
Concerted Actions by PIICP, CTXII, and TNF-α in Patients with Juvenile Idiopathic Arthritis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. The Assay of the Concentration of PIICP, CTXII, and TNF-α
2.3. Statistical Analysis
3. Results
3.1. The Serum Levels of PIICP in Healthy Children and JIA Patients
3.2. The Serum Levels of CTXII in Healthy Children and JIA Patients
3.3. The Serum Levels of TNF-α in Healthy Children and JIA Patients
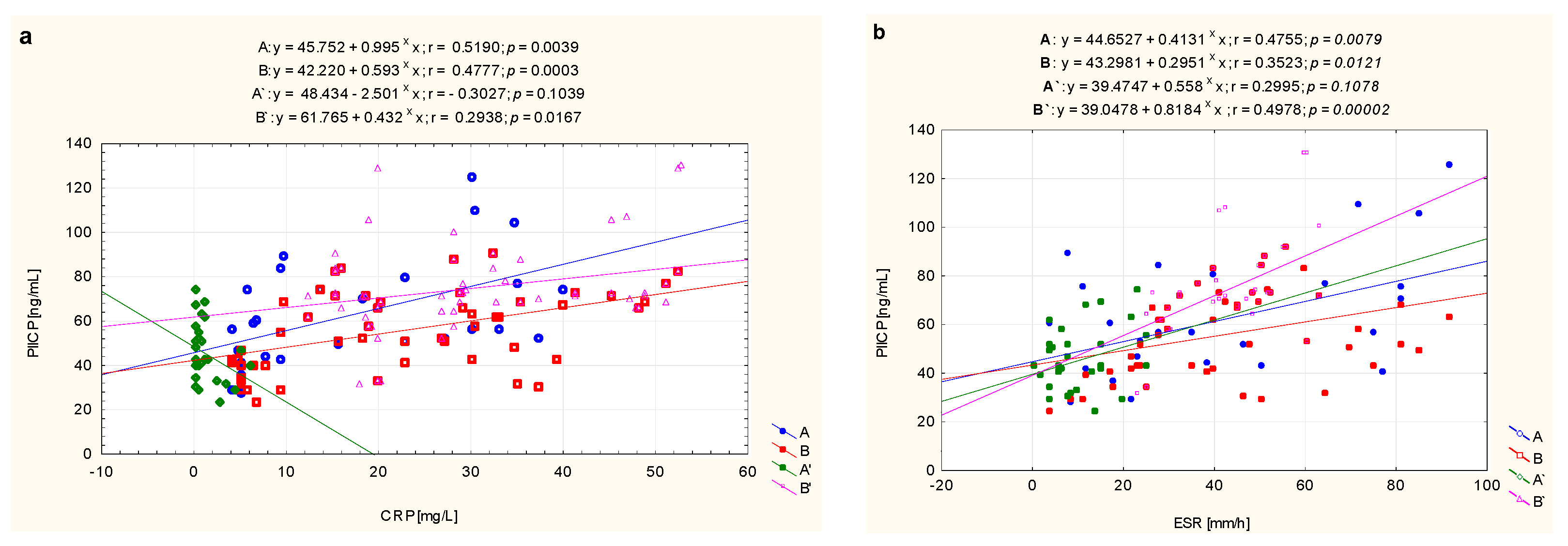
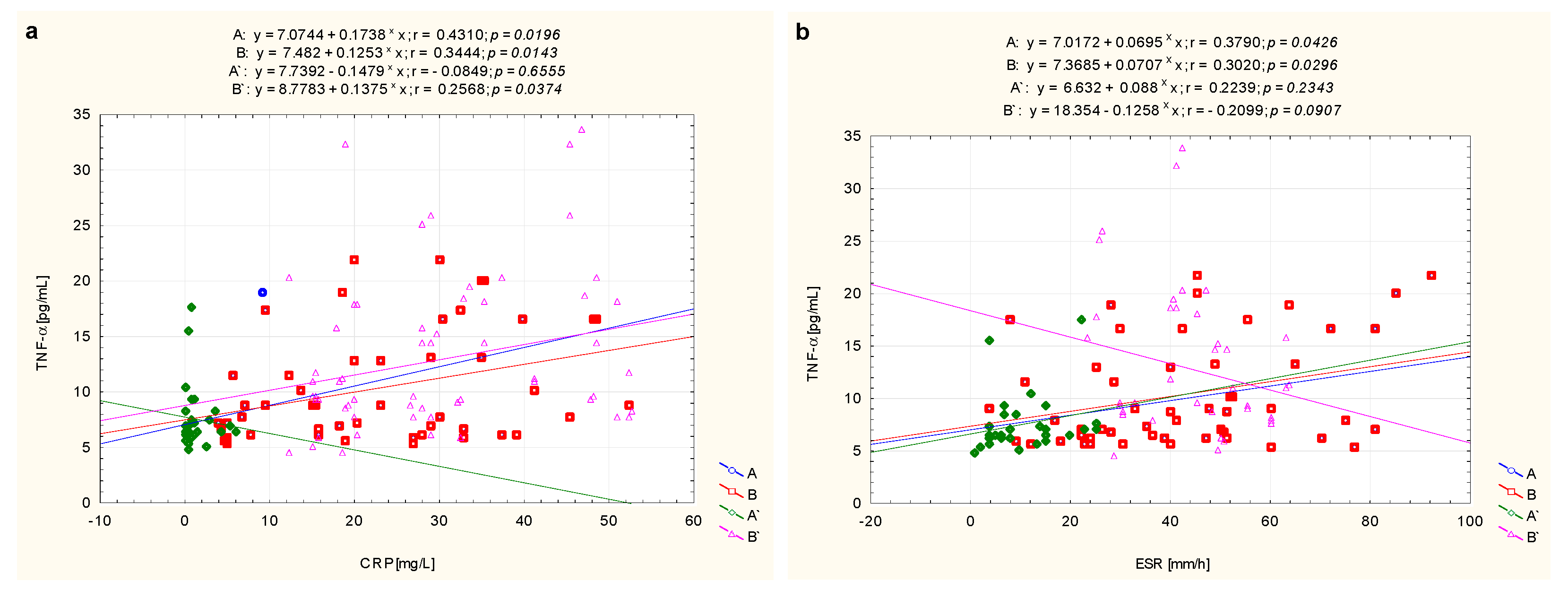
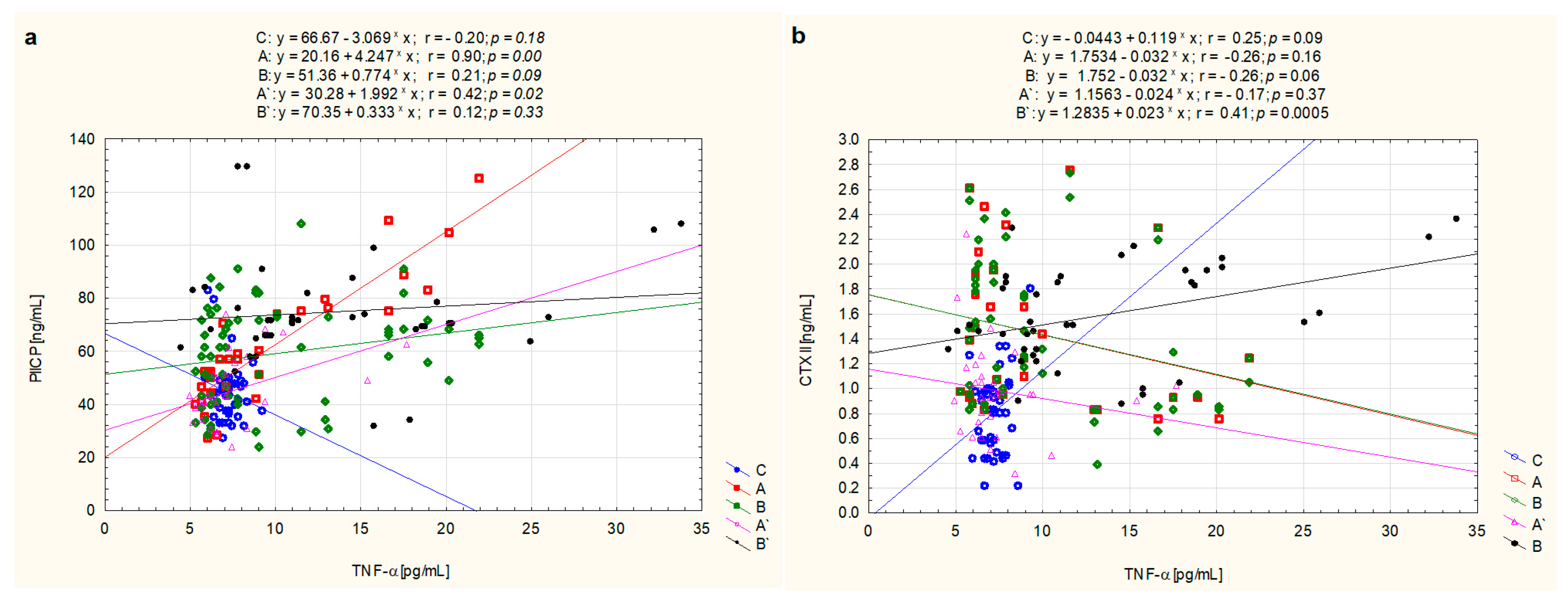
3.4. The Correlations between Markers of Metabolic Changes of Cartilage and TNF-α
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martini, A.; Ravelli, A.; Avcin, T.; Beresford, M.W.; Burgos-Vargas, R.; Cuttica, R.; Ilowite, R.T.; Khubchandani, R.; Laxer, R.M.; Lovell, D.J.; et al. Pediatric Rheumatology International Trials Organization (PRINTO). Toward new classification criteria for juvenile idiopathic arthritis: First steps, Pediatric Rheumatology International Trials Organization International Consensus. J. Rheumatol. 2019, 46, 190–197. [Google Scholar] [CrossRef]
- Ravelli, A.; Consolaro, A.; Horneff, G.; Laxer, R.M.; Lovell, D.J.; Wulffraat, N.M.; Akikusa, J.D.; Al-Mayouf, S.M.; Antón, J.; Avcin, T.; et al. Treating juvenile idiopathic arthritis to target: Recommendations of an international task force. Ann. Rheum. Dis. 2018, 77, 819–828. [Google Scholar] [CrossRef]
- Barut, K.; Adrovic, A.; Şahin, S.; Kasapçopur, Ö. Juvenile idiopathic arthritis. Balk. Med. J. 2017, 34, 90–101. [Google Scholar] [CrossRef]
- Shevchenko, N.; Panko, N.; Rakovska, L.; Holovko, T.O. Connective tissue metabolism in patients with juvenile idiopathic arthritis: 10-year follow-up study. Pediatrics 2019, 6, 5–11. [Google Scholar]
- Mitra, S.; Samui, P.P.; Samanta, M.; Mondal, R.K.; Hazra, A.; Mandal, K.; Sabui, T.K. Ultrasound detected changes in joint cartilage thickness in juvenile idiopathic arthritis. Int. J. Rheum. Dis. 2019, 22, 1263–1270. [Google Scholar] [CrossRef]
- Lewander, P.; Dahle, C.; Larsson, B.; Wetterö, J.; Skogh, T. Circulating cartilage oligomeric matrix protein in juvenile idiopathic arthritis. Scand. J. Rheumatol. 2017, 46, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Theocharis, A.D.; Manou, D.; Karamanos, N.K. The extracellular matrix as a multitasking player in disease. FEBS J. 2019, 286, 2830–2869. [Google Scholar] [CrossRef]
