

Serum Metabolome Adaptations Following 12 Weeks of High-Intensity Interval Training or Moderate-Intensity Continuous Training in Obese Older Adults

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Exercise Interventions
2.3.1. High-Intensity Interval Training (HIIT)
2.3.2. Moderate-Intensity Continuous Training (MICT)
2.4. Clinical Parameters
2.5. Biological Parameters
2.6. Metabolomic Profiling
2.7. Statistical Analyses
3. Results
3.1. Clinical and Biological Characteristics
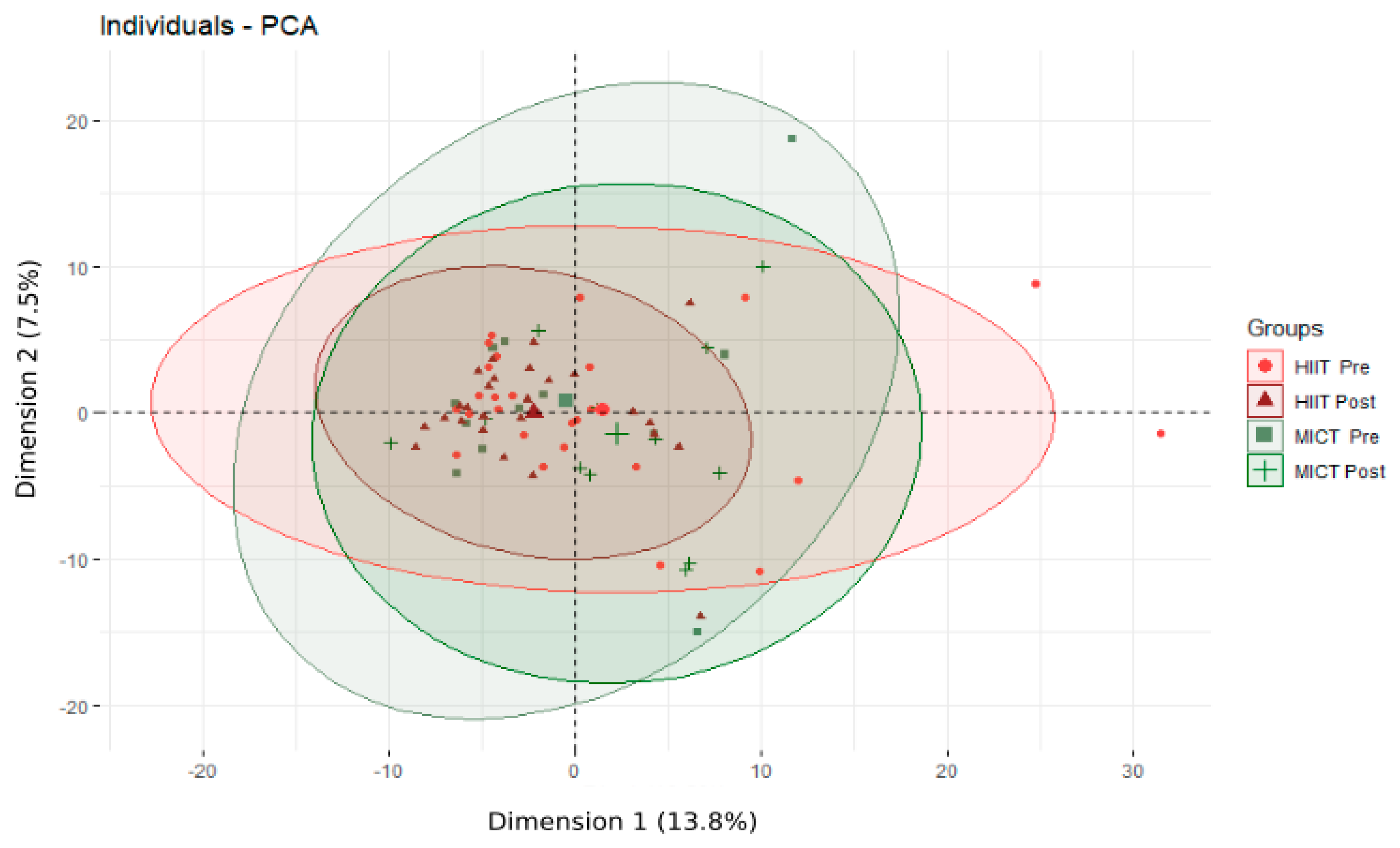
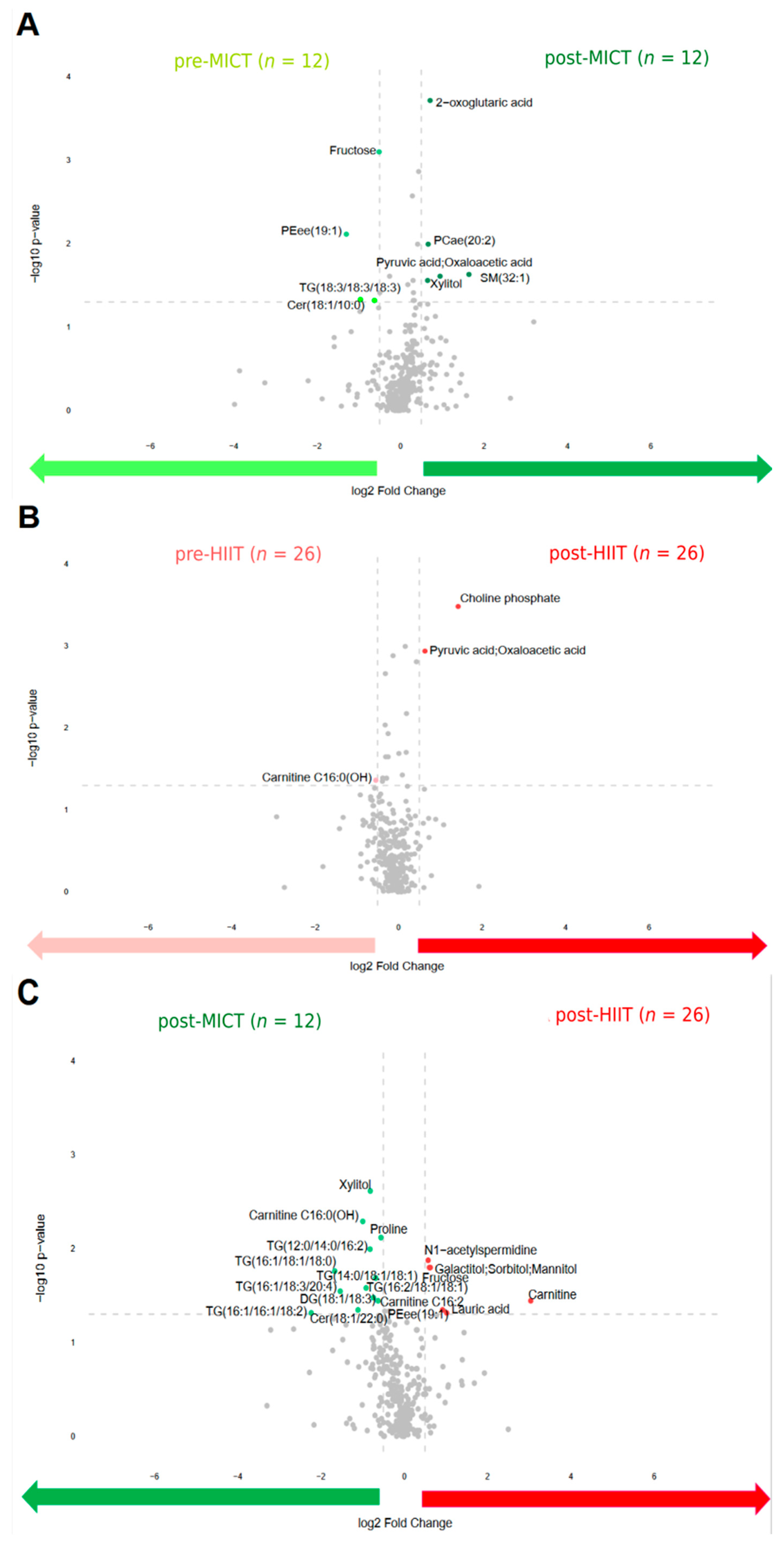
3.2. Overall Metabolomic Profile Adaptations Following the 12-Week Intervention
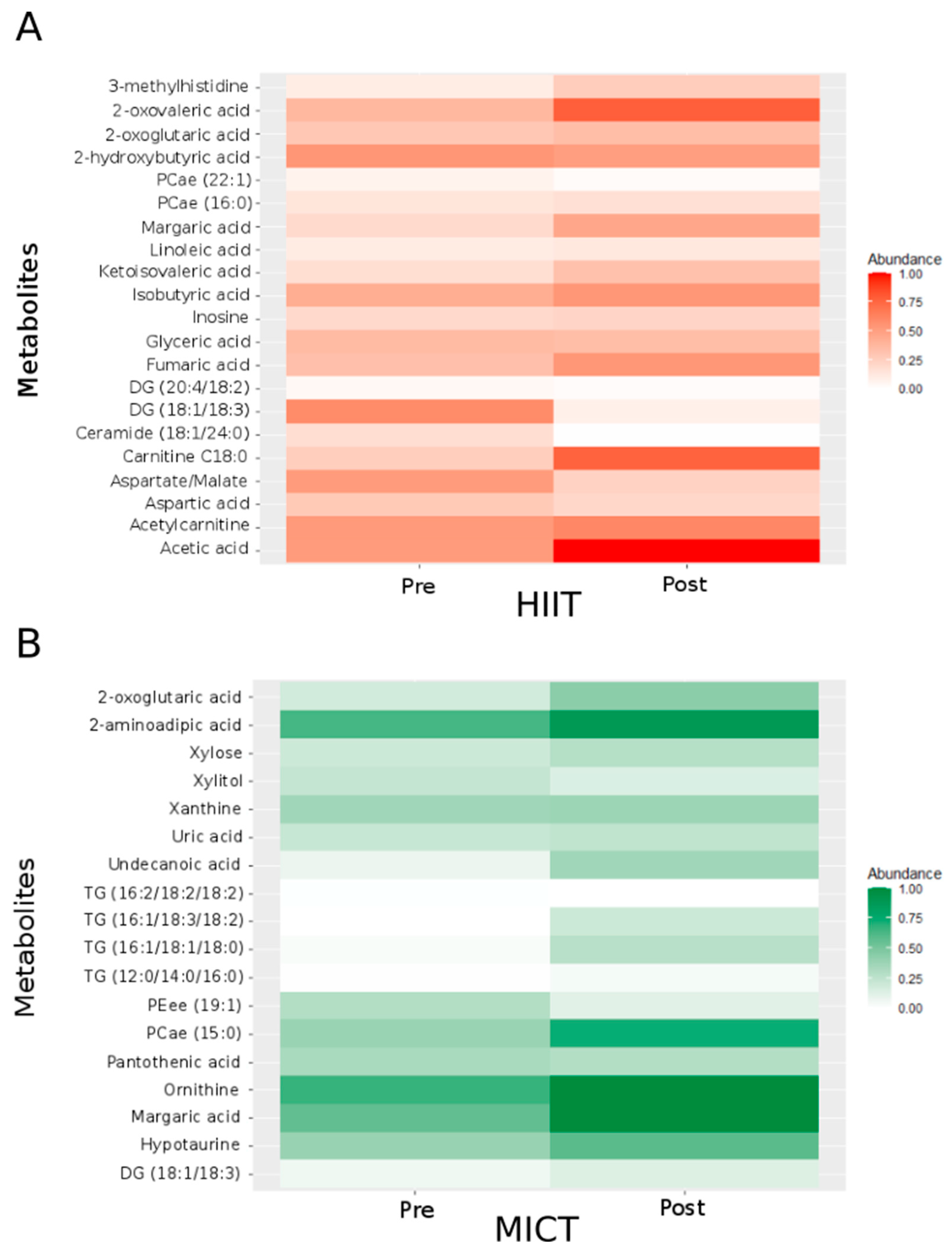
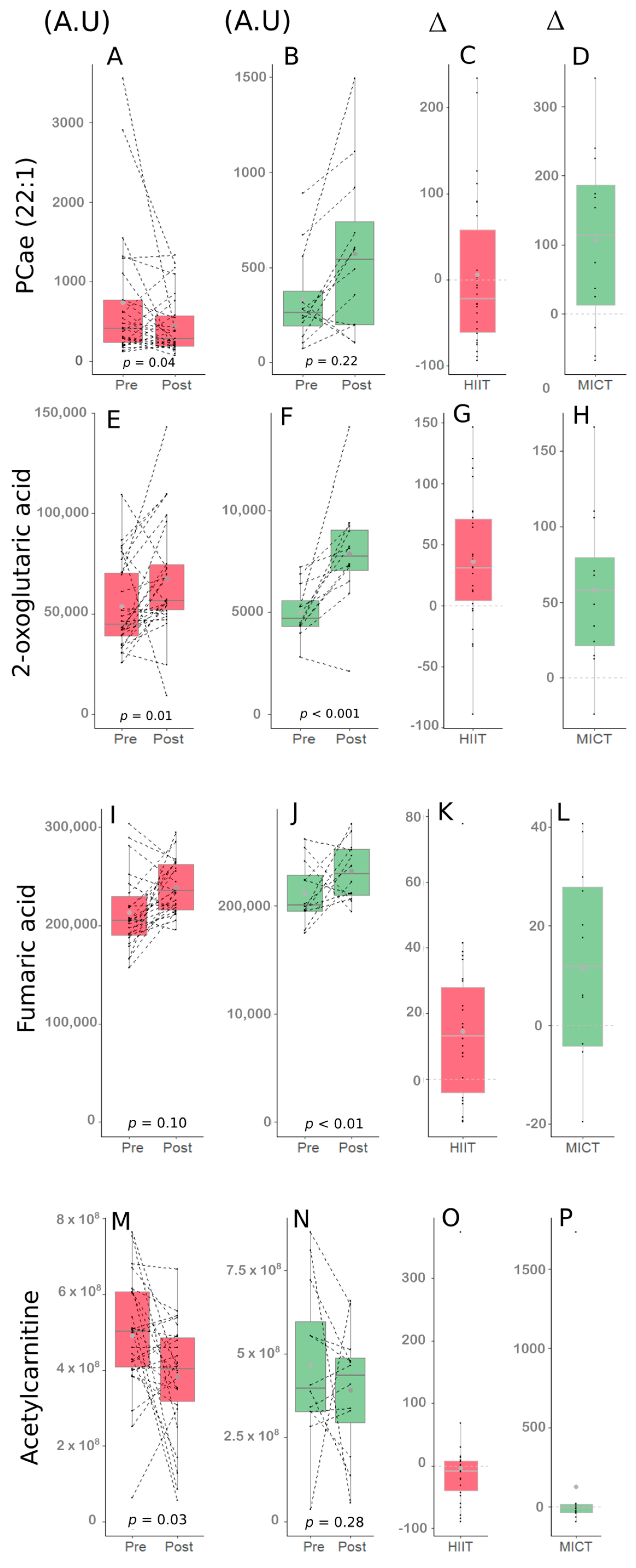
3.3. Alterations of Energetic Metabolisms Following the 12-Week HIIT and MICT Intervention
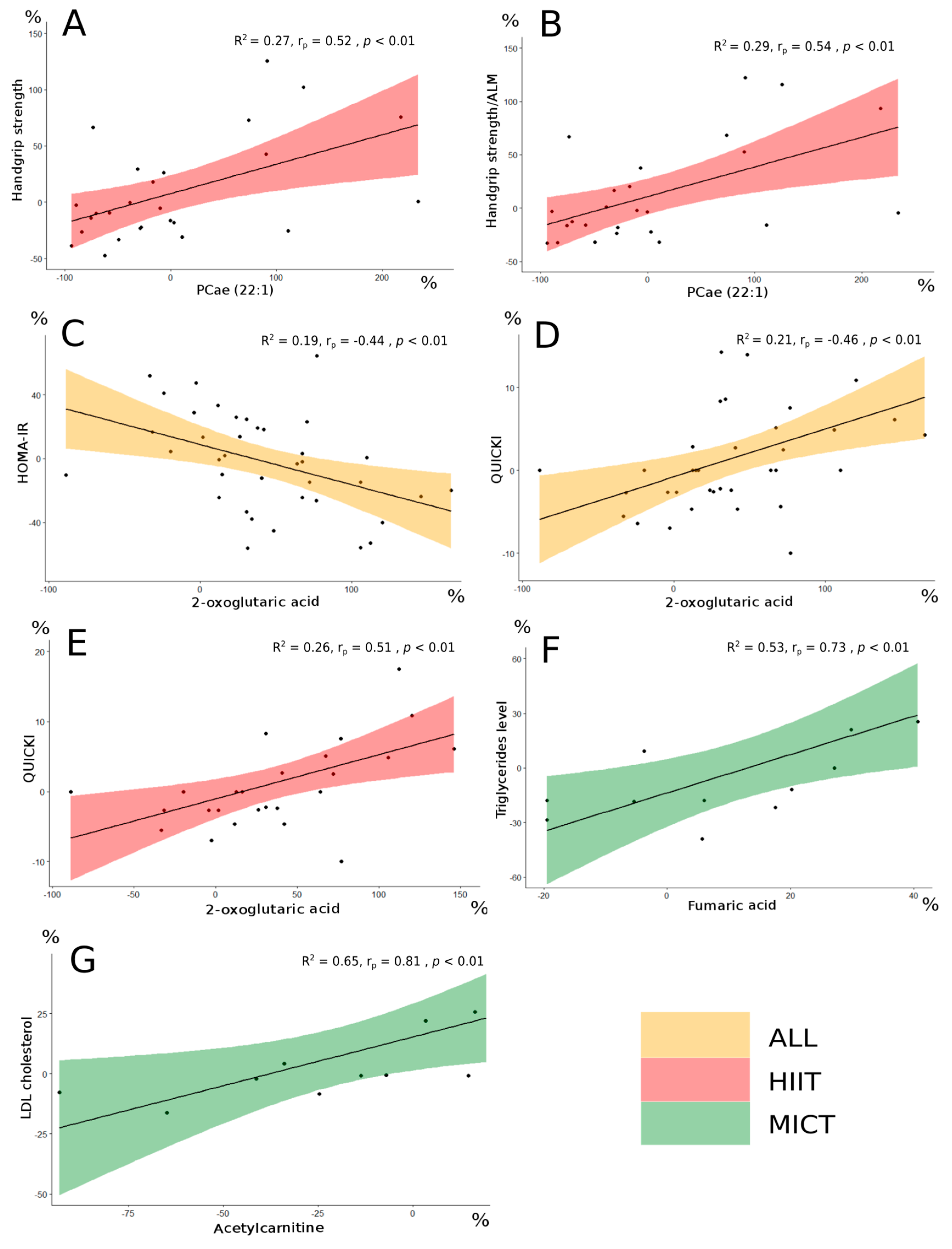
3.4. Associations between Changes in Serum Metabolites and Changes in Clinical and Biological Parameters
4. Discussion
4.1. Metabolome Adaptations
4.2. PCae (22:1) as a Possible Metabolite of Interest for Muscle Strength
4.3. Possible Metabolites of Interest for Glycemic and Lipid Profile Parameters in Obese Older Adults
4.4. Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic Obesity: Time to Meet the Challenge. Obes. Facts 2018, 11, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Youssef, L.; Granet, J.; Marcangeli, V.; Dulac, M.; Hajj-Boutros, G.; Reynaud, O.; Buckinx, F.; Gaudreau, P.; Morais, J.A.; Mauriege, P.; et al. Clinical and Biological Adaptations in Obese Older Adults Following 12-Weeks of High-Intensity Interval Training or Moderate-Intensity Continuous Training. Healthcare 2022, 10, 1346. [Google Scholar] [CrossRef] [PubMed]
- Marcangeli, V.; Youssef, L.; Dulac, M.; Carvalho, L.P.; Hajj-Boutros, G.; Reynaud, O.; Guegan, B.; Buckinx, F.; Gaudreau, P.; Morais, J.A.; et al. Impact of high-intensity interval training with or without l-citrulline on physical performance, skeletal muscle, and adipose tissue in obese older adults. J. Cachexia Sarcopenia Muscle 2022, 13, 1526–1540. [Google Scholar] [CrossRef] [PubMed]
- Duft, R.G.; Castro, A.; Chacon-Mikahil, M.P.T.; Cavaglieri, C.R. Metabolomics and Exercise: Possibilities and perspectives. Mot. Rev. De Educ. Física 2017, 23, e101634. [Google Scholar] [CrossRef]
- Bongiovanni, T.; Pintus, R.; Dessì, A.; Noto, A.; Sardo, S.; Finco, G.; Corsello, G.; Fanos, V. Sportomics: Metabolomics applied to sports. The new revolution? Eur. Rev. Med. Pharm. Sci. 2019, 23, 11011–11019. [Google Scholar] [CrossRef]
