
Effects of the Menstrual Cycle and Hormonal Contraceptive Use on Metabolic Outcomes, Strength Performance, and Recovery: A Narrative Review




Abstract
1. Introduction
1.1. Aims and Methods of the Narrative Review
1.2. Overview of the Eumenorrheic Menstrual Cycle
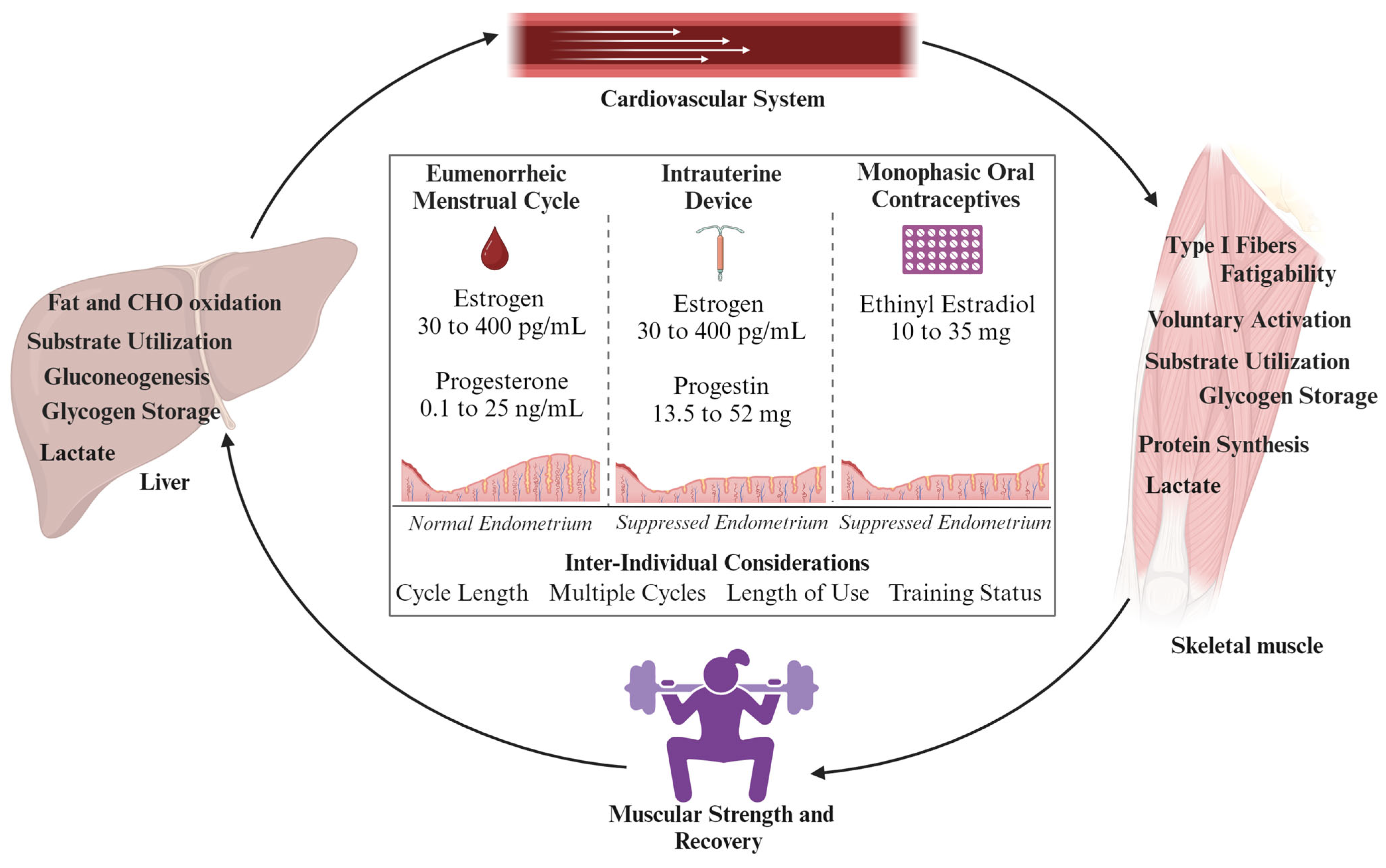
1.3. Overview of Common Hormonal Contraception Methods
2. Defining Metabolic Outcomes in Females: Key Hormonal Considerations
2.1. Substrate Utilization and Female Sex Hormones
2.2. Resting Energy Expenditure and Female Sex Hormones
2.3. Protein Synthesis and Female Sex Hormones
3. Defining Muscular Strength and Power in Females
3.1. Maximal Strength and the Hormone Cycle
3.2. Isometric Dynamometer and the Hormone Cycle
3.3. Muscular Power and the Hormone Cycle
4. Overview of Recovery in Females
4.1. Recovery and the Menstrual Cycle
4.2. Recovery and Hormonal Contraception
5. Limitations and Future Considerations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McNulty, K.L.; Elliott-Sale, K.J.; Dolan, E.; Swinton, P.A.; Ansdell, P.; Goodall, S.; Thomas, K.; Hicks, K.M. The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 1813–1827. [Google Scholar] [CrossRef] [PubMed]
- Pereira, H.M.; Larson, R.D.; Bemben, D.A. Menstrual Cycle Effects on Exercise-Induced Fatigability. Front. Physiol. 2020, 11, 517. [Google Scholar] [CrossRef]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Wycherley, T.P. The Impact of Menstrual Cycle Phase on Athletes’ Performance: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1667. [Google Scholar] [CrossRef]
- Kavanaugh, M.L.; Jerman, J. Contraceptive Method Use in the United States: Trends and Characteristics between 2008, 2012 and 2014. Contraception 2018, 97, 14–21. [Google Scholar] [CrossRef]
- Martin, D.; Sale, C.; Cooper, S.B.; Elliott-Sale, K.J. Period Prevalence and Perceived Side Effects of Hormonal Contraceptive Use and the Menstrual Cycle in Elite Athletes. Int. J. Sports Physiol. Perform. 2018, 13, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Henderson, Z.; Scribbans, T. Intrauterine Contraception and Athletic Performance. Health Fit. J. Can. 2020, 13, 37–45. [Google Scholar] [CrossRef]
- Cabre, H.E.; Ladan, A.N.; Moore, S.R.; Joniak, K.E.; Blue, M.N.M.; Pietrosimone, B.G.; Hackney, A.C.; Smith-Ryan, A.E. Effects of Hormonal Contraception and the Menstrual Cycle on Fatigability and Recovery From an Anaerobic Exercise Test. J. Strength Cond. Res. 2024, 38, 1256–1265. [Google Scholar] [CrossRef]
- Kitajima, Y.; Ono, Y. Estrogens Maintain Skeletal Muscle and Satellite Cell Functions. J. Endocrinol. 2016, 229, 267–275. [Google Scholar] [CrossRef]
- Enns, D.L.; Tiidus, P.M. The Influence of Estrogen on Skeletal Muscle: Sex Matters. Sports Med. 2010, 40, 41–58. [Google Scholar] [CrossRef]
- Van Pelt, R.E.; Gavin, K.M.; Kohrt, W.M. Regulation of Body Composition and Bioenergetics by Estrogens. Endocrinol. Metab. Clin. N. Am. 2015, 44, 663–676. [Google Scholar] [CrossRef]
- Wiik, A.; Ekman, M.; Johansson, O.; Jansson, E.; Esbjörnsson, M. Expression of Both Oestrogen Receptor Alpha and Beta in Human Skeletal Muscle Tissue. Histochem. Cell Biol. 2009, 131, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Wohlgemuth, K.J.; Arieta, L.R.; Brewer, G.J.; Hoselton, A.L.; Gould, L.M.; Smith-Ryan, A.E. Sex Differences and Considerations for Female Specific Nutritional Strategies: A Narrative Review. J. Int. Soc. Sports Nutr. 2021, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Rettberg, J.R.; Yao, J.; Brinton, R.D. Estrogen: A Master Regulator of Bioenergetic Systems in the Brain and Body. Front. Neuroendocrinol. 2014, 35, 8–30. [Google Scholar] [CrossRef]
- Lebrun, C.M.; McKenzie, D.C.; Prior, J.C.; Taunton, J.E. Effects of Menstrual Cycle Phase on Athletic Performance. Med. Sci. Sports Exerc. 1995, 27, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Romero-Moraleda, B.; Coso, J.D.; Gutiérrez-Hellín, J.; Ruiz-Moreno, C.; Grgic, J.; Lara, B. The Influence of the Menstrual Cycle on Muscle Strength and Power Performance. J. Hum. Kinet. 2019, 68, 123–133. [Google Scholar] [CrossRef]
- Sarwar, R.; Niclos, B.B.; Rutherford, O.M. Changes in Muscle Strength, Relaxation Rate and Fatiguability during the Human Menstrual Cycle. J. Physiol. 1996, 493, 267–272. [Google Scholar] [CrossRef]
