
Advanced Oxidative Protein Products Had a Diagnostic Accuracy for Identifying Chronic Kidney Disease in Adult Population

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
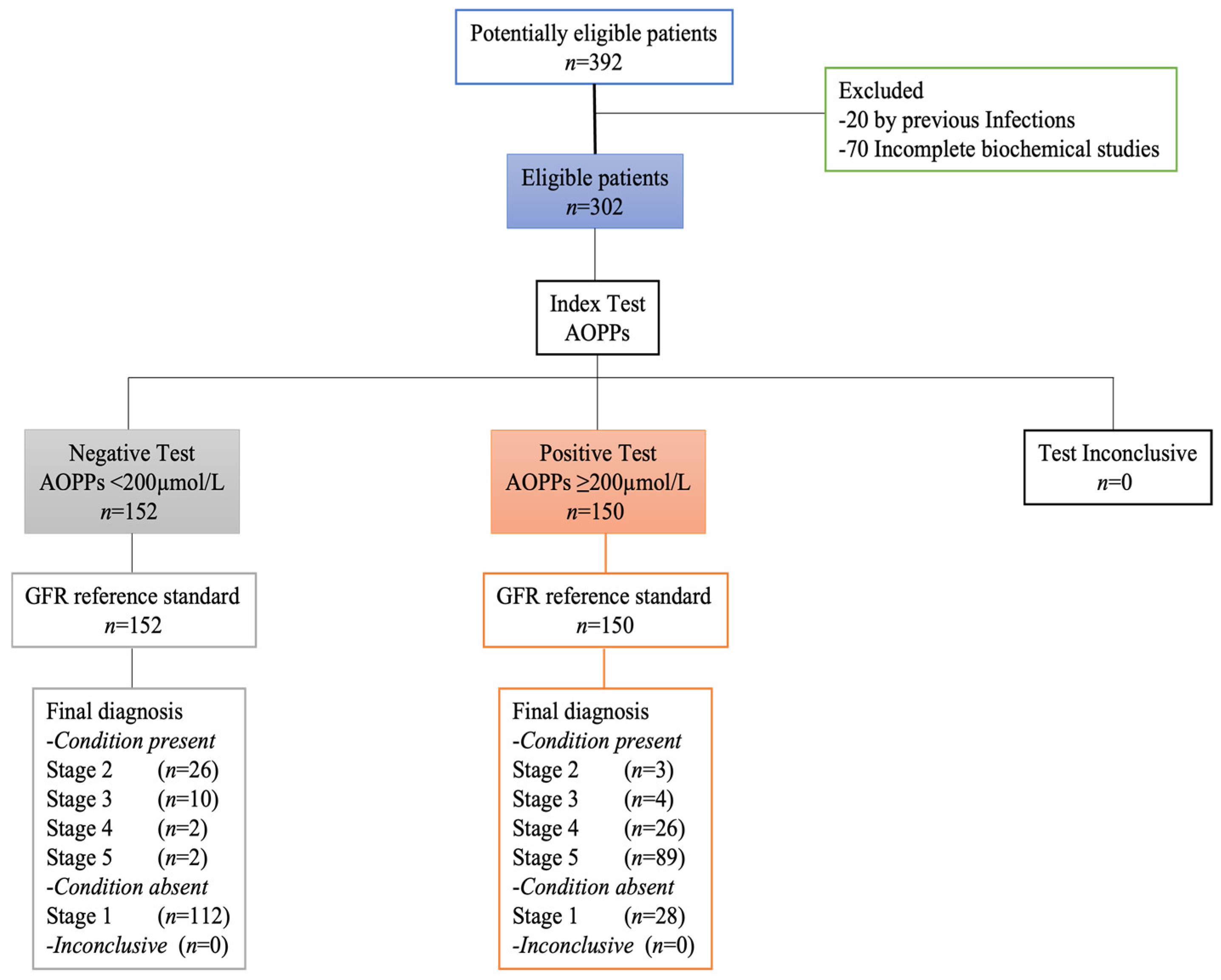
2.1. Sample Size
2.2. Participants
2.3. Biochemical Parameters
2.4. AOPPs Determination
2.5. Calibration Curve
2.6. Sample Analysis
2.7. Ethical Considerations
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kovesdy, C.P.; Furth, S.L.; Zoccali, C.; on behalf of the World Kidney Day Steering Committee. Obesity and kidney disease: Hidden consequences of the Epidemic. J. Bras. Nefrol. 2017, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.A.; Tonelli, M.; Staniferc, J.W. The global burden of kidney disease and the sustainable development goals. Bull. World Health Organ. 2018, 96, 414–422C. [Google Scholar] [CrossRef]
- Wang, J.; Niratharakumar, K.; Gokhale, K.; Tahrani, A.A.; Taverner, T.; Thomas, G.N.; Dasgupta, I. Obesity Without Metabolic Abnormality and Incident CKD: A Population-Based British Cohort Study. Am. J. Kidney Dis. 2022, 79, 24–35.e1. [Google Scholar] [CrossRef] [PubMed]
- Aziz, S.; Ghadzi, S.M.S.; Sulaiman, S.A.S.; Hanafiah, N.H.M.; Harun, S.N. Can Newer Anti-Diabetic Therapies Delay the Development of Diabetic Nephropathy? J. Pharm. Bioallied Sci. 2021, 13, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Musso, C.G.; Álvarez-Gregori, J.; Jauregui, J.; Macías-Núñez, J.F. Glomerular filtration rate equations: A comprehensive review. Int. Urol. Nephrol. 2016, 48, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Michels, W.M.; Grootendorst, D.C.; Verduijn, M.; Elliott, E.G.; Dekker, F.W.; Krediet, R.T. Performance of the Cockcroft-Gault, MDRD, and new CKD-EPI formulas in relation to GFR, age, and body size. Clin. J. Am. Soc. Nephrol. 2010, 5, 1003–1009. [Google Scholar] [CrossRef]
- Yuan, T.; Yang, T.; Chen, H.; Fu, H.; Hu, Y.; Xu, W.; Xie, X. New insights into oxidative stress and inflammation during diabetes mellitus-accelerated atherosclerosis. Redox Biol. 2019, 20, 247–260. [Google Scholar] [CrossRef]