- Castro, A.; Duft, R.G.; de Oliveira-Nunes, S.G.; de Andrade, A.L.L.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T. Association Between Changes in Serum and Skeletal Muscle Metabolomics Profile With Maximum Power Output Gains in Response to Different Aerobic Training Programs: The Times Study. Front. Physiol. 2021, 12, 756618. [Google Scholar] [CrossRef]
- Morville, T.; Sahl, R.E.; Moritz, T.; Helge, J.W.; Clemmensen, C. Plasma Metabolome Profiling of Resistance Exercise and Endurance Exercise in Humans. Cell Rep. 2020, 33, 108554. [Google Scholar] [CrossRef]
- Serra, M.C.; Accardi, C.J.; Ma, C.; Park, Y.; Tran, V.; Jones, D.P.; Hafer-Macko, C.E.; Ryan, A.S. Metabolomics of Aerobic Exercise in Chronic Stroke Survivors: A Pilot Study. J. Stroke Cereb. Dis. 2019, 28, 104453. [Google Scholar] [CrossRef]
- Peake, J.M.; Tan, S.J.; Markworth, J.F.; Broadbent, J.A.; Skinner, T.L.; Cameron-Smith, D. Metabolic and hormonal responses to isoenergetic high-intensity interval exercise and continuous moderate-intensity exercise. Am. J. Physiol. Endocrinol. Metab. 2014, 307, E539–E552. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Wang, Y.; Zhao, D.; Zhang, L.; Chen, P.; Xu, X. Integration of metabolomics and proteomics to reveal the metabolic characteristics of high-intensity interval training. Analyst 2020, 145, 6500–6510. [Google Scholar] [CrossRef] [PubMed]
- Brennan, A.M.; Benson, M.; Morningstar, J.; Herzig, M.; Robbins, J.; Gerszten, R.E.; Ross, R. Plasma Metabolite Profiles in Response to Chronic Exercise. Med. Sci. Sport. Exerc. 2018, 50, 1480–1486. [Google Scholar] [CrossRef]
- Palmnas, M.S.A.; Kopciuk, K.A.; Shaykhutdinov, R.A.; Robson, P.J.; Mignault, D.; Rabasa-Lhoret, R.; Vogel, H.J.; Csizmadi, I. Serum Metabolomics of Activity Energy Expenditure and its Relation to Metabolic Syndrome and Obesity. Sci. Rep. 2018, 8, 3308. [Google Scholar] [CrossRef]
- Liu, X.; Wang, G. The Effect of High-Intensity Interval Training on Physical Parameters, Metabolomic Indexes and Serum Ficolin-3 Levels in Patients with Prediabetes and Type 2 Diabetes. Exp. Clin. Endocrinol. Diabetes 2021, 129, 740–749. [Google Scholar] [CrossRef] [PubMed]
- Kuehnbaum, N.L.; Gillen, J.B.; Gibala, M.J.; Britz-McKibbin, P. Personalized Metabolomics for Predicting Glucose Tolerance Changes in Sedentary Women After High-Intensity Interval Training. Sci. Rep. 2014, 4, 6166. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Gouspillou, G.; Carvalho, L.P.; Marcangeli, V.; El Hajj Boutros, G.; Dulac, M.; Noirez, P.; Morais, J.A.; Gaudreau, P.; Aubertin-Leheudre, M. Effect of High-Intensity Interval Training Combined with L-Citrulline Supplementation on Functional Capacities and Muscle Function in Dynapenic-Obese Older Adults. J. Clin. Med. 2018, 7, 561. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. The Reliability and Validity of a 6-Minute Walk Test as a Measure of Physical Endurance in Older Adults. J. Aging Phys. Act. 1998, 6, 363–375. [Google Scholar] [CrossRef]
- ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef]
- Ostir, G.V.; Volpato, S.; Fried, L.P.; Chaves, P.; Guralnik, J.M. Reliability and sensitivity to change assessed for a summary measure of lower body function: Results from the Women’s Health and Aging Study. J. Clin. Epidemiol. 2002, 55, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.M.; Dobson, F.; Martin, J.; Bennell, K.L.; Hinman, R.S. Interrater and intrarater reliability of common clinical standing balance tests for people with hip osteoarthritis. Phys. Ther. 2014, 94, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Christopher, A.; Kraft, E.; Olenick, H.; Kiesling, R.; Doty, A. The reliability and validity of the Timed Up and Go as a clinical tool in individuals with and without disabilities across a lifespan: A systematic review. Disabil. Rehabil. 2021, 43, 1799–1813. [Google Scholar] [CrossRef] [PubMed]
- Csuka, M.; McCarty, D.J. Simple method for measurement of lower extremity muscle strength. Am. J. Med. 1985, 78, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.M.; Chan, R.W.; Fung, Y.K.; Fong, S.S.; Lam, S.S.; Lai, C.W.; Ng, S.S. Reliability and validity of Alternate Step Test times in subjects with chronic stroke. J. Rehabil. Med. 2014, 46, 969–974. [Google Scholar] [CrossRef]
- Danlos, F.X.; Grajeda-Iglesias, C.; Durand, S.; Sauvat, A.; Roumier, M.; Cantin, D.; Colomba, E.; Rohmer, J.; Pommeret, F.; Baciarello, G.; et al. Metabolomic analyses of COVID-19 patients unravel stage-dependent and prognostic biomarkers. Cell Death Dis. 2021, 12, 258. [Google Scholar] [CrossRef]
- Tran, B.-T.T.; Gelin, A.; Durand, S.; Texier, M.; Daste, A.; Toullec, C.; Benihoud, K.; Breuskin, I.; Gorphe, P.; Garic, F.; et al. Plasma galectins and metabolites in advanced head and neck carcinomas: Evidence of distinct immune characteristics linked to hypopharyngeal tumors. OncoImmunology 2023, 12, 2150472. [Google Scholar] [CrossRef]
- Borai, A.; Livingstone, C.; Kaddam, I.; Ferns, G. Selection of the appropriate method for the assessment of insulin resistance. BMC Med. Res. Methodol. 2011, 11, 158. [Google Scholar] [CrossRef]
- Kistner, S.; Rist, M.J.; Kruger, R.; Doring, M.; Schlechtweg, S.; Bub, A. High-Intensity Interval Training Decreases Resting Urinary Hypoxanthine Concentration in Young Active Men-A Metabolomic Approach. Metabolites 2019, 9, 137. [Google Scholar] [CrossRef]
