
Development of Standardized Fetal Progenitor Cell Therapy for Cartilage Regenerative Medicine: Industrial Transposition and Preliminary Safety in Xenogeneic Transplantation


 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
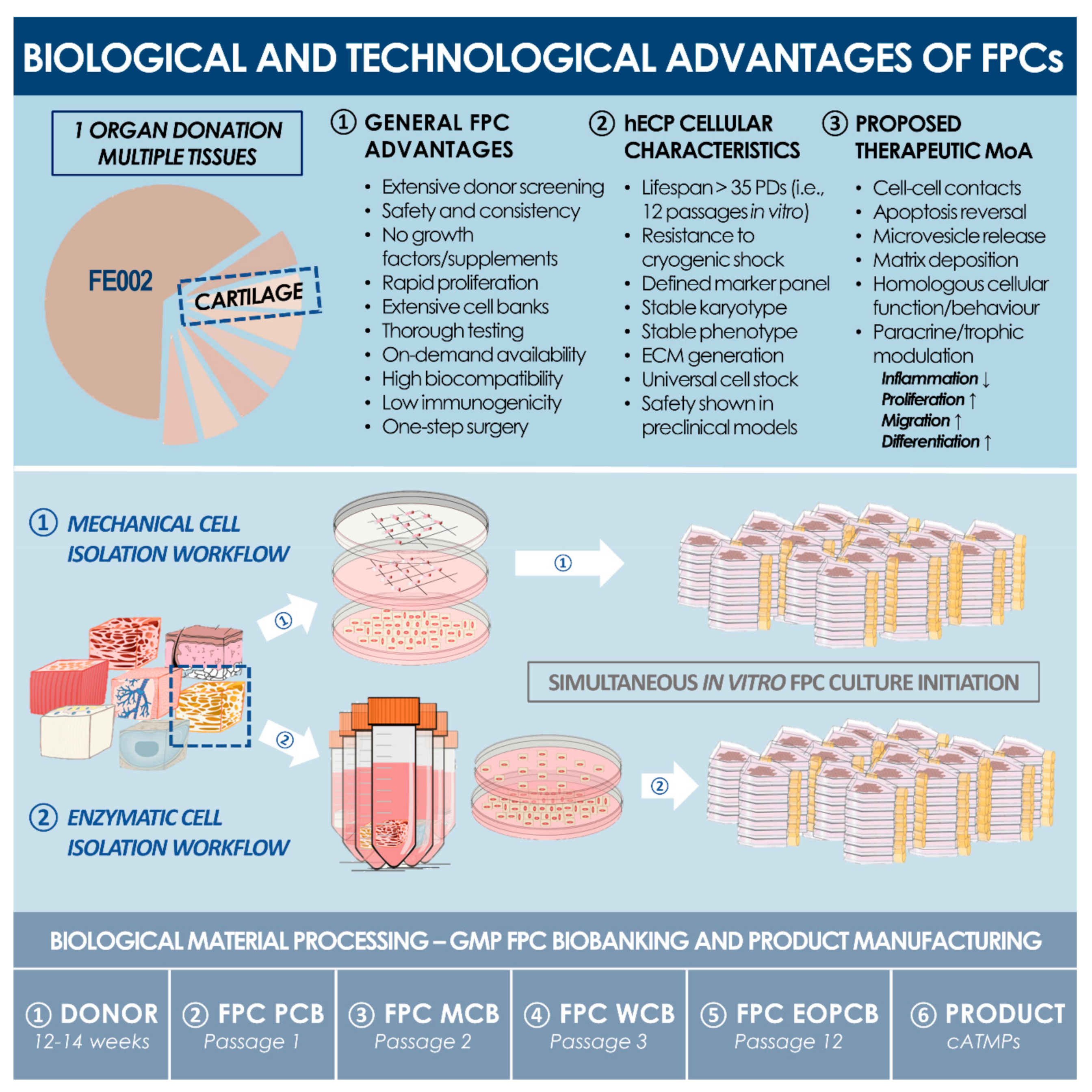
2.1. Primary hECP Isolation, Cell Banking, and Characterization
2.1.1. Fetal Tissue Donation and Procurement
2.1.2. Primary hECP Enzymatic Isolation and PCB Establishment
2.1.3. Pilot hECP Expansion and Cell Banking Campaign
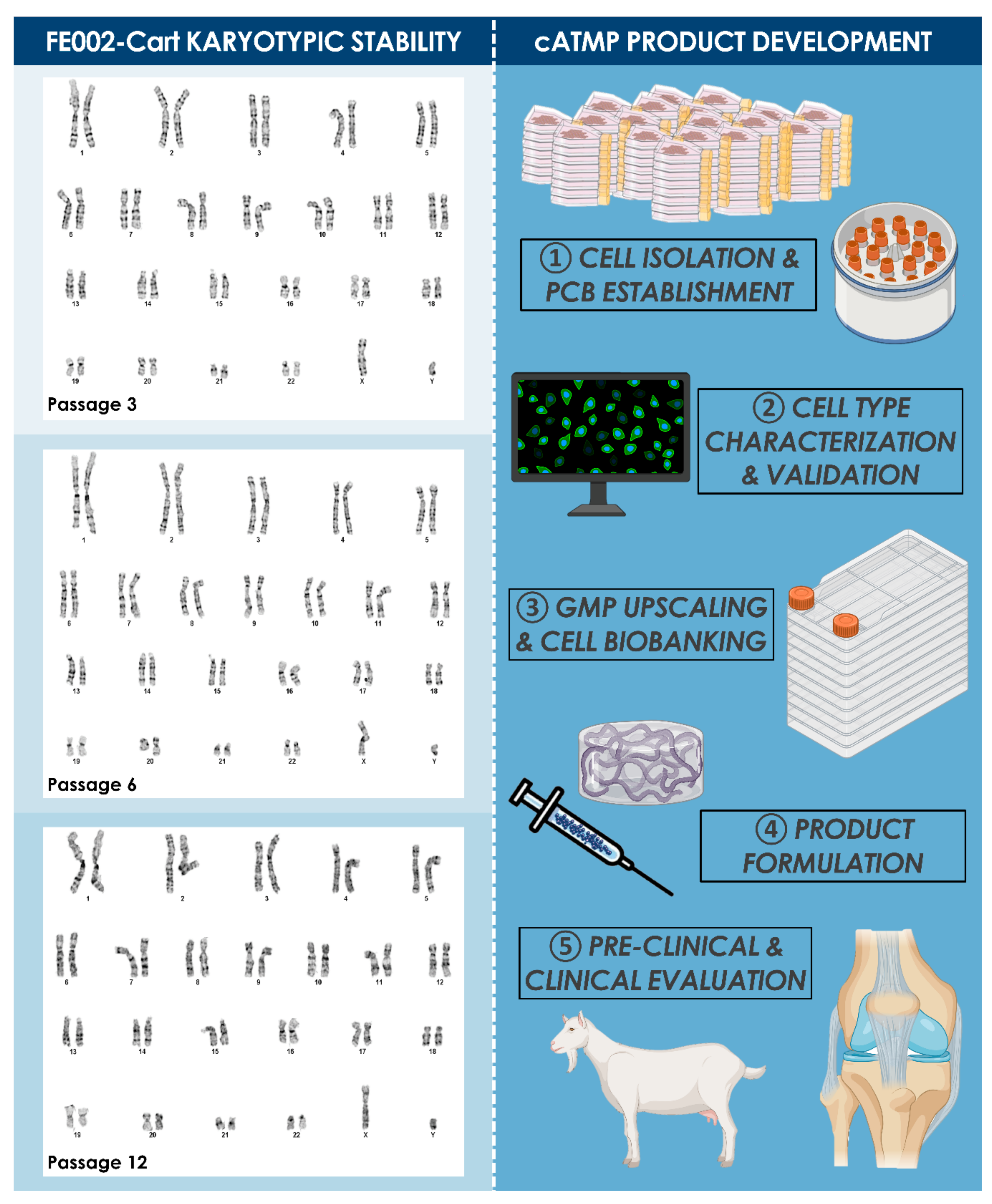
2.1.4. Preliminary Characterization of the Enzymatically Isolated FE002-Cart Cell Type
2.1.5. Optimized Multi-Tiered hECP Biobanking Workflow
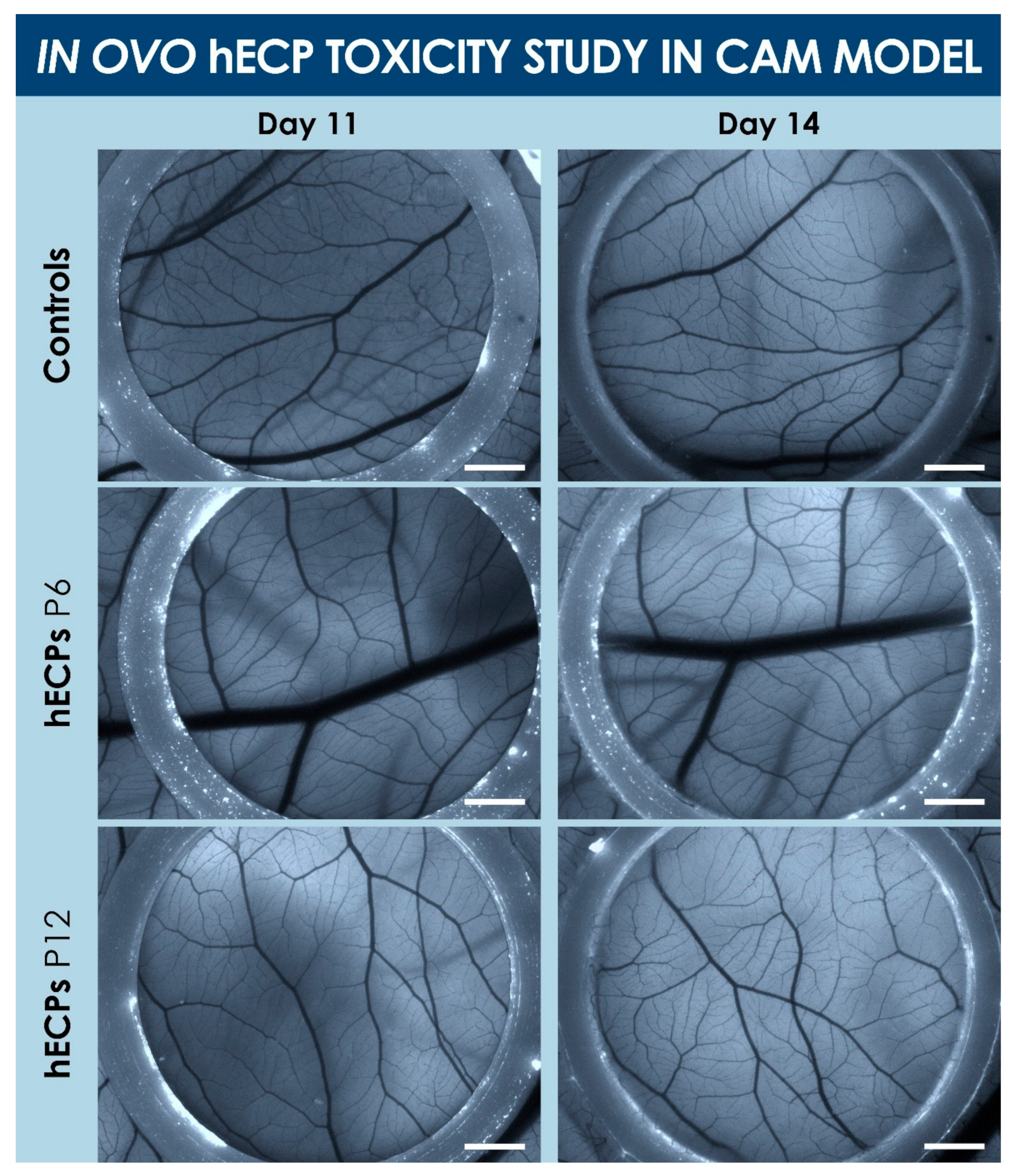
2.2. Preclinical Safety Study of FE002-Cart FPCs in a CAM Model
Study Design
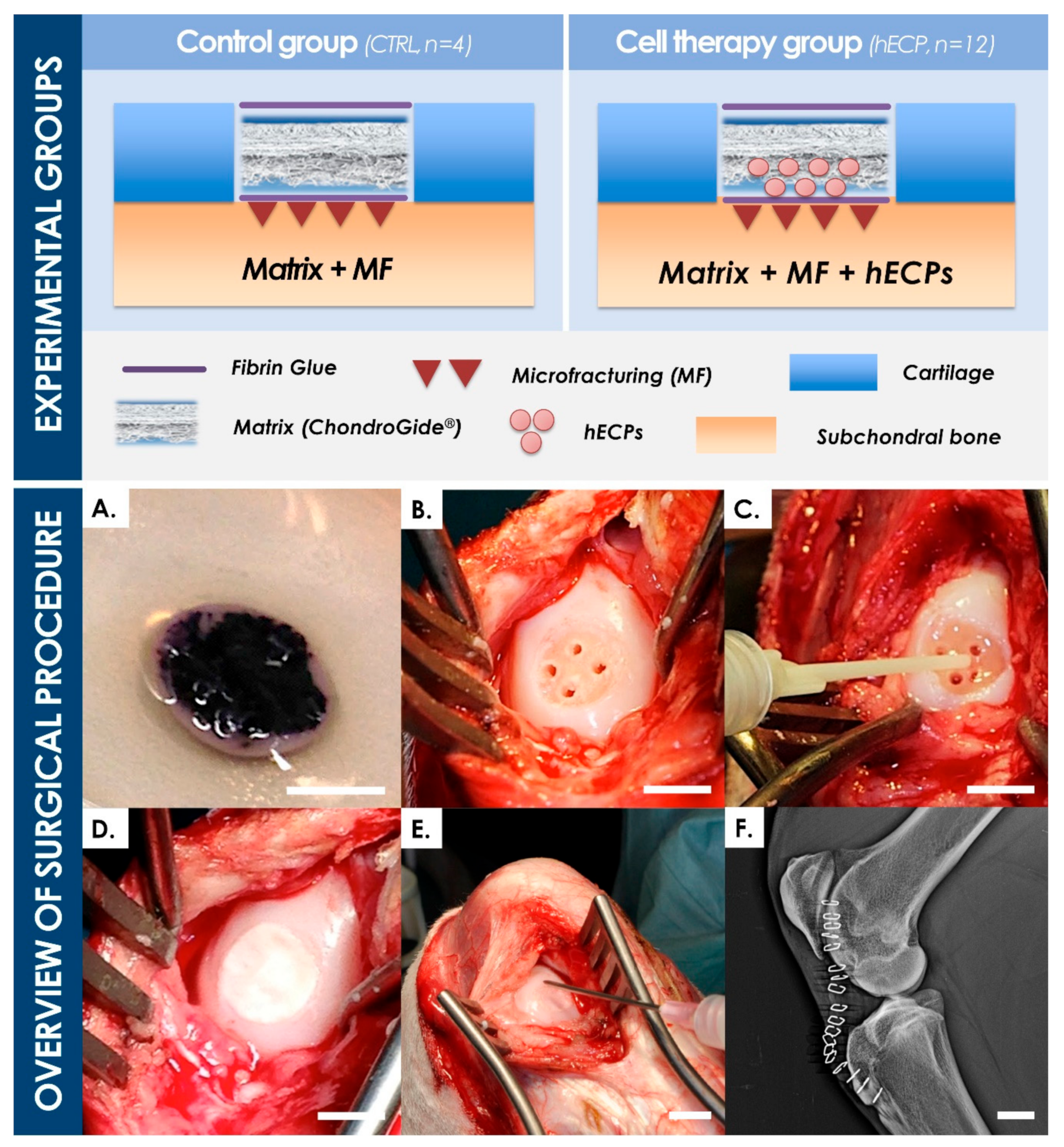
2.3. Preclinical Safety Study in a Caprine Model
2.3.1. Study Norms and Authorizations
2.3.2. Animal Study Design
2.3.3. Cell-Laden Implant Preparation and Viability Control
2.3.4. Animal Sedation and Anesthesia
2.3.5. Surgical Technique
2.3.6. Post-Operative Treatment and Prophylaxis
2.3.7. In-Life Monitoring, Sacrifice, and Tissue Processing
2.3.8. Stifle Imaging and Analysis
2.3.9. Macroscopic Assessment of Condyles, Histological Processing, and Scoring
2.3.10. Synovial Tissue Processing and Evaluation
2.3.11. Statistical Analysis
3. Results
3.1. hECP Isolation and Multi-Tiered Cell Banking
3.2. Safety of hECPs in the CAM Model
3.3. Safety of hECPs in the Caprine Cartilage Defect Model
3.3.1. General Observations
3.3.2. Implant Preparation and Surgical Procedure
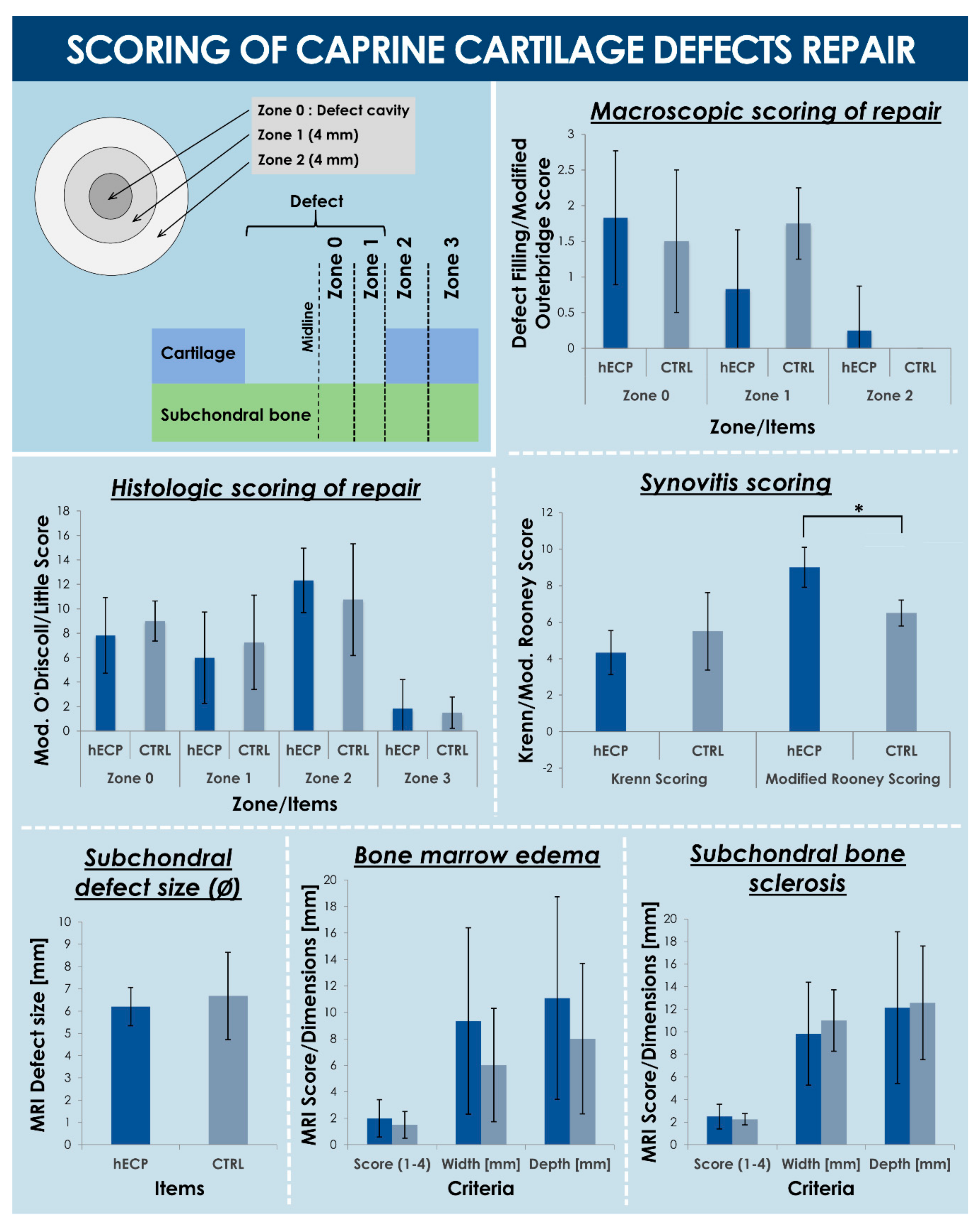
3.3.3. Macroscopic Observations and Scoring of Cartilage Repair
3.3.4. MRI Findings and Scoring
3.3.5. Histological Observations
3.3.6. Synovial Membrane Analysis and Synovitis Scoring
3.3.7. hECP Cell Tracking
4. Discussion
4.1. Unsatisfactory Surgical State of the Art for Cartilage Repair
4.2. Limited Available Cell Therapies for Cartilage Regeneration
4.3. Cultured hECPs as Optimal Candidates for Cell-Based Cartilage Repair
4.4. Tiered hECP Banking for Safe and Sustainable Cartilage Cell Therapies
4.5. FE002-Cart hECPs as Safe Cell Sources for Musculoskeletal Tissue Engineering
4.6. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description—Defect Filling Score Scale (Zones 0 1 and 1 2) | Grade |
| Totally filled | 0 |
| Peripheral and central filling. No MF drill holes visible | 1 |
| Peripheral filling. Very thin transparent filling. Visible drill holes | 2 |
| Peripheral filling and/or blood-tinged | 3 |
| No filling | 4 |
| Description—Modified Outerbridge Score Scale (Zones 2 3 and 3 4) | Grade |
| Normal cartilage appearance (hyaline, flat, smooth on the surface) | 0 |
| Cobblestone appearance, soft, swollen cartilage | 1 |
| Fissures visible in cartilage | 2 |
| Description—Cellular Morphology | Grade |
|---|---|
| Hyaline articular cartilage | 0 |
| Incompletely differentiated mesenchyme | 1 |
| Fibrous tissue | 2 |
| Bone | 3 |
| Description—Safranin-O Staining of the Matrix | Grade |
| Normal | 0 |
| Moderate | 1 |
| Slight | 2 |
| None | 3 |
| Description—Surface coverage | Grade |
| Smooth and intact (100% coverage) | 0 |
| 75–50% coverage | 1 |
| 50–25% coverage | 2 |
| Severe disruption (<25% coverage) | 3 |
| Description—Thickness | Grade |
| 75–100% of normal adjacent cartilage | 0 |
| 50–75% of normal adjacent cartilage | 1 |
| 25–50% of normal adjacent cartilage | 2 |
| 0–25% of normal adjacent cartilage | 3 |
| Description—Bonding of new tissue to adjacent cartilage (Zone 1) | Grade |
| Bonded at both ends | 0 |
| Bonded at one end, or partially at both ends | 1 |
| Not bonded | 2 |
| Description—Hypocellularity of hyaline-like tissue | Grade |
| Non-hyaline | N/A |
| Normal cellularity | 0 |
| Slight hypocellularity or slight hypercellularity | 1 |
| Moderate hypocellularity | 2 |
| Severe hypocellularity | 3 |
| Description—Chondrocyte clustering | Grade |
| Non-hyaline tissue and cells | N/A |
| No chondrocyte clusters | 0 |
| <25% of the cells | 1 |
| 25–100% of the cells | 2 |
| Description—Structure | Grade |
|---|---|
| Normal | 0 |
| Slight surface irregularities | 1 |
| Moderate surface irregularities | 2 |
| Severe surface irregularities | 3 |
| Clefts into transitional zone (1/3 depth) | 4 |
| Clefts into radial zone (2/3 depth) | 5 |
| Clefts into calcified zone (full depth) | 6 |
| Fibrillation and/or loss to transitional zone (1/3 depth) | 7 |
| Fibrillation and/or loss to radial zone (2/3 depth) | 8 |
| Fibrillation and/or loss to calcified zone (full depth) | 9 |
| Fibrillation and/or loss to subchondral bone | 10 |
