Antioxidant Therapy in Neonatal Hypoxic Ischemic Encephalopathy: Adjuvant or Future Alternative to Therapeutic Hypothermia?

 and
and
Abstract

1. Introduction
2. Materials and Methods
3. Neonatal Hypoxic Ischemic Encephalopathy
3.1. Definition
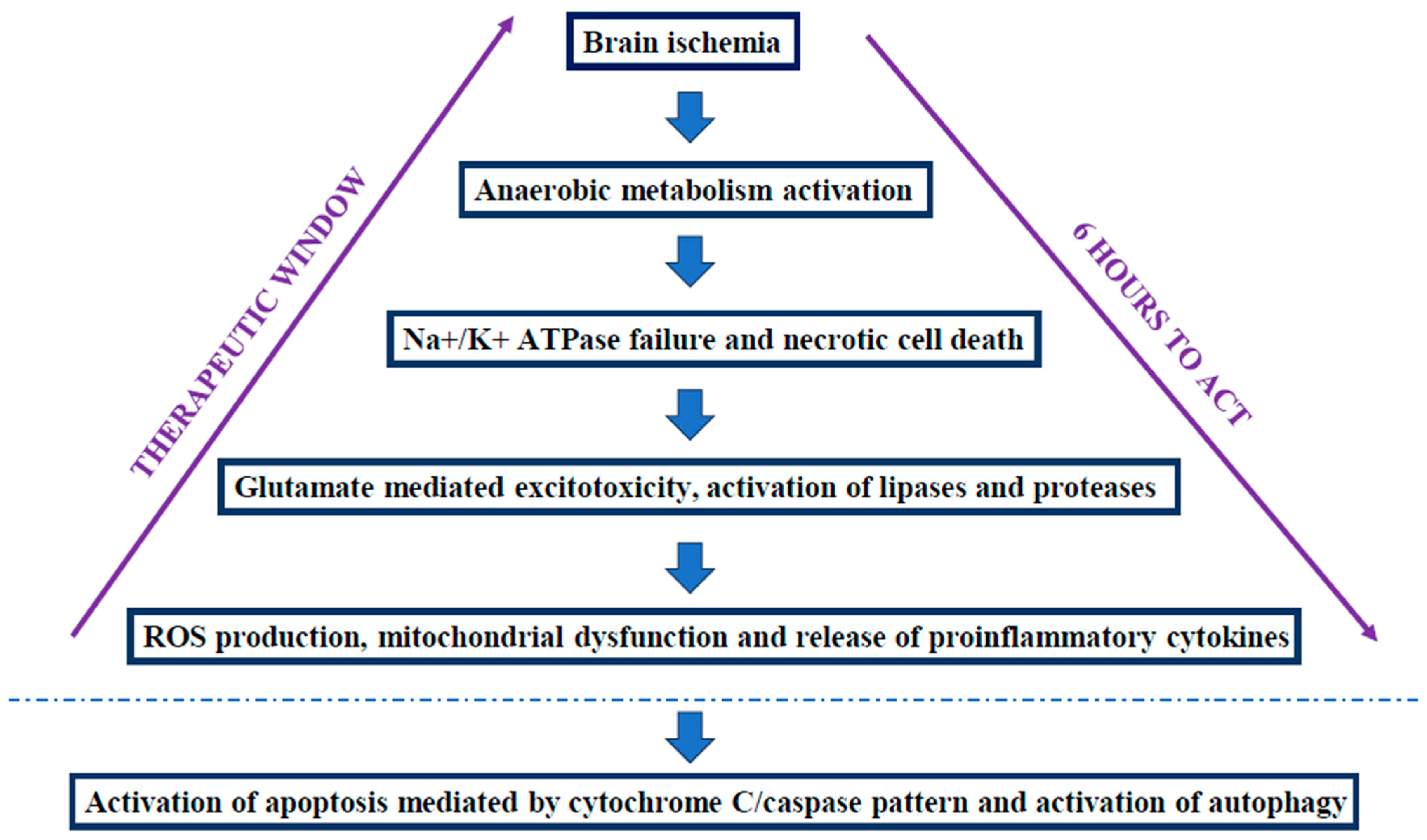
3.2. Pathogenesis of HIE
3.3. Potential Biomarkers of HIE
3.4. Therapeutic Hypothermia (TH)
- -
- An Apgar score ≤5 at 10 min of life; or
- -
- Need to continue neonatal resuscitation using invasive measures and not yet at 10 min of life; or
- -
- Fetal or neonatal acidosis on cord blood gas analysis or on any blood gas analysis obtained in the first 60 min of life (pH ≤ 7; BE ≥ −12 mmol/L).
- At least two of the following signs:
- -
- Lethargy/coma;
- -
- Reduced/absent motility;
- -
- Altered posture;
- -
- Hypotonia/flaccidity;
- -
- Incomplete/weak/absent primitive reflexes;
- -
- Pupillary anomalies.
- -
- Seizures
- -
- Electrical activity moderately abnormal (upper edge > 10 microV and lower edge < 5 microV) or severely abnormal (upper edge < 10 microV and lower edge < 5 microV);
- -
- Electrical crises;
- -
- Discontinuous or inactive electroencephalographic tracing [34].
