
Using Serum Metabolomic Signatures to Investigate Effects of Acupuncture on Pain-Fatigue-Sleep Disturbance in Breast Cancer Survivors

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Procedures
2.3. Acupuncture Intervention
2.4. Metabolite Profiling and Quality Control
2.5. Measures
2.5.1. Demographics and Clinical Characteristics
2.5.2. PROMIS Measures
2.5.3. Dietary Screening and Control
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics of Participants
3.2. Symptoms Before and After Acupuncture
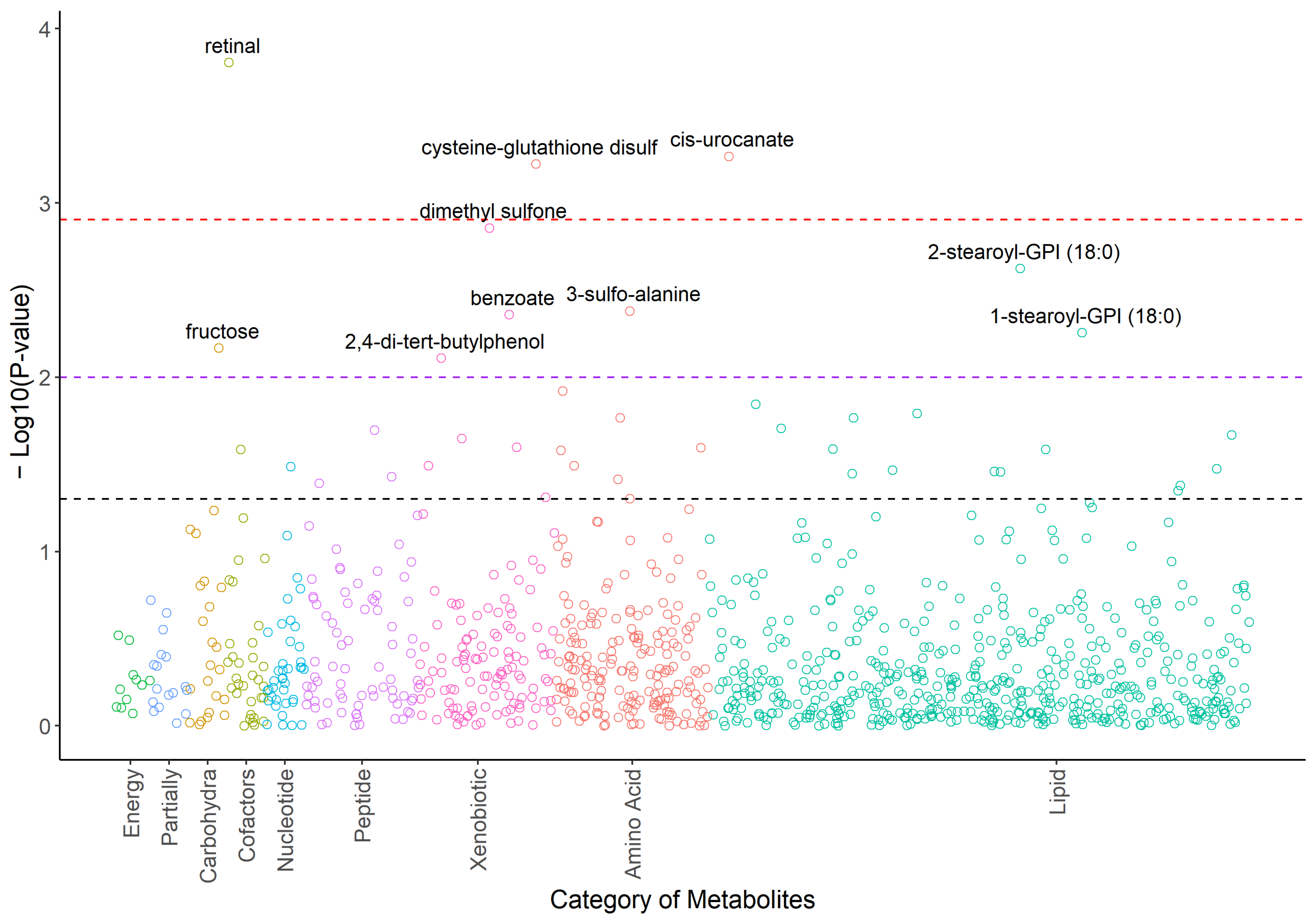
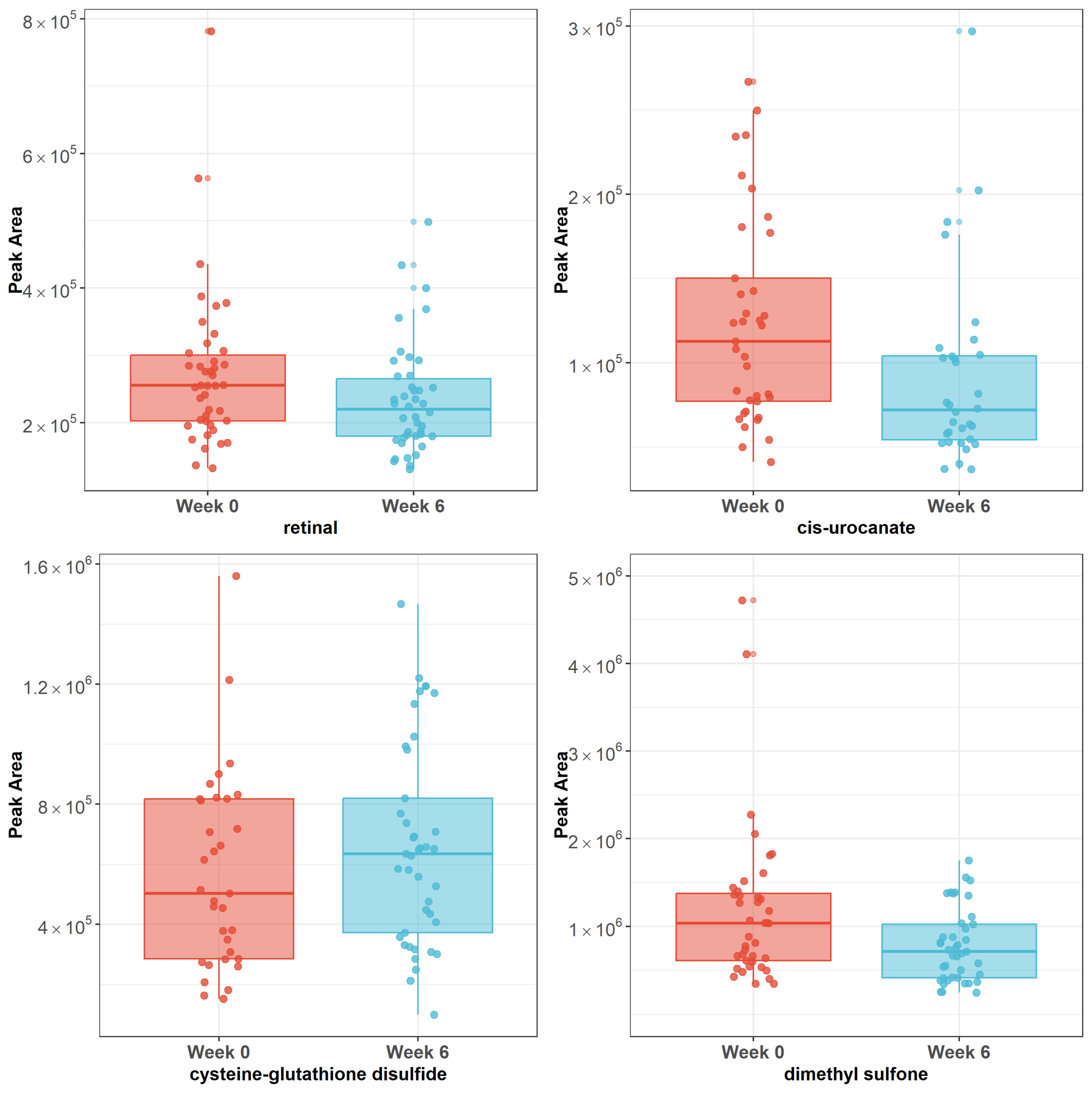
3.3. Changes in Metabolites in 6 Weeks After the 10-Session Acupuncture Treatment
3.4. Association of Changes in Serum Metabolites with Change in the Psychoneurological Symptom Cluster After Acupuncture Treatment
3.5. Potential Metabolites That Modulate Acupuncture’s Impact on Psychoneurological Symptoms over Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Bashaireh, A.M.; Khraisat, O.; Alnazly, E.K.; Aldiqs, M. Inflammatory Markers, Metabolic Profile, and Psychoneurological Symptoms in Women with Breast Cancer: A Literature Review. Cureus 2021, 13, e19953. [Google Scholar] [CrossRef] [PubMed]
- Bjerkeset, E.; Röhrl, K.; Schou-Bredal, I. Symptom cluster of pain, fatigue, and psychological distress in breast cancer survivors: Prevalence and characteristics. Breast Cancer Res. Treat. 2020, 180, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Jackson-Cook, C.; Lyon, D.; Perera, R.; Archer, K.J. Identifying molecular features associated with psychoneurological symptoms in women with breast cancer using multivariate mixed models. Cancer Inform. 2015, 14, CIN-S17276. [Google Scholar] [CrossRef] [PubMed]
- Denieffe, S.; Cowman, S.; Gooney, M. Symptoms, clusters and quality of life prior to surgery for breast cancer. J. Clin. Nurs. 2014, 23, 2491–2502. [Google Scholar] [CrossRef] [PubMed]