- Luo, Y.; Sinkeviciute, D.; He, Y.; Karsdal, M.; Henrotin, Y.; Mobasheri, A.; Önnerfjord, P.; Bay-Jensen, A. The minor collagens in articular cartilage. Protein Cell 2017, 8, 560–572. [Google Scholar] [CrossRef]
- Karsdal, M.A.; Nielsen, M.J.; Sand, J.M.; Henriksen, K.; Genovese, F.; BayJensen, A.C.; Smith, V.; Adamkewicz, J.I.; Christiansen, C.; Leeming, D.J. Extracellular matrix remodeling: The common denominator in connective tissue diseases. Possibilities for evaluation and current understanding of the matrix as more than a passive architecture, but a key player in tissue failure. ASSAY Drug Dev. Technol. 2013, 11, 70–92. [Google Scholar] [CrossRef]
- Winsz-Szczotka, K.; Mencner, Ł.; Olczyk, K. Metabolism of glycosaminoglycans in the course of juvenile idiopathic arthritis. Postep. Hig. Med. Dosw. 2016, 70, 135–142. [Google Scholar] [CrossRef]
- Elsaid, K.A.; Chichester, C.O. Collagen markers in early arthritic diseases. Clin. Chim. Acta 2006, 365, 68–77. [Google Scholar] [CrossRef]
- Löfvall, H.; Katri, A.; Dąbrowska, A.; Karsdal, M.A.; Luo, Y.; He, Y.; Manon-Jensen, T.; Dziegiel, M.H.; Bay-Jensen, A.C.; Thudium, C.S.; et al. GPDPLQ(1237)-a type II collagen neo-epitope biomarker of osteoclast- and inflammation-derived cartilage degradation in vitro. Sci. Rep. 2019, 28, 3050. [Google Scholar] [CrossRef]
- Luo, Y.; He, Y.; Reker, D.; Gudmann, N.S.; Henriksen, K.; Simonsen, O.; Ladel, C.; Michaelis, M.; Mobasheri, A.; Karsdal, M.; et al. A novel high sensitivity type II collagen blood-based biomarker, PRO-C2, for assessment of cartilage formation. Int. J. Mol. Sci. 2018, 19, 3485. [Google Scholar] [CrossRef] [PubMed]
- Kaminiarczyk-Pyzalka, D.; Adamczak, K.; Mikos, H.; Klimecka, I.; Moczko, J.; Niedziela, M. Serum TNF-α levels and indicators of disease activity in children with oligoarticular juvenile idiopathic arthritis (oJIA) in the first year of the disease. Clin. Lab. 2014, 60, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.M.; et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar] [PubMed]