| Description—Cellularity | Grade |
| Normal | 0 |
| Increase or slight decrease | 1 |
| Moderate decrease | 2 |
| Severe decrease | 3 |
| No cells | 4 |
| Description—Cell cloning | Grade |
| Normal | 0 |
| Several doublets | 1 |
| Many doublets | 2 |
| Doublets and triplets | 3 |
| Multiple cell nests | 4 |
| Description—Territorial Toluidine Blue | Grade |
| Normal | 0 |
| Increase or slight decrease in staining | 1 |
| Moderate decrease | 2 |
| Severe decrease | 3 |
| No staining | 4 |
| Description—Interterritorial Toluidine Blue | Grade |
| Normal | 0 |
| Loss of staining in tangential zone (1/3 depth) | 1 |
| Loss of staining in transitional zone (2/3 depth) | 2 |
| Loss of staining in radial zone (full depth) | 3 |
| No staining | 4 |
| Description—Tidemark/Calcified cartilage/Subchondral bone | Grade |
| Intact subchondral bone plate and single tidemark | 0 |
| Intact subchondral bone plate and multilayered tidemark | 1 |
| Blood vessels through subchondral bone to calcified cartilage | 2 |
| Tidemark crossed by blood vessels | 3 |
| Description—Enlargement of Synovial Lining Cell Layer | Grade |
|---|---|
| Lining cells form 1 layer | 0 |
| Lining cells form 2–3 layers | 1 |
| Lining cells form 4–5 layers, with few multinucleated cells | 2 |
| Lining cells form more than 5 layers, with ulceration, multinucleated cells | 3 |
| Description—Density of Resident Cells | Grade |
| Synovial stroma shows normal cellularity | 0 |
| Cellularity slightly increased | 1 |
| Cellularity moderately increased, multinuclear cells might occur | 2 |
| Cellularity greatly increased, multinucleated giant cells, pannus, rheumatoid granulomas | 3 |
| Description—Inflammatory Infiltrate | Grade |
| No inflammatory infiltrate | 0 |
| Few, mostly perivascular situated lymphocytes or plasma cells | 1 |
| Numerous lymphocytes or plasma cells, sometimes forming follicle-like aggregates | 2 |
| Dense band-like inflammatory infiltrate or numerous large follicle-like aggregates | 3 |
| Description—Synovitis | Total |
| No synovitis | 0–1 |
| Low-grade synovitis | 2–4 |
| High-grade synovitis | 5–9 |
| Synoviocyte Hyperplasia: Predominant Cell Depth of Synovial Lining Layer | |
|---|---|
| Description | Grade |
| 1–2 | 0 |
| 3–4 | 1 |
| 5–6 | 2 |
| 7–8 | 3 |
| 9–10 | 4 |
| >10 | 5 |
| Fibrosis: Percentage of Fibrosis in Subsynovial Layer | |
| Description | Grade |
| <10 | 0 |
| 10–30 | 1 |
| 30–50 | 2 |
| 50–70 | 3 |
| 70–90 | 4 |
| >90 | 5 |
| Proliferating blood vessels: Number of Vessels Per High Power Field 1 | |
| Description | Grade |
| 0–3 | 0 |
| 4–8 | 1 |
| 9–13 | 2 |
| 14–18 | 3 |
| 18–22 | 4 |
| >22 | 5 |
| Perivascular Infiltrates of Lymphocytes: Percentage of Vessels Per High Power Field | |
| Description | Grade |
| <5 | 0 |
| 5–25 | 1 |
| 25–50 | 2 |
| 50–75 | 3 |
| 100 | 4 |
| Focal lymphocyte Aggregates: Number of Cells in Diameter | |
| Description | Grade |
| 10 | 0 |
| 20 | 1 |
| 30 | 2 |
| 40 | 3 |
| 50 | 4 |
| ≥55 | 5 |
| Diffuse Infiltrates of Lymphocytes: Percentage of Diffuse Lymphocytes Per High Power Field | |
| Description | Grade |
| 0 | 0 |
| 5–20 | 1 |
| 20–40 | 2 |
| 40–60 | 3 |
| 60–80 | 4 |
| 100 | 5 |
| Description | Grade |
|---|---|
| No finding | 0 |
| Mild | 1 |
| Moderate | 2 |
| Severe | 3 |
| Profound | 4 |
References
- Vacanti, J.P.; Langer, R. Tissue engineering: The design and fabrication of living replacement devices for surgical reconstruction and transplantation. Lancet 1999, 354, 32–34. [Google Scholar] [CrossRef]
- Marks, P.; Gottlieb, S. Balancing safety and innovation for cell-based regenerative medicine. N. Engl. J. Med. 2018, 378, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Vrahas, M.S.; Mithoefer, K.; Joseph, D. The long-term effects of articular impaction. Clin. Orthop. Relat. Res. 2004, 423, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Flanigan, D.C.; Harris, J.D.; Trinh, T.Q.; Siston, R.A.; Brophy, R.H. Prevalence of chondral defects in athletes’ knees: A systematic review. Med. Sci. Sports Exerc. 2010, 42, 1795–1801. [Google Scholar] [CrossRef]
- Makris, E.A.; Gomoll, A.H.; Malizos, K.N.; Hu, J.C.; Athanasiou, K.A. Repair and tissue engineering techniques for articular cartilage. Nat. Rev. Rheumatol. 2015, 11, 21–34. [Google Scholar] [CrossRef]
- Brittberg, M.; Lindahl, A.; Nilsson, A.; Ohlsson, C.; Isaksson, O.; Peterson, L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N. Engl. J. Med. 1994, 331, 889–895. [Google Scholar] [CrossRef]