- Phillips, S.K.; Sanderson, A.G.; Birch, K.; Bruce, S.A.; Woledge, R.C. Changes in Maximal Voluntary Force of Human Adductor Pollicis Muscle during the Menstrual Cycle. J. Physiol. 1996, 496, 551–557. [Google Scholar] [CrossRef]
- Haines, M.; McKinley-Barnard, S.K.; Andre, T.L.; Gann, J.J.; Hwang, P.S.; Willoughby, D.S. Skeletal Muscle Estrogen Receptor Activation in Response to Eccentric Exercise Up-Regulates Myogenic-Related Gene Expression Independent of Differing Serum Estradiol Levels Occurring during the Human Menstrual Cycle. J. Sports Sci. Med. 2018, 17, 31–39. [Google Scholar] [PubMed]
- Sung, E.; Han, A.; Hinrichs, T.; Vorgerd, M.; Manchado, C.; Platen, P. Effects of Follicular versus Luteal Phase-Based Strength Training in Young Women. SpringerPlus 2014, 3, 668. [Google Scholar] [CrossRef]
- Elliott-Sale, K.J.; McNulty, K.L.; Ansdell, P.; Goodall, S.; Hicks, K.M.; Thomas, K.; Swinton, P.A.; Dolan, E. The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-Analysis. Sports Med. Auckl. NZ 2020, 50, 1785–1812. [Google Scholar] [CrossRef]
- Blagrove, R.C.; Bruinvels, G.; Pedlar, C.R. Variations in Strength-Related Measures during the Menstrual Cycle in Eumenorrheic Women: A Systematic Review and Meta-Analysis. J. Sci. Med. Sport 2020, 23, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Cowley, E.S.; Olenick, A.A.; McNulty, K.L.; Ross, E.Z. “Invisible Sportswomen”: The Sex Data Gap in Sport and Exercise Science Research. Women Sport Phys. Act. J. 2021, 29, 146–151. [Google Scholar] [CrossRef]
- Oosthuyse, T.; Bosch, A.N. The Effect of the Menstrual Cycle on Exercise Metabolism: Implications for Exercise Performance in Eumenorrhoeic Women. Sports Med. 2010, 40, 207–227. [Google Scholar] [CrossRef] [PubMed]
- Draper, C.F.; Duisters, K.; Weger, B.; Chakrabarti, A.; Harms, A.C.; Brennan, L.; Hankemeier, T.; Goulet, L.; Konz, T.; Martin, F.P.; et al. Menstrual Cycle Rhythmicity: Metabolic Patterns in Healthy Women. Sci. Rep. 2018, 8, 14568. [Google Scholar] [CrossRef] [PubMed]
- Elliott-Sale, K.J.; Minahan, C.L.; de Jonge, X.A.K.J.; Ackerman, K.E.; Sipilä, S.; Constantini, N.W.; Lebrun, C.M.; Hackney, A.C. Methodological Considerations for Studies in Sport and Exercise Science with Women as Participants: A Working Guide for Standards of Practice for Research on Women. Sports Med. 2021, 51, 843–861. [Google Scholar] [CrossRef]
- Myllyaho, M.M.; Ihalainen, J.K.; Hackney, A.C.; Valtonen, M.; Nummela, A.; Vaara, E.; Häkkinen, K.; Kyröläinen, H.; Taipale, R.S. Hormonal Contraceptive Use Does Not Affect Strength, Endurance, or Body Composition Adaptations to Combined Strength and Endurance Training in Women. J. Strength Cond. Res. 2021, 35, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.; White, S.; Crossley, K. The Oral Contraceptive Pill: A Revolution for Sportswomen? Br. J. Sports Med. 1999, 33, 231–238. [Google Scholar] [CrossRef]
- Rickenlund, A.; Carlström, K.; Ekblom, B.; Brismar, T.B.; von Schoultz, B.; Hirschberg, A.L. Effects of Oral Contraceptives on Body Composition and Physical Performance in Female Athletes. J. Clin. Endocrinol. Metab. 2004, 89, 4364–4370. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. National Survey of Family Growth, 2017–2019; National Center for Health Statistics: Quincy, MA, USA, 2022. [Google Scholar]
- Cooper, D.B.; Patel, P.; Mahdy, H. Oral Contraceptive Pills. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Regidor, P.-A. The Clinical Relevance of Progestogens in Hormonal Contraception: Present Status and Future Developments. Oncotarget 2018, 9, 34628–34638. [Google Scholar] [CrossRef] [PubMed]
- Xiao, B.; Zeng, T.; Wu, S.; Sun, H.; Xiao, N. Effect of Levonorgestrel-Releasing Intrauterine Device on Hormonal Profile and Menstrual Pattern after Long-Term Use. Contraception 1995, 51, 359–365. [Google Scholar] [CrossRef]
- Tostes, R.C.; Nigro, D.; Fortes, Z.B.; Carvalho, M.H.C. Effects of Estrogen on the Vascular System. Braz. J. Med. Biol. Res. 2003, 36, 1143–1158. [Google Scholar] [CrossRef]
- Oosthuyse, T.; Strauss, J.A.; Hackney, A.C. Understanding the Female Athlete: Molecular Mechanisms Underpinning Menstrual Phase Differences in Exercise Metabolism. Eur. J. Appl. Physiol. 2023, 123, 423–450. [Google Scholar] [CrossRef]