- Winsz-Szczotka, K.; Kuźnik-Trocha, K.; Gruenpeter, A.; Wojdas, M.; Dąbkowska, K.; Olczyk, K. Association of circulating COMP and YKL-40 as markers of metabolic changes of cartilage with adipocytokines in juvenile idiopathic arthritis. Metabolites 2020, 10, 61. [Google Scholar] [CrossRef]
- Karsdal, M.A.; Genovese, F.; Madsen, E.A.; Manon-Jensen, T.; Schuppan, D. Collagen and tissue turnover as a function of age: Implications for fibrosis. J. Hepatol. 2016, 64, 103–109. [Google Scholar] [CrossRef]
- Briot, K.; Roux, C.; Gossec, L.; Charni, N.; Kolta, S.; Dougados, M.; Garnero, P. Effects of etanercept on serum biochemical markers of cartilage metabolism in patients with spondyloarthropathy. J. Rheumatol. 2008, 35, 310–314. [Google Scholar]
- Kopec-Medrek, M.; Kucharz, E.J. Fibulin-3 and other cartilage metabolism biomarkers in relationship to calprotectin (MRP8/14) and disease activity in rheumatoid arthritis patients treated with anti-TNF therapy. Adv. Clin. Exp. Med. 2018, 27, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, S.; Itokazu, M.; Suzuki, Y.; Shimizu, K. Procollagen II C propeptide level in the synovial fluid as a predictor of radiographic progression in early knee osteoarthritis. Ann. Rheum. Dis. 2003, 62, 27–32. [Google Scholar] [CrossRef]
- Tomonaga, A.; Watanabe, K.; Fukagawa, M.; Suzuki, A.; Kurokawa, M.; Nagaoka, I. Evaluation of the effect of N-acetyl-glucosamine administration on biomarkers for cartilage metabolism in healthy individuals without symptoms of arthritis: A randomized double-blind placebo-controlled clinical study. Exp. Ther. Med. 2016, 12, 1481–1489. [Google Scholar] [CrossRef][Green Version]
- Fraser, A.; Fearon, U.; Billinghurst, R.C.; Ionescu, M.; Reece, R.; Barwick, T.; Emery, P.; Poole, A.R.; Veale, D.J. Turnover of type II collagen and aggrecan in cartilage matrix at the onset of inflammatory arthritis in humans: Relationship to mediators of systemic and local inflammation. Arthritis Rheumatol. 2003, 48, 3085–3095. [Google Scholar] [CrossRef] [PubMed]