- Horas, U.; Pelinkovic, D.; Herr, G.; Aigner, T.; Schnettler, R. Autologous chondrocyte implantation and osteochondral cylinder transplantation in cartilage repair of the knee joint. A prospective, comparative trial. J. Bone Joint Surg. Am. 2003, 85, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Dhanaraj, S.; Wang, Z.; Bradley, D.M.; Bowman, S.M.; Cole, B.J.; Binette, F. Minced cartilage without cell culture serves as an effective intraoperative cell source for cartilage repair. J. Orthop. Res. 2006, 24, 1261–1270. [Google Scholar] [CrossRef]
- Katopodi, T.; Tew, S.R.; Clegg, P.D.; Hardingham, T.E. The influence of donor and hypoxic conditions on the assembly of cartilage matrix by osteoarthritic human articular chondrocytes on Hyalograft® matrices. Biomaterials 2009, 30, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Vinardell, T.; Sheehy, E.J.; Buckley, C.T.; Kelly, D.J. A comparison of the functionality and in vivo phenotypic stability of cartilaginous tissues engineered from different stem cell sources. Tissue Eng. Part A 2012, 18, 1161–1170. [Google Scholar] [CrossRef]
- Quintin, A.; Schizas, C.; Scaletta, C.; Jaccoud, S.; Applegate, L.A.; Pioletti, D.P. Plasticity of fetal cartilaginous cells. Cell Transplant. 2010, 19, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Studer, D.; Cavalli, E.; Formica, F.A.; Kuhn, G.A.; Salzmann, G.; Mumme, M.; Steinwachs, M.R.; Laurent-Applegate, L.A.; Maniura-Weber, K.; Zenobi-Wong, M. Human chondroprogenitors in alginate-collagen hybrid scaffolds produce stable cartilage in vivo. J. Tissue Eng. Regen. Med. 2017, 11, 3014–3026. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Gelse, K.; Frank, S.; von der Mark, K.; Aigner, T.; Schneider, H. Transgene-activated mesenchymal cells for articular cartilage repair: A comparison of primary bone marrow-, perichondrium/periosteum- and fat-derived cells. J. Gene Med. 2006, 8, 112–125. [Google Scholar] [CrossRef]
- Wakitani, S.; Nawata, M.; Tensho, K.; Okabe, T.; Machida, H.; Ohgushi, H. Repair of articular cartilage defects in the patello-femoral joint with autologous bone marrow mesenchymal cell transplantation: Three case reports involving nine defects in five knees. J. Tissue Eng. Regen. Med. 2007, 1, 74–79. [Google Scholar] [CrossRef]
- Hwang, N.S.; Varghese, S.; Elisseeff, J. Derivation of chondrogenically-committed cells from human embryonic cells for cartilage tissue regeneration. PLoS ONE 2008, 3, e2498. [Google Scholar] [CrossRef]
- Prockop, D.J. Repair of tissues by adult stem/progenitor cells (MSCs): Controversies, myths, and changing paradigms. Mol. Ther. 2009, 17, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Saw, K.Y.; Hussin, P.; Loke, S.C.; Azam, M.; Chen, H.C.; Tay, Y.G.; Low, S.; Wallin, K.L.; Ragavanaidu, K. Articular cartilage regeneration with autologous marrow aspirate and hyaluronic acid: An experimental study in a goat model. Arthroscopy 2009, 25, 1391–1400. [Google Scholar] [CrossRef]
- Fortier, L.A.; Potter, H.G.; Rickey, E.J.; Schnabel, L.V.; Foo, L.F.; Chong, L.R.; Stokol, T.; Cheetham, J.; Nixon, A.J. Concentrated bone marrow aspirate improves full-thickness cartilage repair compared with microfracture in the equine model. J. Bone Joint Surg. Am. 2010, 92, 1927–1937. [Google Scholar] [CrossRef]
- Toh, W.S.; Lee, E.H.; Guo, X.M.; Chan, J.K.; Yeow, C.H.; Choo, A.B.; Cao, T. Cartilage repair using hyaluronan hydrogel-encapsulated human embryonic stem cell-derived chondrogenic cells. Biomaterials 2010, 31, 6968–6980. [Google Scholar] [CrossRef]
- Zscharnack, M.; Hepp, P.; Richter, R.; Aigner, T.; Schulz, R.; Somerson, J.; Josten, C.; Bader, A.; Marquass, B. Repair of chronic osteochondral defects using predifferentiated mesenchymal stem cells in an ovine model. Am. J. Sports Med. 2010, 38, 1857–1869. [Google Scholar] [CrossRef]
- Gupta, P.K.; Das, A.K.; Chullikana, A.; Majumdar, A.S. Mesenchymal stem cells for cartilage repair in osteoarthritis. Stem Cell Res. Ther. 2012, 3, 25. [Google Scholar] [CrossRef]
- Torrero, J.I.; Aroles, F.; Ferrer, D. Treatment of knee chondropathy with platelet rich plasma. Preliminary results at 6 months of follow-up with only one injection. J. Biol. Regul. Homeost. Agents 2012, 26, 71–78. [Google Scholar]
- Bekkers, J.E.; Creemers, L.B.; Tsuchida, A.I.; van Rijen, M.H.; Custers, R.J.; Dhert, W.J.; Saris, D.B. One-stage focal cartilage defect treatment with bone marrow mononuclear cells and chondrocytes leads to better macroscopic cartilage regeneration compared to microfracture in goats. Osteoarthr. Cartil. 2013, 21, 950–956. [Google Scholar] [CrossRef]
- Lee, G.W.; Son, J.H.; Kim, J.D.; Jung, G.H. Is platelet-rich plasma able to enhance the results of arthroscopic microfracture in early osteoarthritis and cartilage lesion over 40 years of age? Eur. J. Orthop. Surg. Traumatol. 2013, 23, 581–587. [Google Scholar] [CrossRef]