- Iwase, S.; Kawaguchi, T.; Tokoro, A.; Yamada, K.; Kanai, Y.; Matsuda, Y.; Kashiwaya, Y.; Okuma, K.; Inada, S.; Ariyoshi, K. Assessment of cancer-related fatigue, pain, and quality of life in cancer patients at palliative care team referral: A multicenter observational study (JORTC PAL-09). PLoS ONE 2015, 10, e0134022. [Google Scholar] [CrossRef]
- Langford, D.J.; Paul, S.M.; Cooper, B.; Kober, K.M.; Mastick, J.; Melisko, M.; Levine, J.D.; Wright, F.; Hammer, M.J.; Cartwright, F.; et al. Comparison of subgroups of breast cancer patients on pain and co-occurring symptoms following chemotherapy. Support. Care Cancer 2016, 24, 605–614. [Google Scholar] [CrossRef]
- MacPherson, H.; Thomas, K.; Walters, S.; Fitter, M. The York acupuncture safety study: Prospective survey of 34,000 treatments by traditional acupuncturists. BMJ 2001, 323, 486–487. [Google Scholar] [CrossRef]
- Hershman, D.L.; Unger, J.M.; Greenlee, H.; Capodice, J.L.; Lew, D.L.; Darke, A.K.; Kengla, A.T.; Melnik, M.K.; Jorgensen, C.W.; Kreisle, W.H.; et al. Effect of Acupuncture vs Sham Acupuncture or Waitlist Control on Joint Pain Related to Aromatase Inhibitors Among Women With Early-Stage Breast Cancer: A Randomized Clinical Trial. JAMA 2018, 320, 167–176. [Google Scholar] [CrossRef]
- Smith, C.; Carmady, B.; Thornton, C.; Perz, J.; Ussher, J.M. The effect of acupuncture on post-cancer fatigue and well-being for women recovering from breast cancer: A pilot randomised controlled trial. Acupunct. Med. 2013, 31, 9–15. [Google Scholar] [CrossRef]
- Otte, J.L.; Carpenter, J.S.; Zhong, X.; Johnstone, P.A. Feasibility study of acupuncture for reducing sleep disturbances and hot flashes in postmenopausal breast cancer survivors. Clin. Nurse Spec. 2011, 25, 228–236. [Google Scholar] [CrossRef]
