
Association of Metabolomic Biomarkers with Sleeve Gastrectomy Weight Loss Outcomes



 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Cohort
- Body mass index (BMI)
- ○
- 40 kg/m2 or above;
- ○
- Or 35 to <40 kg/m2 with an obesity-related comorbidity, such as type 2 diabetes, heart disease, or obstructive sleep apnea [19].
- Age 18–70 years old.
- Enrolled in the health system’s multidisciplinary bariatric surgery program.
- Inability to comply with regular post-operative follow-up visits,
- Pregnancy, and
- Any medical or psychiatric condition which in the opinion of the investigator makes the patient unlikely to be able to properly participate in this study.
2.2. Measures and Samples
2.3. Metabolomic Analyses
2.3.1. 1H NMR Analysis Sample Preparation
Fecal Samples
Serum Samples
1H NMR Data Acquisition
2.3.2. DI-LC/MS/MS Sample Preparation and Analysis
2.4. Statistical Analyses
2.4.1. Univariate Analysis
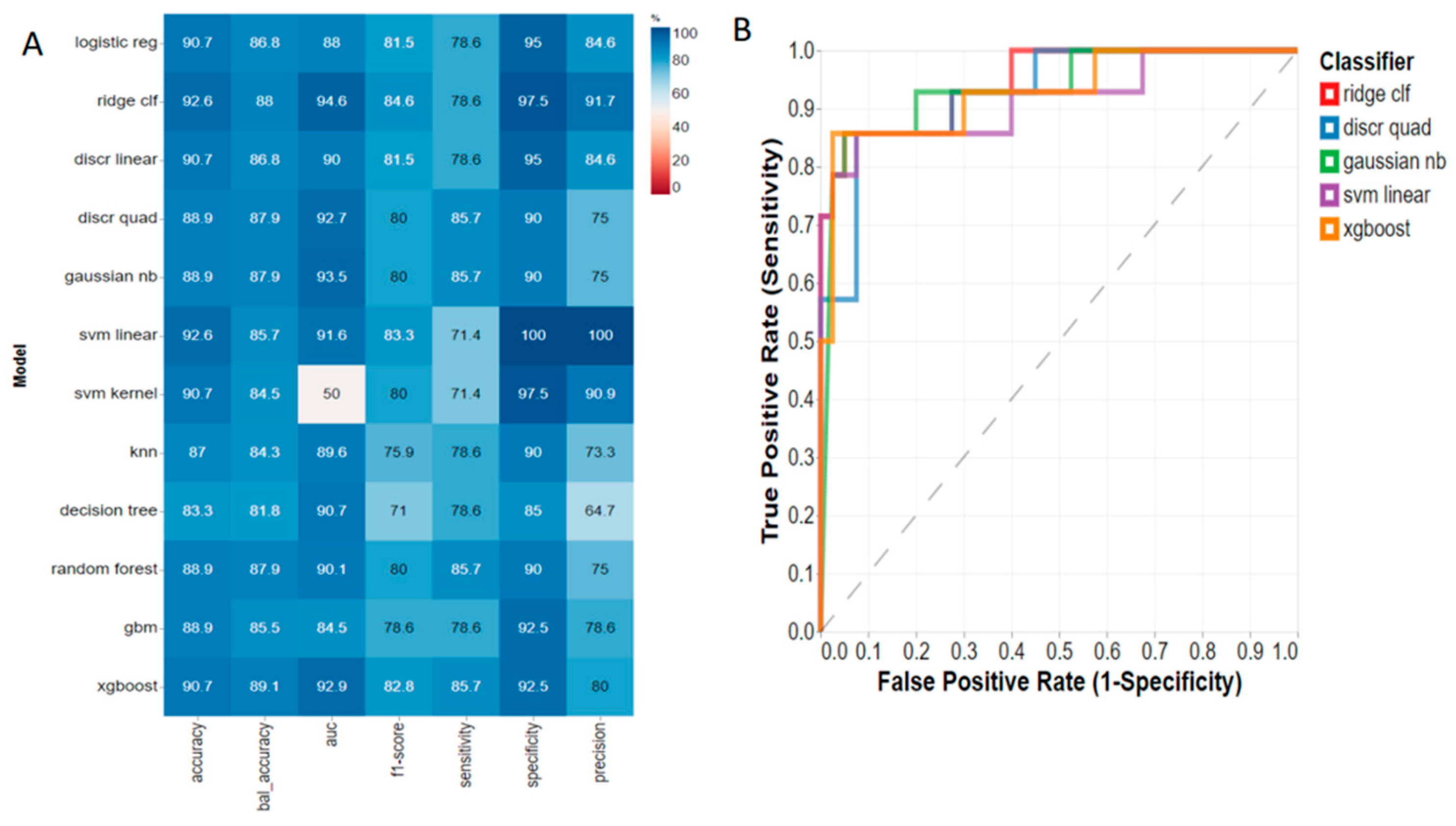
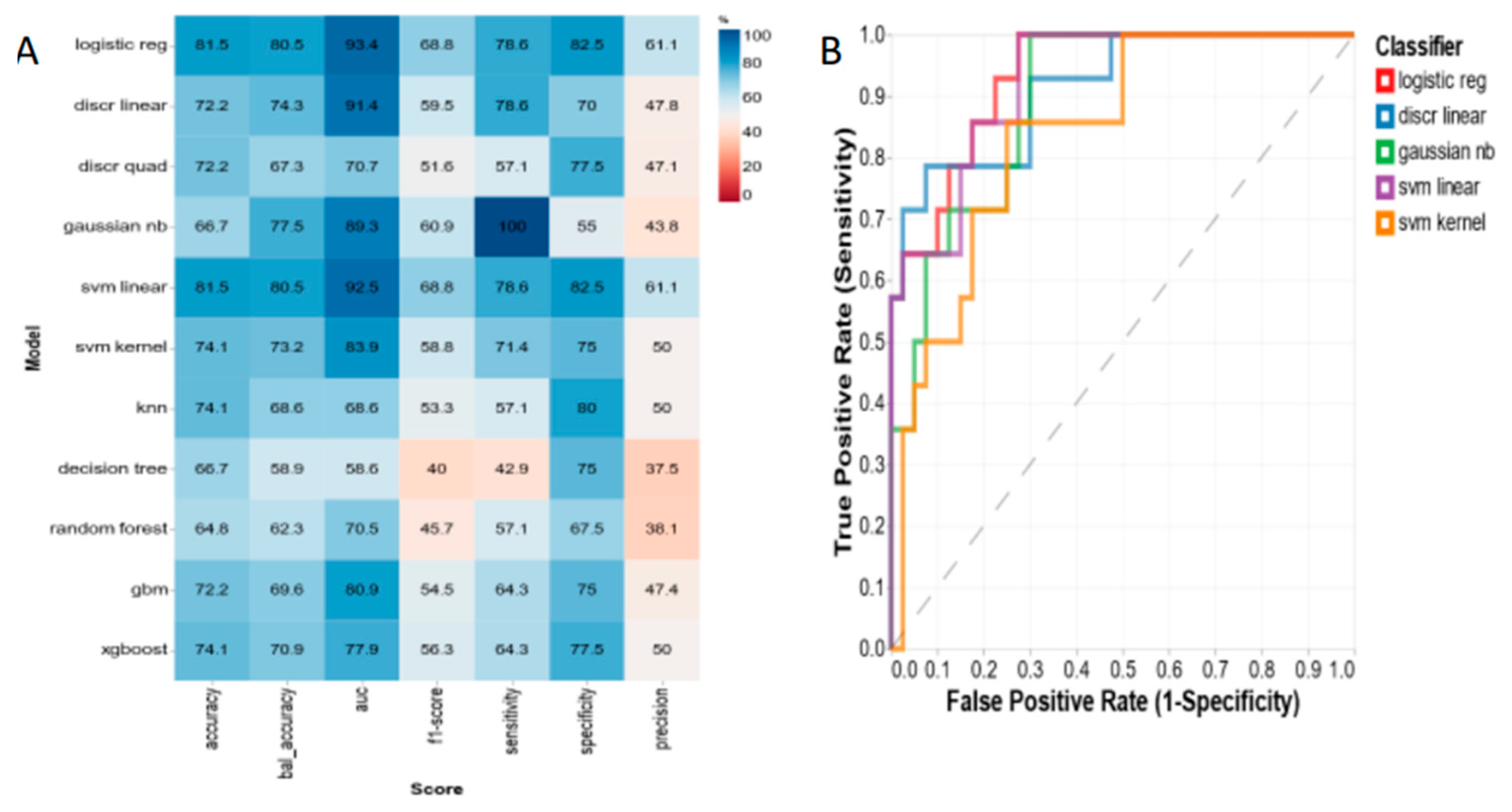
2.4.2. Machine Learning Models
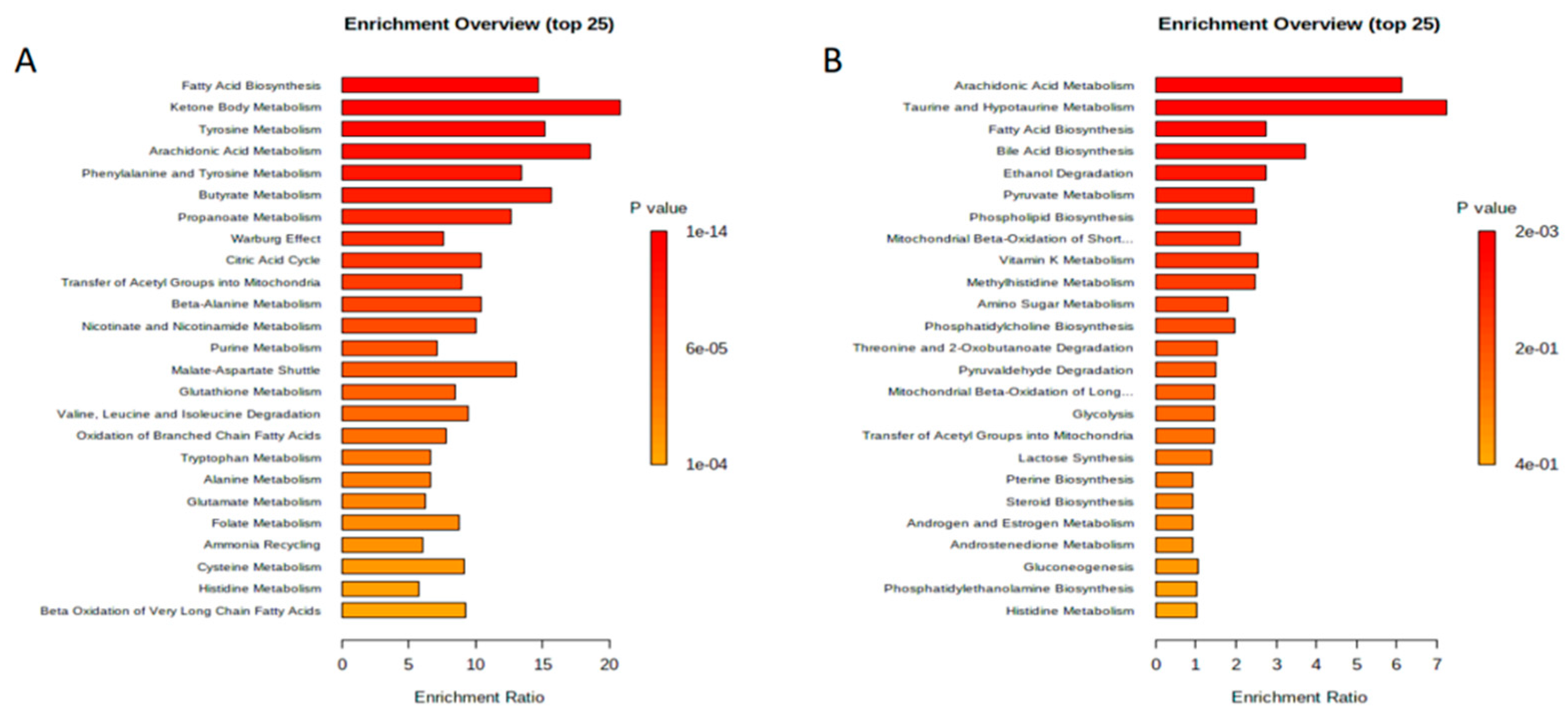
2.5. Metabolic Set-Enrichment Analysis
3. Results
3.1. Serum Metabolomics
3.2. Fecal Metabolomics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention, Overweight and Obesity. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 4 February 2023).
