
Immunocytometric Analysis of Oral Pemphigus vulgaris Patients after Treatment with Rituximab as Adjuvant

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Anti-Dsg-1 and Dsg-3 IgG Enzyme-Linked Immunosorbent Assay (ELISA)
2.3. Leucocytes Immunophenotyping
2.4. Clinical Parameters
2.5. Therapeutic Procedure
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Clinical Course of Patients
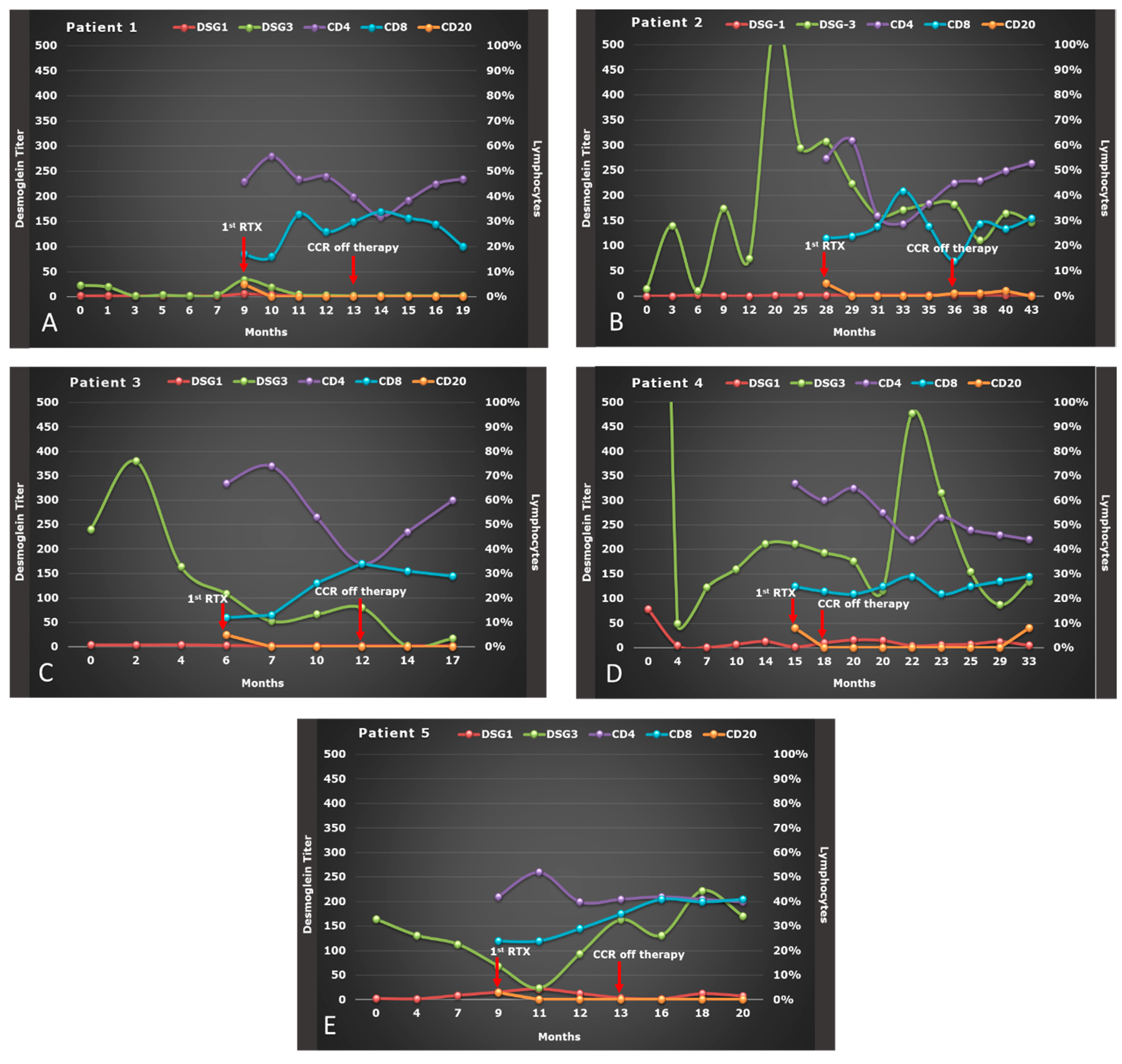
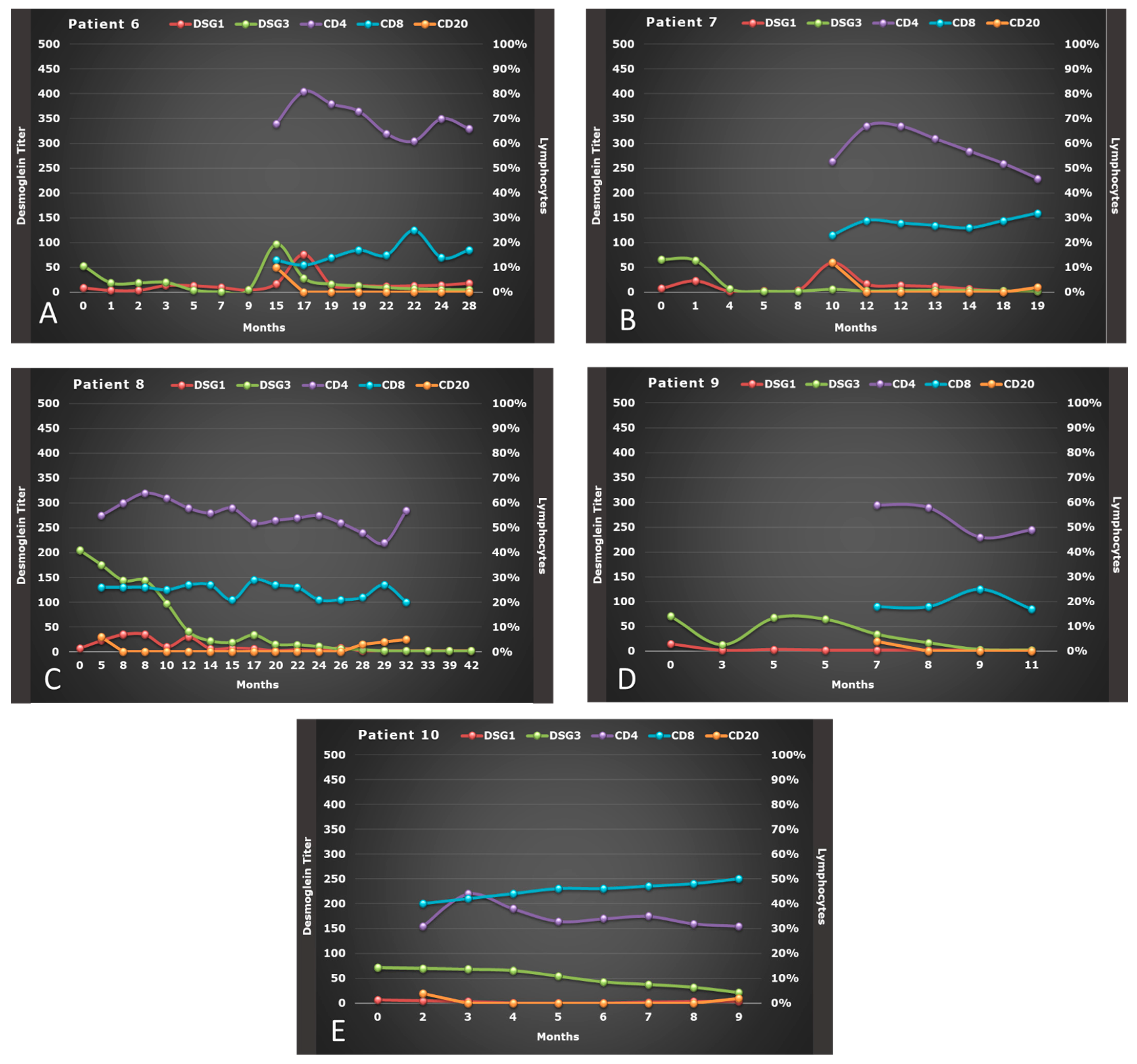
3.2. Serologic Response to RTX Therapy
3.3. Effect of RTX on Lymphocytes Subsets
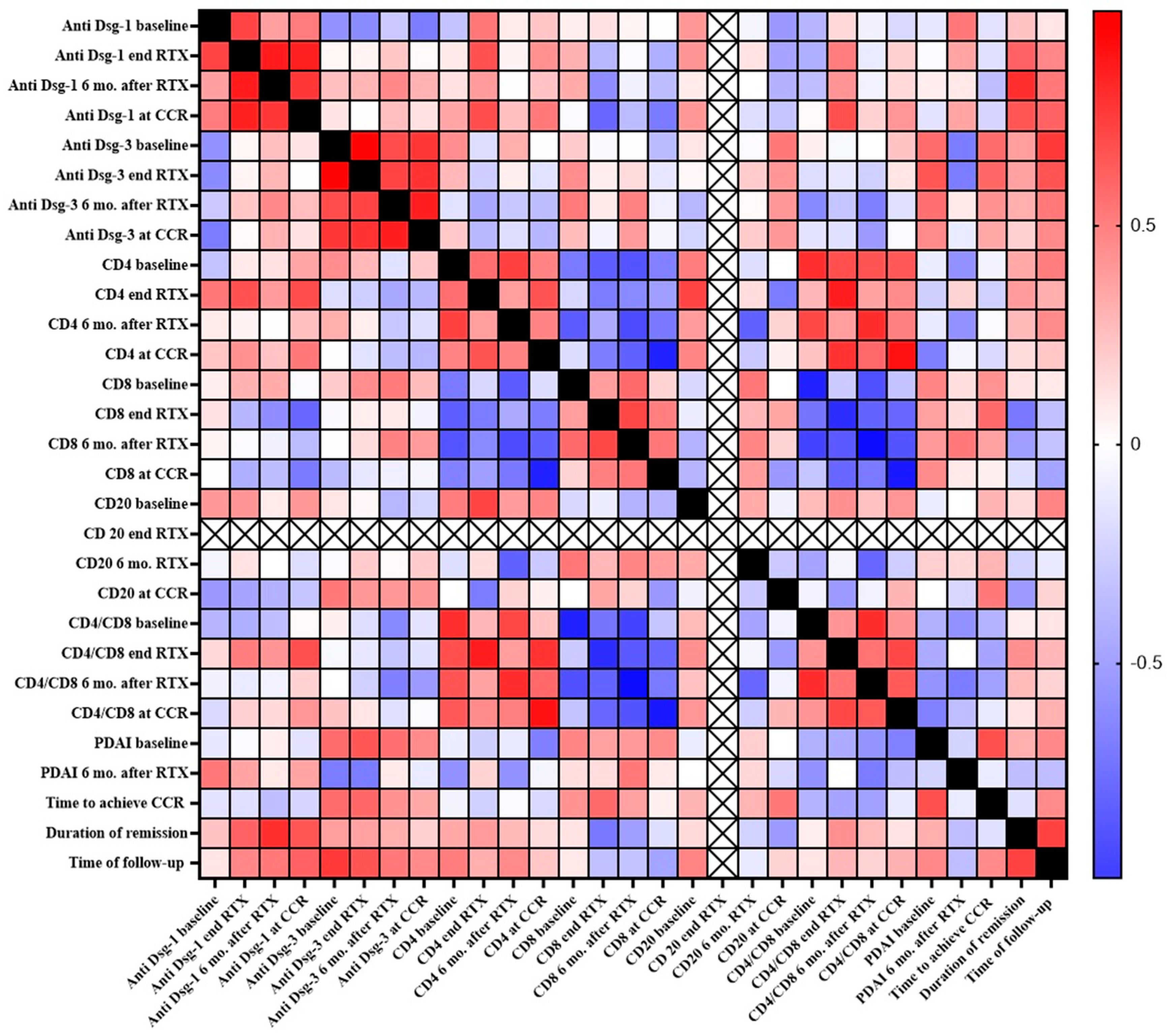
3.4. Correlation between Clinical and Immunological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kasperkiewicz, M.; Ellebrecht, C.T.; Takahashi, H.; Yamagami, J.; Zillikens, D.; Payne, A.S.; Amagai, M. Pemphigus. Nat. Rev. Dis. Primer 2017, 3, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amagai, M.; Klaus-Kovtun, V.; Stanley, J.R. Autoantibodies against a novel epithelial cadherin in pemphigus vulgaris, a disease of cell adhesion. Cell 1991, 67, 869–877. [Google Scholar] [CrossRef]
- Amber, K.T.; Valdebran, M.; Grando, S.A. Non-Desmoglein Antibodies in Patients with Pemphigus Vulgaris. Front. Immunol. 2018, 9, 1190. [Google Scholar] [CrossRef]
- Mignogna, M.D.; Fortuna, G.; Leuci, S.; Ruoppo, E. Oropharyngeal Pemphigus Vulgaris and Clinical Remission: A Long-Term, Longitudinal Study. Am. J. Clin. Dermatol. 2010, 11, 137–145. [Google Scholar] [CrossRef]
- Cholera, M.; Chainani-Wu, N. Management of Pemphigus Vulgaris. Adv. Ther. 2016, 33, 910–958. [Google Scholar] [CrossRef] [Green Version]
- Craythorne, E.; du Viver, A.; Mufti, G.J.; Warnakulasuriya, S. Rituximab for the treatment of corticosteroid–refractory pemphi-gus vulgaris with oral and skin manifestations. J. Oral Pathol. Med. 2011, 40, 616–620. [Google Scholar] [CrossRef]