- Li, H.; Schlaeger, J.M.; Jang, M.K.; Lin, Y.; Park, C.; Liu, T.; Sun, M.; Doorenbos, A.Z. Acupuncture Improves Multiple Treatment-Related Symptoms in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. J. Altern. Complement. Med. 2021, 27, 1084–1097. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-Y.; Kwok, S.W.H.; Tan, J.-Y.B.; Bressington, D.; Liu, X.-L.; Wang, T.; Chen, S.-L. Somatic acupressure for the fatigue-sleep disturbance-depression symptom cluster in breast cancer survivors: A phase II randomized controlled trial. Eur. J. Oncol. Nurs. Off. J. Eur. Oncol. Nurs. Soc. 2023, 66, 102380. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.K.; Lacey, J.; Kerin-Ayres, K.; Heller, G.; Grant, S. Acupuncture for the treatment of the pain-fatigue-sleep disturbance-numbness/tingling symptom cluster in breast cancer survivors: A feasibility trial. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2024, 32, 332. [Google Scholar] [CrossRef] [PubMed]
- Zick, S.M.; Sen, A.; Hassett, A.L.; Schrepf, A.; Wyatt, G.K.; Murphy, S.L.; Arnedt, J.T.; Harris, R.E. Impact of self-acupressure on co-occurring symptoms in cancer survivors. JNCI Cancer Spectr. 2018, 2, pky064. [Google Scholar] [CrossRef] [PubMed]
- Zick, S.M.; Zwickey, H.; Wood, L.; Foerster, B.; Khabir, T.; Wright, B.; Ichesco, E.; Sen, A.; Harris, R.E. Preliminary differences in peripheral immune markers and brain metabolites between fatigued and non-fatigued breast cancer survivors: A pilot study. Brain Imaging Behav. 2014, 8, 506–516. [Google Scholar] [CrossRef]
- Beger, R.D.; Dunn, W.; Schmidt, M.A.; Gross, S.S.; Kirwan, J.A.; Cascante, M.; Brennan, L.; Wishart, D.S.; Oresic, M.; Hankemeier, T. Metabolomics enables precision medicine: “A white paper, community perspective”. Metabolomics 2016, 12, 149. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Connelly, J.; Lindon, J.C.; Holmes, E. Metabonomics: A platform for studying drug toxicity and gene function. Nat. Rev. Drug Discov. 2002, 1, 153. [Google Scholar] [CrossRef]
- Zhang, A.; Yan, G.; Sun, H.; Cheng, W.; Meng, X.; Liu, L.; Xie, N.; Wang, X. Deciphering the biological effects of acupuncture treatment modulating multiple metabolism pathways. Sci. Rep. 2016, 6, 19942. [Google Scholar] [CrossRef]