- Orozco, L.; Munar, A.; Soler, R.; Alberca, M.; Soler, F.; Huguet, M.; Sentis, J.; Sanchez, A.; Garcia-Sancho, J. Treatment of knee osteoarthritis with autologous mesenchymal stem cells: A pilot study. Transplantation 2013, 95, 1535–1541. [Google Scholar] [CrossRef]
- Pelttari, K.; Pippenger, B.; Mumme, M.; Feliciano, S.; Scotti, C.; Mainil-Varlet, P.; Procino, A.; von Rechengerg, B.; Schwamborn, T.; Jakob, M.; et al. Adult human neural crest-derived cells for articular cartilage repair. Sci. Transl. Med. 2014, 6, 251ra119. [Google Scholar] [CrossRef]
- Pleumeekers, M.M.; Nimeskern, L.; Koevoet, W.L.; Kops, N.; Poublon, R.M.; Stok, K.S.; van Osch, G.J. The in vitro and in vivo capacity of culture-expanded human cells from several sources encapsulated in alginate to form cartilage. Eur. Cells Mater. 2014, 27, 264–280. [Google Scholar] [CrossRef]
- Steinwachs, M.R.; Waibl, B.; Wopperer, S.; Mumme, M. Matrix-associated chondroplasty: A novel platelet-rich plasma and concentrated nucleated bone marrow cell-enhanced cartilage restoration technique. Arthrosc. Tech. 2014, 3, 279–282. [Google Scholar] [CrossRef] [PubMed]
- De Buys Roessingh, A.S.; Hohlfeld, J.; Scaletta, C.; Hirt-Burri, N.; Gerber, S.; Hohlfeld, P.; Gebbers, J.O.; Applegate, L.A. Development, characterization, and use of a fetal skin cell bank for tissue engineering in wound healing. Cell Transplant. 2006, 15, 823–834. [Google Scholar] [CrossRef] [PubMed]
- Applegate, L.A.; Scaletta, C.; Hirt-Burri, N.; Raffoul, W.; Pioletti, D. Whole-cell bioprocessing of human fetal cells for tissue engineering of skin. Skin Pharmacol. Physiol. 2009, 22, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, K.F.; Dhollander, A.A.; Verdonk, P.C.; Forsyth, R.; Verdonk, R.; Verbruggen, G. Treatment of cartilage defects in the knee using alginate beads containing human mature allogenic chondrocytes. Am. J. Sports Med. 2009, 37, 1920–1929. [Google Scholar] [CrossRef] [PubMed]
- Adkisson, H.D.; Milliman, C.; Zhang, X.; Mauch, K.; Maziraz, R.T.; Streeter, P.R. Immune evasion by neocartilage-derived chondrocytes: Implications for biologic repair of joint articular cartilage. Stem Cell Res. 2010, 4, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Acosta, F.L.; Metz, L.; Adkisson, H.D.; Liu, J.; Carruthers-Liebenberg, E.; Milliman, C.; Maloney, M.; Lotz, J.C. Porcine intervertebral disc repair using allogeneic juvenile articular chondrocytes or mesenchymal stem cells. Tissue Eng. Part A 2011, 17, 3045–3055. [Google Scholar] [CrossRef] [PubMed]
- Darwiche, S.E.; Scaletta, C.; Raffoul, W.; Pioletti, D.P.; and Applegate, L.A. Epiphyseal chondroprogenitors provide a stable cell source for cartilage cell therapy. Cell Med. 2012, 4, 23–32. [Google Scholar] [CrossRef]
- Dhollander, A.A.; Verdonk, P.C.; Lambrecht, S.; Verdonk, R.; Elewaut, D.; Verbruggen, G.; Almqvist, K.F. Midterm results of the treatment of cartilage defects in the knee using alginate beads containing human mature allogenic chondrocytes. Am. J. Sports Med. 2012, 40, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, E.; Fisch, P.; Formica, F.A.; Gareus, R.; Linder, T.; Applegate, L.A.; Zenobi-Wong, M. A comparative study of cartilage engineered constructs in immunocompromised, humanized and immunocompetent mice. J. Immunol. Regen. Med. 2018, 2, 36–46. [Google Scholar] [CrossRef]
- Zimmermann, P.; Boeuf, S.; Dickhut, A.; Boehmer, S.; Olek, S.; Richter, W. Correlation of COL10A1 induction during chondrogenesis of mesenchymal stem cells with demethylation of two CpG sites in the COL10A1 promoter. Arthritis Rheum. 2008, 58, 2743–2753. [Google Scholar] [CrossRef]
- Tompkins, M.; Adkisson, H.D.; Bonner, K.F. De novo NT allograft. Operat. Techn. Sports Med. 2013, 21, 82–89. [Google Scholar] [CrossRef]
- Doyle, A.; Griffiths, J.B. Cell and Tissue Culture: Laboratory Procedures in Biotechnology; Wiley & Sons: New York, NY, USA, 1998. [Google Scholar]
- Quintin, A.; Hirt-Burri, N.; Scaletta, C.; Schizas, C.; Pioletti, D.P.; Applegate, L.A. Consistency and safety of cell banks for research and clinical use: Preliminary analysis of fetal skin banks. Cell Transplant. 2007, 16, 675–684. [Google Scholar] [CrossRef]
- Laurent, A.; Lin, P.; Scaletta, C.; Hirt-Burri, N.; Michetti, M.; de Buys Roessingh, A.S.; Raffoul, W.; She, B.R.; Applegate, L.A. Bringing Safe and Standardized Cell Therapies to Industrialized Processing for Burns and Wounds. Front Bioeng. Biotechnol. 2020, 8, 581. [Google Scholar] [CrossRef]
- Shah, M.; Foreman, D.M.; Ferguson, M.W.J. Control of scarring in adult wounds by neutralising antibody to transforming growth factor β. Lancet 1992, 339, 213–214. [Google Scholar] [CrossRef]