- Rebholz, C.M.; Lichtenstein, A.H.; Zheng, Z.; Appel, L.J.; Coresh, J. Serum untargeted metabolomic profile of the Dietary Approaches to Stop Hypertension (DASH) dietary pattern. Am. J. Clin. Nutr. 2018, 108, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Zhang, J.; Fang, B.; Tian, X.; Feng, Y.; Cheng, Z.; Fu, Z.; Zhang, J.; Wu, J. Runners’ metabolomic changes following marathon. Nutr. Metab. 2020, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.B.; Haggerty, C.L.; Goodpaster, B.; Harris, T.; Kritchevsky, S.; Nevitt, M.; Miles, T.P.; Visser, M. Strength and muscle quality in a well-functioning cohort of older adults: The Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2003, 51, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Syddall, H.; Cooper, C.; Martin, F.; Briggs, R.; Aihie Sayer, A. Is grip strength a useful single marker of frailty? Age Ageing 2003, 32, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.K.S.; Kovalik, J.P.; Ching, J.; Chan, A.W.; Matchar, D.B. Novel metabolomics markers are associated with pre-clinical decline in hand grip strength in community-dwelling older adults. Mech. Ageing Dev. 2021, 193, 111405. [Google Scholar] [CrossRef] [PubMed]
- van der Veen, J.N.; Kennelly, J.P.; Wan, S.; Vance, J.E.; Vance, D.E.; Jacobs, R.L. The critical role of phosphatidylcholine and phosphatidylethanolamine metabolism in health and disease. Biochim. Biophys. Acta Biomembr. 2017, 1859 Pt B, 1558–1572. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HIIT | MICT | p-Value | |
|---|---|---|---|
| Age (years) | 67.73 ± 3.87 | 70.41 ± 3.89 | 0.71 |
| Men/women (n) | 13/13 | 8/4 | N/A |
| Fat mass (%—Men/Women) | 33.03 ± 5.01 | 43.30 ± 6.38 | 0.64/0.60 |
| BMI (kg/m2) | 29.77 ± 2.96 | 30.08 ± 7.66 | 0.53 |
| Total fat mass (%) | 37.75 ± 7.93 | 37.34 ± 7.22 | 0.87 |
| Android fat mass (%) | 47.07 ± 7.46 | 47.47 ± 5.90 | 0.87 |
| Gynoid fat mass (%) | 39.88 ± 10.48 | 38.75 ± 11.05 | 0.75 |
| Steps per day (n) | 6658 ± 3299 | 6595 ± 2454 | 0.81 |
| Energy intake (kcal/day) | 2308 ± 466 | 2153 ± 521 | 0.39 |
| MoCA (/30) | 27.24 ± 2.23 | 27.76 ± 2.34 | 0.07 |
| Metabolites | HIIT (n = 26) | MICT (n = 12) | p-Value | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Time Effect | Time × Group Effect | |
| TCA cycle | ||||||
| 2-oxoglutaric acid | 5.4 × 104 ± 2.2 × 104 | 6.7 × 104 ± 2.9 × 104 # | 5.0 × 104 ± 1.3 × 104 | 7.9 × 104 ± 2.7 × 104 ### | 0.0002 | 0.13 |
| 3-methylhistidine | 1.4 × 104 ± 3.9 × 103 | 1.2 × 104 ± 3.5 × 103 # | 1.4 × 104 ± 2.3 × 103 | 1.1 × 104 ± 2.0 × 103 | 0.006 | 0.79 |
| Aspartic acid | 3.7 × 105 ± 2.2 × 105 | 2.6 × 105 ± 8.2 × 104 ## | 1.5 × 105 ± 4.8 × 104 | 2.4 × 105 ± 6.6 × 104 | 0.12 | 0.005 |
| Fumaric acid | 2.1 × 105 ± 3.7 × 104 | 2.4 × 105 ± 2.6 × 104 ## | 2.1 × 105 ± 2.8 × 104 | 2.3 × 105 ± 2.7 × 104 | 0.001 | 0.71 |
| Pyruvic acid and Oxaloacetic acid | 3.6 × 105 ± 3.0 × 105 | 4.9 × 105 ± 3.2 × 105 | 3.6 × 105 ± 1.9 × 105 | 5.8 × 105 ± 5.6 × 105 | 0.03 | 0.56 |