- Yang, M.; Yu, Z.; Deng, S.; Chen, X.; Chen, L.; Guo, Z.; Zheng, H.; Chen, L.; Cai, D.; Wen, B. A targeted metabolomics MRM-MS study on identifying potential hypertension biomarkers in human plasma and evaluating acupuncture effects. Sci. Rep. 2016, 6, 25871. [Google Scholar] [CrossRef]
- Li, W.; Sun, M.; Yin, X.; Lao, L.; Kuang, Z.; Xu, S. The effect of acupuncture on depression and its correlation with metabolic alterations: A randomized controlled trial. Medicine 2020, 99, e22752. [Google Scholar] [CrossRef]
- Lv, Z.; Liu, R.; Su, K.; Gu, Y.; Fang, L.; Fan, Y.; Gao, J.; Ruan, X.; Feng, X. Acupuncture ameliorates breast cancer-related fatigue by regulating the gut microbiota-gut-brain axis. Front. Endocrinol. 2022, 13, 921119. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Zou, M.; Yang, M.; Zhou, S.; Yan, X.; Sun, B.; Wang, Y.; Chang, S.; Tang, Y.; Liang, F. Revealing potential biomarkers of functional dyspepsia by combining 1 H NMR metabonomics techniques and an integrative multi-objective optimization method. Sci. Rep. 2016, 6, 18852. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; White, A.; Cummings, M.; Jobst, K.A.; Rose, K.; Niemtzow, R.C. Standards for Reporting Interventions in Controlled Trials of Acupuncture: The STRICTA recommendations. J. Altern. Complement. Med. 2002, 8, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Schlaeger, J.M.; Patil, C.L.; Danciu, O.; Chen, Z.; Lif, N.; Gao, S.; Doorenbos, A.Z. Feasibility of implementing acupuncture in medically underserved breast cancer survivors (FAB): A protocol. Contemp. Clin. Trials 2024, 136, 107387. [Google Scholar] [CrossRef]
- DeHaven, C.D.; Evans, A.M.; Dai, H.; Lawton, K.A. Software techniques for enabling high-throughput analysis of metabolomic datasets. Metabolomics 2012, 10, 167–192. [Google Scholar]
- Peterson, R. Normalizing Transformation Functions [R Package bestNormalize Version 1.3.0]. 2018. Available online: https://github.com/petersonR/bestNormalize (accessed on 6 November 2024).