- Cass, D.L.; Meuli, M.; Adzick, N.S. Scar wars: Implications of fetal wound healing for the pediatric burn patient. Pediatr. Surg. Int. 1997, 12, 484–489. [Google Scholar] [CrossRef]
- Ribatti, D. The chick embryo chorioallantoic membrane (CAM). A multifaceted experimental model. Mech. Dev. 2016, 141, 70–77. [Google Scholar] [CrossRef]
- Outerbridge, R.E. The etiology of chondromalacia patellae. J. Bone Joint Surg. Br. 1961, 43-B, 752–757. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W.; Marx, R.G.; Beaton, D.E.; Miura, Y.; Gallay, S.H.; Fitzsimmons, J.S. Validation of a simple histological-histochemical cartilage scoring system. Tissue Eng. 2001, 7, 313–320. [Google Scholar] [CrossRef]
- Little, C.; Smith, S.; Ghosh, P.; Bellenger, C. Histomorphological and immunohistochemical evaluation of joint changes in a model of osteoarthritis induced by lateral meniscectomy in sheep. J. Rheumatol. 1997, 24, 2199–2209. [Google Scholar] [PubMed]
- Krenn, V.; Morawietz, L.; Burmester, G.R.; Kinne, R.W.; Mueller-Ladner, U.; Muller, B.; Haupl, T. Synovitis score: Discrimination between chronic low-grade and high-grade synovitis. Histopathology 2006, 49, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, H.; Goto, K.; Miyamoto, K. Scoring evaluation for histopathological features of synovium in patients with rheumatoid arthritis during anti-tumor necrosis factor therapy. Rheumatol. Int. 2010, 30, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.A.; Hincke, M.T. Strategies for articular cartilage lesion repair and functional restoration. Tissue Eng. Part B Rev. 2010, 16, 305–329. [Google Scholar] [CrossRef] [PubMed]
- Bedi, A.; Feeley, B.T.; Williams, R.J. Management of articular cartilage defects of the knee. J. Bone Joint Surg. Am. 2010, 92, 994–1009. [Google Scholar] [CrossRef] [PubMed]
- Brittberg, M. Cell carriers as the next generation of cell therapy for cartilage repair: A review of the matrix-induced autologous chondrocyte implantation procedure. Am. J. Sports Med. 2010, 38, 1259–1271. [Google Scholar] [CrossRef]
- Teo, A.Q.A.; Wong, K.L.; Shen, L.; Lim, J.Y.; Wei, S.T.; Lee, H.; Hui, J.H.P. Equivalent 10-year outcomes after implantation of autologous bone marrow-derived mesenchymal stem cells versus autologous chrondrocyte implantation for chondral defects of the knee. Am. J. Sports Med. 2019, 47, 2881–2887. [Google Scholar] [CrossRef]
- Benthien, J.P.; Behrens, P. The treatment of chondral and osteochondral defects of the knee with autologous matrix-induced chondrogenesis (AMIC): Method description and recent developments. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1316–1319. [Google Scholar] [CrossRef] [PubMed]
- Mithoefer, K.; McAdams, T.; Williams, R.J.; Kreuz, P.C.; Mandelbaum, B.R. Clinical efficacy of the microfracture technique for articular cartilage repair in the knee: An evidence-based systematic analysis. Am. J. Sports Med. 2009, 37, 2053–2063. [Google Scholar] [CrossRef] [PubMed]
- Gille, J.; Behrens, P.; Volpi, P.; de Girolamo, L.; Reiss, E.; Zoch, W.; Anders, S. Outcome of Autologous Matrix Induced Chondrogenesis (AMIC) in cartilage knee surgery: Data of the AMIC Registry. Arch. Orthop. Trauma Surg. 2013, 133, 87–93. [Google Scholar] [CrossRef]
- Piotet, L.-M. Third Generation of Cellular Therapies for Chondral Defects: A Bibliographic Search. Master’s Thesis, University of Lausanne, Lausanne, Switzerland, 2018. [Google Scholar]
- Minas, T.; Peterson, L. Autologous chondrocyte transplantation. Oper. Tech. Sports Med. 2012, 20, 72–86. [Google Scholar] [CrossRef]
- Kon, E.; Roffi, A.; Filardo, G.; Tesei, G.; Marcacci, M. Scaffold-based cartilage treatments: With or without cells? A systematic review of preclinical and clinical evidence. Arthroscopy 2015, 31, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Dhollander, A.A.; De Neve, F.; Almqvist, K.F.; Verdonk, R.; Lambrecht, S.; Elewaut, D.; Verbruggen, G.; Verdonk, P.C. Autologous matrix-induced chondrogenesis combined with platelet-rich plasma gel: Technical description and a five pilot patients report. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Mumme, M.; Barbero, A.; Miot, S.; Wixmerten, A.; Feliciano, S.; Wolf, F.; Asnaghi, A.M.; Baumhoer, D.; Bieri, O.; Kretzcchmar, M.; et al. Nasal chondrocyte-based engineered autologous cartilage tissue for repair of articular cartilage defects: An observational first-in-human trial. Lancet 2016, 388, 1985–1994. [Google Scholar] [CrossRef]
- Noh, M.J.; Copeland, R.O.; Yi, Y.; Choi, K.-B.; Meschter, C.; Hwang, S.; Lim, C.-L.; Yip, V.; Hyun, J.-P.; Lee, H.-Y.; et al. Pre-clinical studies of retrovirally transduced human chondrocytes expressing transforming growth factor-beta.1 (TG-C). Cytotherapy 2010, 12, 384–393. [Google Scholar] [CrossRef]