- Ahmed, A.R.; Dahl, M.V. Consensus Statement on the Use of Intravenous Immunoglobulin Therapy in the Treatment of Auto-immune Mucocutaneous Blistering Diseases. Arch. Dermatol. 2003, 139, 1051–1059. [Google Scholar] [CrossRef]
- Ahmed, A.R.; Spigelman, Z.; Cavacini, L.A.; Posner, M.R. Treatment of pemphigus vulgaris with rituximab and intravenous im-mune globulin. N. Engl. J. Med. 2006, 355, 1772–1779. [Google Scholar] [CrossRef] [PubMed]
- Mignogna, M.D.; Fortuna, G.; Ruoppo, E.; Adamo, D.; Leuci, S.; Fedele, S. Variations in serum hemoglobin, albumin, and electro-lytes in patients receiving intravenous immunoglobulin therapy: A real clinical threat? Am. J. Clin. Dermatol. 2007, 8, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Mignogna, M.D.; Fortuna, G.; Leuci, S.; Ruoppo, E.; Adamo, D.; Fedele, S. Analysis of thromboembolic risk related to high-dose intravenous immunoglobulin treatment: A preliminary clinical study of 10 patients with autoimmune mucocutaneous blis-tering diseases. Clin. Exp. Dermatol. 2009, 34, 145–150. [Google Scholar] [CrossRef]
- Cianchini, G.; Lupi, F.; Masini, C.; Corona, R.; Puddu, P.; De Pità, O. Therapy with rituximab for autoimmune pemphigus: Re-sults from a single-center observational study on 42 cases with long-term follow-up. J. Am. Acad. Dermatol. 2012, 67, 617–622. [Google Scholar] [CrossRef]
- Esposito, M.; Capriotti, E.; Giunta, A.; Bianchi, L.; Chimenti, S. Long-lasting remission of pemphigus vulgaris treated with rituxi-mab. Acta. Derm. Venereol. 2006, 86, 87–89. [Google Scholar] [PubMed]
- Robinson, A.J.; Vu, M.A.; Unglik, G.A.; Varigos, G.; Scardamaglia, L. Low-dose rituximab and concurrent adjuvant therapy for pemphigus: Protocol and single-centre long-term review of nine patients. Australas. J. Dermatol. 2018, 59, e47–e52. [Google Scholar] [CrossRef] [PubMed]