| Aspartate/Malate | 3.82 ± 1.81 | 2.81 ± 1.08 ## | 1.72 ± 0.56 | 2.58 ± 0.98 | 0.13 | 0.003 |
| Carbohydrate metabolism | ||||||
| Acetic acid | 3.7 × 104 ± 3.4 × 103 | 3.4 × 104 ± 5.3 × 103 # | 3.7 × 104 ± 6.0 × 103 | 3.6 × 104 ± 5.3 × 103 | 0.04 | 0.32 |
| Glyceric acid | 2.1 × 106 ± 6.4 × 105 | 1.6 × 106 ± 3.7 × 105 ### | 1.6 × 106 ± 5.4 × 105 | 1.4 × 106 ± 2.4 × 105 | <0.0001 | 0.09 |
| Ribitol | 1.4 × 105 ± 3.0 × 104 | 1.4 × 105 ± 2.6 × 104 | 1.3 × 105 ± 2.9 × 104 | 1.4 × 105 ± 2.4 × 104 | 0.75 | 0.04 |
| Xylitol | 2.8 × 104 ± 8.0 × 103 | 2.9 × 104 ± 5.4 × 103 | 2.9 × 104 ± 7.9 × 103 | 5.2 × 104 ± 3.8 × 104 ### | 0.02 | 0.004 |
| Xylose | 4.1 × 104 ± 1.6 × 104 | 3.9 × 104 ± 8.2 × 103 | 3.2 × 104 ± 4.7 × 103 | 4.3 × 104 ± 8.2 × 103 ## | 0.31 | 0.009 |
| Amino acid metabolism | ||||||
| 2-aminoadipic acid | 5.1 × 105 ± 1.2 × 105 | 4.1 × 105 ± 1.6 × 104 | 1.7 × 105 ± 8.2 × 104 | 4.7 × 105 ± 1.8 × 105 ## | 0.03 | 0.08 |
| 2-hydroxybutyric acid | 3.0 × 104 ± 1.4 × 104 | 3.0 × 104 ± 1.4 × 104 # | 4.9 × 104 ± 1.7 × 104 | 3.0 × 104 ± 1.4 × 104 | 0.12 | 0.04 |
| 2-oxovaleric acid | 6.4 × 103 ± 1.4 × 103 | 5.4 × 103 ± 1.6 × 103 # | 6.1 × 103 ± 1.1 × 103 | 5.5 × 103 ± 1.4 × 103 | 0.01 | 0.57 |
| 3-hydroxybutyric acid | 3.8 × 104 ± 2.5 × 104 | 2.8 × 104 ± 2.0 × 104 | 5.9 × 104 ± 5.6 × 104 | 3.8 × 104 ± 2.2 × 104 | 0.03 | 0.44 |
| Ketoisovaleric acid | 1.0 × 105 ± 3.4 × 104 | 1.1 × 105 ± 3.0 × 104 ## | 8.9 × 104 ± 1.8 × 104 | 1.2 × 105 ± 2.7 × 104 | 0.002 | 0.05 |
| Hypotaurine | 2.1 × 105 ± 8.7 × 104 | 2.2 × 105 ± 8.8 × 104 | 1.9 × 105 ± 6.6 × 104 | 2.7 × 105 ± 7.5 × 104 ## | 0.07 | 0.04 |
| Inosine | 1.9 × 104 ± 6.3 × 103 | 1.5 × 104 ± 3.9 × 103 ### | 1.4 × 104 ± 3.7 × 103 | 1.5 × 104 ± 3.5 × 103 | 0.01 | 0.01 |
| Ornithine | 7.1 × 106 ± 1.7 × 106 | 7.8 × 106 ± 2.4 × 106 | 6.7 × 106 ± 1.8 × 106 | 8.5 × 106 ± 2.5 × 106 # | 0.01 | 0.21 |
| Proline | 2.6 × 106 ± 2.1 × 106 | 2.3 × 106 ± 1.2 × 106 | 2.6 × 106 ± 1.5 × 106 | 3.5 × 106 ± 1.2 × 106 | 0.68 | 0.04 |
| Uric acid | 2.9 × 106 ± 2.2 × 106 | 2.6 × 106 ± 1.4 × 106 | 2.6 × 106 ± 1.2 × 106 | 4.1 × 106 ± 2.2 × 106 ## | 0.36 | 0.002 |
| Xanthine | 3.0 × 104 ± 1.4 × 104 | 2.9 × 104 ± 1.1 × 104 | 1.9 × 104 ± 6.3 × 103 | 2.8 × 104 ± 8.3 × 103 ## | 0.27 | 0.01 |
| Metabolites | HIIT (n = 26) | MICT (n = 12) | p-Value | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Time Effect | Time × Group Effect | |
| Fat metabolism | ||||||
| Acetylcarnitine | 4.9 × 108 ± 1.6 × 108 | 3.8 × 108 ± 1.5 × 108 # | 4.7 × 108 ± 2.4 × 108 | 3.9 × 108 ± 1.9 × 108 | 0.02 | 0.71 |
| Arachidonic acid | 2.4 × 105 ± 1.0 × 105 | 2.8 × 105 ± 8.6 × 104 | 1.7 × 105 ± 6.3 × 104 | 2.2 × 105 ± 7.3 × 104 | 0.02 | 0.78 |
| Butanoic acid | 2.0 × 103 ± 8.4 × 102 | 1.6 × 103 ± 8.2 × 102 | 2.3 × 103 ± 7.8 × 102 | 7.8 × 103 ± 7.9 × 102 | 0.03 | 0.84 |