- Perri, M.G. Effects of behavioral treatment on long-term weight loss: Lessons learned from the look AHEAD trial. Obesity 2014, 22, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Keith, J.N. Pharmacotherapy in Treatment of Obesity. Gastroenterol. Clin. N. Am. 2016, 45, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Puzziferri, N.; Roshek, T.B., 3rd; Mayo, H.G.; Gallagher, R.; Belle, S.H.; Livingston, E.H. Long-term follow-up after bariatric surgery: A systematic review. JAMA 2014, 312, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Hutter, M.M.; Schirmer, B.D.; Jones, D.B. Laparoscopic sleeve gastrectomy has morbidity and effectiveness positioned between the band and the bypass. Ann. Surg. 2011, 254, 410. [Google Scholar] [CrossRef] [PubMed]
- English, W.J.; DeMaria, E.J.; Hutter, M.M.; Kothari, S.N.; Mattar, S.G.; Brethauer, S.A.; Morton, J.M. American Society for Metabolic and Bariatric Surgery 2018 estimate of metabolic and bariatric procedures performed in the United States. Surg. Obes. Relat. Dis. 2020, 16, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Lindon, J.C. Systems biology: Metabolomics. Nature 2008, 455, 1054–1056. [Google Scholar] [CrossRef]
- Wishart, D.S.; Knox, C.; Guo, A.C.; Eisner, R.; Young, N.; Gautam, B.; Hau, D.D.; Psychogios, N.; Dong, E.; Bouatra, S.; et al. HMDB: A knowledgebase for the human metabolome. Nucleic Acids Res. 2009, 37, D603–D610. [Google Scholar] [CrossRef]
- Gralka, E.; Luchinat, C.; Tenori, L.; Ernst, B.; Thurnheer, M.; Schultes, B. Metabolomic fingerprint of severe obesity is dynamically affected by bariatric surgery in a procedure-dependent manner. Am. J. Clin. Nutr. 2015, 102, 1313–1322. [Google Scholar] [CrossRef]
- Zhou, J.; Yin, Y. Strategies for large-scale targeted metabolomics quantification by liquid chromatography-mass spectrometry. Analyst 2016, 141, 6362–6373. [Google Scholar] [CrossRef]
- Sussulini, A. (Ed.) Metabolomics: From Fundamentals to Clinical Applications; Springer: Berlin/Heidelberg, Germany, 2017; Volume 965. [Google Scholar]
- Nicholson, J.K.; Lindon, J.C.; Holmes, E. ‘Metabonomics’: Understanding the metabolic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica 1999, 29, 1181–1189. [Google Scholar] [CrossRef]
- Nicholson, J.K. Global systems biology, personalized medicine and molecular epidemiology. Mol. Syst. Biol. 2006, 2, 52. [Google Scholar] [CrossRef] [PubMed]
- Shockcor, J.P.; Holmes, E. Metabonomic applications in toxicity screening and disease diagnosis. Curr. Top. Med. Chem. 2002, 2, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.; Jang, M.; Lee, Y.; Ha, J.; Park, S. Amino Acid Metabolites and Slow Weight Loss in the Early Postoperative Period after Sleeve Gastrectomy. J. Clin. Med. 2020, 9, 2348. [Google Scholar] [CrossRef] [PubMed]
- Cuperlovic-Culf, M. Machine Learning Methods for Analysis of Metabolic Data and Metabolic Pathway Modeling. Metabolites 2018, 8, 4. [Google Scholar] [CrossRef] [PubMed]
- Kouznetsova, V.L.; Kim, E.; Romm, E.L.; Zhu, A.; Tsigelny, I.F. Recognition of early and late stages of bladder cancer using metabolites and machine learning. Metabolomics 2019, 15, 94. [Google Scholar] [CrossRef]
- Liebal, U.W.; Phan, A.N.T.; Sudhakar, M.; Raman, K.; Blank, L.M. Machine Learning Applications for Mass Spectrometry-Based Metabolomics. Metabolites 2020, 10, 243. [Google Scholar] [CrossRef]
- NIH. National Institute of Diabetes and Digestive and Kidney Disease: Weight-Loss (Bariatric) Surgery. Available online: https://www.niddk.nih.gov/health-information/weight-management/bariatric-surgery/potential-candidates (accessed on 4 February 2023).