- Cessna, J.M.; Jim, H.S.L.; Sutton, S.K.; Asvat, Y.; Small, B.J.; Salsman, J.M.; Zachariah, B.; Fishman, M.; Field, T.; Fernandez, H.; et al. Evaluation of the psychometric properties of the PROMIS Cancer Fatigue Short Form with cancer patients. J. Psychosom. Res. 2016, 81, 9–13. [Google Scholar] [CrossRef]
- Quach, C.W.; Langer, M.M.; Chen, R.C.; Thissen, D.; Usinger, D.S.; Emerson, M.A.; Reeve, B.B. Reliability and validity of PROMIS measures administered by telephone interview in a longitudinal localized prostate cancer study. Qual. Life Res. 2016, 25, 2811–2823. [Google Scholar] [CrossRef]
- Amtmann, D.; Cook, K.F.; Jensen, M.P.; Chen, W.-H.; Choi, S.; Revicki, D.; Cella, D.; Rothrock, N.; Keefe, F.; Callahan, L.; et al. Development of a PROMIS item bank to measure pain interference. Pain 2010, 150, 173–182. [Google Scholar] [CrossRef]
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. Initial Adult Health Item Banks and First Wave Testing of the Patient-Reported Outcomes Measurement Information System (PROMIS™) Network: 2005–2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef]
- Yu, L.; Buysse, D.J.; Germain, A.; Moul, D.E.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Pilkonis, P.A. Development of Short Forms From the PROMIS™ Sleep Disturbance and Sleep-Related Impairment Item Banks. Behav. Sleep. Med. 2012, 10, 6–24. [Google Scholar] [CrossRef]
- Thompson, F.E.; Midthune, D.; Kahle, L.; Dodd, K.W. Development and Evaluation of the National Cancer Institute’s Dietary Screener Questionnaire Scoring Algorithms. J. Nutr. 2017, 147, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Butawan, M.; Benjamin, R.L.; Bloomer, R.J. Methylsulfonylmethane: Applications and safety of a novel dietary supplement. Nutrients 2017, 9, 290. [Google Scholar] [CrossRef] [PubMed]
- McFarlin, B.K.; Vingren, J.L.; Hill, D.W.; Bridgeman, E.A. MSM Supplementation Is Associated with Reduced Inflammation and Improved Innate Immune Response following In Vitro LPS-Stimulation in Humans after a Bout of Downhill Running. Muscles 2023, 2, 204–217. [Google Scholar] [CrossRef]
- Dambrova, M.; Makrecka-Kuka, M.; Kuka, J.; Vilskersts, R.; Nordberg, D.; Attwood, M.M.; Smesny, S.; Sen, Z.D.; Guo, A.C.; Oler, E. Acylcarnitines: Nomenclature, biomarkers, therapeutic potential, drug targets, and clinical trials. Pharmacol. Rev. 2022, 74, 506–551. [Google Scholar] [CrossRef] [PubMed]
- Zhang, I.W.; Sánchez-Rodríguez, M.B.; López-Vicario, C.; Casulleras, M.; Duran-Güell, M.; Flores-Costa, R.; Aguilar, F.; Rothe, M.; Segalés, P.; García-Ruiz, C.; et al. Palmitoylcarnitine impairs immunity in decompensated cirrhosis. JHEP Rep. 2024, 6, 101187. [Google Scholar] [CrossRef]