- Ha, C.-W.; Noh, M.J.; Choi, K.B.; Lee, K.H. Initial phase I safety of retrovirally transduced human chondrocytes expressing transforming growth factor-beta-1 in degenerative arthritis patients. Cytotherapy 2012, 14, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Broguiere, N.; Cavalli, E.; Salzmann, G.M.; Applegate, L.A.; Zenobi-Wong, M. Factor XIII cross-linked hyaluronan hydrogels for cartilage tissue engineering. ACS Biomater. Sci. Eng. 2016, 2, 2176–2184. [Google Scholar] [CrossRef]
- Madeira, C.; Santhagunam, A.; Salgueiro, J.B.; Cabral, J.M. Advanced cell therapies for articular cartilage regeneration. Trends Biotechnol. 2015, 33, 35–42. [Google Scholar] [CrossRef]
- Mardones, R.; Jofré, C.M.; Minguell, J.J. Cell therapy and tissue engineering approaches for cartilage repair and/or regeneration. Int. J. Stem Cells 2015, 8, 48–53. [Google Scholar] [CrossRef]
- Häuselmann, H.J.; Fernandes, R.J.; Mok, S.S.; Schmid, T.M.; Block, J.A.; Aydelotte, M.B.; Kuettner, K.E.; Thonar, E.J. Phenotypic stability of bovine articular chondrocytes after long-term culture in alginate beads. J. Cell Sci. 1994, 107, 17–27. [Google Scholar] [PubMed]
- Mhanna, R.; Kashyap, A.; Palazzolo, G.; Vallmajo-Martin, Q.; Becher, J.; Möller, S.; Schnabelrauch, M.; Zenobi-Wong, M. Chondrocyte culture in three-dimensional alginate sulfate hydrogels promotes proliferation while maintaining expression of chondrogenic markers. Tissue Eng. Part A 2014, 20, 1454–1464. [Google Scholar] [CrossRef]
- Mellor, L.F.; Baker, T.L.; Brown, R.J.; Catlin, L.W.; Oxford, J.T. Optimal 3D culture of primary articular chondrocytes for use in the rotating wall vessel bioreactor. Aviat. Space Environ. Med. 2014, 85, 798–804. [Google Scholar] [CrossRef]
- Abdel-Sayed, P.; Darwiche, S.E.; Kettenberger, U.; Pioletti, D.P. The role of energy dissipation of polymeric scaffolds in the mechanobiological modulation of chondrogenic expression. Biomaterials 2014, 35, 1890–1897. [Google Scholar] [CrossRef] [PubMed]
- Hunter, C.J.; Mouw, J.K.; Levenston, M.E. Dynamic compression of chondrocyte-seeded fibrin gels: Effects on matrix accumulation and mechanical stiffness. Osteoarthr. Cartil. 2004, 12, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Mauck, R.L.; Byers, B.A.; Yuan, X.; Tuan, R.S. Regulation of cartilaginous ECM gene transcription by chondrocytes and MSCs in 3D culture in response to dynamic loading. Biomech. Model Mechanobiol. 2007, 6, 113–125. [Google Scholar] [CrossRef]
- Thorpe, S.D.; Buckley, C.T.; Vinardell, T.; O’Brien, F.J.; Campbell, V.A.; Kelly, D.J. Dynamic compression can inhibit chondrogenesis of mesenchymal stem cells. Biochem. Biophys. Res. Commun. 2008, 14, 319–331. [Google Scholar] [CrossRef]
- Wendt, D.; Marsano, A.; Jakob, M.; Heberer, M.; Martin, I. Oscillating perfusion of cell suspensions through three-dimensional scaffolds enhances cell seeding efficiency and uniformity. Biotechnol. Bioeng. 2003, 84, 205–214. [Google Scholar] [CrossRef]
- Melchels, F.P.; Barradas, A.M.; van Blitterswijk, C.A.; de Boer, J.; Feijen, J.; Grijpma, D.W. Effects of the architecture of tissue engineering scaffolds on cell seeding and culturing. Acta Biomater. 2010, 6, 4208–4217. [Google Scholar] [CrossRef] [PubMed]
- Burg, K.J.; Holder, W.D., Jr.; Culberson, C.R.; Beiler, R.J.; Greene, K.G.; Loebsack, A.B.; Roland, W.D.; Eiselt, P.; Mooney, D.J.; Halberstadt, C.R. Comparative study of seeding methods for three-dimensional polymeric scaffolds. J. Biomed. Mater. Res. 2000, 51, 642–649. [Google Scholar] [CrossRef]
- Alvarez-Barreto, J.F.; Linehan, S.M.; Shambaugh, R.L.; Sikavitsas, V.I. Flow perfusion improves seeding of tissue engineering scaffolds with different architectures. Ann. Biomed. Eng. 2007, 35, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Roh, J.D.; Nelson, G.N.; Udelsman, B.V.; Brennan, M.P.; Lockhart, B.; Fong, P.M.; Lopez-Soler, R.I.; Salzman, W.M.; Breuer, C.K. Centrifugal seeding increases seeding efficiency and cellular distribution of bone marrow stromal cells in porous biodegradable scaffolds. Tissue Eng. 2007, 13, 2743–2749. [Google Scholar] [CrossRef]
- Thevenot, P.; Nair, A.; Dey, J.; Yang, J.; Tang, L. Method to analyze three-dimensional cell distribution and infiltration in degradable scaffolds. Tissue Eng. Part C Methods 2008, 377, 458–462. [Google Scholar] [CrossRef]
- Moretti, M.; Wendt, D.; Dickinson, S.C.; Sims, T.J.; Hollander, A.P.; Kelly, D.J.; Prendergast, P.J.; Heberer, M.; Martin, I. Effects of in vitro preculture on in vivo development of human engineered cartilage in an ectopic model. Tissue Eng. 2005, 11, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Roche, S.; Ronzière, M.C.; Herbage, D.; Freyria, A.M. Native and DPPA cross-linked collagen sponges seeded with fetal bovine epiphyseal chondrocytes used for cartilage tissue engineering. Biomaterials 2001, 22, 9–18. [Google Scholar] [CrossRef]