- Mercier, P.; Lewis, M.J.; Chang, D.; Baker, D.; Wishart, D.S. Towards automatic metabolomic profiling of high-resolution one-dimensional proton NMR spectra. J. Biomol. NMR. 2011, 49, 307–323. [Google Scholar] [CrossRef]
- Ravanbakhsh, S.; Liu, P.; Bjordahl, T.C.; Mandal, R.; Grant, J.R.; Wilson, M.; Eisner, R.; Sinelnikov, I.; Hu, X.; Luchinat, C.; et al. Accurate, fully-automated NMR spectral profiling for metabolomics. PLoS ONE 2015, 10, e0124219. [Google Scholar] [CrossRef]
- Barupal, D.K.; Fan, S.; Fiehn, O. Integrating bioinformatics approaches for a comprehensive interpretation of metabolomics datasets. Curr. Opin. Biotechnol. 2018, 54, 1–9. [Google Scholar] [CrossRef]
- Richhariya, B.; Tanveer, M.; Rashid, A.H. Diagnosis of Alzheimer’s disease using universum support vector machine based recursive feature elimination (USVM-RFE). Biomed. Signal Process. Control 2020, 59, 101903. [Google Scholar] [CrossRef]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.-É.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the gap between raw spectra and functional insights. Nucleic Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S. The physiological and pathophysiological roles of taurine in adipose tissue in relation to obesity. Life Sci. 2017, 186, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Sonnweber, T.; Pizzini, A.; Nairz, M.; Weiss, G.; Tancevski, I. Arachidonic Acid Metabolites in Cardiovascular and Metabolic Diseases. Int. J. Mol. Sci. 2018, 19, 3285. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Larrauri, A.; Presa, N.; Dominguez-Herrera, A.; Ouro, A.; Trueba, M.; Gomez-Muñoz, A. Role of bioactive sphingolipids in physiology and pathology. Essays Biochem. 2020, 64, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Krivosheev, A.B.; Kuimov, A.D.; Kondratova, M.A.; Tuguleva, T.A. Porphyrin metabolism in women with metabolic syndrome. Klin. Med. (Mosk) 2014, 92, 49–54. [Google Scholar] [PubMed]
- Carlsson, E.R.; Allin, K.H.; Madsbad, S.; Fenger, M. Phosphatidylcholine and its relation to apolipoproteins A-1 and B changes after Roux-en-Y gastric bypass: A cohort study. Lipids Health Dis. 2019, 18, 169. [Google Scholar] [CrossRef]
- Lee, G.; Park, Y.S.; Cho, C.; Lee, H.; Park, J.; Park, D.J.; Lee, J.H.; Lee, H.-J.; Ha, T.K.; Kim, Y.-J.; et al. Short-term changes in the serum metabolome after laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass. Metabolomics 2021, 17, 71. [Google Scholar] [CrossRef]
- Noel, O.F.; Still, C.D.; Argyropoulos, G.; Edwards, M.; Gerhard, G.S. Bile Acids, FXR, and Metabolic Effects of Bariatric Surgery. J. Obes. 2016, 2016, 4390254. [Google Scholar] [CrossRef]