- Jinushi, R.; Masuda, S.; Tanisaka, Y.; Nishiguchi, S.; Shionoya, K.; Sato, R.; Sugimoto, K.; Shin, T.; Shiomi, R.; Fujita, A.; et al. Comparison of serum acylcarnitine levels in patients with myalgic encephalomyelitis/chronic fatigue syndrome and healthy controls: A systematic review and meta-analysis. J. Transl. Med. 2023, 21, 398. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Di Lascio, S.; Fornasari, D. Acetyl-L-carnitine in chronic pain: A narrative review. Pharmacol. Res. 2021, 173, 105874. [Google Scholar] [CrossRef]
- Storesund, S.K.; Karaji, I.; Strand, E.; Svardal, A.; Lønnebakken, M.T.; Berge, R.K.; Tveitevåg Svingen, G.F.; Nygård, O.K.; Pedersen, E.R. Even chained acylcarnitines predict long-term cardiovascular prognosis in patients with chest pain and non-obstructive coronary artery disease. Int. J. Cardiol. Cardiovasc. Risk Prev. 2022, 14, 200134. [Google Scholar] [CrossRef]
- Palczewski, K.; Kiser, P.D. Shedding new light on the generation of the visual chromophore. Proc. Natl. Acad. Sci. USA 2020, 117, 19629–19638. [Google Scholar] [CrossRef]
- Xia, Q.; Yu, L.; Song, J.; Sun, Z. The role of acupuncture in women with advanced reproductive age undergoing in vitro fertilization-embryo transfer: A randomized controlled trial and follicular fluid metabolomics study. Medicine 2023, 102, e34768. [Google Scholar] [CrossRef]
- Jocelyn, P.C. The standard redox potential of cysteine-cystine from the thiol-disulphide exchange reaction with glutathione and lipoic acid. Eur. J. Biochem. 1967, 2, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Goralski, T.; Ram, J.L. Extracellular Calcium Receptor as a Target for Glutathione and Its Derivatives. Int. J. Mol. Sci. 2022, 23, 717. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, F.; Azizi, H.; Sahebkar, M.S.; Mehraban Moghadam, S.; Jarahi, L.; Safarian, M.; Bahrami Taghanaki, H.R.; Zahedi Avval, F. Effects of Acupuncture on the Glutathione System in Overweight and Obese Individuals. J. Nutr. Fasting Health 2021, 9, 196–201. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhou, B.; Zhang, G.; Xu, S.; Yang, J.; Deng, S.; Yao, Z.; Geng, Q.; Ouyang, B.; Xia, T. The effect of acupuncture on oxidative stress: A systematic review and meta-analysis of animal models. PLoS ONE 2022, 17, e0271098. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Schlaeger, J.M.; Patil, C.L.; Danciu, O.C.; Xia, Y.; Sun, J.; Doorenbos, A.Z. Feasibility of Acupuncture and Exploration of Metabolomic Alterations for Psychoneurological Symptoms Among Breast Cancer Survivors. Biol. Res. Nurs. 2023, 25, 326–335. [Google Scholar] [CrossRef]
- Kaneko, K.; Walker, S.L.; Lai-Cheong, J.; Matsui, M.S.; Norval, M.; Young, A.R. cis-Urocanic acid enhances prostaglandin E2 release and apoptotic cell death via reactive oxygen species in human keratinocytes. J. Investig. Dermatol. 2011, 131, 1262–1271. [Google Scholar] [CrossRef]