| Carnitine C18:0 | 68.78 ± 38.11 | 120.40 ± 101.14 # | 84.5 ± 57.0 | 94.92 ± 51.95 | 0.04 | 0.55 |
| Ceramide (18:1/22:0) | 5.9 × 105 ± 4.9 × 105 | 4.0 × 105 ± 3.4 × 105 | 4.9 × 105 ± 4.9 × 105 | 8.7 × 105 ± 7.6 × 105 | 0.94 | 0.02 |
| Ceramide (18:1/24:0) | 8.5 × 106 ± 4.7 × 106 | 6.2 × 106 ± 3.1 × 106 # | 6.7 × 106 ± 4.3 × 106 | 9.1 × 106 ± 4.7 × 106 | 0.39 | 0.03 |
| DG (18:1/18:3) | 1.3 × 103 ± 7.2 × 102 | 9.4 × 102 ± 6.4 × 102 # | 8.9 × 102 ± 8.5 × 102 | 1.8 × 103 ± 1.1 × 103 ## | 0.86 | 0.0004 |
| DG (20:4/18:2) | 8.7 × 102 ± 1.1 × 103 | 4.4 × 102 ± 3.0 × 102 # | 7.9 × 102 ± 9.9 × 102 | 5.2 × 102 ± 4.3 × 102 | 0.04 | 0.67 |
| Isobutyric acid | 1.0 × 104 ± 2.2 × 103 | 8.4 × 103 ± 2.9 × 103 ## | 8.9 × 103 ± 1.1 × 103 | 8.6 × 103 ± 1.2 × 103 | 0.007 | 0.15 |
| Linolenic acid | 1.4 × 108 ± 3.7 × 108 | 1.4 × 107 ± 3.7 × 107 # | 1.4 × 107 ± 3.7 × 107 | 1.4 × 107 ± 3.7 × 107 | 0.03 | 0.66 |
| Margaric acid | 3.6 × 105 ± 8.3 × 104 | 4.1 × 105 ± 7.5 × 104 # | 3.4 × 105 ± 5.0 × 104 | 4.2 × 105 ± 9.6 × 104 ## | 0.001 | 0.28 |
| Pantothenic acid | 1.5 × 104 ± 6.4 × 103 | 1.5 × 104 ± 6.5 × 103 | 1.2 × 104 ± 4.5 × 103 | 1.5 × 104 ± 7.6 × 103 ### | 0.09 | 0.003 |
| PCae (15:0) | 4.8 × 104 ± 3.0 × 104 | 3.5 × 104 ± 1.3 × 104 | 3.1 × 104 ± 1.4 × 104 | 4.1 × 104 ± 1.5 × 104 # | 0.18 | 0.01 |
| PCae (16:0) | 4.7 × 106 ± 3.1 × 106 | 3.5 × 106 ± 1.5 × 106 # | 3.2 × 106 ± 1.1 × 106 | 4.1 × 106 ± 1.4 × 106 | 0.19 | 0.02 |
| PCae (20:2) | 1.4 × 104 ± 1.3 × 104 | 1.1 × 104 ± 6.8 × 103 | 9.7 × 103 ± 5.9 × 103 | 1.5 × 104 ± 7.5 × 103 | 0.75 | 0.03 |
| PCae (22:1) | 7.4 × 102 ± 8.3 × 102 | 4.5 × 102 ± 3.8 × 102 # | 3.3 × 102 ± 2.5 × 102 | 5.7 × 102 ± 4.3 × 102 | 0.29 | 0.03 |
| PCae (22:4) | 1.0 × 103 ± 1.2 × 103 | 7.4 × 102 ± 7.2 × 102 | 5.2 × 102 ± 6.2 × 102 | 1.2 × 103 ± 1.2 × 103 | 0.92 | 0.04 |
| PEaa (36:1) | 2.9 × 105 ± 2.1 × 105 | 2.2 × 105 ± 1.6 × 105 | 2.1 × 105 ± 1.3 × 105 | 3.3 × 105 ± 2.3 × 105 | 0.67 | 0.04 |
| PEaa (38:6) | 1.4 × 104 ± 2.0 × 104 | 7.8 × 105 ± 8.3 × 105 | 1.0 × 105 ± 1.0 × 105 | 2.1 × 105 ± 2.0 × 105 | 0.74 | 0.02 |
| PEee (19:1) | 2.0 × 102 ± 1.6 × 102 | 1.7 × 102 ± 1.0 × 102 | 2.6 × 102 ± 2.2 × 102 | 8.9 × 101 ± 3.0 × 101 ## | 0.02 | 0.03 |
| TG (12:0/12:0/16:1) | 3.3 × 103 ± 4.1 × 103 | 1.7 × 103 ± 1.5 × 103 | 4.8 × 103 ± 8.7 × 103 | 1.7 × 103 ± 1.2 × 103 | 0.04 | 0.48 |
| TG (12:0/14:0/16:0) | 4.7 × 104 ± 6.6 × 104 | 2.6 × 104 ± 1.8 × 104 | 8.1 × 104 ± 1.2 × 105 | 2.5 × 104 ± 2.7 × 104 # | 0.02 | 0.24 |
| TG (14:0/16:0/16:0) | 6.9 × 105 ± 3.5 × 105 | 5.5 × 105 ± 2.2 × 105 | 7.4 × 105 ± 8.7 × 105 | 5.4 × 105 ± 3.7 × 105 | 0.04 | 0.74 |
| TG (14:0/16:2/16:2) | 9.3 × 103 ± 6.0 × 103 | 6.8 × 103 ± 5.6 × 103 | 9.9 × 103 ± 1.0 × 104 | 6.8 × 103 ± 4.6 × 103 | 0.03 | 0.81 |