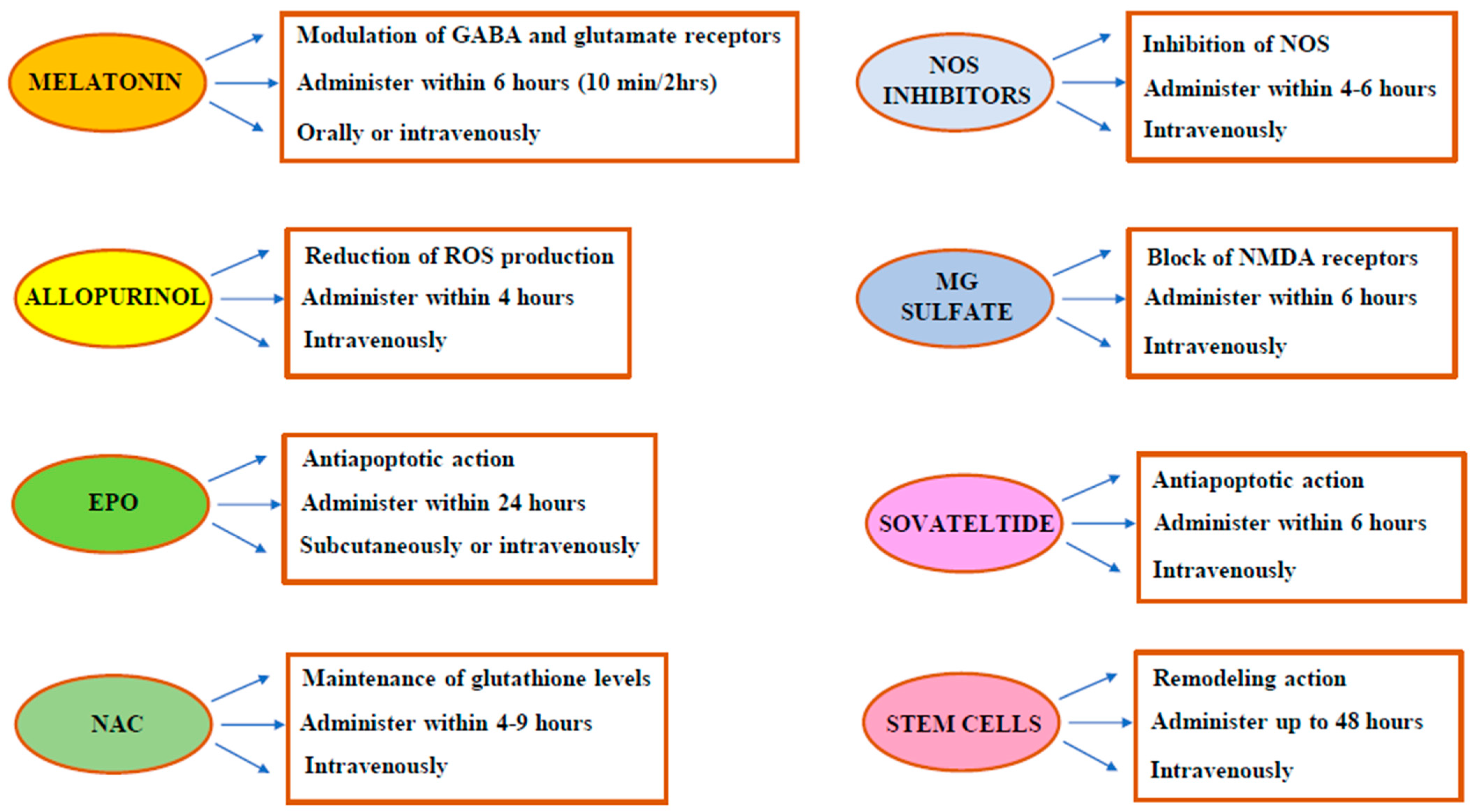
4. Antioxidant Therapies in Neonatal HIE
4.1. Melatonin
4.2. Allopurinol
4.3. Erythropoietin (EPO)
4.4. N-Acetylcysteine
4.5. NOS Inhibitors
4.6. Magnesium (Mg) Sulfate
4.7. Sovateltide
4.8. Stem Cells
4.9. Other Promising Antioxidants: Miscellany
- Docosahexaenoic Acid (DHA)
- 2.
- Lactoferrin
- 3.
- Lutein
- 4.
- Vitamins C and E
- 5.
- Deferoxamine
- 6.
- Dihydroartemisinin
- 7.
- Edaravone
- 8.
- Exendin-4
- 9.
- Carnosine
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nuňez, A.; Benavente, I.; Blanco, D.; Boix, H.; Cabaňas, F.; Chaffanel, M.; Fernández-Colomer, B.; Fernández-Lorenzo, J.R.; Loureiro, B.; Fernández-Lorenzo, J.R.; et al. Oxidative stress in perinatal asphyxia and hypoxic-ischaemic encephalopathy. An. Pediatr. 2018, 88, 228.e1–228.e9. [Google Scholar] [CrossRef]
- Ozsurekci, Y.; Aykac, K. Oxidative Stress Related Diseases in Newborns. Oxid. Med. Cell Longev. 2016, 2016, 2768365. [Google Scholar] [CrossRef] [PubMed]
- Saugstad, O.D. The oxygen radical disease in neonatology. Indian. J. Pediatr. 1989, 56, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.; Robbins, M.E.; Revhaug, C.; Saugstad, O.D. Oxygen radical disease in the newborn, revisited: Oxidative stress and disease in the newborn period. Free Radic. Biol. Med. 2019, 142, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Montante, C.; Notarbartolo, V.; Giuffrè, M. Antioxidants: Role the in prevention and treatment of bronchopulmonary dysplasia. Paediatr. Respir. Rev. 2022, 42, 53–58. [Google Scholar] [CrossRef]
- Wang, J.; Dong, W. Oxidative stress and bronchopulmonary dysplasia. Gene 2018, 678, 177–183. [Google Scholar] [CrossRef]
- Berkelhamer, S.K.; Farrow, K.N. Developmental Regulation of Antioxidant Enzymes and Their Impact on Neonatal Lung Disease. Antioxid. Redox Signal. 2014, 21, 1837–1848. [Google Scholar] [CrossRef]
- Martini, S.; Austin, T.; Aceti, A.; Faldella, G.; Corvaglia, L. Free radicals and neonatal encephalopathy: Mechanisms of injury, biomarkers, and antioxidant treatment perspectives. Pediatr. Res. 2020, 87, 823–833. [Google Scholar] [CrossRef]
- Perrone, S.; Lembo, C.; Giordano, M.; Petrolini, C.; Cannavò, L.; Gitto, E. Molecular mechanisms of oxidative stress-related neonatal jaundice. J. Biochem. Mol. Toxicol. 2023, 37, e23349. [Google Scholar] [CrossRef]
- Matyas, M.; Hasmasanu, M.G.; Zaharie, G. Antioxidant Capacity of Preterm Neonates Assessed by Hydrogen Donor Value. Medicina 2019, 55, 720. [Google Scholar] [CrossRef]
- Boskabadi, H.; Ghayour-Mobarhan, M.; Saeidinia, A. Serum pro-oxidant/antioxidant balance in term versus preterm neonates. Medicine 2022, 101, e31381. [Google Scholar] [CrossRef] [PubMed]
- Victor, S.; Rocha-Ferreira, E.; Rahim, A.; Hagberg, H.; Edwards, D. New possibilities for neuroprotection in neonatal hypoxic-ischemic encephalopathy. Eur. J. Pediatr. 2022, 181, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.C.; Yu, C.S.; Hu, Y.C.; Wang, X.A. Unconjugated bilirubin is correlated with the severeness and neurodevelopmental outcomes in neonatal hypoxic-ischemic encephalopathy. Sci. Rep. 2023, 13, 23075. [Google Scholar] [CrossRef]
- Popescu, M.R.; Panaitescu, A.M.; Pavel, B.; Zagrean, L.; Peltecu, G.; Zagrean, A.M. Getting an Early Start in Understanding Perinatal Asphyxia Impact on the Cardiovascular System. Front. Pediatr. 2020, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Torres-Cuevas, I.; Corral-Debrinski, M.; Gressens, P. Brain oxidative damage in murine models of neonatal hypoxia/ischemia and reoxygenation. Free Radic. Biol. Med. 2019, 142, 3–15. [Google Scholar] [CrossRef]
- Douglas-Escobar, M.; Weiss, M.D. Hypoxic-ischemic encephalopathy: A review for the clinician. JAMA Pediatr. 2015, 169, 397–403. [Google Scholar] [CrossRef]
- Bano, S.; Chaudhary, V.; Garga, U.C. Neonatal Hypoxic-ischemic Encephalopathy: A Radiological Review. J. Pediatr. Neurosci. 2017, 12, 1–6. [Google Scholar] [CrossRef]
- Efstathiou, N.; Theodoridis, G.; Sarafidis, K. Understanding neonatal hypoxic-ischemic encephalopathy with metabolomics. Hippokratia 2017, 21, 115–123. [Google Scholar]