- Moore, D.R.; Sygo, J.; Morton, J.P. Fuelling the Female Athlete: Carbohydrate and Protein Recommendations. Eur. J. Sport Sci. 2021, 22, 684–696. [Google Scholar] [CrossRef]
- Willett, H.N.; Koltun, K.J.; Hackney, A.C. Influence of Menstrual Cycle Estradiol-β-17 Fluctuations on Energy Substrate Utilization-Oxidation during Aerobic, Endurance Exercise. Int. J. Environ. Res. Public Health 2021, 18, 7209. [Google Scholar] [CrossRef]
- Hackney, A.C.; McCracken-Compton, M.A.; Ainsworth, B. Substrate Responses to Submaximal Exercise in the Midfollicular and Midluteal Phases of the Menstrual Cycle. Int. J. Sport Nutr. 1994, 4, 299–308. [Google Scholar] [CrossRef]
- Oosthuyse, T.; Bosch, A.N. Oestrogen’s Regulation of Fat Metabolism during Exercise and Gender Specific Effects. Curr. Opin. Pharmacol. 2012, 12, 363–371. [Google Scholar] [CrossRef]
- Hackney, A.C. Menstrual Cycle Hormonal Changes and Energy Substrate Metabolism in Exercising Women: A Perspective. Int. J. Environ. Res. Public Health 2021, 18, 10024. [Google Scholar] [CrossRef]
- Davis, H.C.; Hackney, A.C. The Hypothalamic–Pituitary–Ovarian Axis and Oral Contraceptives: Regulation and Function. In Sex Hormones, Exercise and Women; Hackney, A.C., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–17. ISBN 978-3-319-44557-1. [Google Scholar]
- Hargreaves, M.; Spriet, L.L. Skeletal Muscle Energy Metabolism during Exercise. Nat. Metab. 2020, 2, 817–828. [Google Scholar] [CrossRef]
- Kaminski, J.; Junior, C.M.; Pavesi, H.; Drobrzenski, B.; Amaral, G.M.D. Effects of Oral versus Transdermal Estradiol plus Micronized Progesterone on Thyroid Hormones, Hepatic Proteins, Lipids, and Quality of Life in Menopausal Women with Hypothyroidism: A Clinical Trial. Menopause 2021, 28, 1044–1052. [Google Scholar] [CrossRef]
- Ignacio, D.L.; Da S Silvestre, D.H.; Cavalcanti-de-Albuquerque, J.P.A.; Louzada, R.A.; Carvalho, D.P.; Werneck-de-Castro, J.P. Thyroid Hormone and Estrogen Regulate Exercise-Induced Growth Hormone Release. PLoS ONE 2015, 10, e0122556. [Google Scholar] [CrossRef]
- Isacco, L.; Duché, P.; Boisseau, N. Influence of Hormonal Status on Substrate Utilization at Rest and during Exercise in the Female Population. Sports Med. 2012, 42, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Bisdee, J.T.; James, W.P.T.; Shaw, M.A. Changes in Energy Expenditure during the Menstrual Cycle. Br. J. Nutr. 1989, 61, 187–199. [Google Scholar] [CrossRef]
- Benton, M.J.; Hutchins, A.M.; Dawes, J.J. Effect of Menstrual Cycle on Resting Metabolism: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0236025. [Google Scholar] [CrossRef] [PubMed]
- Day, D.S.; Gozansky, W.S.; Van Pelt, R.E.; Schwartz, R.S.; Kohrt, W.M. Sex Hormone Suppression Reduces Resting Energy Expenditure and {beta}-Adrenergic Support of Resting Energy Expenditure. J. Clin. Endocrinol. Metab. 2005, 90, 3312–3317. [Google Scholar] [CrossRef]
- Cabre, H.; Moore, S.; Smith-Ryan, A.; Hackney, A. Relative Energy Deficiency in Sport (RED-S): Scientific, Clinical, Andpractical Implications for the Female Athlete. Dtsch. Z. Für Sportmed. J. Sports Med. 2022, 73, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Kimm, S.Y.S. Effects of Race, Cigarette Smoking, and Use of Contraceptive Medications on Resting Energy Expenditure in Young Women. Am. J. Epidemiol. 2001, 154, 718–724. [Google Scholar] [CrossRef]
- Eck, L.H.; Bennett, A.G.; Egan, B.M.; Ray, J.W.; Mitchell, C.O.; Smith, M.A.; Klesges, R.C. Differences in Macronutrient Selections in Users and Nonusers of an Oral Contraceptive. Am. J. Clin. Nutr. 1997, 65, 419–424. [Google Scholar] [CrossRef]
- Diffey, B.; Piers, L.S.; Soares, M.J.; O’dea, K. The Effect of Oral Contraceptive Agents on the Basal Metabolic Rate of Young Women. Br. J. Nutr. 1997, 77, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, A.; Zanin, R.; Palma, F.; Romani, C.; Grandi, G.; Di Carlo, C.; Cagnacci, A. Body Composition and Resting Metabolic Rate of Perimenopausal Women Using Continuous Progestogen Contraception. Eur. J. Contracept. Reprod. Health Care 2016, 21, 168–175. [Google Scholar] [CrossRef]
- Duhita, M.R.; Schutz, Y.; Montani, J.-P.; Dulloo, A.G.; Miles-Chan, J.L. Oral Contraceptive Pill Alters Acute Dietary Protein-Induced Thermogenesis in Young Women: Acute Protein-Induced Thermogenesis in Young Women. Obesity 2017, 25, 1482–1485. [Google Scholar] [CrossRef]