- Månsson, B.; Carey, D.; Alini, M.; Ionescu, M.; Rosenberg, L.C.; Poole, A.R.; Heinegård, D.; Saxne, T. Cartilage and bone metabolism in rheumatoid arthritis. Differences between rapid and slow progression of diseaseidentified by serum markers of cartilage metabolism. J. Clin. Investig. 1995, 95, 1071–1077. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Yoshihara, Y.; Roos, H.; Kobayashi, T.; Yamada, H.; Shinmei, M. Procollagen II C-propeptide in joint fluid: Changes in concentration with age, time after knee injury, and osteoarthritis. J. Rheumatol. 1996, 23, 1765–1769. [Google Scholar]
- Poole, A.R.; Kobayashi, M.; Yasuda, T.; Laverty, S.; Mwale, F.; Kojima, T.; Sakai, T.; Wahl, C.; El-Maadawy, S.; Webb, G.; et al. Type II collagen degradation and its regulation in articular cartilage in osteoarthritis. Ann. Rheum. Dis. 2002, 61, ii78–ii81. [Google Scholar] [CrossRef]
- Peake, N.J.; Foster, H.E.; Khawaja, K.; Cawston, T.E.; Rowan, A.D. Assessment of the clinical significance of gelatinase activity in patients with juvenile idiopathic arthritis using quantitative protein substrate zymography. Ann. Rheum. Dis. 2006, 65, 501–507. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Huebner, J.L.; Haaland, B.; Wong, S.B.S.; Kraus, V.B. Synovial fluid pro-inflammatory profile differs according to the characteristics of knee pain. Osteoarthr. Cartil. 2017, 25, 1420–1427. [Google Scholar] [CrossRef]
- Roux, C.H.; Foltz, V.; Maheu, E.; Baron, G.; Gandjbakhch, F.; Lukas, C.; Wendling, D.; Loeuille, D.; Lafforgue, P.; Euler-Ziegler, L.; et al. French Section on Osteoarthritis. MRI and serum biomarkers correlate with radiographic features in painful hand osteoarthritis. Clin. Exp. Rheumatol. 2016, 34, 991–998. [Google Scholar]
- Catterall, J.B.; Stabler, T.V.; Flannery, C.R.; Kraus, V.B. Changes in serum and synovial fluid biomarkers after acute injury (NCT00332254). Arthritis Res. Ther. 2010, 12, R229. [Google Scholar] [CrossRef]
- Klocke, R.; Levasseur, K.; Kitas, G.D.; Smith, J.P.; Hirsch, G. Cartilage turnover and intra-articular corticosteroid injections in knee osteoarthritis. Rheumatol. Int. 2018, 38, 455–459. [Google Scholar] [CrossRef]
- Saberi Hosnijeh, F.; Siebuhr, A.S.; Uitterlinden, A.G.; Oei, E.H.; Hofman, A.; Karsdal, M.A.; Bierma-Zeinstra, S.M.; Bay-Jensen, A.C.; van Meurs, J.B. Association between biomarkers of tissue inflammation and progression of osteoarthritis: Evidence from the Rotterdam study cohort. Arthritis Res. Ther. 2016, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Struglics, A.; Saleh, R.; Sundberg, E.; Olsson, M.; Harris, H.E.; Aulin, C. Juvenile idiopathic arthritis patients have a distinct cartilage and bone biomarker profile that differs from healthy and knee-injured children. Clin. Exp. Rheumatol. 2020, 38, 355–365. [Google Scholar]