- Acuña, I.; Ruiz, A.; Cerdó, T.; Cantarero, S.; López-Moreno, A.; Aguilera, M.; Campoy, C.; Suárez, A. Rapid and simultaneous determination of histidine metabolism intermediates in human and mouse microbiota and biomatrices. BioFactors 2022, 48, 315–328. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; McCarty, M.F.; OKeefe, J.H. Role of dietary histidine in the prevention of obesity and metabolic syndrome. Open Heart 2018, 5, e000676. [Google Scholar] [CrossRef]
- Xing, B.-B.; Huang, M.; Zhang, D.; Ding, G.-H. Subcutaneous Metabolites Involving Acupoint Sensitization Induced by Myocardial Ischemia and Acupuncture Stimulation in Rabbits. Zhen Ci Yan Jiu Acupunct. Res. 2018, 43, 433–439. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Sociodemographic Characteristics | Mean ± SD or N (%) |
|---|---|
| Sex | |
| Female | 42 (100%) |
| Age | 52.0 ± 10.5 |
| BMI | 30.0 ± 6.0 |
| Ethnicity | |
| Hispanic | 9 (21.4%) |
| Non-Hispanic | 33 (78.6%) |
| Race | |
| Asian | 1 (2.4%) |
| Black/African American | 17 (40.5%) |
| White/Caucasian | 21 (50.0%) |
| Other | 3 (7.1%) |
| Education level | |
| Less Than High School | 1 (2.4%) |
| High School Graduate | 5 (11.9%) |
| Some College | 7 (16.7%) |
| Bachelor’s Degree | 14 (33.3%) |
| Some Graduate School | 1 (2.4%) |
| Graduate School | 14 (33.3%) |
| Marital status | |
| Never Married | 14 (33.3%) |
| Married/Living with Partner | 15 (35.7%) |
| Divorced/Separated | 11 (26.2%) |
| Widowed | 2 (4.8%) |
| Household income | |
| Less than USD 35,000 | 12 (28.6%) |
| USD 35,000–USD 55,000 | 10 (23.8%) |
| USD 55,000–USD 100,000 | 12 (28.6%) |
| More than USD 100,000 | 8 (19.0%) |
| Stage of cancer | |
| 0 | 2 (4.8%) |
| 1 | 17 (40.5%) |
| 2 | 17 (40.5%) |
| 3 | 6 (14.3%) |
| Types of treatments | |
| Endocrine therapy | 42 (100%) |
| Radiation therapy | 33 (78.6%) |
| Chemotherapy | 27 (64.3%) |
| Antidepressant use | |
| Yes | 10 (23.8%) |
| No | 22 (52.4%) |
| Unknown | 10 (23.8%) |
| Mean ± SD | Week 0 (Baseline) | Week 6 |
|---|---|---|
| Predicted intake of fiber (gm) per day * | 13.3 ± 1.2 | 13.3 ± 1.5 |
| Predicted intake of total added sugars (tsp equivalents) per day * | 11.7 ± 1.6 | 12.0 ± 2.5 |
| Predicted intake of added sugars from sugar-sweetened beverages (tsp equivalents) per day * | 4.1 ± 0.9 | 4.1 ± 0.6 |
| Predicted intake of dairy (cup equivalents) per day * | 1.3 ± 0.3 | 1.3 ± 0.5 |
| Predicted intake of fruits and vegetables including legumes and excluding French fries (cup equivalents) per day * | 1.9 ± 0.4 | 1.9 ± 0.3 |
| Predicted intake of vegetables including legumes and excluding French fries (cup equivalents) per day * | 1.4 ± 0.3 | 1.4 ± 0.4 |
| Predicted intake of fruits (cup equivalents) per day * | 0.5 ± 0.1 | 0.5 ± 0.1 |
| Frequency of red meat intake per day | 0.2 ± 0.3 | 0.3 ± 0.4 |
| Frequency of processed meat intake per day | 0.2 ± 0.2 | 0.2 ± 0.3 |
| Outcomes | Before (T Score ± SD) | After (T Score ± SD) | Change * (T Score ± SD) | Change ** (T Score ± SD) |
|---|---|---|---|---|
| Pain interference | 58.8 ± 9.0 | 53.6 ± 9.2 | 5.2 ± 6.4 (p < 0.001) | 6.0 ± 6.4 (p < 0.001) |