- Jensen, M.D.; Levine, J. Effects of Oral Contraceptives on Free Fatty Acid Metabolism in Women. Metabolism 1998, 47, 280–284. [Google Scholar] [CrossRef]
- Church, D.D.; Hirsch, K.R.; Park, S.; Kim, I.-Y.; Gwin, J.A.; Pasiakos, S.M.; Wolfe, R.R.; Ferrando, A.A. Essential Amino Acids and Protein Synthesis: Insights into Maximizing the Muscle and Whole-Body Response to Feeding. Nutrients 2020, 12, 3717. [Google Scholar] [CrossRef]
- Kriengsinyos, W.; Wykes, L.J.; Goonewardene, L.A.; Ball, R.O.; Pencharz, P.B. Phase of Menstrual Cycle Affects Lysine Requirement in Healthy Women. Am. J. Physiol.-Endocrinol. Metab. 2004, 287, E489–E496. [Google Scholar] [CrossRef]
- Hamadeh, M.J.; Devries, M.C.; Tarnopolsky, M.A. Estrogen Supplementation Reduces Whole Body Leucine and Carbohydrate Oxidation and Increases Lipid Oxidation in Men during Endurance Exercise. J. Clin. Endocrinol. Metab. 2005, 90, 3592–3599. [Google Scholar] [CrossRef]
- Miller, B.F.; Hansen, M.; Olesen, J.L.; Flyvbjerg, A.; Schwarz, P.; Babraj, J.A.; Smith, K.; Rennie, M.J.; Kjaer, M. No Effect of Menstrual Cycle on Myofibrillar and Connective Tissue Protein Synthesis in Contracting Skeletal Muscle. Am. J. Physiol.-Endocrinol. Metab. 2006, 290, E163–E168. [Google Scholar] [CrossRef]
- Hansen, M.; Langberg, H.; Holm, L.; Miller, B.F.; Petersen, S.G.; Doessing, S.; Skovgaard, D.; Trappe, T.; Kjaer, M. Effect of Administration of Oral Contraceptives on the Synthesis and Breakdown of Myofibrillar Proteins in Young Women: Effect of OC on Muscle Protein Turnover. Scand. J. Med. Sci. Sports 2011, 21, 62–72. [Google Scholar] [CrossRef]
- Lariviere, F.; Moussalli, R.; Garrel, D.R. Increased Leucine Flux and Leucine Oxidation during the Luteal Phase of the Menstrual Cycle in Women. Am. J. Physiol.-Endocrinol. Metab. 1994, 267, E422–E428. [Google Scholar] [CrossRef]
- Dave, H.; Shook, M.; Varacallo, M. Anatomy, Skeletal Muscle. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Grgic, J.; Lazinica, B.; Schoenfeld, B.J.; Pedisic, Z. Test-Retest Reliability of the One-Repetition Maximum (1RM) Strength Assessment: A Systematic Review. Sports Med.-Open 2020, 6, 31. [Google Scholar] [CrossRef]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological Sex Differences Affect the Integrative Response to Exercise: Acute and Chronic Implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef]
- Tarnopolsky, M.A. Gender Differences in Substrate Metabolism During Endurance Exercise. Can. J. Appl. Physiol. 2000, 25, 312–327. [Google Scholar] [CrossRef]
- Hunter, S.K.; Angadi, S.S.; Bhargava, A.; Harper, J.; Hirschberg, A.L.; Levine, B.D.; Moreau, K.L.; Nokoff, N.J.; Stachenfeld, N.S.; Bermon, S. The Biological Basis of Sex Differences in Athletic Performance: Consensus Statement for the American College of Sports Medicine. Transl. J. Am. Coll. Sports Med. 2023, 8, 1–33. [Google Scholar] [CrossRef]
- Tarnopolsky, M.A.; Rennie, C.D.; Robertshaw, H.A.; Fedak-Tarnopolsky, S.N.; Devries, M.C.; Hamadeh, M.J. Influence of Endurance Exercise Training and Sex on Intramyocellular Lipid and Mitochondrial Ultrastructure, Substrate Use, and Mitochondrial Enzyme Activity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R1271–R1278. [Google Scholar] [CrossRef]
- Dulhunty, A. Excitation-Contraction Coupling from the 1950s into the New Millennium. Clin. Exp. Pharmacol. Physiol. 2006, 33, 763–772. [Google Scholar] [CrossRef]
- Meeusen, R.; Roelands, B. Fatigue: Is It All Neurochemistry? Eur. J. Sport Sci. 2018, 18, 37–46. [Google Scholar] [CrossRef]
- Hunter, S.K. Sex Differences in Fatigability of Dynamic Contractions: Sex Differences in Skeletal Muscle Fatigue. Exp. Physiol. 2016, 101, 250–255. [Google Scholar] [CrossRef]
- Stoffel-Wagner, B. Neurosteroid Metabolism in the Human Brain. Eur. J. Endocrinol. 2001, 145, 669–679. [Google Scholar] [CrossRef]
- Ansdell, P.; Brownstein, C.G.; Škarabot, J.; Hicks, K.M.; Simoes, D.C.M.; Thomas, K.; Howatson, G.; Hunter, S.K.; Goodall, S. Menstrual Cycle-Associated Modulations in Neuromuscular Function and Fatigability of the Knee Extensors in Eumenorrheic Women. J. Appl. Physiol. 2019, 126, 1701–1712. [Google Scholar] [CrossRef]