- Fortuna, G.; Calabria, E.; Ruoppo, E.; Adamo, D.; Aria, M.; Amato, M.; Mignogna, M.D. The use of rituximab as an adjuvant in the treatment of oral pemphigus vulgaris. J. Oral Pathol. Med. 2020, 49, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Breedveld, F.; Agarwal, S.; Yin, M.; Ren, S.; Li, N.F.; Shaw, T.M.; Davies, B.E. Rituximab Pharmacokinetics in Patients With Rheumatoid Arthritis: B-Cell Levels Do Not Correlate With Clinical Response. J. Clin. Pharmacol. 2007, 47, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Santagostino, A.; Garbaccio, G.; Pistorio, A.; Bolis, V.; Camisasca, G.; Pagliaro, P.; Girotto, M. An Italian national multicenter study for the definition of reference ranges for normal values of peripheral blood lymphocyte subsets in healthy adults. Haematol. 1999, 84, 499–504. [Google Scholar]
- Romano, C.; De Fanis, U.; Sellitto, M.A.; Dalla Mora, L.; Chiurazzi, F.; Giunta, R.; Rotoli, B.; Lucivero, G. Effects of Preactivated Autologous T Lym-phocytes on CD80, CD86 and CD95 Expression by Chronic Lymphocytic Leukemia B Cells. Leuk Lymphoma. 2003, 44, 1963–1971. [Google Scholar] [CrossRef]
- Cacciapuoti, S.; De Rosa, A.; Gelzo, M.; Megna, M.; Raia, M.; Pinchera, B.; Pontarelli, A.; Scotto, R.; Scala, E.; Scarano, F.; et al. Immunocytometric analysis of COVID patients: A contribution to personalized therapy? Life. Sci. 2020, 261, 118355. [Google Scholar] [CrossRef]
- Rosenbach, M.; Murrell, D.F.; Bystryn, J.-C.; Dulay, S.; Dick, S.; Fakharzadeh, S.; Hall, R.; Korman, N.J.; Lin, J.; Okawa, J.; et al. Reliability and Convergent Validity of Two Outcome Instruments for Pemphigus. J. Investig. Dermatol. 2009, 129, 2404–2410. [Google Scholar] [CrossRef] [Green Version]
- Murrell, D.F.; Dick, S.; Ahmed, A.R.; Amagai, M.; Barnadas, M.A.; Borradori, L.; Bystryn, J.-C.; Cianchini, G.; Diaz, L.; Fivenson, D.; et al. Consensus statement on definitions of disease, end points, and therapeutic response for pemphigus. J. Am. Acad. Dermatol. 2008, 58, 1043–1046. [Google Scholar] [CrossRef] [Green Version]