- Świdrowska-Jaros, J.; Orczyk, K.; Smolewska, E. Macrophages-silent enemies in juvenile idiopathic arthritis. Postep. Hig. Med. Dosw. 2016, 70, 743–750. [Google Scholar] [CrossRef]
- Funk, R.S.; Chan, M.A.; Becker, M.L. Cytokine biomarkers of disease activity and therapeutic response after initiating methotrexate therapy in patients with juvenile idiopathic arthritis. Pharmacotherapy 2017, 37, 700–711. [Google Scholar] [CrossRef]
- Honorati, M.C.; Neri, S.; Cattini, L.; Facchini, A. Interleukin-17, a regulator of angiogenic factor release by synovial fibroblasts. Osteoarthr. Cartil. 2006, 14, 345–352. [Google Scholar] [CrossRef]
- Yamane, K.; Ihn, H.; Asano, Y.; Jinnin, M.; Tamaki, K. Antagonistic effects of TNF-alpha on TGF-beta signaling through down-regulation of TGF-beta receptor type II in human dermal fibroblasts. J. Immunol. 2003, 171, 3855–3862. [Google Scholar] [CrossRef]
- Grounds, M.D.; Radley, H.G.; Gebski, B.L.; Bogoyevitch, M.A.; Shavlakadze, T. Implications of cross-talk between tumour necrosis factor and insulin-like growth factor-1 signalling in skeletal muscle. Clin. Exp. Pharm. Physiol. 2008, 35, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Winsz-Szczotka, K.; Komosińska-Vassev, K.; Kuźnik-Trocha, K.; Siwiec, A.; Żegleń, B.; Olczyk, K. Circulating keratan sulfate as a marker of metabolic changes of cartilage proteoglycan in juvenile idiopathic arthritis; influence of growth factors as well as proteolytic and prooxidative agents on aggrecan alterations. Clin. Chem. Lab. Med. 2015, 53, 291–297. [Google Scholar] [CrossRef]
- Vignola, S.; Picco, P.; Falcini, F.; Sabatini, F.; Buoncompagni, A.; Gattorno, M. Serum and synovial fluid concentration of vascular endothelial growth factor in juvenile idiopathic arthritides. Rheumatology 2002, 41, 691–696. [Google Scholar] [CrossRef]
- Lundell, A.C.; Erlandsson, M.; Bokarewa, M.; Liivamägi, H.; Uibo, K.; Tarraste, S.; Rebane, T.; Talvik, T.; Pruunsild, C.; Pullerits, R. Low serum IGF-1 in boys with recent onset of juvenile idiopathic arthritis. J. Immunol. Res. 2018, 2018, 3856897. [Google Scholar] [CrossRef]