- Zhao, M.; Zhu, P.; Fujino, M.; Zhuang, J.; Guo, H.; Sheikh, I.; Zhao, L.; Li, X.K. Oxidative Stress in Hypoxic-Ischemic Encephalopathy: Molecular Mechanisms and Therapeutic Strategies. Int. J. Mol. Sci. 2016, 17, 2078. [Google Scholar] [CrossRef]
- Shankaran, S.; Laptook, A.R.; McDonald, S.A.; Hintz, S.R.; Barnes, P.D.; Das, A.; Higgins, R.D.; Eunice Kennedy Shriver National Institute of Child Health; Human Development Neonatal Research Network. Acute Perinatal Sentinel Events, Neonatal Brain Injury Pattern and Outcome of Infants Undergoing a Trial of Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy. J. Pediatr. 2017, 180, 275–278.e2. [Google Scholar] [CrossRef]
- Yildiz, E.P.; Ekici, B.; Tatli, B. Neonatal hypoxic ischemic encephalopathy: An update on disease pathogenesis and treatment. Expert. Rev. Neurother. 2017, 17, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Bennet, L.; Tan, S.; van den Heuij, L.; Derrick, M.; Groenendaal, F.; van Bel, F.; Juul, S.; Back, S.A.; Northington, F.; Robertson, N.J.; et al. Cell therapy for neonatal hypoxia-ischemia and cerebral palsy. Ann. Neurol. 2012, 71, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Cheng, J.; Zhong, Y.; Mahgoub, O.K.; Akter, F.; Fan, Y.; Aldughaim, M.; Xie, Q.; Qin, L.; Gu, L.; et al. Mechanism and Treatment Related to Oxidative Stress in Neonatal Hypoxic-Ischemic Encephalopathy. Front. Mol. Neurosci. 2019, 12, 88. [Google Scholar] [CrossRef]
- Cerio, F.G.; Lara-Celador, I.; Alvarez, A.; Hilario, E. Neuroprotective therapies after perinatal hypoxic-ischemic brain injury. Brain Sci. 2013, 3, 191–214. [Google Scholar] [CrossRef] [PubMed]
- Rompis, J.; Murdono, D.; Daud, D.; Wilar, R.; Hatta, M.; Umboh, A. Role of Caspase-3 Level in Perinatal Asphyxia. Iran. J. Neonatol. 2021, 12, 1–7. [Google Scholar]
- Negro, S.; Benders, M.J.N.L.; Tataranno, M.L.; Coviello, C.; de Vries, L.S.; van Bel, F.; Groenendaal, F.; Longini, M.; Proietti, F.; Belvisi, E.; et al. Early Prediction of Hypoxic-Ischemic Brain Injury by a New Panel of Biomarkers in a Population of Term Newborns. Oxid. Med. Cell Longev. 2018, 28, 7608108. [Google Scholar] [CrossRef]
- Patel, K.P.; Makadia, M.G.; Patel, V.I.; Nilayangode, H.N.; Nimbalkar, S.M. Urinary Uric Acid/Creatinine Ratio—A Marker For Perinatal Asphyxia. J. Clin. Diagn. Res. 2017, 11, SC08–SC10. [Google Scholar] [CrossRef]
- Mondal, N.; Bhat, B.V.; Banupriya, C.; Koner, B.C. Oxidative Stress in Perinatal Asphyxia in Relation to Outcome. Indian J. Pediatr. 2010, 77, 515–517. [Google Scholar] [CrossRef]
- El-Mazary, A.A.M.; Abdel-Aziz, R.A.; Mahmoud, R.A.; El-Said, M.A.; Mohammed, N.R. Correlations between maternal and neonatal serum selenium levels in full term neonates with hypoxic ischemic encephalopathy. Ital. J. Pediatr. 2015, 41, 83. [Google Scholar] [CrossRef]
- Haga, M.; Kawabata, K.; Sumiya, W.; Kurita, S.; Imanishi, T.; Kanno, C.; Kanno, M.; Kanno, M.; Shimizu, M. The relationship between serum total bilirubin and severity of hypoxic injury in neonatal hypoxic-ischemic encephalopathy. Am. J. Perinatol. 2022, 39, 944–950. [Google Scholar] [CrossRef]
- Luo, Q.; Pin, T.; Dai, L.; Chen, G.; Chen, Y.; Tian, F.; Zhang, M. The Role of S100B Protein at 24 Hours of Postnatal Age as Early Indicator of Brain Damage and Prognostic Parameter of Perinatal Asphyxia. Glob. Pediatr. Health. 2019, 6, 2333794X19833729. [Google Scholar] [CrossRef] [PubMed]
- Gruppo di Studio di Neurologia Neonatale. Raccomandazioni per L’assistenza al Neonato con Encefalopatia Ipossico-Ischemica Possible Candidato al Trattamento Ipotermico; Società Italiana di Neonatologia: Milano, Italy, 2009. [Google Scholar]
- Azzopardi, D.; Strohm, B.; Marlow, N.; Brocklehurst, P.; Deierl, A.; Eddama, O.; Goodwin, J.; Halliday, H.L.; Juszczak, E.; Kapellou, O.; et al. Effects of hypothermia for perinatal asphyxia on childhood outcomes. N. Engl. J. Med. 2014, 371, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Gruppo di Studio di Neurologia Neonatale e Follow-Up. Raccomandazioni per L’assistenza al Neonato con Encefalopatia Ipossico-Ischemica Candidato al Trattamento Ipotermico; Società Italiana di Neonatologia: Milano, Italy, 2023; Available online: www.sin-neonatologia.it (accessed on 4 July 2024).