- Calabria, E.; Fortuna, G.; Aria, M.; Mignogna, M.D. Autoimmune mucocutaneous blistering diseases in the south of Italy: A 25-year retrospective study on 169 patients. J. Oral Pathol. Med. 2020, 49, 672–680. [Google Scholar] [CrossRef]
- Tavakolpour, S.; Mahmoudi, H.; Balighi, K.; Abedini, R.; Daneshpazhooh, M. Sixteen-year history of rituximab therapy for 1085 pemphigus vulgaris patients: A systematic review. Int. Immunopharmacol. 2018, 54, 131–138. [Google Scholar] [CrossRef]
- Joly, P.; Maho-Vaillant, M.; Prost-Squarcioni, C.; Hebert, V.; Houivet, E.; Calbo, S.; Caillot, F.; Golinski, M.L.; Labeille, B.; Picard-Dahan, C.; et al. First-line rituximab combined with short-term prednisone versus prednisone alone for the treatment of pemphigus (Ritux 3): A prospective, multicentre, parallel-group, open-label randomised trial. Lancet 2017, 389, 2031–2040. [Google Scholar] [CrossRef]
- De Bhattacharjee, R.D.; Handa, S.; Minz, R.W.; Saikia, B.; Joshi, N. Assessment of the Effects of Rituximab Monotherapy on Dif-ferent Subsets of Circulating T-Regulatory Cells and Clinical Disease Severity in Severe Pemphigus Vulgaris. Dermatology 2016, 232, 572–577. [Google Scholar] [CrossRef]
- Cho, Y.; Lee, F.; Chu, C.; Wang, L. First-line Combination Therapy with Rituximab and Corticosteroids is Effective and Safe for Pemphigus. Acta. Derm. Venereol. 2014, 94, 472–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortazavi, H.; Shahdi, M.; Amirzargar, A.A.; Naraghi, Z.S.; Valikhani, M.; Daneshpazhooh, M.; Vasheghani-Farahani, A.; Sedaghat, M.; Chams-Davatch, C. Desmoglein ELISA in the di-agnosis of pemphigus and its correlation with the severity of pemphigus vulgaris. Iran. J. Allergy Asthma Immunol. 2009, 8, 53–56. [Google Scholar] [PubMed]
- Daneshpazhooh, M.; Chams-Davatchi, C.; Khamesipour, A.; Mansoori, P.; Taheri, A.; Firooz, A.; Mortazavi, H.; Esmaili, N.; Dowlati, Y. Desmoglein 1 and 3 en-zyme-linked immunosorbent assay in Iranian patients with pemphigus vulgaris: Correlation with phenotype, severity, and disease activity. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 1319–1324. [Google Scholar] [CrossRef]
