C.; Silveira, A.; Hemdahl, A.L.; Hamsten, A.; Hedin, U.; Swedenborg, J.; Eriksson, P. Presence of NGAL/MMP-9 complexes in human abdominal aortic aneurysms. Thromb. Haemost. 2007, 98, 427–433. [Google Scholar] [CrossRef]
- Adolph, R.; Vorp, D.A.; Steed, D.L.; Webster, M.W.; Kameneva, M.V.; Watkins, S.C. Cellular content and permeability of intraluminal thrombus in abdominal aortic aneurysm. J. Vasc. Surg. 1997, 25, 916–926. [Google Scholar] [CrossRef]
- Kazi, M.; Thyberg, J.; Religa, P.; Roy, J.; Eriksson, P.; Hedin, U.; Swedenborg, J. Influence of intraluminal thrombus on structural and cellular composition of abdominal aortic aneurysm wall. J. Vasc. Surg. 2003, 38, 1283–1292. [Google Scholar] [CrossRef]
- Polzer, S.; Gasser, T.C.; Swedenborg, J.; Bursa, J. The impact of intraluminal thrombus failure on the mechanical stress in the wall of abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Behr Andersen, C.; Lindholt, J.S.; Urbonavicius, S.; Halekoh, U.; Jensen, P.S.; Stubbe, J.; Rasmussen, L.M.; Beck, H.C. Abdominal Aortic Aneurysms Growth Is Associated with High Concentrations of Plasma Proteins in the Intraluminal Thrombus and Diseased Arterial Tissue. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 2254–2267. [Google Scholar] [CrossRef] [PubMed]
- Launcelott, S.L.; Lozowy, R.J.; Kuhn, D.C.S.; Boyd, A.J. Abdominal Aortic Aneurysm Growth Is Associated with Changes in Thrombus Deposition. J. Vasc. Surg. 2015, 64, 1546. [Google Scholar] [CrossRef]
- Tong, J.; Cohnert, T.; Regitnig, P.; Holzapfel, G.A. Effects of age on the intraluminal thrombus elastic properties and the thrombus-covered wall in abdominal aortic aneurysms: Biaxial extension behaviour and material modelling. Eur. J. Vasc. Endovasc. Surg. 2011, 42, 207–219. [Google Scholar] [CrossRef]
- Wiernicki, I.; Millo, B.; Safranow, K.; Gorecka-Szyld, B.; Gutowski, P. MMP-9, homocysteine and CRP circulating levels are associated with intraluminal thrombus thickness of abdominal aortic aneurysms: New implication of the old biomarkers. Dis. Marker 2011, 31, 67–74. [Google Scholar] [CrossRef]
- Siennicka, A.; Zuchowski, M.; Kaczmarczyk, M.; Cnotliwy, M.; Clark, J.S.; Jastrzebska, M. Spatial differences of matrix metalloproteinase-2 and matrix metalloproteinase-9 within abdominal aortic aneurysm wall and intraluminal thrombus. J. Physiol. Pharmacol. 2016, 67, 903–910. [Google Scholar]
- Malaponte, G.; Signorelli, S.S.; Bevelacqua, V.; Polesel, J.; Taborelli, M.; Guarneri, C.; Fenga, C.; Umezawa, K.; Libra, M. Increased levels of NF-κB-dependent markers in cancer-associated deep venous thrombosis. PLoS ONE 2015, 10, e0132496. [Google Scholar] [CrossRef]
- Ramos-Mozo, P.; Madrigal-Matute, J.; Vega de Ceniga, M.; Blanco-Colio, L.M.; Meilhac, O.; Feldman, L.; Michel, J.B.; Clancy, P.; Golledge, J.; Norman, P.E. Increased plasma levels of NGAL, a marker of neutrophil activation, in patients with abdominal aortic aneurysm. Atherosclerosis 2012, 220, 552–556. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| AAA (n = 36) | Control (n = 29) | p | ||
|---|---|---|---|---|
| Age (years) | 71 ± 8 | 63 ± 7 | 0.00009 | |
| Sex (male/female) | 27 (75)/9 (25) | 21 (69)/9 (31) | 0.589 | |
| Current smoker | 17 (47) | 18 (62) | 0.232 | |
| Diabetes mellitus | 7 (19) | 7 (24) | 0.647 | |
| Hypertension | 23 (64) | 17 (59) | 0.664 | |
| CVD | Myocardial infarction | 2 (6) | 6 (21) | 0.065 |
| Stroke | 2 (6) | 5 (17) | 0.131 | |