- Guszczyn, T.; Rzeczycka, J.; Popko, J. IGF-I and IGF-binding proteins in articular exudates of children with post-traumatic knee damage and juvenile idiopathic arthritis. Pathobiology 2009, 76, 260–266. [Google Scholar] [CrossRef]
- Troeberg, L.; Nagase, H. Proteases involved in cartilage matrix degradation in osteoarthritis. Biochim. Biophys. Acta 2012, 1824, 133–145. [Google Scholar] [CrossRef]
- Araki, Y.; Mimura, T. Matrix metalloproteinase gene activation resulting from disordred epigenetic mechanisms in rheumatoid arthritis. Int. J. Mol. Sci. 2017, 18, 905. [Google Scholar] [CrossRef]
- Cui, N.; Hu, M.; Khalil, R.A. Biochemical and biological attributes of matrix metalloproteinases. Prog. Mol. Biol. Transl. Sci. 2017, 147, 1–73. [Google Scholar] [CrossRef]
- Van Doren, S.R. Matrix metalloproteinase interactions with collagen and elastin. Matrix Biol. 2015, 44–46, 224–231. [Google Scholar] [CrossRef]
- Fields, G.B. Interstitial collagen catabolism. J. Biol. Chem. 2013, 288, 8785–8793. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, V.; Myles, A.; Dayal, R.; Aggarwal, A. Levels of serum matrix metalloproteinase-3 correlate with disease activity in the enthesitis-related arthritis category of juvenile idiopathic arthritis. J. Rheumatol. 2011, 38, 2482–2487. [Google Scholar] [CrossRef]
- Kobus, A.; Bagińska, J.; Łapińska-Antończuk, J.; Ławicki, S.; Kierklo, A. Levels of selected matrix metalloproteinases, their inhibitors in saliva, and oral status in juvenile idiopathic arthritis patients vs. healthy controls. BioMed. Res. Int. 2019, 2019, 7420345. [Google Scholar] [CrossRef]
- Kaĭlina, A.N.; Ogorodova, L.M.; Chasovskikh, I.; Kremer, E.E. Indices of matrix metalloproteinases (MMP-2, MMP-9, TIMP-1) with juvenile arthritis in children. Annals Russ. Acad. Med. Sci. 2013, 7, 36–40. [Google Scholar] [CrossRef][Green Version]
- Winsz-Szczotka, K.; Komosińska-Vassev, K.; Kuźnik-Trocha, K.; Gruenpeter, A.; Lachór-Motyka, I.; Olczyk, K. Influence of proteolytic-antiproteolytic enzymes and prooxidative-antioxidative factors on proteoglycan alterations in children with juvenile idiopathic arthritis. Clin. Biochem. 2014, 47, 829–834. [Google Scholar] [CrossRef]