- Yeoh, S.; Byth-Wilson, K.; Murrell, D.F.; Schifter, M.; Lin, M.; Fulcher, D.A. Pemphigus vulgaris disease activity: The role of antibodies to desmogleins and their isotype. J. Oral Pathol. Med. 2019, 48, 619–625. [Google Scholar] [CrossRef]
- Sardana, K.; Garg, V.; Agarwal, P. Is there an emergent need to modify the desmoglein compensation theory in pemphigus on the basis of Dsg ELISA data and alternative pathogenic mechanisms? Br. J. Dermatol. 2012, 168, 669–674. [Google Scholar] [CrossRef]
- Albers, L.N.; Liu, Y.; Bo, N.; Swerlick, R.A.; Feldman, R.J. Developing biomarkers for predicting clinical relapse in pemphigus pa-tients treated with rituximab. J. Am. Acad. Dermatol. 2017, 7, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, H.; Matsue, H.; Nagasaka, A.; Nakamura, Y.; Tsukamoto, K.; Shibagaki, N.; Kawamura, T.; Kitamura, R.; Ando, N.; Shimada, S. CD4+CD25high Regulatory T Cells Are Markedly Decreased in Blood of Patients with Pemphigus Vulgaris. Dermatology 2007, 214, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.-C.; Zhu, H.-Q.; Li, W.-P.; Zhao, X.-Q.; Yuan, H.-J.; Zheng, J.; Pan, M. The imbalance of Th17 and regulatory T cells in pemphigus patients. Eur. J. Dermatol. 2013, 23, 795–802. [Google Scholar] [CrossRef] [PubMed]
- El-Zawahry, B.; Bassiouny, D.; Hegazy, R.; Gawdat, H.; Shalaby, S.; Khorshied, M.; Saleh, M.A. Rituximab treatment in pemphigus vul-garis: Effect on circulating Tregs. Arch. Dermatol. Res. 2017, 309, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Vinay, K.; Cazzaniga, S.; Amber, K.T.; Feldmeyer, L.; Naldi, L.; Borradori, L. Rituximab as first-line adjuvant therapy for pemphi-gus: Retrospective analysis of long-term outcomes at a single center. J. Am. Acad. Dermatol. 