- Birch, K.; Reilly, T. The diurnal rhythm in isometric muscular performance differs with eumenorrheic menstrual cycle phase. Chronobiol. Int. 2002, 19, 731–742. [Google Scholar] [CrossRef]
- Tenan, M.S.; Hackney, A.C.; Griffin, L. Maximal Force and Tremor Changes across the Menstrual Cycle. Eur. J. Appl. Physiol. 2016, 116, 153–160. [Google Scholar] [CrossRef]
- Kraemer, W.; Ratamess, N.; Fry, A.; French, D.; Maud, P.; Foster, C. Strength Testing: Development and Evaluation of Methodology; Human Kinetics: Champaign, IL, USA, 2006. [Google Scholar]
- Zazulak, B.T.; Paterno, M.; Myer, G.D.; Romani, W.A.; Hewett, T.E. The Effects of the Menstrual Cycle on Anterior Knee Laxity: A Systematic Review. Sports Med. 2006, 36, 847–862. [Google Scholar] [CrossRef]
- Ekenros, L.; Hirschberg, A.L.; Heijne, A.; Fridén, C. Oral Contraceptives Do Not Affect Muscle Strength and Hop Performance in Active Women. Clin. J. Sport Med. 2013, 23, 202–207. [Google Scholar] [CrossRef]
- Giacomoni, M.; Bernard, T.; Gavarry, O.; Altare, S.; Falgairette, G. Influence of the Menstrual Cycle Phase and Menstrual Symptoms on Maximal Anaerobic Performance. Med. Sci. Sports Exerc. 2000, 32, 486. [Google Scholar] [CrossRef]
- Nichols, A.W.; Hetzler, R.K.; Villanueva, R.J.; Stickley, C.D.; Kimura, I.F. Effects of Combination Oral Contraceptives on Strength Development in Women Athletes. J. Strength Cond. Res. 2008, 22, 1625–1632. [Google Scholar] [CrossRef]
- Elliott, K.J. Does Oral Contraceptive Use Affect Maximum Force Production in Women? Br. J. Sports Med. 2005, 39, 15–19. [Google Scholar] [CrossRef]
- Rechichi, C.; Dawson, B. Effect of Oral Contraceptive Cycle Phase on Performance in Team Sport Players. J. Sci. Med. Sport 2009, 12, 190–195. [Google Scholar] [CrossRef]
- Phillips, S.K.; Rook, K.M.; Siddle, N.C.; Bruce, S.A.; Woledge, R.C. Muscle Weakness in Women Occurs at an Earlier Age than in Men, but Strength Is Preserved by Hormone Replacement Therapy. Clin. Sci. 1993, 84, 95–98. [Google Scholar] [CrossRef]
- Montgomery, M.M.; Shultz, S.J. Isometric Knee-Extension and Knee-Flexion Torque Production During Early Follicular and Postovulatory Phases in Recreationally Active Women. J. Athl. Train. 2010, 45, 586–593. [Google Scholar] [CrossRef]
- Fisher, A.L. Models of Sarcopenia. In Handbook of Models for Human Aging; Elsevier: Amsterdam, The Netherlands, 2006; pp. 977–991. ISBN 978-0-12-369391-4. [Google Scholar]
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and Performance in Sport: Consensus Statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef]
- Beltrame, T.; Villar, R.; Hughson, R.L. Sex Differences in the Oxygen Delivery, Extraction, and Uptake during Moderate-Walking Exercise Transition. Appl. Physiol. Nutr. Metab. 2017, 42, 994–1000. [Google Scholar] [CrossRef]
- Russ, D.W.; Lanza, I.R.; Rothman, D.; Kent-Braun, J.A. Sex Differences in Glycolysis during Brief, Intense Isometric Contractions. Muscle Nerve 2005, 32, 647–655. [Google Scholar] [CrossRef]
- Solleiro Pons, M.; Bernert, L.; Hume, E.; Hughes, L.; Williams, Z.; Burnley, M.; Ansdell, P. No Sex Differences in Oxygen Uptake or Extraction Kinetics in the Moderate or Heavy Exercise Intensity Domains. J. Appl. Physiol. 2024, 136, 472–481. [Google Scholar] [CrossRef]
- Ansdell, P.; Brownstein, C.G.; Škarabot, J.; Hicks, K.M.; Howatson, G.; Thomas, K.; Hunter, S.K.; Goodall, S. Sex Differences in Fatigability and Recovery Relative to the Intensity–Duration Relationship. J. Physiol. 2019, 597, 5577–5595. [Google Scholar] [CrossRef]
- Azevedo, M.R.; Araújo, C.L.P.; Reichert, F.F.; Siqueira, F.V.; da Silva, M.C.; Hallal, P.C. Gender Differences in Leisure-Time Physical Activity. Int. J. Public Health 2007, 52, 8–15. [Google Scholar] [CrossRef]
- Ansdell, P.; Škarabot, J.; Atkinson, E.; Corden, S.; Tygart, A.; Hicks, K.M.; Thomas, K.; Hunter, S.K.; Howatson, G.; Goodall, S. Sex Differences in Fatigability Following Exercise Normalised to the Power–Duration Relationship. J. Physiol. 2020, 598, 5717–5737. [Google Scholar] [CrossRef]
- Borne, R.; Hausswirth, C.; Bieuzen, F. Relationship Between Blood Flow and Performance Recovery: A Randomized, Placebo-Controlled Study. Int. J. Sports Physiol. Perform. 2017, 12, 152–160. [Google Scholar] [CrossRef]