- Feng, C.; Yang, M.; Lan, M.; Liu, C.; Zhang, Y.; Huang, B.; Liu, H.; Zhou, Y. ROS: Crucial intermediators in the pathogenesis of intervertebral disc degeneration. Oxid. Med. Cell. Longev. 2017, 2017, 5601593. [Google Scholar] [CrossRef] [PubMed]
- Araujo, G.R.; Fonseca, J.E.; Fujimura, P.T.; Cunha-Junior, J.P.; Silva, C.H.; Mourão, A.F.; Canhão, H.; Goulart, L.R.; Gonçalves, J.; Ueira-Vieira, C. Anti-type II collagen antibodies detection and avidity in patients with oligoarticular and polyarticular forms of juvenile idiopathic arthritis. Immunol. Lett. 2015, 165, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Berntson, L.; Nordal, E.; Fasth, A.; Aalto, K.; Herlin, T.; Nielsen, S.; Rygg, M.; Zak, M.; Rönnelid, J. Anti-type II collagen antibodies, anti-CCP, IgA RF and IgM RF are associated with joint damage, assessed eight years after onset of juvenile idiopathic arthritis (JIA). Pediatr. Rheumatol. 2014, 12, 1–7. [Google Scholar] [CrossRef]
- Resnick, C.M.; Vakilian, P.M.; Breen, M.; Zurakowski, D.; Caruso, P.; Henderson, L.; Nigrovic, P.A.; Kaban, L.B.; Peacock, Z.S. Quantifying temporomandibular joint synovitis in children with juvenile idiopathic arthritis. Arthritis Care Res. 2016, 68, 1795–1802. [Google Scholar] [CrossRef]
- Sambataro, S.; Cervino, G.; Bocchieri, S.; La Bruna, R.; Cicciù, M. TMJ dysfunctions systemic implications and postural assessments: A review of recent literature. J. Funct. Morphol. Kinesiol. 2019, 4, 58. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control Subjects (n = 45) | JIA Patients before Treatment (n = 96) | JIA Patients after Treatment | |
|---|---|---|---|---|
| Inactive Disease (n = 30) | Active Disease (n = 66) | |||
| Age (years) | 8.25 ± 2.03 | 8.23 ± 3.48 | 8.71 ± 3.70 | 7.95 ± 2.51 |
| Sex, female/male | 34/11 | 77/19 | 19/11 | 58/8 |
| JADAS-27 | - | 18 ± 8.66 | 4 ± 2.48 b | 15 ± 4.57 |
| BMI (kg/m2) | 18.34 ± 2.12 | 16.18 ± 2.14 a | 18.02 ± 3.55 b | 16.67 ± 3.12 a |
| WBC (103/µL) | 7.85 ± 2.34 | 14.66 ± 4.59 a | 6.45 ± 2.70 | 9.72 ± 2.18 b |
| RBC (106/µL) | 4.75 ± 0.32 | 4.26 ± 0.42 | 4.62 ± 0.36 | 4.02 ± 0.33 a |
| Hb (g/dL) | 14.08 ± 0.74 | 11.25 ± 1.78 a | 12.94 ± 1.53 a,b | 12,02 ± 1.27 a,b |
| Ht (%) | 40.68 ± 3.26 | 35.67 ± 3.52 a | 37.22 ± 7.51 a,b | 37.19 ± 3.57 a,b |