2018, 78, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Ellebrecht, C.T.; Bhoj, V.G.; Nace, A.; Choi, E.J.; Mao, X.; Cho, M.J.; Di Zenzo, G.; Lanzavecchia, A.; Seykora, J.T.; Cotsarelis, G.; et al. Reengineering chimeric antigen receptor T cells for targeted therapy of autoimmune disease. Science 2016, 353, 179–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No. of Patients (%) | |
|---|---|
| Total | 10 (100) |
| Male | 3 (30) |
| Female | 7 (70) |
| Mean age in years at diagnosis (range) | M: 51.7 (49–57) F: 42.4 (30–55) |
| Drug therapy before therapy with rituximab | |
| Corticosteroids and immunosuppressants | 8 (80) |
| Azathioprine | 5 (50) |
| Sulfasalazine | 3 (30) |
| Corticosteroids only | 2 (20) |
| Clinical remission after therapy with rituximab | |
| CCR “off-therapy” after RTX | 10 (100) |
| Transient side effects due to RTX (headache and tachycardia) | 2 (20) |
| Relapse after RTX | 2 (20) |
| Pts | Age | Sex | Anti-Dsg-1 Baseline * | Anti-Dsg-1 End of RTX | Anti-Dsg-1 6 mo. after RTX | p-Value | Anti-Dsg-3 Baseline | Anti-Dsg-3 End of RTX | Anti-Dsg-3 6 mo. after RTX | p-Value | CD4/CD8 Baseline | CD4/CD8 End of RTX | CD4/CD8 6 mo. after RTX | p-Value |
| 1 | 57 | M | 6.0 | 2.0 | 2.0 | 0.085 | 34 | 3.4 | 2 | <0.001 | 2.71 | 1.85 | 2.35 | 0.011 |
| 2 | 45 | M | 2.0 | 2.0 | 2.0 | 308 | 183 | 165 | 2.39 | 1.32 | 1.71 | |||
| 3 | 55 | F | 3.0 | 2.0 | 2.0 | 109 | 67 | 17.3 | 5.58 | 2.04 | 2.07 | |||
| 4 | 44 | F | 2.0 | 10.0 | 5.0 | 211 | 193.5 | 135 | 2.68 | 2.61 | 1.52 | |||
| 5 | 28 | F | 15.4 | 21.8 | 7.5 | 68.3 | 23.5 | 170 | 1.75 | 2.17 | 0.98 | |||
| 6 | 49 | M | 17.0 | 75.8 | 12.1 | 97 | 28.2 | 8.8 | 5.23 | 7.36 | 4.27 | |||
| 7 | 44 | F | 59.5 | 13.6 | 2.0 | 5.8 | 3 | 2 | 2.30 | 2.39 | 1.44 | |||
| 8 | 42 | F | 23.0 | 35.0 | 6.0 | 175 | 144 | 22.8 | 2.12 | 2.46 | 2.07 | |||
| 9 | 54 | F | 2.0 | 2.0 | 2.0 | 34.2 | 17.1 | 2 | 3.28 | 3.22 | 2.88 | |||