- Malone, J.K.; Coughlan, G.F.; Crowe, L.; Gissane, G.C.; Caulfield, B. The Physiological Effects of Low-Intensity Neuromuscular Electrical Stimulation (NMES) on Short-Term Recovery from Supra-Maximal Exercise Bouts in Male Triathletes. Eur. J. Appl. Physiol. 2012, 112, 2421–2432. [Google Scholar] [CrossRef]
- Parker, B.A.; Smithmyer, S.L.; Pelberg, J.A.; Mishkin, A.D.; Herr, M.D.; Proctor, D.N. Sex Differences in Leg Vasodilation during Graded Knee Extensor Exercise in Young Adults. J. Appl. Physiol. 2007, 103, 1583–1591. [Google Scholar] [CrossRef]
- Roepstorff, C.; Thiele, M.; Hillig, T.; Pilegaard, H.; Richter, E.A.; Wojtaszewski, J.F.P.; Kiens, B. Higher Skeletal Muscle α 2 AMPK Activation and Lower Energy Charge and Fat Oxidation in Men than in Women during Submaximal Exercise: Sex Difference in AMPK Activation by Exercise. J. Physiol. 2006, 574, 125–138. [Google Scholar] [CrossRef]
- Korthuis, R.J. Skeltal Muscle Circulation; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2011. [Google Scholar]
- Tiidus, P.M. Influence of Estrogen on Skeletal Muscle Damage, Inflammation, and Repair. Exerc. Sport Sci. Rev. 2003, 31, 40–44. [Google Scholar] [CrossRef]
- Hackney, A.C.; Kallman, A.L.; Ağgön, E. Female Sex Hormones and the Recovery from Exercise: Menstrual Cycle Phase Affects Responses. Biomed. Hum. Kinet. 2019, 11, 87–89. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Barba-Moreno, L.; Rael, B.; Alfaro-Magallanes, V.M.; Cupeiro, R.; Díaz, Á.E.; Calderón, F.J.; Peinado, A.B. Influence of the Menstrual Cycle on Blood Markers of Muscle Damage and Inflammation Following Eccentric Exercise. Int. J. Environ. Res. Public Health 2020, 17, 1618. [Google Scholar] [CrossRef]
- Markofski, M.M.; Braun, W.A. Influence of Menstrual Cycle on Indices of Contraction-Induced Muscle Damage. J. Strength Cond. Res. 2014, 28, 2649–2656. [Google Scholar] [CrossRef]
- Chaffin, M.E.; Berg, K.E.; Meendering, J.R.; Llewellyn, T.L.; French, J.A.; Davis, J.E. Interleukin-6 and Delayed Onset Muscle Soreness Do Not Vary During the Menstrual Cycle. Res. Q. Exerc. Sport 2011, 82, 693–701. [Google Scholar] [CrossRef]
- Tsampoukos, A.; Peckham, E.A.; James, R.; Nevill, M.E. Effect of Menstrual Cycle Phase on Sprinting Performance. Eur. J. Appl. Physiol. 2010, 109, 659–667. [Google Scholar] [CrossRef]
- Middleton, L.E.; Wenger, H.A. Effects of Menstrual Phase on Performance and Recovery in Intense Intermittent Activity. Eur. J. Appl. Physiol. 2006, 96, 53–58. [Google Scholar] [CrossRef]
- Lara, B.; Gutiérrez Hellín, J.; Ruíz-Moreno, C.; Romero-Moraleda, B.; Del Coso, J. Acute Caffeine Intake Increases Performance in the 15-s Wingate Test during the Menstrual Cycle. Br. J. Clin. Pharmacol. 2020, 86, 745–752. [Google Scholar] [CrossRef]
- Štefanovský, M.; Péterová, A.; Vanderka, M.; Lengvarský, L. Influence of Selected Phases of the Menstrual Cycle on Performance in Special Judo Fitness Test and Wingate Test. Acta Gymnica 2016, 46, 136–142. [Google Scholar] [CrossRef]
- Minahan, C.; Melnikoff, M.; Quinn, K.; Larsen, B. Response of Women Using Oral Contraception to Exercise in the Heat. Eur. J. Appl. Physiol. 2017, 117, 1383–1391. [Google Scholar] [CrossRef]
- Williams, J.S.; Dunford, E.C.; MacDonald, M.J. Impact of the Menstrual Cycle on Peripheral Vascular Function in Premenopausal Women: Systematic Review and Meta-Analysis. Am. J. Physiol.-Heart Circ. Physiol. 2020, 319, H1327–H1337. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.S.; MacDonald, M.J. Influence of Hormonal Contraceptives on Peripheral Vascular Function and Structure in Premenopausal Females: A Review. Am. J. Physiol.-Heart Circ. Physiol. 2021, 320, H77–H89. [Google Scholar] [CrossRef] [PubMed]
- Angstwurm, M.W.A.; Gärtner, R.; Ziegler-Heitbrock, H.W.L. Cyclic Plasma IL-6 Levels During Normal Menstrual Cycle. Cytokine 1997, 9, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.; Paton, B.; Poole, L.; Sun, W.; Ferguson, C.; Wilson, J.; Kemi, O.J. Blood Lactate Clearance after Maximal Exercise Depends on Active Recovery Intensity. J. Sports Med. Phys. Fitness 2014, 54, 271–278. [Google Scholar]
- Sims, S.T.; Ware, L.; Capodilupo, E.R. Patterns of Endogenous and Exogenous Ovarian Hormone Modulation on Recovery Metrics across the Menstrual Cycle. BMJ Open Sport Exerc. Med. 2021, 7, e001047. [Google Scholar] [CrossRef] [PubMed]