- Jacobs, S.E.; Berg, M.; Hunt, R.; Tarnow-Mordi, W.O.; Inder, T.E.; Davis, P.G. Cooling for newborns with hypoxic ischaemic encephalopathy (Review). Cochrane Database Syst. Rev. 2013, 2013, CD003311. [Google Scholar]
- Proietti, J.; Boylan, G.B.; Walsh, B.H. Regional variability in therapeutic hypothermia eligibility criteria for neonatal hypoxic-ischemic encephalopathy. Pediatr. Res. 2024, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Available online: www.nornet.org.uk (accessed on 7 July 2024).
- Sakr, M.; Shah, M.; Balasundaram, P. Neonatal Therapeutic Hypothermia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- D’angelo, G.; Cannavò, L.; Reiter, R.J.; Gitto, E. Melatonin Administration from 2000 to 2020 to Human Newborns with Hypoxic-Ischemic Encephalopathy. Am. J. Perinatol. 2022, 39, 824–829. [Google Scholar] [CrossRef]
- Notarbartolo, V.; Montante, C.; Ferrante, G.; Giuffrè, M. Antioxidant Effects of Dietary Supplements on Adult COVID-19 Patients: Why Do We Not Also Use Them in Children? Antioxidants 2022, 11, 1638. [Google Scholar] [CrossRef]
- Pluta, R.; Furmaga-Jabłońska, W.; Januszewski, S.; Tarkowska, A. Melatonin: A Potential Candidate for the Treatment of Experimental and Clinical Perinatal Asphyxia. Molecules 2023, 28, 1105. [Google Scholar] [CrossRef]
- Ahmed, J.; Pullattayil, S.A.K.; Robertson, N.J.; More, K. Melatonin for neuroprotection in neonatal encephalopathy: A systematic review & meta-analysis of clinical trials. Eur. J. Paediatr. Neurol. 2021, 31, 38–45. [Google Scholar]
- Tarocco, A.; Caroccia, N.; Morciano, G.; Wieckowski, M.R.; Ancora, G.; Garani, G.; Pinton, P. Melatonin as a master regulator of cell death and inflammation: Molecular mechanisms and clinical implications for newborn care. Cell Death Dis. 2019, 10, 317. [Google Scholar] [CrossRef]
- Toader, A.M.; Hoteiuc, O.; Bidian, C.; Oltean, D.D.; Tabaran, F.; Grad, O.; Clichici, S.; Rodica Mitrea, D. Neuronal apoptosis can be prevented by the combined therapy with melatonin and hypothermia in a neonatal rat model of hypoxic-ischemic encephalopathy. Med. Pharm. Rep. 2021, 94, 197–207. [Google Scholar] [CrossRef]
- Fulia, F.; Gitto, E.; Cuzzocrea, S.; Reiter, R.J.; Dugo, L.; Gitto, P.; Barberi, S.; Cordaro, S.; Barberi, I. Increased levels of malondialdehyde and nitrite/nitrate in the blood of asphyxiated newborns: Reduction by melatonin. J. Pineal Res. 2001, 31, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Aly, H.; Elmahdy, H.; El-Dib, M.; Rowisha, M.; Awny, M.; El-Gohary, T.; Elbatch, M.; Hamisa, M.; El-Mashad, A.R. Melatonin use for neuroprotection in perinatal asphyxia: A randomized controlled pilot study. J. Perinatol. 2015, 35, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Balduini, W.; Weiss, M.D.; Carloni, S.; Rocchi, M.; Sura, L.; Rossignol, C.; Longini, M.; Bazzini, F.; Perrone, S.; Ott, D.; et al. Melatonin pharmacokinetics and dose extrapolation after enteral infusion in neonates subjected to hypothermia. J. Pineal Res. 2019, 66, e12565. [Google Scholar] [CrossRef] [PubMed]
- Carloni, S.; Proietti, F.; Rocchi, M.; Longini, M.; Marseglia, L.; D’Angelo, G.; Balduini, W.; Gitto, E.; Buonocore, G. Melatonin Pharmacokinetics Following Oral Administration in Preterm Neonates. Molecules 2017, 22, 2115. [Google Scholar] [CrossRef]
- Robertson, N.J.; Martinello, K.; Lingam, I.; Avdic-Belltheus, A.; Meehan, C.; Alonso-Alconada, D.; Ragab, S.; Bainbridge, A.; Sokolska, M.; Tachrount, M.; et al. Melatonin as an adjunct to therapeutic hypothermia in a piglet model of neonatal encephalopathy: A translational study. Neurobiol. Dis. 2019, 121, 240–251. [Google Scholar] [CrossRef]
- Ahmad, Q.M.; Chishti, A.L.; Waseem, N. Role of melatonin in management of hypoxic ischaemic encephalopathy in newborns: A randomized control trial. J. Pak. Med. Assoc. 2018, 68, 1233–1237. [Google Scholar]
- Jerez-Calero, A.; Salvatierra-Cuenca, M.T.; Benitez-Feliponi, Á.; Fernández-Marín, C.E.; Narbona-López, E.; Uberos- Fernández, J.; Muňoz-Hoyos, A. Hypothermia Plus Melatonin in Asphyctic Newborns: A Randomized-Controlled Pilot Study. Pediatr. Crit. Care Med. 2020, 21, 647–655. [Google Scholar] [CrossRef]
- Miller, S.L.; Yan, E.B.; Castillo-Meléndez, M.; Jenkin, G.; Walker, D.W. Melatonin provides neuroprotection in the late-gestation fetal sheep brain in response to umbilical cord occlusion. Dev. Neurosci. 2005, 27, 200–210. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov (accessed on 3 July 2024).