- Forrester, J.; Kikuchi, S.; Hernandes, M.; Xu, Q.; Griendling, K. Reactive oxygen species in metabolic and inflammatory signaling. Circ. Res. 2018, 122, 877–902. [Google Scholar] [CrossRef]
- Witko-Sarsat, V.; Friedlander, M.; Capeillère-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced oxidation protein products as a novel marker of oxidative stress in uraemia. Kidney Int. 1996, 49, 1304–1309. [Google Scholar] [CrossRef]
- Villalpando-Sánchez, D.C.; Alvarez-Aguilar, C.; Gómez-García, A. Productos avanzados de oxidación proteica (PAOP) y su relación con los factores de riesgo cardiovascular en jóvenes aparentemente sanos. Clín. E Investig. En Arterioscler. 2017, 407, 1–7. [Google Scholar] [CrossRef]
- Arimura, N.; Watanabe, H.; Kato, H.; Imafuku, T.; Nakano, T.; Sueyoshi, M.; Chikamatsu, M.; Tokumaru, K.; Nagasaki, T.; Maeda, H.; et al. Advanced Oxidation Protein Products Contribute to Chronic-Kidney-Disease-Induced Adipose Inflammation through Macrophage Activation. Toxins 2023, 15, 179. [Google Scholar] [CrossRef] [PubMed]
- Conti, G.; Caccamo, D.; Siligato, R.; Gembillo, G.; Satta, E.; Pazzano, D.; Carucci, N.; Carella, A.; Del Campo, G.; Salvo, A.; et al. Association of Higher Advanced Oxidation Protein Products (AOPPs) Levels in Patients with Diabetic and Hypertensive Nephropathy. Medicina 2019, 55, 675. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Li, X.; Tian, J.; Xu, L.; Wan, J.; Liu, Y. A new model of diabetic nephropathy in C57BL/6 mice challenged with advanced oxidation protein products. Free Radic. Biol. Med. 2018, 118, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.; Villaseñor, L.; Yanowsky, G.; Andrade, J. Oxidative Stress in Diabetic Nephropathy with Early Chronic Kidney Disease. J. Diabetes Res. 2016, 2016, 7047238. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Sample size estimation in diagnostic test studies of biomedical informatics. J. Biomed. Inform. 2014, 48, 193–204. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.W.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; Lefevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef]
- WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy; World Health Organization: Geneva, Switzerland, 2010.