| TG (16:1/18:1/18:0) | 2.2 × 104 ± 1.9 × 104 | 1.5 × 104 ± 1.7 × 104 | 2.6 × 104 ± 2.4 × 104 | 5.7 × 104 ± 5.5 × 104 ## | 0.35 | 0.003 |
| TG (16:1/18:3/18:2) | 5.7 × 105 ± 8.7 × 106 | 4.4 × 105 ± 8.7 × 106 | 1.5 × 106 ± 8.7 × 106 | 4.8 × 106 ± 8.7 × 106 ### | 0.09 | 0.004 |
| TG (16:1/18:3/20:4) | 3.2 × 104 ± 5.4 × 104 | 1.7 × 104 ± 1.4 × 104 | 1.7 × 104 ± 1.2 × 104 | 4.8 × 104 ± 5.4 × 104 | 0.96 | 0.02 |
| TG (16:2/18:2/18:2) | 8.4 × 104 ± 2.5 × 105 | 7.6 × 104 ± 2.2 × 105 | 5.0 × 105 ± 1.6 × 106 | 2.2 × 106 ± 3.8 × 106 ### | 0.04 | 0.002 |
| Undecanoic acid | 1.4 × 105 ± 5.2 × 104 | 9.4 × 104 ± 3.4 × 104 | 9.3 × 104 ± 3.4 × 104 | 1.2 × 105 ± 4.4 × 104 ### | 0.06 | 0.001 |
| Parameters | Intervention (n = 38) | HIIT (n = 26) | MICT (n = 12) |
|---|---|---|---|
| 6 min walking test | PEee (19:1): 0.6 *** | - | - |
| 4 m walk test normal | TG (12:0/12:0/16:1): 0.45 ** | - | - |
| 4 m walk test fast | Ceramide (18:1/24:0): 0.49 ** DG (18:1/18:3): 0.55 *** TG (16:1/18:1/18:0): 0.61 *** TG (16:1/18:3/18:2): 0.55 *** TG (16:1/18:3/20:4): 0.61 *** | - | - |
| Unipodal Balance Test | - | - | Xanthine: 0.75 ** |
| Chair test | Insosine: 0.48 ** TG (16:1/18:1/18:0): 0.44 ** TG (16:1/18:3/18:2): 0.48 ** | - | 3-methylhistidine: −0.73 ** TG (14:0/16:2/16:2):−0.78 ** |
| Timed Up and Go Test | Ceramide (18:1/22:0): −0.49 ** PEaa (36:1): −0.64 *** | - | |
| Handgrip strength | - | PCae (22:1): 0.52 ** | - |
| Handgrip strength/BW | - | PCae (22:1): 0.54 ** | - |
| Handgrip strength/ALM | - | PCae (22:1): 0.54 ** | Ceramide (18:1/24:0): 0.76 ** |
| Quadriceps strength/BW | - | - | Glyceric acid: −0.82 ** |
| Quadriceps strength/LLM | - | - | 2-hydroxyglutaric acid: 0.77 ** |
| Lower Limb power | Acetic acid: 0.45 ** PCae (16:0): 0.5 ** | - | - |
| Parameters | Intervention (n = 38) | HIIT (n = 26) | MICT (n = 12) |
|---|---|---|---|
| Body weight | Ceramide (18:1/24:0): 0.45 ** PEaa (36:1): 0.44 ** TG (16:1/18:1/18:0): 0.48 ** | - | - |
| BMI | Ceramide (18:1/24:0): 0.45 ** PEaa (36:1): 0.44 ** TG (16:1/18:1/18:0): 0.48 ** | - | - |
| Relative total fat mass | 2-aminoadipic acid: −0.49 ** PCae (20:2): −0.5 ** | Aspartic acid: −0.53 ** Aspartate/Malate: −0.54 ** | Aspartic acid: 0.74 ** |
| Relative arms fat mass | Panthotenic acid: 0.51 *** TG (16:1/18:3/18:2): 0.49 ** | - | - |
| Relative leg fat mass | 2-aminoadipic acid: −0.43 ** PCae (20:2): −0.47 ** | - | TG (14:0/16:2/16:2): 0.75 ** |
| Relative android fat mass | Acetic acid: −0.56 ** | Proline: 0.75 ** Ribitol: 0.72 ** | |
| Relative gynoid fat mass | 2-aminoadipic acid: 0.52 *** Acetylcarnitine: 0.42 ** Aspartic acid: −0.44 ** PCae (20:2): −0.46 ** | Aspartic acid: −0.54 ** Aspartate/Malate: −0.58 ** | PEee (19:1): 0.78 *** |