- Mor, A.; Sharp, L.; Portenier, D.; Sudan, R.; Torquati, A. Weight loss at first postoperative visit predicts long-term outcome of Roux-en-Y gastric bypass using Duke weight loss surgery chart. Surg. Obes. Relat. Dis. 2012, 8, 556–560. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cohort (N = 45) | T3 (n = 15) | T1 (n = 15) | p-Value (T3 vs. T1) | |
|---|---|---|---|---|
| Age (years) | 48.2 ± 11.5 | 47.3 ± 12.1 | 51.0 ± 9.4 | 0.35 |
| Weight (kg) | 125.7 ± 20.6 | 123.8 ± 25.1 | 130.6 ± 18.7 | 0.38 |
| BMI (kg/m2) | 45.3 ± 7.3 | 42.0 ± 5.4 | 48.8 ± 8.7 | 0.02 |
| Gender (female) | 89% | 73% | 100% | 0.10 |
| Race | ||||
| - White | 60% | 73% | 60% | 0.43 |
| - Black | 36% | 20% | 40% | |
| - Two races | 2% | 7% | 0% | |
| - Native American | 2% | 0% | 0% | |
| Diabetes | 29% | 13% | 40% | 0.22 |
| Dyslipidemia | 56% | 53% | 47% | 0.72 |
| Hypertension | 64% | 53% | 80% | 0.12 |
| Tertile 1 (T1) | Tertile 2 (T2) | Tertile 3 (T3) |
|---|---|---|
| Hydroxybutyric acid | Hydroxybutyric acid | Acetone |
| Citric acid | Acetoacetate | Hydroxybutyric acid |
| Acetone | Citric acid | Acetoacetate |
| Acetoacetate | Acetone | Citric acid |
| Tertile 1 (T1) | Tertile 2 (T2) | Tertile 3 (T3) |
|---|---|---|
| Phosphatidylcholine (PC aa C40:1) | Phosphatidylcholine (PC aa C40:1) | Phosphatidylcholine (PC aa C40:1) |
| Hydroxyoctadecenoylcarnitine (C18:1-OH) | Hydroxyoctadecenoylcarnitine (C18:1-OH) | Hydroxyoctadecenoylcarnitine (C18:1-OH) |
| Glycerophospholipid (PC aa C36:0) | Glycerophospholipid (PC aa C36:0) | Glycerophospholipid (PC aa C36:0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, W.M.; Ziegler, K.M.; Yilmaz, A.; Saiyed, N.; Ustun, I.; Akyol, S.; Idler, J.; Sims, M.D.; Maddens, M.E.; Graham, S.F. Association of Metabolomic Biomarkers with Sleeve Gastrectomy Weight Loss Outcomes. Metabolites 2023, 13, 506. https://doi.org/10.3390/metabo13040506
Miller WM, Ziegler KM, Yilmaz A, Saiyed N, Ustun I, Akyol S, Idler J, Sims MD, Maddens ME, Graham SF. Association of Metabolomic Biomarkers with Sleeve Gastrectomy Weight Loss Outcomes. Metabolites. 2023; 13(4):506. https://doi.org/10.3390/metabo13040506
Chicago/Turabian StyleMiller, Wendy M., Kathryn M. Ziegler, Ali Yilmaz, Nazia Saiyed, Ilyas Ustun, Sumeyya Akyol, Jay Idler, Matthew D. Sims, Michael E. Maddens, and Stewart F. Graham. 2023. "Association of Metabolomic Biomarkers with Sleeve Gastrectomy Weight Loss Outcomes" Metabolites 13, no. 4: 506. https://doi.org/10.3390/metabo13040506
APA StyleMiller, W. M., Ziegler, K. M., Yilmaz, A., Saiyed, N., Ustun, I., Akyol, S., Idler, J., Sims, M. D., Maddens, M. E., & Graham, S. F. (2023). Association of Metabolomic Biomarkers with Sleeve Gastrectomy Weight Loss Outcomes. Metabolites, 13(4), 506. https://doi.org/10.3390/metabo13040506