- Cauci, S.; Francescato, M.P.; Curcio, F. Combined Oral Contraceptives Increase High-Sensitivity C-Reactive Protein but Not Haptoglobin in Female Athletes. Sports Med. 2017, 47, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Dreon, D.M.; Slavin, J.L.; Phinney, S.D. Oral Contraceptive Use and Increased Plasma Concentration of C-Reactive Protein. Life Sci. 2003, 73, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Meulenberg, P.M.M.; Ross, H.A.; Swinkels, L.M.J.W.; Benraad, T.J. The Effect of Oral Contraceptives on Plasma-Free and Salivary Cortisol and Cortisone. Clin. Chim. Acta 1987, 165, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Bozzini, B.N.; McFadden, B.A.; Elliott-Sale, K.J.; Swinton, P.A.; Arent, S.M. Evaluating the Effects of Oral Contraceptive Use on Biomarkers and Body Composition during a Competitive Season in Collegiate Female Soccer Players. J. Appl. Physiol. 2021, 130, 1971–1982. [Google Scholar] [CrossRef] [PubMed]
- Najmabadi, S.; Schliep, K.C.; Simonsen, S.E.; Porucznik, C.A.; Egger, M.J.; Stanford, J.B. Menstrual Bleeding, Cycle Length, and Follicular and Luteal Phase Lengths in Women without Known Subfertility: A Pooled Analysis of Three Cohorts. Paediatr. Perinat. Epidemiol. 2020, 34, 318–327. [Google Scholar] [CrossRef]
- Bansode, O.M.; Sarao, M.S.; Cooper, D.B. Contraception. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Montalvo, A.M.; Tse-Dinh, Y.-C.; Liu, Y.; Swartzon, M.; Hechtman, K.S.; Myer, G.D. Precision Sports Medicine: The Future of Advancing Health and Performance in Youth and Beyond. Strength Cond. J. 2017, 39, 48–58. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Metabolic Monitoring for Military Field Applications. The Study of Individual Differences: Statistical Approaches to Inter- and Intraindividual Variability. In Monitoring Metabolic Status: Predicting Decrements in Physiological and Cognitive Performance; National Academies Press: Washington, DC, USA, 2004; Volume 2. [Google Scholar]
- Treloar, A.E.; Boynton, R.E.; Behn, B.G.; Brown, B.W. Variation of the Human Menstrual Cycle through Reproductive Life. Int. J. Fertil. 1967, 12, 77–126. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| EUM Females Compared to Females Using HC | |||||
|---|---|---|---|---|---|
| Source | Outcome | EUM Females | Hormonal Contraceptive Users | n | |
| Myllyaho et al. [26] | Maximal Strength and Isometric/Isokinetic Contractability “ “ “ | ↔ | ↔ | EUM: 9 HC: 9 | |
| Nichols et al. [78] | ↔ | ↔ | EUM: 18 OC: 13 | ||
| Elliott et al. [79] | ↔ | ↔ | EUM: 7 OC: 14 | ||
| Ekenros et al. [76] | ↔ | ↔ | EUM: 9 OC: 8 | ||
| Giacomoni et al. [77] | Muscular Power | ↔ | ↔ | EUM: 7 OC: 10 | |
| EUM Females across the Menstrual Cycle | |||||
| Source | Outcome | Follicular Phase | Late Follicular/Ovulatory Phase | Luteal Phase | n |
| Ekenros et al. [76] | Isometric/Isokinetic Contractability Muscular Strength | ↔ | ↔ | ↑ | 9 |
| Elliott et al. [79] | ↔ | - | ↔ | 7 | |
| Romero-Moraleda et al. [15] | ↔ | ↔ | ↔ | 13 | |
| Lebrun et al. [14] | Isometric/Isokinetic Contractability | ↔ | - | ↔ | 16 |
| Ekenros et al. [76] | “ “ “ “ | ↔ | ↔ | ↔ | 9 |
| Sarwar et al. [16] | ↔ | ↑ | ↔ | 10 | |
| Phillips et al. [81] | ↑ | ↓ | ↑ * | 22 | |
| Elliott et al. [79] | ↔ | - | ↔ | 7 | |
| Montgomery et al. [82] | ↔ | - | ↔ | 71 | |
| Romero-Moraleda et al. [15] | Muscular Power “ | ↔ | ↔ | ↔ | 13 |
| Giacomoni et al. [77] | ↔ | - | ↔ | 7 | |
| Ansdell et al. [71] | Neuromuscular Function | ↓ | ↑ | ↑ | 15 |
| Hormonal Contraceptive Users | |||||
| Source | Outcome | Pill Withdrawal Phase | Active Pill Phase | n | |
| Ekenros et al. [76] | Maximal Strength “ | ↔ | ↔ | 8 | |
| Elliott et al. [79] | ↔ | ↔ | 14 | ||
| Ekenros et al. [76] | Isometric/Isokinetic Contractability “ | ↔ | ↔ | 8 | |
| Elliott et al. [79] | ↔ | ↔ | 14 | ||
| Sarwar et al. [16] | ↔ | ↔ | 10 | ||
| Rechichi et al. [80] | Muscular Power “ | ↓ | ↑ | 10 | |
| Giacomoni et al. [77] | ↔ | ↔ | 10 | ||
| Inflammatory Markers and BLA Across the Eumenorrheic Menstrual Cycle | ||||||
|---|---|---|---|---|---|---|
| Source | Biomarker | Follicular Phase | Late Follicular Phase/Ovulation | Luteal Phase | Timepoint(s) of Significant Finding | n |
| Hackney et al. [97] | IL-6 | ↑ | - | ↓ | 0-hr POST, 24-hr POST, 72-hr POST | 8 |
| CK | ↑ | - | ↓ | 24-hr POST, 72-hr POST | ||