- Hasegawa, T.; Miwa, M.; Sakai, Y.; Niikura, T.; Lee, S.Y.; Oe, K.; Iwakura, T.; Kurosaka, M.; Komori, T. Efficient cell-seeding into scaffolds improves bone formation. J. Dent. Res. 2010, 89, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Erickson, I.E.; Kestle, S.R.; Zellars, K.H.; Farrell, M.J.; Kim, M.; Burdick, J.A.; Mauck, R.L. High mesenchymal stem cell seeding densities in hyaluronic acid hydrogels produce engineered cartilage with native tissue properties. Acta Biomater. 2012, 8, 3027–3034. [Google Scholar] [CrossRef]
- Hollister, S.J. Porous scaffold design for tissue engineering. Nat. Mater. 2005, 4, 518–524. [Google Scholar] [CrossRef]
- Kemppainen, J.M.; Hollister, S.J. Differential effects of designed scaffold permeability on chondrogenesis by chondrocytes and bone marrow stromal cells. Biomaterials 2010, 31, 279–287. [Google Scholar] [CrossRef]
- Huang, A.H.; Farrell, M.J.; Kim, M.; Mauck, R.L. Long-term dynamic loading improves the mechanical properties of chondrogenic mesenchymal stem cell-laden hydrogel. Eur. Cells Mater. 2010, 19, 72–85. [Google Scholar] [CrossRef]
- Campbell, J.J.; Lee, D.A.; Bader, D.L. Dynamic compressive strain influences chondrogenic gene expression in human mesenchymal stem cells. Biorheology 2006, 43, 455–470. [Google Scholar]
- Terraciano, V.; Hwang, N.; Moroni, L.; Park, H.B.; Zhang, Z.; Mizrahi, J.; Seliktar, D.; Elisseeff, J. Differential response of adult and embryonic mesenchymal progenitor cells to mechanical compression in hydrogels. Stem Cells 2007, 25, 2730–2738. [Google Scholar] [CrossRef]
- Montjovent, M.O.; Bocelli-Tyndall, C.; Scaletta, C.; Scherberich, A.; Mark, S.; Martin, I.; Applegate, L.A.; Pioletti, D.P. In vitro characterization of immune-related properties of human fetal bone cells for potential tissue engineering applications. Tissue Eng. Part A 2009, 15, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Ramelet, A.A.; Hirt-Burri, N.; Raffoul, W.; Scaletta, C.; Pioletti, D.P.; Offord, E.; Mansourian, R.; Applegate, L.A. Chronic wound healing by fetal cell therapy may be explained by differential gene profiling observed in fetal versus old skin cells. Exp. Gerontol. 2009, 44, 208–218. [Google Scholar] [CrossRef]
- Pritchard, S.; Bianchi, D.W. Fetal cell microchimerism in the maternal heart: Baby gives back. Circ. Res. 2012, 110, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Levinson, C.; Truong, V.X.; Laurent-Applegate, L.A.; Maniura-Weber, K.; Thissen, H. Microencapsulation improves chondrogenesis in vitro and cartilaginous matrix stability in vivo compared to bulk encapsulation. Biomater. Sci. 2020, 8, 1711–1725. [Google Scholar] [CrossRef] [PubMed]
- Nasrollahzadeh, N.; Applegate, L.A.; Pioletti, D.P. Development of an effective cell seeding technique: Simulation, implementation, and analysis of contributing factors. Tissue Eng. Part C Methods 2017, 23, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.; Lee, M.; Applegate, L.A.; Zenobi-Wong, M. An injectable heparin-conjugated hyaluronan scaffold for local delivery of transforming growth factor β1 promotes successful chondrogenesis. Acta Biomater. 2019, 99, 168–180. [Google Scholar] [CrossRef]
- Park, D.Y.; Min, B.H.; Park, S.R.; Oh, H.J.; Truong, M.D.; Kim, M.; Choi, J.Y.; Park, I.S.; Choi, B.H. Engineered cartilage utilizing fetal cartilage-derived progenitor cells for cartilage repair. Sci. Rep. 2020, 10, 5722. [Google Scholar] [CrossRef] [PubMed]
- Cherian, J.J.; Parvizi, J.; Bramlet, D.; Lee, K.H.; Romness, D.W.; Mont, M.A. Preliminary results of a phase II randomized study to determine the efficacy and safety of genetically engineered allogeneic human chondrocytes expressing TGF-B1 in patients with grade 3 chronic degenerative joint disease of the knee. Osteoarthr. Cart. 2015, 23, 2109–2118. [Google Scholar] [CrossRef] [PubMed]






| Treatment | Description | Benefits | Limitations |
|---|---|---|---|
| Non-surgical methods | Analgesics, weight loss, physical re-education, physical therapy, complementary medicine (e.g., acupuncture) | No surgery necessary Relatively inexpensive | Palliative treatment options Chronic analgesic use potential |
| Arthroscopic chondroplasty | Arthroscopic resection of detached cartilage fragments to prevent further joint irritation and damage | Rapid, minimally invasive procedureImmediate weight-bearing possible | Palliative treatment Benefits not proven Brief pain relief |