- Engel, C.; Rüdiger, M.; Benders, M.J.N.L.; van Bel, F.; Allegaert, K.; Naulaers, G.; Bassler, D.; Klebermaß-Schrehof, K.; Vento, M.; Vilan, A.; et al. Detailed statistical analysis plan for ALBINO: Effect of Allopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome—A blinded randomized placebo-controlled parallel group multicenter trial for superiority (phase III). Trials 2024, 25, 81. [Google Scholar] [CrossRef]
- Durán Fernández-Feijóo, C.; Rodríguez-Fanjul, J.; Lopez-Abat, M.; Hadley, S.; Cavía-Saiz, M.; Muňiz, P.; Arnaez, J.; Fernández-Lorenzo, J.R.; Camprubí Camprubí, M. Effects of Hypothermia and Allopurinol on Oxidative Status in a Rat Model of Hypoxic Ischemic Encephalopathy. Antioxidants 2021, 10, 1523. [Google Scholar] [CrossRef]
- Arteaga, O.; Álvarez, A.; Revuelta, M.; Santaolalla, F.; Urtasun, A.; Hilario, E. Role of Antioxidants in Neonatal Hypoxic-Ischemic Brain Injury: New Therapeutic Approaches. Int. J. Mol. Sci. 2017, 18, 265. [Google Scholar] [CrossRef]
- Sabir, H.; Maes, E.; Zweyer, M.; Schleehuber, Y.; Imam, F.B.; Silverman, J.; White, Y.; Pang, R.; Pasca, A.M.; Robertson, N.J.; et al. Comparing the efficacy in reducing brain injury of different neuroprotective agents following neonatal hypoxia-ischemia in newborn rats: A multi-drug randomized controlled screening trial. Sci. Rep. 2023, 13, 9467. [Google Scholar] [CrossRef] [PubMed]
- Cánovas-Ahedo, M.; Alonso-Alconada, D. Combined therapy in neonatal hypoxic-ischaemic encephalopathy. An. Pediatr. 2019, 91, 59. [Google Scholar] [CrossRef]
- Chu, W.Y.; Annink, K.V.; Nijstad, A.L.; Maiwald, C.A.; Schroth, M.; El Bakkali, L.; van Bel, F.; Benders, M.J.N.L.; van Weissenbruch, M.M.; Hagen, A.; et al. Pharmacokinetic/Pharmacodynamic Modelling of Allopurinol, its Active Metabolite Oxypurinol, and Biomarkers Hypoxanthine, Xanthine and Uric Acid in Hypoxic-Ischemic Encephalopathy Neonates. Clin. Pharmacokinet. 2022, 61, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Gunes, T.; Ozturk, M.A.; Koklu, E.; Kose, K.; Gunes, I. Effect of allopurinol supplementation on nitric oxide levels in asphyxiated newborns. Pediatr. Neurol. 2007, 36, 17–24. [Google Scholar] [CrossRef]
- Torrance, H.L.; Benders, M.J.; Derks, J.B.; Rademaker, C.M.; Bos, A.F.; van den Berg, P.; Longini, M.; Buonocore, G.; Venegas, M.; Baquero, H.; et al. Maternal allopurinol during fetal hypoxia lowers cord blood levels of the brain injury marker S-100B. Pediatrics 2009, 124, 350–357. [Google Scholar] [CrossRef]
- Martini, S.; Castellini, L.; Parladori, R.; Paoletti, V.; Aceti, A.; Corvaglia, L. Free Radicals and Neonatal Brain Injury: From Underlying Pathophysiology to Antioxidant Treatment Perspectives. Antioxidants 2021, 10, 2012. [Google Scholar] [CrossRef] [PubMed]
- Kaandorp, J.J.; van Bel, F.; Veen, S.; Derks, J.B.; Groenendaal, F.; Rijken, M.; Roze, E.; Unikem Venema, M.M.A.; Rademaker, C.M.A.; Bos, A.F.; et al. Long-term neuroprotective effects of allopurinol after moderate perinatal asphyxia: Follow-up of two randomised controlled trials. Arch. Dis. Child. Fetal Neonatal Ed. 2012, 97, F162–F166. [Google Scholar] [CrossRef]
- Maiwald, C.A.; Annink, K.V.; Rüdiger, M.; Benders, M.J.N.L.; van Bel, F.; Allegaert, K.; Naulaers, G.; Bassler, D.; KlebermanB-Schrehof, K.; Vento, M.; et al. Effect of allopurinol in addition to hypothermia treatment in neonates for hypoxic-ischemic brain injury on neurocognitive outcome (ALBINO): Study protocol of a blinded randomized placebocontrolled parallel group multicenter trial for superiority (phase III). BMC Pediatr. 2019, 19, 210. [Google Scholar]
- Ranjan, A.K.; Gulati, A. Advances in Therapies to Treat Neonatal Hypoxic-Ischemic Encephalopathy. J. Clin. Med. 2023, 12, 6653. [Google Scholar] [CrossRef]
- Albrecht, M.; Zitta, K.; Groenendaal, F.; van Bel, F.; Peeters-Scholte, C. Neuroprotective strategies following perinatal hypoxia-ischemia: Taking aim at NOS. Free Radic. Biol. Med. 2019, 142, 123–131. [Google Scholar] [CrossRef]
- Elmahdy, H.; El-Mashad, A.R.; El-Bahrawy, H.; El-Gohary, T.; El-Barbary, A.; Aly, H. Human recombinant erythropoietin in asphyxia neonatorum: Pilot trial. Pediatrics 2010, 125, e1135–e1142. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.W.; Mathur, A.M.; Chang, T.; McKinstry, R.C.; Mulkey, S.B.; Mayock, D.E.; Van Meurs, K.P.; Rogers, E.E.; Gonzalez, F.F.; Comstock, D.E.; et al. High-Dose Erythropoietin and Hypothermia for Hypoxic-Ischemic Encephalopathy: A Phase II Trial. Pediatrics 2016, 137, e20160191. [Google Scholar] [CrossRef] [PubMed]
- Juul, S.E.; Voldal, E.; Comstock, B.A.; Massaro, A.N.; Bammler, T.K.; Mayock, D.E.; Heagerty, P.J.; Wu, Y.W.; Numis, A.L.; HEAL consortium. Association of High-Dose Erythropoietin With Circulating Biomarkers and Neurodevelopmental Outcomes Among Neonates With Hypoxic Ischemic Encephalopathy: A Secondary Analysis of the HEAL Randomized Clinical Trial. JAMA Netw. Open. 2023, 6, e2322131. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.J.; Wu, Y.; Liu, Y.; Cheng, R.; Chen, X.Q.; Yang, Y. The effect of erythropoietin on neonatal hypoxic-ischemic encephalopathy: An updated meta-analysis of randomized control trials. Front. Pediatr. 2023, 10, 1074287. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.D.; Wiest, D.B.; Mulvihill, D.M.; Hlavacek, A.M.; Majstoravich, S.J.; Brown, T.R.; Taylor, J.J.; Buckley, J.R.; Turner, R.P.; Rollins, L.G.; et al. Fetal and Neonatal Effects of N-Acetylcysteine When Used for Neuroprotection in Maternal Chorioamnionitis. J. Pediatr. 2016, 168, 67–76.e6. [Google Scholar] [CrossRef]
- Jenkins, D.D.; Moss, H.G.; Brown, T.R.; Yazdani, M.; Thayyil, S.; Montaldo, P.; Vento, M.; Kuligowski, J.; Wagner, C.; Hollis, B.W.; et al. NAC and Vitamin D Improve CNS and Plasma Oxidative Stress in Neonatal HIE and Are Associated with Favorable Long-Term Outcomes. Antioxidants 2021, 10, 1344. [Google Scholar] [CrossRef]