- Hudson, J.Q.; Nyman, H.A. Use of estimated glomerular filtration rate for drug dosing in the chronic kidney disease patient. Curr. Opin. Nephrol. Hypertens. 2011, 20, 482–491. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E. Summary of KDIGO 2012 CKD Guideline: Behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2013, 85, 49–61. [Google Scholar] [CrossRef]
- de Jong, P.E.; Brenner, B.M. From secondary to primary prevention of progressive renal disease: The case for screening for albuminuria. Kidney Int. 2004, 66, 2109–2118. [Google Scholar] [CrossRef]
- Piwowar, A.; Knapik-Kordecka, M.; Szczecinska, J.; Warmas, M. Plasma glycooxidation protein products in type 2 diabetic patients with nephropathy. Diabetes Metab. Res. Rev. 2008, 24, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Hou, F.F.; Nie, J. AOPPs and the progression of kidney disease. Kidney Int. Sup. 2014, 4, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Xun, T.; Lin, Z.; Wang, X.; Zhan, X.; Feng, H.; Gan, D.; Yang, X. Advanced oxidation protein products downregulate CYP1A2 and CYP3A4 expression and activity via the NF-κB-mediated signaling pathway in vitro and in vivo. Lab. Investig. 2021, 101, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, N.; Thornalley, P.J. Advanced glycation end products in the pathogenesis of chronic kidney disease. Kidney Int. 2018, 93, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Hou, F.F.; Zhang, X.; Chen, P.Y.; Liu, S.X.; Feng, J.X.; Liu, Z.Q.; Shan, Y.X.; Wang, G.B.; Zhou, Z.M.; et al. Advanced oxidation protein products accelerate renal fibrosis in a remnant kidney model. J. Am. Soc. Nephrol. 2007, 18, 528–538. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.Y.; Hou, F.F.; Niu, H.X.; Wang, G.B.; Xie, D.; Guo, Z.J.; Zhou, Z.M.; Yang, F.; Tian, J.W.; Zhang, X. Advanced oxidation protein products promote inflammation in diabetic kidney through activation of renal nicotinamide adenine dinucleotide phosphate oxidase. Endocrinology 2008, 149, 1829–1839. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Wu, S.; Jiang, J.; Tian, J.; Chen, J.; Yu, X.; Chen, P.; Mei, C.; Xiong, F.; Shi, W.; et al. Accumulation of circulating advanced oxidation protein products is an independent risk factor for ischaemic heart disease in maintenance haemodialysis patients. Nephrology 2012, 17, 642–649. [Google Scholar] [CrossRef]
- Marsche, G.; Frank, S.; Hrzenjak, A.; Holzer, M.; Dirnberger, S.; Wadsack, C.; Scharnagl, H.; Stojakovic, T.; Heinemann, A.; Oettl, K. Plasma-advanced oxidation protein products are potent high-density lipoprotein receptor antagonists in vivo. Circ. Res. 2009, 104, 750–757. [Google Scholar] [CrossRef]
- Kalousova, M.; Skrha, J.; Zima, T. Advanced glycation end products and advanced oxidation protein products in patients with diabetes mellitus. Physiol. Res. 2002, 51, 597–604. [Google Scholar]
- Heidari, F.; Rabizadeh, S.; Rajab, A.; Heidari, F.; Mouodi, M.; Mirmiranpour, H.; Esteghamati, A.; Nakhjavani, M. Advanced glycation end-products and advanced oxidation protein products levels are correlates of duration of type 2 diabetes. Life Sci. 2020, 260, 118422. [Google Scholar] [CrossRef]
- Xu, H.; Cabezas-Rodriguez, I.; Qureshi, A.R.; Heimburger, O.; Barany, P.; Snaedal, S.; Anderstam, B.; Helin, A.-C.B.; Carrero, J.J.; Stenvinkel, P.; et al. Increased Levels of Modified Advanced Oxidation Protein Products Are Associated with Central and Peripheral Blood Pressure in Peritoneal Dialysis Patients. Perit. Dial. Int. 2015, 35, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Suvakov, S.; Jerotic, D.; Damjanovic, T.; Milic, N.; Pekmezovic, T.; Djukic, T.; Jelic-Ivanovic, Z.; Radojevic, A.S.; Pljesa-Ercegovac, M.; Matic, M.; et al. Markers of Oxidative Stress and Endothelial Dysfunction Predict Haemodialysis Patients Survival. Am. J. Nephrol. 2019, 50, 115–125. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| VARIABLES | With DM2 n = 213 | Without DM2 n = 89 | p |