| Fatigue | 56.7 ± 8.6 | 48.8 ± 8.6 | 8.0 ± 8.7 (p < 0.001) | 9.3 ± 8.8 (p < 0.001) |
| Sleep disturbance | 58.7 ± 6.3 | 51.5 ± 8.0 | 7.2 ± 9.3 (p < 0.001) | 6.6 ± 9.4 (p < 0.001) |
| Psychoneurological symptom cluster (pain interference + fatigue + sleep disturbance) | 58.1 ± 6.3 | 51.3 ± 6.5 | 6.8 ± 6.6 (p < 0.001) | 6.2 ± 6.7 (p < 0.001) |
| Rank | Metabolites | Sub-Pathway | β * | p Value |
|---|---|---|---|---|
| 1 | dimethyl sulfone | Chemical | 1.97 | 0.047 |
| 2 | retinal | Vitamin A Metabolism | 2.27 | 0.136 |
| 3 | cysteine-glutathione disulfide | Glutathione Metabolism | −0.29 | 0.796 |
| 4 | cis-urocanate | Histidine Metabolism | −0.21 | 0.825 |
| Rank | Metabolites | Sub-Pathway | β * | p Value |
|---|---|---|---|---|
| 1 | cytosine | Pyrimidine Metabolism | 3.85 | <0.001 |
| 2 | lauroylcarnitine (C12) | Fatty Acid Metabolism (Acyl Carnitine, Medium Chain) | −3.70 | <0.001 |
| 3 | N-acetylglycine | Glycine, Serine, and Threonine Metabolism | −3.39 | 0.001 |
| 4 | 5-dodecenoylcarnitine (C12:1) | Fatty Acid Metabolism (Acyl Carnitine, Monounsaturated) | −3.31 | 0.002 |
| 5 | hexanoylcarnitine (C6) | Fatty Acid Metabolism (Acyl Carnitine, Medium Chain) | −3.37 | 0.004 |
| 6 | 2-oxoarginine | Urea Cycle; Arginine and Proline Metabolism | 3.37 | 0.004 |
| 7 | 2-aminophenol sulfate | Food Component/Plant | 3.52 | 0.005 |
| 8 | pipecolate | Lysine Metabolism | 3.11 | 0.005 |
| 9 | acetyl carnitine (C2) | Fatty Acid Metabolism (Acyl Carnitine, Short Chain) | −3.26 | 0.006 |
| 10 | 2-acrylamidoglycolic acid | Chemical | 3.15 | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Doorenbos, A.Z.; Xia, Y.; Sun, J.; Choi, H.; Harris, R.E.; Gao, S.; Sullivan, K.; Schlaeger, J.M. Using Serum Metabolomic Signatures to Investigate Effects of Acupuncture on Pain-Fatigue-Sleep Disturbance in Breast Cancer Survivors. Metabolites 2024, 14, 698. https://doi.org/10.3390/metabo14120698
Li H, Doorenbos AZ, Xia Y, Sun J, Choi H, Harris RE, Gao S, Sullivan K, Schlaeger JM. Using Serum Metabolomic Signatures to Investigate Effects of Acupuncture on Pain-Fatigue-Sleep Disturbance in Breast Cancer Survivors. Metabolites. 2024; 14(12):698. https://doi.org/10.3390/metabo14120698
Chicago/Turabian StyleLi, Hongjin, Ardith Z. Doorenbos, Yinglin Xia, Jun Sun, Hannah Choi, Richard E. Harris, Shuang Gao, Katy Sullivan, and Judith M. Schlaeger. 2024. "Using Serum Metabolomic Signatures to Investigate Effects of Acupuncture on Pain-Fatigue-Sleep Disturbance in Breast Cancer Survivors" Metabolites 14, no. 12: 698. https://doi.org/10.3390/metabo14120698
APA StyleLi, H., Doorenbos, A. Z., Xia, Y., Sun, J., Choi, H., Harris, R. E., Gao, S., Sullivan, K., & Schlaeger, J. M. (2024). Using Serum Metabolomic Signatures to Investigate Effects of Acupuncture on Pain-Fatigue-Sleep Disturbance in Breast Cancer Survivors. Metabolites, 14(12), 698. https://doi.org/10.3390/metabo14120698