| PLT (103/µL) | 284.42 ± 68.22 | 398.26 ± 111.87 a | 359.26 ± 80.06 b | 344.32 ± 70.15 |
| Total cholesterol (mM/L) | 4.32 ± 0.84 | 4.69 ± 1.39 a | 4.27 ± 1.55 b | 4.48 ± 0.69 |
| Glucose (mM/L) | 4.21 ± 0.38 | 4.18 ± 1.26 | 4.44 ± 0.56 b | 4.51 ± 0.93 b |
| Creatinine (µM/L) | 61.42 ± 12.45 | 77.58 ± 9.21 a | 64.35 ± 14.57 a,b | 82.58 ± 1.11 a,b |
| CRP (mg/L) | 1.20 ± 1.39 | 19.66 ± 21.68 a | 3.57 ± 0.62 b | 12.47 ± 16.88 a,c |
| ESR (mm/h) | 9.22 ± 7.41 | 41.66 ± 22.04 a | 12.01 ± 5.15 b | 24.95 ± 15.89 a,c |
| ANA | - | 57% (positive) | 57% (positive) | 57% (positive) |
| RF | - | 100% (negative) | 100%(negative) | 100% (negative) |
| Parameter | Control Subjects (n = 45) | JIA Patients before Treatment | JIA Patients after Treatment | ||
|---|---|---|---|---|---|
| A (n = 30) | B (n = 66) | A’ (Inactive Disease) (n = 30) | B’ (Active Disease) (n = 66) | ||
| PIICP (ng/mL) | 44.62 ± 10.66 | 62.00 ± 23.48 a | 59.18 ± 18.71 b | 45.33 ± 13.10 e | 74.64 ± 18.81 a,f,i |
| CTX II (ng/mL) | 0.81 ± 0.21 | 1.43 ± 0.75 c | 1.42 ± 0.59 c | 0.98 ± 0.32 d,g | 1.58 ± 0.67 c,i |
| TNF-α (pg/mL) | 7.19 ± 0.71 | 9.85 ± 4.96 d | 10.11 ± 5.02 d | 7.56 ± 2.76 e | 12.88 ± 6.86 c,h,j |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winsz-Szczotka, K.; Kuźnik-Trocha, K.; Lachór-Motyka, I.; Lemski, W.; Olczyk, K. Concerted Actions by PIICP, CTXII, and TNF-α in Patients with Juvenile Idiopathic Arthritis. Biomolecules 2021, 11, 648. https://doi.org/10.3390/biom11050648
Winsz-Szczotka K, Kuźnik-Trocha K, Lachór-Motyka I, Lemski W, Olczyk K. Concerted Actions by PIICP, CTXII, and TNF-α in Patients with Juvenile Idiopathic Arthritis. Biomolecules. 2021; 11(5):648. https://doi.org/10.3390/biom11050648
Chicago/Turabian StyleWinsz-Szczotka, Katarzyna, Kornelia Kuźnik-Trocha, Iwona Lachór-Motyka, Wojciech Lemski, and Krystyna Olczyk. 2021. "Concerted Actions by PIICP, CTXII, and TNF-α in Patients with Juvenile Idiopathic Arthritis" Biomolecules 11, no. 5: 648. https://doi.org/10.3390/biom11050648
APA StyleWinsz-Szczotka, K., Kuźnik-Trocha, K., Lachór-Motyka, I., Lemski, W., & Olczyk, K. (2021). Concerted Actions by PIICP, CTXII, and TNF-α in Patients with Juvenile Idiopathic Arthritis. Biomolecules, 11(5), 648. https://doi.org/10.3390/biom11050648