|---|---|---|---|
| Age (years) | 60 (28–75) | 40 (21–56) | 0.0001 |
| Gender (woman/men) | 85/128 | 78/11 | 0.0001 |
| SBP (mmHg) | 120 (110–130) | 110 (100–120) | 0.001 |
| DBP (mmHg) | 80 (60–90) | 80 (50–90) | 0.001 |
| Weight (kg) | 69 (60–114) | 68.9 (61.5–78) | 0.887 |
| BMI (kg/m2) | 27.1 (25–34.4) | 28.4 (18.03–31.7) | 0.140 |
| Glucose (mg/dL) | 133 (101.2–168.5) | 88.9 (32–96.3) | 0.0001 |
| TC (mg/dL) | 168 (131–338) | 192 (55–220.92) | 0.0001 |
| TG (mg/dL) | 157 (127–298.36) | 167 (60–223.4) | 0.240 |
| LDL-c (mg/dL) | 98 (90–122) | 132.7 (104–238) | 0.0001 |
| HDL-c (mg/dL) | 48 (25–80) | 23 (12–55) | 0.0001 |
| Creatinine (mg/dL) | 3.35 (0.8–10.01) | 0.7 (0.5–0.9) | 0.0001 |
| AOPPs (µmol/L) | 487.3 (115.57–522.42) | 158.5 (113.4–212.10) | 0.0001 |
| SBP | DBP | Glucose | TC | TG | Cr | GFR | |
|---|---|---|---|---|---|---|---|
| AOPPs | 0.401 ** | 0.159 ** | 0.168 ** | −0.390 ** | 0.009 | 0.754 ** | −0.826 ** |
| SBP | 0.609 ** | 0.163 ** | −0.138 ** | −0.038 | 0.331 ** | −0.383 ** | |
| DBP | 0.117 * | −0.112 | 0.026 | 0.082 | −0.102 | ||
| Glucose | 0.018 | 0.172 ** | 0.009 | −0.098 | |||
| TC | 0.401 ** | −0.295 ** | 0.335 ** | ||||
| TG | 0.053 | 0.060 | |||||
| Cr | −0.734 ** |
| Stage 1 GFR ≥90 mL/min/1.73 m2 | Stage 2 GFR 60–89 mL/min/1.73 m2 | Stage 3 GFR 30–59 mL/min/1.73 m2 | Stage 4 GFR 15–29 mL/min/1.73 m2 | Stage 5 GFR <15 mL/min/1.73 m2 | p * | |
|---|---|---|---|---|---|---|
| C–G | 133.45 (91.72–186.86) | 105.95 (81.35–141.40) | 161.75 (120.16–229.38) | 532.95 (496.25–566.95) | 539.61 (509.56–569.41) | 0.0001 |
| MDRD | 132.16 (93.47–185.34) | 112.13 (84.95–151.41) | 176.15 (122.20–229.90) | 555.62 (511.53–609.31) | 538.99 (505.49–562.69) | 0.0001 |
| CKD-EPI | 129.30 (93.92–183.99) | 113.60 (79.70–158.20) | 205.80 (143.20–249.60) | 549.95 (505.86–609.61) | 538.99 (505.49–562.69) | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villalpando-Sánchez, D.C.; Barajas-Medina, C.A.; Alvarez-Aguilar, C.; López-Ortiz, G.; Romero-Henríquez, L.F.; Gómez-García, A. Advanced Oxidative Protein Products Had a Diagnostic Accuracy for Identifying Chronic Kidney Disease in Adult Population. Metabolites 2024, 14, 37. https://doi.org/10.3390/metabo14010037
Villalpando-Sánchez DC, Barajas-Medina CA, Alvarez-Aguilar C, López-Ortiz G, Romero-Henríquez LF, Gómez-García A. Advanced Oxidative Protein Products Had a Diagnostic Accuracy for Identifying Chronic Kidney Disease in Adult Population. Metabolites. 2024; 14(1):37. https://doi.org/10.3390/metabo14010037
Chicago/Turabian StyleVillalpando-Sánchez, Diana Carolina, César Arturo Barajas-Medina, Cleto Alvarez-Aguilar, Geovani López-Ortiz, Luisa F. Romero-Henríquez, and Anel Gómez-García. 2024. "Advanced Oxidative Protein Products Had a Diagnostic Accuracy for Identifying Chronic Kidney Disease in Adult Population" Metabolites 14, no. 1: 37. https://doi.org/10.3390/metabo14010037
APA StyleVillalpando-Sánchez, D. C., Barajas-Medina, C. A., Alvarez-Aguilar, C., López-Ortiz, G., Romero-Henríquez, L. F., & Gómez-García, A. (2024). Advanced Oxidative Protein Products Had a Diagnostic Accuracy for Identifying Chronic Kidney Disease in Adult Population. Metabolites, 14(1), 37. https://doi.org/10.3390/metabo14010037