- Kesidou, E.; Bitsina, C.; Chatzisotiriou, A.; Theotokis, P.; Dandi, E.; Tata, D.A.; Spandou, E. N-Acetylcysteine Administration Attenuates Sensorimotor Impairments Following Neonatal Hypoxic-Ischemic Brain Injury in Rats. Int. J. Mol. Sci. 2022, 23, 16175. [Google Scholar] [CrossRef]
- Moss, H.G.; Brown, T.R.; Wiest, D.B.; Jenkins, D.D. N-Acetylcysteine rapidly replenishes central nervous system glutathione measured via magnetic resonance spectroscopy in human neonates with hypoxic-ischemic encephalopathy. J. Cereb. Blood Flow. Metab. 2018, 38, 950–958. [Google Scholar] [CrossRef]
- Tataranno, M.L.; Perrone, S.; Longini, M.; Buonocore, G. New antioxidant drugs for neonatal brain injury. Oxid. Med. Cell Longev. 2015, 2015, 108251. [Google Scholar] [CrossRef]
- Favié, L.M.A.; Cox, A.R.; van den Hoogen, A.; Nijboer, C.H.A.; Peeters-Scholte, C.M.P.C.D.; van Bel, F.; Egberts, T.C.G.; Rademaker, C.M.A.; Groenendaal, F. Nitric oxide synthase inhibition as a neuroprotective strategy following hypoxic–ischemic encephalopathy: Evidence from animal studies. Front. Neurol. 2018, 9, 258. [Google Scholar] [CrossRef] [PubMed]
- Zitta, K.; Peeters-Scholte, C.; Sommer, L.; Gruenewald, M.; Hummitzsch, L.; Parczany, K.; Steinfath, M.; Albrecht, M. 2-Iminobiotin superimposed on hypothermia protects human neuronal cells from hypoxia-induced cell damage: An in vitro study. Front. Pharm. 2017, 8, 971. [Google Scholar] [CrossRef] [PubMed]
- Clinicaltrials.eu. Available online: https://clinicaltrials.eu (accessed on 5 July 2024).
- El Farargy, M.S.; Soliman, N.A. A randomized controlled trial on the use of magnesium sulfate and melatonin in neonatal hypoxic ischemic encephalopathy. J. Neonatal Perinat. Med. 2019, 12, 379–384. [Google Scholar] [CrossRef]
- Siddiqui, M.A.; Butt, T.K. Role of Intravenous Magnesium Sulphate in Term Neonates with Hypoxic Ischemic Encephalopathy (HIE) in a Low-income Country: A Randomised Clinical Trial. J. Coll. Physicians Surg. Pak. 2021, 31, 817–820. [Google Scholar]
- Ramos, M.D.; Briyal, S.; Prazad, P.; Gulati, A. Neuroprotective Effect of Sovateltide (IRL 1620, PMZ 1620) in a Neonatal Rat Model of Hypoxic-Ischemic Encephalopathy. Neuroscience 2022, 480, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.Y.; Chang, Y.S.; Sung, D.K.; Sung, S.I.; Park, W.S. Hypothermia broadens the therapeutic time window of mesenchymal stem cell transplantation for severe neonatal hypoxic ischemic encephalopathy. Sci. Rep. 2018, 8, 7665. [Google Scholar] [CrossRef]
- Cottem, C.M.; Murtha, A.P.; Goldberg, R.N.; Grotegut, C.A.; Smith, P.B.; Goldstein, R.F.; Fisher, K.A.; Gustafson, K.E.; Waters-Pick, B.; Swamy, G.K.; et al. Feasibility of autologous cord blood cells for infants with hypoxic-ischemic encephalopathy. J. Pediatr. 2014, 164, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Basak, S.; Mallick, R.; Duttaroy, A.K. Maternal Docosahexaenoic Acid Status during Pregnancy and Its Impact on Infant Neurodevelopment. Nutrients 2020, 12, 3615. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, Y.; Wei, L.; Zhang, H.; Zhang, J.; Zhou, X.; Zhu, S.; Du, Y.; Su, R.; Fang, C.; et al. DHA supplementation and pregnancy complications. J. Transl. Med. 2023, 21, 394. [Google Scholar] [CrossRef]
- Schirmbeck, G.H.; Sizonenko, S.; Sanches, E.F. Neuroprotective Role of Lactoferrin during Early Brain Development and Injury through Lifespan. Nutrients 2022, 14, 2923. [Google Scholar] [CrossRef]
- Miura, S.; Ishida, A.; Nakajima, W.; Ohmura, A.; Kawamura, M.; Takada, G. Intraventricular ascorbic acid administration decreases hypoxic-ischemic brain injury in newborn rats. Brain Res. 2006, 1095, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Li, S.; Zhao, Q.; Huang, J.; Meng, J.; Yan, W.; Wang, J.; Ren, C.; Hao, L. Mechanisms of Vitamin C Regulating Immune and Inflammation Associated with Neonatal Hypoxic-Ischemic Encephalopathy Based on Network Pharmacology and Molecular Simulation Technology. Evid. Based Complement. Alternat Med. 2022, 2022, 4904325. [Google Scholar] [CrossRef] [PubMed]
- Kolnik, S.; Wood, T.R. Role of Vitamin E in Neonatal Neuroprotection: A Comprehensive Narrative Review. Life 2022, 12, 1083. [Google Scholar] [CrossRef] [PubMed]
- Kolnik, S.; Corry, K.; Hildahl, K.; Filteau, J.; White, O.; Brandon, O.; Farid, L.; Shearlock, A.M.; Moralejo, D.; Juul, S.E.; et al. Vitamin E Decreases Cytotoxicity and Mitigates Inflammatory and Oxidative Stress Responses in a Ferret Organotypic Brain Slice Model of Neonatal Hypoxia-Ischemia. Dev. Neurosci. 2022, 44, 233–245. [Google Scholar] [CrossRef]
- Xiong, Q.; Li, X.; Xia, L.; Yao, Z.; Shi, X.; Dong, Z. Dihydroartemisinin attenuates hypoxic-ischemic brain damage in neonatal rats by inhibiting oxidative stress. Mol. Brain. 2022, 15, 36. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, H.; Aihara, Y.; Yamaguchi, K.; Kawamata, T.; Okada, Y. Efficacy, safety, and outcomes in 17 pediatric cases treated with the free radical scavenger edaravone. Childs Nerv. Syst. 2015, 31, 1533–1540. [Google Scholar] [CrossRef]
- Zhou, K.Q.; Dhillon, S.K.; Bennet, L.; Gunn, A.J.; Davidson, J.O. Targeting Persistent Neuroinflammation after Hypoxic-Ischemic Encephalopathy-Is Exendin-4 the Answer? Int. J. Mol. Sci. 2022, 23, 10191. [Google Scholar] [CrossRef]
- Byun, J.C.; Lee, S.R.; Kim, C.S. Effects of carnosine and hypothermia combination therapy on hypoxic-ischemic brain injury in neonatal rats. Clin. Exp. Pediatr. 2021, 64, 422–428. [Google Scholar] [CrossRef]
