


Changes in Lipoprotein Particles in the Blood Serum of Patients with Lichen Planus

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Volunteer Recruitment
2.2. Blood Samples
2.3. Mass-Spectrometric Analysis
2.4. Data Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fox, B.J.; Odom, R.B. Papulosquamous Diseases: A Review. J. Am. Acad. Dermatol. 1985, 12, 597–624. [Google Scholar] [CrossRef] [PubMed]
- Le Cleach, L.; Chosidow, O. Clinical Practice. Lichen Planus. N. Engl. J. Med. 2012, 366, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Bolognia, J.; Schaffer, J.; Cerroni, L. Dermatology, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 188–199. [Google Scholar]
- Fiocco, Z.; Kupf, S.; Patzak, L.; Kämmerer, T.; Pumnea, T.; French, L.E.; Reinholz, M. Quality of Life and Psychopathology in Lichen Planus: A Neglected Disease Burden. Acta Derm. Venereol. 2021, 101, adv00619. [Google Scholar] [CrossRef]
- Alirezaei, P.; Ahmadpanah, M.; Rezanejad, A.; Soltanian, A.; Bahmani, D.S.; Brand, S. Compared to Controls, Individuals with Lichen Planopilaris Have More Depression, a Lower Self-Esteem, and a Lower Quality of Life. S. Neuropsychobiology 2019, 78, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Jalenques, I.; Lauron, S.; Almon, S.; Pereira, B.; D’Incan, M.; Rondepierre, F. Prevalence and Odds of Signs of Depression and Anxiety in Patients with Lichen Planus: Systematic Review and Meta-Analyses. Acta Derm. Venereol. 2020, 100, adv00330. [Google Scholar] [CrossRef]
- Boch, K.; Langan, E.A.; Kridin, K.; Zillikens, D.; Ludwig, R.J.; Bieber, K. Lichen Planus. Front. Med. 2021, 8, 737813. [Google Scholar] [CrossRef]
- Porter, K.; Klouda, P.; Scully, C.; Bidwell, J.; Porter, S. Class I and II HLA Antigens in British Patients with Oral Lichen Planus. Oral Surg. Oral Med. Oral Pathol. 1993, 75, 176–180. [Google Scholar] [CrossRef]
- Carrozzo, M.; Di Celle, P.F.; Gandolfo, S.; Carbone, M.; Conrotto, D.; Fasano, M.E.; Roggero, S.; Rendine, S.; Ghisetti, V. Increased frequency of HLA-DR6 allele in Italian patients with hepatitis C virus-associated oral lichen planus. Br. J. Dermatol. 2001, 144, 803–808. [Google Scholar] [CrossRef]
- Hussein, M.R. Evaluation of Angiogenesis in Normal and Lichen Planus Skin by CD34 Protein Immunohistochemistry: Preliminary Findings. Cell Biol. Int. 2007, 31, 1292–1295. [Google Scholar] [CrossRef]
- Lehman, J.S.; Tollefson, M.M.; Gibson, L.E. Lichen Planus. Int. J. Dermatol. 2009, 48, 682–694. [Google Scholar] [CrossRef]
- Garcia-Pola, M.J.; Llorente-Pendás, S.; Seoane-Romero, J.M.; Berasaluce, M.J.; García-Martín, J.M. Thyroid Disease and Oral Lichen Planus as Comorbidity: A Prospective Case-Control Study. Dermatology 2016, 232, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.A.; Raju, P.V.K.; Gopal, K.V.T.; Rao, T.N. Comorbidities in Lichen Planus: A Case-Control Study in Indian Patients. Indian Dermatol. Online J. 2019, 10, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Chen, D.; Deng, X.; Xu, Y.; Wang, Y.; Qiu, X.; Yuan, P.; Zhang, Z.; Xu, H.; Jiang, L. Prevalence of Oral Lichen Planus in Patients with Diabetes Mellitus: A Cross-Sectional Study. Oral Dis. 2022; Early View. [Google Scholar] [CrossRef]
- Panchal, F.H.; Ray, S.; Munshi, R.P.; Bhalerao, S.S.; Nayak, C.S. Alterations in Lipid Metabolism and Antioxidant Status in Lichen Planus. Indian J. Dermatol. 2015, 60, 439–455. [Google Scholar] [CrossRef]
- Daye, M.; Işık, B.; Temiz, S.A.; Durduran, Y. Relationship between Acanthosis Nigricans, Acrochordon and Metabolic Syndrome in Patients with Lichen Planus. Int. J. Clin. Pract. 2021, 75, e14687. [Google Scholar] [CrossRef] [PubMed]
- Singla, R.; Ashwini, P.K.; Jayadev, B. Lichen Planus and Metabolic Syndrome: Is There a Relation? Indian Dermatol. Online J. 2019, 10, 555–559. [Google Scholar] [CrossRef]
- Arias-Santiago, S.; Buendia-Eisman, A.; Aneiros-Fernandez, J.; Giron-Prieto, M.S.; Gutierrez-Salmeron, M.T.; Mellado, V.G.; Naranjo-Sintes, R. Cardiovascular Risk Factors in Patients with Lichen Planus. Am. J. Med. 2011, 124, 543–548. [Google Scholar] [CrossRef]
- Lai, Y.C.; Yew, Y.W.; Schwartz, R.A. Lichen Planus and Dyslipidemia: A Systematic Review and Meta-analysis of Observational Studies. Int. J. Dermatol. 2016, 55, e295–e304. [Google Scholar] [CrossRef]
- Leasure, A.C.; Acosta, J.N.; Sansing, L.H.; Sheth, K.N.; Cohen, J.M.; Falcone, G.J. Association of Lichen Planus with Cardiovascular Disease: A Combined Analysis of the UK Biobank and All of Us Study. J. Am. Acad. Dermatol. 2021, 87, 454–456. [Google Scholar] [CrossRef]