| 10 | 30 | F | 4.7 | 3.2 | 3.4 | 70 | 68.5 | 21.4 | 0.78 | 1.05 | 0.62 | |||
| Pts | Cd4 (%) Baseline | CD4 (%) End of RTX | CD4 (%) 6 mo. after RTX | p-Value | CD8 (%) Baseline | CD8 (%) End of RTX | CD8 (%) 6 mo. after RTX | p-Value | CD20 (%) Baseline | CD20 (%) End of RTX | CD20 (%) 6 mo. after RTX | p-Value | ||
| 1 | 46 | 48 | 47 | 0.081 | 17 | 26 | 20 | 0.009 | 5 | 0 | 0 | <0.001 | ||
| 2 | 55 | 37 | 53 | 23 | 28 | 31 | 5 | 0 | 0 | |||||
| 3 | 67 | 53 | 60 | 12 | 26 | 29 | 5 | 0 | 0 | |||||
| 4 | 67 | 60 | 44 | 25 | 23 | 29 | 8 | 0 | 8 | |||||
| 5 | 42 | 52 | 40 | 24 | 24 | 41 | 3 | 0 | 0 | |||||
| 6 | 68 | 81 | 64 | 13 | 11 | 15 | 10 | 0 | 0 | |||||
| 7 | 53 | 67 | 46 | 23 | 28 | 32 | 12 | 0 | 2 | |||||
| 8 | 55 | 64 | 56 | 26 | 26 | 27 | 6 | 0 | 0 | |||||
| 9 | 59 | 58 | 49 | 18 | 18 | 17 | 4 | 0 | 0 | |||||
| 10 | 31 | 44 | 31 | 40 | 42 | 50 | 4 | 0 | 2 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fortuna, G.; Calabria, E.; Aria, M.; Giudice, A.; Mignogna, M.D. Immunocytometric Analysis of Oral Pemphigus vulgaris Patients after Treatment with Rituximab as Adjuvant. Biomolecules 2021, 11, 1634. https://doi.org/10.3390/biom11111634
Fortuna G, Calabria E, Aria M, Giudice A, Mignogna MD. Immunocytometric Analysis of Oral Pemphigus vulgaris Patients after Treatment with Rituximab as Adjuvant. Biomolecules. 2021; 11(11):1634. https://doi.org/10.3390/biom11111634
Chicago/Turabian StyleFortuna, Giulio, Elena Calabria, Massimo Aria, Amerigo Giudice, and Michele Davide Mignogna. 2021. "Immunocytometric Analysis of Oral Pemphigus vulgaris Patients after Treatment with Rituximab as Adjuvant" Biomolecules 11, no. 11: 1634. https://doi.org/10.3390/biom11111634
APA StyleFortuna, G., Calabria, E., Aria, M., Giudice, A., & Mignogna, M. D. (2021). Immunocytometric Analysis of Oral Pemphigus vulgaris Patients after Treatment with Rituximab as Adjuvant. Biomolecules, 11(11), 1634. https://doi.org/10.3390/biom11111634