- Mohsenpour, H.; Pesce, M.; Patruno, A.; Bahrami, A.; Pour, P.M.; Farzaei, M.H. A Review of Plant Extracts and Plant-Derived Natural Compounds in the Prevention/Treatment of Neonatal Hypoxic-Ischemic Brain Injury. Int. J. Mol. Sci. 2021, 22, 833. [Google Scholar] [CrossRef]
- Lee, M.T.; McNicholas, R.; Miall, L.; Simpson, N.; Goss, K.C.W.; Robertson, N.J.; Chumas, P. Progesterone as a Neuroprotective Agent in Neonatal Hypoxic-Ischaemic Encephalopathy: A Systematic Review. Dev. Neurosci. 2023, 45, 76–93. [Google Scholar] [CrossRef]
- Domoki, F. Hydrogen-induced Neuroprotection in Neonatal Hypoxic-ischemic Encephalopathy. Curr. Pharm. Des. 2021, 27, 687–694. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Asphyxia (Criterion A) | Neurological Examination Abnormalities (Criterion B) | aEEG/EEG Anomalies (Criterion C) | Recommendation Level |
|---|---|---|---|---|
| GE > 35 wks BW > 1800 g Timing <6 h | Strong | Strong | Strong | Strong |
| GE > 35 wks BW > 1800 g Timing < 6 h | Strong | Strong | Not Evaluable/Not Available | Strong |
| GE = 35 wks BW > 1800 g Timing < 6 h | Strong | Strong | Strong | Weak |
| GE >35 wks BW > 1800 g Timing < 6 h | Not Satisfied | Strong | Strong | Research Context |
| GE > 35 wks BW > 1800 g Timing 6–24 h | Strong | Strong | Not Applicable | Research Context |
| SUPC GE >35 wks BW > 1800 g Timing < 6 h | Strong | Strong | Strong | Research Context |
| Melatonin | |||||
|---|---|---|---|---|---|
| Authors | Publication Date | No. of Patients | Dosages/Formulations Used | PMID | Conclusions |
| Fulia et al. [45] | 2001 | 20 newborns with perinatal asphyxia were investigated | 10 asphyxiated infants received 8 doses of 10 mg each separated by 2-h intervals of melatonin orally; 10 asphyxiated infants received placebo. | 11703564 | Reduction in malondialdehyde and nitrite/nitrate levels in asphyxiated children treated with melatonin compared to the placebo. |
| Aly et al. [46] | 2015 | 30 neonates affected by HIE were investigated | 15 asphyxiated infants received both TH and melatonin in a dose of 10 mg/kg daily for a total of five doses orally; 15 asphyxiated infants received only TH. | 25393080 | Combination of melatonin and TH in moderate to severe HIE, reduced oxidative stress (SOD and NO), the number of seizures and white matter lesions, improving neurodevelopmental outcomes at 6-months of age. |
| Ahmad et al. [50] | 2018 | 80 newborns with perinatal asphyxia were investigated | 40 asphyxiated infants received both TH and melatonin in a dose of 10 mg in single-shot; 40 asphyxiated infants received only TH. | 30108392 | Combination of melatonin and TH improved survival rate. |
| Jerez-Calero et al. [51] | 2020 | 25 newborns with perinatal asphyxia were investigated | 12 asphyxiated infants received both TH and melatonin in a dose of 5 mg/kg for 3 days intravenously; 13 asphyxiated infants received only TH. | 32168305 | Combination of melatonin and TH improved the composite cognitive score (p-value < 0.05) at 18-months of age. |
| Allopurinol | |||||
|---|---|---|---|---|---|
| Authors | Publication Date | No. of Patients | Dosages/Formulations Used | PMID | Conclusions |
| Gunes et al. [60] | 2007 | 30 newborns with perinatal asphyxia were investigated | 30 asphyxiated infants received 3 doses of 40 mg/kg/day of allopurinol intravenously; first dose within 2 h of birth. | 17162192 | Improvement in neurodevelopmental outcomes. |
| Torrance et al. [61] ALLO-trial NCT00189007 | 2009 | 53 mothers during the delivery of 54 fetuses with hypoxia or incipient hypoxia | 26 mothers received 500 mg of allopurinol intravenously; 27 mothers received placebo (mannitol). | 19564319 | Reduction in S-100β protein level in cord blood of treated pregnant women. Allopurinol was safe for both the neonates and the mothers. |
| Kaandrop et al. [63] | 2012 | 22 children with history of perinatal asphyxia were investigated | 13 children were treated with high doses of allopurinol (40 mg/kg twice per day) within 4 h of birth. 9 children received the placebo. | 22102633 | Decreased risk of death or severe long-term disability at 4–8 years of age without significant side effects. |
| Erythropoietin | |||||
|---|---|---|---|---|---|
| Authors/ Study | Publication Date | No. of Patients | Dosages/Formulations Used | PMID | Conclusions |
| Elmahdy et al. [67] NCT00945789 | 2010 | 30 infants with HIE; 15 healthy infants | 15 infants with HIE received 2500 IU/kg/die of EPO, subcutaneously for 5 days, within the first 24 h of life. 15 infants with HIE received the placebo. | 20385632 | Improvement in electoencephalographic backgrounds and decreased NO concentrations at two weeks of age in the treated group. Reduction in the incidence of seizures and neurological abnormalities at 6 months of age in the treated group. |
| Wu et al. [68] | 2016 | 50 infants with moderate/severe encephalopathy | 24 infants received 1000 IU/kg of EPO at 1, 2, 3, 5 and 7 days of age plus TH. 26 infants received placebo at 1, 2, 3, 5, and 7 days of age plus TH. | 27244862 | Brain MRI scans of the EPO+TH group showed lower incidence of moderate/severe brain injury, subcortical injury and cerebellar injury than the placebo+TH group in the first week of life; around 1 year of life EPO-treated infants demonstrated better motor performance than the placebo-treated infants. |
| PAEN, NCT03079167 [53] | 2024 | 300 infants with HIE | 150 infants received 1000 IU/kg of EPO at 1, 2, 3, 5, and 7 days of life plus TH; 150 infants received the placebo at 1, 2, 3, 5 and 7 days of life plus TH. | / | EPO administration to newborns undergoing TH for HIE did not result in a lower risk of death or neurodevelopmental impairment than the placebo and was associated with a higher rate of serious adverse events. |