| MF 1 | Arthroscopic procedure to create small lesions in the osteochondral interface to direct osteoprogenitor cells into damaged cartilage tissue | No graft required for defects < 2 cm2 Rapid recovery | Fibrocartilage formation potential Variable functional outcomes Rapid deterioration |
| Mosaicoplasty | Osteochondral autografts harvested from patient non-loaded zones of the joint | Optimal for small lesions (1–4 cm2) Pain relief | Sub-optimal surrounding tissue graft adherence Graft-site morbidity |
| ACI 2 | Autologous cultured and expanded chondrocytes implanted in the lesion under a tissue flap | Hyaline cartilage formation potential Extensive lesion treatment (<10 cm2) | Graft delamination Periosteal hypertrophy Qualitative variability of regenerated tissue Onerous protocol |
| MACI 3 | Autologous cultured and expanded chondrocytes seeded onto 3D scaffolds and implanted into defect | Treatment of large lesions Hyaline cartilage formation potential Limited periosteal hypertrophy | Graft delamination Limited integration Qualitative variability of regenerated tissue Onerous protocol |
| Joint arthroplasty | Replacement of arthritic joint with an artificial implant | Pain relief Functional resurgence potential | Infectious risk Functional outcome variability Implant wear or loosening |
| Cell Type Characteristic | Data, Findings 1 | References |
|---|---|---|
| Identity | “FE002-Cart”, primary diploid cell type, from ulnar epiphysis Fibroblast-like stable cellular morphology in 2D in vitro culture Defined surface marker profile (i.e., CD14−, CD34−, CD45−, HLA-DP/DQ/DR−, CD26+, CD44+, CD73+, CD90+, CD105+, CD166+, HLA-ABC+) 2 | [34] |
| Stability | Establishment and testing of EOPCB 3 at Passage 12 1 Normal 46X,Y karyotype stable up to Passage 12 1 Lifespan > 35 PDs 4 with stable in vitro expansion kinetics Resistance to adipogenic and osteogenic induction, cryogenic shock | [34] |
| Cytocompatibility | Cytocompatible with various hydrogel formulations (e.g., alginate and hyaluronan-based polymer gels) High shear stress resistance for seeding in bioengineered constructs Clinically relevant scaffold stiffness generation under stimulation | [64,92,93] |
| Safety | Non-toxic and no angiogenesis perturbation in CAM 5 model 1 Non-immunogenic and non-tumorigenic in murine and rat models of cartilage defect or subcutaneous implantation Non-immunogenic, non-tumorigenic, and no slowing of cartilage defect healing in caprine model 1 | [36,92] |
| Functionality | Spontaneous chondrogenic activity in 3D micropellets Potent and stable production of ECM 6 (i.e., GAGs 7, aggrecan, types I and II collagen) Important functional responsiveness to mechanostimulation in dynamic scaffold culture conditions Highly responsive chondrogenic potential under biochemical stimulation (e.g., alginate, TGF-β1) Highly responsive chondrogenic potential in specific formulations (e.g., therapeutic cell microencapsulation) | [12,34,36,70,92,94] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laurent, A.; Abdel-Sayed, P.; Ducrot, A.; Hirt-Burri, N.; Scaletta, C.; Jaccoud, S.; Nuss, K.; de Buys Roessingh, A.S.; Raffoul, W.; Pioletti, D.; et al. Development of Standardized Fetal Progenitor Cell Therapy for Cartilage Regenerative Medicine: Industrial Transposition and Preliminary Safety in Xenogeneic Transplantation. Biomolecules 2021, 11, 250. https://doi.org/10.3390/biom11020250
Laurent A, Abdel-Sayed P, Ducrot A, Hirt-Burri N, Scaletta C, Jaccoud S, Nuss K, de Buys Roessingh AS, Raffoul W, Pioletti D, et al. Development of Standardized Fetal Progenitor Cell Therapy for Cartilage Regenerative Medicine: Industrial Transposition and Preliminary Safety in Xenogeneic Transplantation. Biomolecules. 2021; 11(2):250. https://doi.org/10.3390/biom11020250
Chicago/Turabian StyleLaurent, Alexis, Philippe Abdel-Sayed, Aurélie Ducrot, Nathalie Hirt-Burri, Corinne Scaletta, Sandra Jaccoud, Katja Nuss, Anthony S. de Buys Roessingh, Wassim Raffoul, Dominique Pioletti, and et al. 2021. "Development of Standardized Fetal Progenitor Cell Therapy for Cartilage Regenerative Medicine: Industrial Transposition and Preliminary Safety in Xenogeneic Transplantation" Biomolecules 11, no. 2: 250. https://doi.org/10.3390/biom11020250
APA StyleLaurent, A., Abdel-Sayed, P., Ducrot, A., Hirt-Burri, N., Scaletta, C., Jaccoud, S., Nuss, K., de Buys Roessingh, A. S., Raffoul, W., Pioletti, D., von Rechenberg, B., Applegate, L. A., & Darwiche, S. (2021). Development of Standardized Fetal Progenitor Cell Therapy for Cartilage Regenerative Medicine: Industrial Transposition and Preliminary Safety in Xenogeneic Transplantation. Biomolecules, 11(2), 250. https://doi.org/10.3390/biom11020250