| Romero-parra et al. [98] | IL-6 | ↓ | ↔ | ↑ | 2-hr POST > PRE, 24-hr POST, 48-hr POST | 19 |
| CK | ↔ | ↔ | ↔ | |||
| Markofski et al. [99] | CK | ↓ | - | ↑ | 96-hr POST | 16 |
| Chaffin et al. [100] | IL-6 | ↔ | - | ↔ | 9 | |
| Tsampoukos et al. [101] | BLA | ↔ | ↔ | ↔ | 8 | |
| Middleton et al. [102] | BLA | ↔ | - | ↔ | 6 | |
| Lara et al. [103] | BLA | ↔ | ↔ | ↔ | 13 | |
| Štefanovský et al. [104] | BLA | ↔ | - | ↔ | 8 | |
| Cabre et al. [7] | BLA | ↔ | - | ↔ | No differences between pre-, half-way, post-, or 10-min post-BLA measures | 19 |
| Blood Lactate in Eumenorrheic Females Compared to Oral Contraceptive Users or Hormonal IUD Users | ||||||
| Minahan et al. [105] | EUM | ↔ Assessed on day 2–6 of cycle | - | - | No significant differences were observed between EUM and OC groups. | 8 |
| OC Users | - | - | ↔ Assessed on day 2–21 of active pill phase | 8 | ||
| Cabre et al. [7] | EUM | ↔ Assessed on day 0–9 of cycle | - | ↔ Assessed between 2 days after ovulation or 5 days before next predicted period | No significant differences were observed between EUM, OC, or Hormonal IUD groups or across phases. | 19 |
| OC Users | - Assessed on days 0–7 of placebo pill | - | - Assessed on days 1–21 of active pill | 21 | ||
| IUD Users | - Assessed on days 0–9 of cycle | - | - Assessed between 2 days after ovulation or 5 days before next predicted period | 24 | ||
| Vascular Outcomes across the Eumenorrheic Menstrual Cycle and Cycles with Contraceptive Use | ||||||
| Source | Measurement Outcome | Follicular Phase/Inactive Pill Phase | Late Follicular Phase | Luteal Phase/Active Pill Phase | Timepoint(s) of Significant Finding | n |
| Williams et al. [106] | Endothelial function | ↔ | ↑ * | ↔ | * Meta-analysis rated this finding with ‘very low’ certainty of evidence. | 30 studies; n = 1363 EUM |
| Smooth muscle function | ↔ | ↔ | ↔ | |||
| Williams et al. [107] | Endothelial function Group: | |||||
| Combined estrogen/progestin contraceptives | ↑,↓,↔ * | - | ↑,↓,↔ * | * Dependent on specific contraceptive | 12 studies | |
| Progestin-only contraceptives | ↔ | - | ↔ | 2 studies | ||
| Smooth muscle function Group: | ||||||
| Combined estrogen/progestin contraceptives | ↔ | - | ↔ | 10 studies | ||
| Progestin-only contraceptives | ↔ | - | ↔ | 2 studies | ||
| Blood flow in Eumenorrheic Females Compared to Oral Contraceptive Users or Hormonal IUD Users | ||||||
| Minahan et al. [105] | EUM | ↔ Assessed on day 2–6 of cycle | - | - | Skin blood flow plateaued in EUM from 7.5 min in the heated (35 °C condition), whereas in OC users, increased for 15 min | 8 |
| OC Users | - | - | ↑ Assessed on day 2–21 of active pill phase | 8 | ||
| Cabre et al. [7] | EUM | ↔ Assessed on day 0–9 of cycle | - | ↔ Assessed between 2 days after ovulation or 5 days before next predicted period | No significant differences were observed between EUM, OC, or Hormonal IUD groups or across phases. | 19 |
| OC User | - Assessed on days 0–7 of placebo pill | - | - Assessed on day 1–21 of active pill | 21 | ||
| IUD Users | - Assessed on days 0–9 of cycle | - | - Assessed between 2 days after ovulation or 5 days before next predicted period | 24 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabre, H.E.; Gould, L.M.; Redman, L.M.; Smith-Ryan, A.E. Effects of the Menstrual Cycle and Hormonal Contraceptive Use on Metabolic Outcomes, Strength Performance, and Recovery: A Narrative Review. Metabolites 2024, 14, 347. https://doi.org/10.3390/metabo14070347
Cabre HE, Gould LM, Redman LM, Smith-Ryan AE. Effects of the Menstrual Cycle and Hormonal Contraceptive Use on Metabolic Outcomes, Strength Performance, and Recovery: A Narrative Review. Metabolites. 2024; 14(7):347. https://doi.org/10.3390/metabo14070347
Chicago/Turabian StyleCabre, Hannah E., Lacey M. Gould, Leanne M. Redman, and Abbie E. Smith-Ryan. 2024. "Effects of the Menstrual Cycle and Hormonal Contraceptive Use on Metabolic Outcomes, Strength Performance, and Recovery: A Narrative Review" Metabolites 14, no. 7: 347. https://doi.org/10.3390/metabo14070347
APA StyleCabre, H. E., Gould, L. M., Redman, L. M., & Smith-Ryan, A. E. (2024). Effects of the Menstrual Cycle and Hormonal Contraceptive Use on Metabolic Outcomes, Strength Performance, and Recovery: A Narrative Review. Metabolites, 14(7), 347. https://doi.org/10.3390/metabo14070347