| Pan et al. [70] | 2023 | 1262 infants with HIE in 11 different studies | 636 infants treated with different dosages of EPO that ranged from 200 IU/kg to 1000 IU/kg (subcutaneously or intravenously); 626 infants treated with the placebo. | 36699298 | The metanalysis showed that using EPO would not increase the risk of adverse events, however, it is not beneficial for reducing death and improving neurological impairment in HIE-affected neonates. |
| N-Acetylcysteine | |||||
|---|---|---|---|---|---|
| Authors | Publication Date | No. of Patients | Dosages/Formulations Used | PMID | Conclusions |
| Jenkins et al. [72] | 2021 | 30 infants with moderate or severe HIE in hypothermia | 10 newborns received 25 mg/kg dose of NAC twice per day intravenously + 0.05 ug/kg/dose of calcitriol D twice per day, for 10 days; 10 newborns received 25 mg/kg dose of NAC twice per day intravenously + 0.03 ug/kg/dose of calcitriol D twice per day for 10 days; 10 newborns received 40 mg/kg dose of NAC twice per day intravenously + 0.03 ug/kg/dose of calcitriol D once a day for 10 days. | 34572976 | The study participants were evaluated through MRI, magnetic resonance spectroscopy, and reduced glutathione levels. In all 30 treated asphyxiated infants, there was no evidence of cerebral palsy, autism, or neurocognitive impairment at 1–2 years of age. |
| Moss et al. [74] | 2018 | 24 infants with moderate or severe HIE in hypothermia | Newborns received daily intravenous NAC and calcitriol infusions as NAC 25–40 mg/kg every 12 h and calcitriol 0.03–0.1 mg/kg/day from 6 h of life to 10 days or discharge. | 29561203 | In all 24 treated asphyxiated infants, the neuroprotective effect of NAC and calcitriol was demonstrated by evaluating the brain MRI. |
| NOS Inhibitors | |||||
| NCT01626924 [78] | 2016 | 6 near-term newborns with moderate or severe HIE | 0.08–0.16 mg/kg of 2-IB have been administered every 4 or 6 h intravenously, for 24 or 48 h. | / | 2-IB was administered without any severe side effects. |
| Magnesium (Mg) Sulfate | |||||
| El Farargy et al. [79] | 2019 | 60 infants with moderate HIE (Sarnat II) have been recruited | 30 infants received 25 mg/kg/day of MgSO4 intravenously, at days 0 and 1; then, they received 10 mg/kg/day of melatonin for 5 days, orally. 30 infants received only 10 mg/kg/day of melatonin for 5 days, orally. | 31609707 | Serum S100B concentration, which correlates with the severity of HIE, was significantly reduced in the infants who received both magnesium and melatonin, suggesting a synergistic effect of magnesium and melatonin in neuroprotection. |
| Sovateltide | |||||
| NCT05514340 [65] | Ongoing trial | 40 infants with HIE | 20 infants treated with TH+0.3 µg/kg/dose of sovateltide, intravenously, every 3 h on days 1, 3 and 6; 20 infants treated with TH+ the same dose and scheme of placebo. | / | The primary aim of the study is to evaluate the percentage of patients with death or disability (moderate or severe) in the sovateltide group compared to the control group. |
| Stem Cells | |||||
| Cotten et al. [83] | 2014 | 52 infants with HIE | 52 infants received 5 × 107 cells/kg of autologous cord blood for 4 infusions plus TH. | 24388332 | 74% of the newborns that received stem cells survived with scores of 85 or higher in the Bayley scales, compared to 41% of the newborns treated with TH alone (historical controls). |
| NEOSTEM trial NCT02881970 [clinicaltrials.gov] | Ongoing trial | 20 infants | All children will receive 5 × 107/kg of autologous mononuclear cells from umbilical cord blood. | / | The aims will be to evaluate adverse clinical or paraclinical event rates due to stem cell preparation until 2 years of age and to assess neurodevelopmental function until 2 years of age |
| NCT06427642 [clinicaltrials.gov] | Ongoing trial | 120 infants with HIE, bronchopulmonary dysplasia, or short bowel syndrome | Therapy with mononuclear cells obtained from umbilical cord blood+TH will be compared with TH only. | / | The aims of the study will be to evaluate the incidence of adverse reactions, the incidence of complications, the frequency of seizures via EEG, ventilator support time, and oxygen demand. |
| Potential Antioxidant Use in HIE (Animal Models) | |
|---|---|
| Dietary elements | Docosahexaenoic acid [8], lactoferrin [86], lutein [75], vitamin C [87], vitamin E [90] |
| Drugs | Deferoxamine [75], dihydroartemisinin [91], edaravone [92], exendin-4 [93], mitochondrial therapy [23] |
| Endogenous substances | Carnosine [94], progesterone [96] |
| Natural plant products | Caffeine, cannabidiol, resveratrol [56,57,95] |
| Others | Hyperbaric oxygen therapy [23], molecular hydrogen [97] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Notarbartolo, V.; Badiane, B.A.; Angileri, V.M.; Piro, E.; Giuffrè, M. Antioxidant Therapy in Neonatal Hypoxic Ischemic Encephalopathy: Adjuvant or Future Alternative to Therapeutic Hypothermia? Metabolites 2024, 14, 630. https://doi.org/10.3390/metabo14110630
Notarbartolo V, Badiane BA, Angileri VM, Piro E, Giuffrè M. Antioxidant Therapy in Neonatal Hypoxic Ischemic Encephalopathy: Adjuvant or Future Alternative to Therapeutic Hypothermia? Metabolites. 2024; 14(11):630. https://doi.org/10.3390/metabo14110630
Chicago/Turabian StyleNotarbartolo, Veronica, Bintu Ayla Badiane, Vita Maria Angileri, Ettore Piro, and Mario Giuffrè. 2024. "Antioxidant Therapy in Neonatal Hypoxic Ischemic Encephalopathy: Adjuvant or Future Alternative to Therapeutic Hypothermia?" Metabolites 14, no. 11: 630. https://doi.org/10.3390/metabo14110630
APA StyleNotarbartolo, V., Badiane, B. A., Angileri, V. M., Piro, E., & Giuffrè, M. (2024). Antioxidant Therapy in Neonatal Hypoxic Ischemic Encephalopathy: Adjuvant or Future Alternative to Therapeutic Hypothermia? Metabolites, 14(11), 630. https://doi.org/10.3390/metabo14110630