| Total lean mass | - | - | Fumaric acid: 0.86 ** |
| Parameters | Intervention (n = 38) | HIIT (n = 26) | MICT (n = 12) |
|---|---|---|---|
| Adiponectin/Adipoleptin | Hypotaurine: 0.44 ** | - | - |
| Adiponectin | - | - | TG (16:1/18:3/20:4): 0.78 ** |
| Leptin | - | - | 3-hydroxubutyric acid: −0.78 ** |
| Free fatty acids | Acetic acid: 0.45 ** Ketoisovaleric acid: 0.43 ** Linoleic acid: 0.6 *** | 3-methylhistidine: 0.61 ** | - |
| Total cholesterol | TG (14:0/16:2/16:2): 0.46 ** | - | PEaa (38:6): −0.79 ** |
| LDL cholesterol | - | - | Acetylcarnitine: 0.81 ** |
| Triglycerides | Carnitine C18:0: 0.71 ** | - | Fumaric acid: 0.73 ** |
| Ferritin | - | - | Uric acid: −0.77 ** |
| IGF1 | - | - | Ornithine: −0.78 ** |
| IGF1/IGFBP3 | Butanoic acid: −0.44 ** Aspartate/Malate: 0.46 ** | - | TG (16:1/18:1/18:0): −0.72 ** |
| Glucose | PCae (22:4): −0.46 ** | Linoleic acid: −0.54 ** | - |
| HOMA-IR | 2-oxoglutaric acid: −0.44 ** | Linoleic acid: −0.52 ** | - |
| QUICKI | 2-oxoglutaric acid: 0.46 ** | 2-oxoglutaric acid: 0.51 ** | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, L.; Bourgin, M.; Durand, S.; Aprahamian, F.; Lefevre, D.; Maiuri, M.C.; Marcangeli, V.; Dulac, M.; Hajj-Boutros, G.; Buckinx, F.; et al. Serum Metabolome Adaptations Following 12 Weeks of High-Intensity Interval Training or Moderate-Intensity Continuous Training in Obese Older Adults. Metabolites 2023, 13, 198. https://doi.org/10.3390/metabo13020198
Youssef L, Bourgin M, Durand S, Aprahamian F, Lefevre D, Maiuri MC, Marcangeli V, Dulac M, Hajj-Boutros G, Buckinx F, et al. Serum Metabolome Adaptations Following 12 Weeks of High-Intensity Interval Training or Moderate-Intensity Continuous Training in Obese Older Adults. Metabolites. 2023; 13(2):198. https://doi.org/10.3390/metabo13020198
Chicago/Turabian StyleYoussef, Layale, Mélanie Bourgin, Sylvère Durand, Fanny Aprahamian, Deborah Lefevre, Maria Chiara Maiuri, Vincent Marcangeli, Maude Dulac, Guy Hajj-Boutros, Fanny Buckinx, and et al. 2023. "Serum Metabolome Adaptations Following 12 Weeks of High-Intensity Interval Training or Moderate-Intensity Continuous Training in Obese Older Adults" Metabolites 13, no. 2: 198. https://doi.org/10.3390/metabo13020198
APA StyleYoussef, L., Bourgin, M., Durand, S., Aprahamian, F., Lefevre, D., Maiuri, M. C., Marcangeli, V., Dulac, M., Hajj-Boutros, G., Buckinx, F., Peyrusqué, E., Gaudreau, P., Morais, J. A., Gouspillou, G., Kroemer, G., Aubertin-Leheudre, M., & Noirez, P. (2023). Serum Metabolome Adaptations Following 12 Weeks of High-Intensity Interval Training or Moderate-Intensity Continuous Training in Obese Older Adults. Metabolites, 13(2), 198. https://doi.org/10.3390/metabo13020198