| DVT | 1 (3) | 1 (3) | 0.876 | |
| Statin therapy | 3 (8) | 8 (28) | 0.039 | |
| MPO (ng/mL) ‡ | 491 ± 183 | 601 ± 204 | 0.025 | |
| NGAL (ng/mL) | 190 (129–351) | 439 (242–733) | 0.001 | |
| Elastase (ng/mL) | 906 (535–1317) | 1237 (842–1865) | 0.045 | |
| IL-6 (pg/mL) | 40.0 (21.6–79.4) | 32.8 (16.8–58.3) | 0.229 | |
| TNF-a (pg/mL) | 0.001 (0.001–0.008) | 0.001 (0.001–0.004) | 0.443 | |
| AAA diameter ‡ | 59 ± 12 | |||
| ILT thickness ‡ | 32 ± 10 | |||
| Correlation | AAA Wall Parts Adjacent to ILT | Intraluminal Thrombus | ||||||
|---|---|---|---|---|---|---|---|---|
| Site Adjacent to Thin ILT | Site Adjacent to Thick ILT | Site Thin | Site Thick | |||||
| R | p Corrected p-Values | R | p Corrected p-Values | R | p-Values | R | p Corrected p-Values | |
| NGAL vs. elastase | 0.81 | 0.0001 | 0.76 | 0.0001 | 0.85 | 0.0001 | 0.78 | 0.0001 |
| NGAL vs. MPO | 0.75 | 0.0001 | 0.71 | 0.0001 | 0.90 | 0.0001 | 0.77 | 0.0001 |
| NGAL vs. IL-6 | 0.30 | 0.079 | 0.43 | 0.011 | 0.23 | 0.184 | 0.40 | 0.018 |
| NGAL vs. TNF-α | −0.02 | 0.920 | −0.25 | 0.162 | 0.08 | 0.637 | −0.06 | 0.754 |
| Elastase vs. MPO | 0.85 | 0.0001 | 0.84 | 0.0001 | 0.87 | 0.0001 | 0.82 | 0.0001 |
| Elastase vs. IL-6 | 0.28 | 0.122 | 0.39 | 0.017 | 0.19 | 0.276 | 0.38 | 0.024 |
| Elastase vs. TNF-α | −0.11 | 0.554 | −0.19 | 0.252 | 0.27 | 0.222 | 0.17 | 0.341 |
| MPO vs. IL-6 | 0.50 | 0.002 | 0.58 | 0.0002 | 0.20 | 0.242 | 0.23 | 0.174 |
| MPO vs. TNF-α | −0.01 | 0.989 | −0.11 | 0.505 | 0.15 | 0.421 | 0.15 | 0.400 |
| IL-6 vs. TNF-α | 0.27 | 0.121 | 0.23 | 0.170 | 0.32 | 0.066 | 0.16 | 0.388 |
| Correlation | Thin Parts | Thick Part | ||
|---|---|---|---|---|
| Between Thin ILT and Adjacent Walls of AAA | Between Thick ILT and Adjacent Walls of AAA | |||
| R p Corrected p-Values | p p Corrected p-Values | R p Values | p p Corrected p-Values | |
| NGAL | 0.33 | 0.047 | 0.28 | 0.111 |
| Elastase | 0.31 | 0.090 | 0.35 | 0.035 |
| MPO | 0.35 | 0.034 | 0.52 | 0.001 |
| IL-6 | 0.18 | 0.040 | 0.39 | 0.022 |
| TNF-a | 0.39 | 0.028 | 0.68 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siennicka, A.; Adamowicz, M.; Grzesch, N.; Kłysz, M.; Woźniak, J.; Cnotliwy, M.; Galant, K.; Jastrzębska, M. Association of Aneurysm Tissue Neutrophil Mediator Levels with Intraluminal Thrombus Thickness in Patients with Abdominal Aortic Aneurysm. Biomolecules 2022, 12, 254. https://doi.org/10.3390/biom12020254
Siennicka A, Adamowicz M, Grzesch N, Kłysz M, Woźniak J, Cnotliwy M, Galant K, Jastrzębska M. Association of Aneurysm Tissue Neutrophil Mediator Levels with Intraluminal Thrombus Thickness in Patients with Abdominal Aortic Aneurysm. Biomolecules. 2022; 12(2):254. https://doi.org/10.3390/biom12020254
Chicago/Turabian StyleSiennicka, Aldona, Monika Adamowicz, Natalie Grzesch, Magdalena Kłysz, Jarosław Woźniak, Miłosław Cnotliwy, Katarzyna Galant, and Maria Jastrzębska. 2022. "Association of Aneurysm Tissue Neutrophil Mediator Levels with Intraluminal Thrombus Thickness in Patients with Abdominal Aortic Aneurysm" Biomolecules 12, no. 2: 254. https://doi.org/10.3390/biom12020254
APA StyleSiennicka, A., Adamowicz, M., Grzesch, N., Kłysz, M., Woźniak, J., Cnotliwy, M., Galant, K., & Jastrzębska, M. (2022). Association of Aneurysm Tissue Neutrophil Mediator Levels with Intraluminal Thrombus Thickness in Patients with Abdominal Aortic Aneurysm. Biomolecules, 12(2), 254. https://doi.org/10.3390/biom12020254