- Aksu, F.; Karadag, A.S.; Caliskan, M.; Uzuncakmak, T.K.; Keles, N.; Ozlu, E.; Yilmaz, Y.; Akdeniz, N. Does Lichen Planus Cause Increased Carotid Intima-Media Thickness and Impaired Endothelial Function? Can. J. Cardiol. 2016, 32, 1246.e1–1246.e6. [Google Scholar] [CrossRef]
- Yan, D.; Afifi, L.; Jeon, C.; Trivedi, M.; Chang, H.W.; Lee, K.; Liao, W. The Metabolomics of Psoriatic Disease. Psoriasis Targets Ther. 2017, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ilves, L.; Ottas, A.; Kaldvee, B.; Abram, K.; Soomets, U.; Zilmer, M.; Jaks, V.; Kingo, K. Metabolomic Analysis of Skin Biopsies from Patients with Atopic Dermatitis Reveals Hallmarks of Inflammation, Disrupted Barrier Function and Oxidative Stress. Acta Derm. Venereol. 2021, 101, adv00407. [Google Scholar] [CrossRef]
- Yang, X.-Y.; Zhang, S.-N.; Li, X.-Z.; Wang, Y.; Yin, X.-D. Analysis of Human Serum Metabolome for Potential Biomarkers Identification of Erosive Oral Lichen Planus. Clin. Chim. Acta 2017, 468, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.Á.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral Potentially Malignant Disorders: A Consensus Report from an International Seminar on Nomenclature and Classification, Convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Gouveia-Figueira, S.; Danielsson, K.; Fowler, C.J. Changes in Proportions of Linoleic Acid-Derived Oxylipins in Oral Lichen Planus. Acta Derm. Venereol. 2019, 99, 1051–1052. [Google Scholar] [CrossRef]
- Soininen, P.; Kangas, A.J.; Würtz, P.; Suna, T.; Ala-Korpela, M. Quantitative Serum Nuclear Magnetic Resonance Metabolomics in Cardiovascular Epidemiology and Genetics. Circ. Cardiovasc. Genet. 2015, 8, 192–206. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. 2018. Available online: https://www.R-project.org/ (accessed on 21 April 2021).
- Daye, M.; Temiz, S.A.; Isık, B. The Relationship between Lichen Planus and Metabolic Syndrome. J. Cosmet. Dermatol. 2021, 20, 2635–2639. [Google Scholar] [CrossRef]
- Kolovou, G.D.; Anagnostopoulou, K.K.; Cokkinos, D.V. Pathophysiology of dyslipidaemia in the metabolic syndrome. Postgrad. Med. J. 2005, 81, 358–366. [Google Scholar] [CrossRef]
- Kopin, L.; Lowenstein, C. Dyslipidemia. Ann. Intern. Med. 2017, 167, ITC81–ITC95. [Google Scholar] [CrossRef]
- Illingworth, D.R. Lipoprotein Metabolism. Am. J. Kidney Dis. 1993, 22, 90–97. [Google Scholar] [CrossRef]
- Feingold, K.R.; Anawalt, B.; Boyce, A.; Chrousos, G.; de Herder, W.W.; Dhatariya, K.; Dungan, K.; Hershman, J.M.; Hofland, J.; Kalra, S.; et al. Introduction to Lipids and Lipoproteins. In Endotext; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Mahley, R.W.; Innerarity, T.L.; Rall, S.C., Jr.; Weisgraber, K.H. Plasma Lipoproteins: Apolipoprotein Structure and Function. J. Lipid Res. 1984, 25, 1277–1294. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jornet, P.; Camacho-Alonso, F.; Rodriguez-Martines, M.A. Alterations in serum lipid profile patterns in oral lichen planus: A cross-sectional study. Am. J. Clin. Dermatol. 2012, 13, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Grammer, T.B.; Kleber, M.E.; März, W.; Silbernagel, G.; Siekmeier, R.; Wieland, H.; Pilz, S.; Tomaschitz, A.; Koenig, W.; Scharnagl, H. Low-density lipoprotein particle diameter and mortality: The Ludwigshafen Risk and Cardiovascular Health Study. Eur. Heart J. 2015, 36, 31–38. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ruuth, M.; Nguyen, S.D.; Vihervaara, T.; Hilvo, M.; Laajala, T.D.; Kondadi, P.K.; Gisterå, A.; Lähteenmäki, H.; Kittilä, T.; Huusko, J.; et al. Susceptibility of Low-Density Lipoprotein Particles to Aggregate Depends on Particle Lipidome, Is Modifiable, and Associates with Future Cardiovascular Deaths. Eur. Heart J. 2018, 39, 2562–2573. [Google Scholar] [CrossRef] [PubMed]
- Annema, W.; von Eckardstein, A. Dysfunctional High-Density Lipoproteins in Coronary Heart Disease: Implications for Diagnostics and Therapy. Transl. Res. 2016, 173, 30–57. [Google Scholar] [CrossRef]
- Annema, W.; von Eckardstein, A. High-Density Lipoproteins—Multifunctional but Vulnerable Protections from Atherosclerosis. Circ. J. 2013, 77, 2432–2448. [Google Scholar] [CrossRef]
- Ganjali, S.; Dallinga-Thie, G.M.; Simental-Mendía, L.E.; Banach, M.; Pirro, M.; Sahebkar, A. HDL Functionality in Type 1 Diabetes. Atherosclerosis 2017, 267, 99–109. [Google Scholar] [CrossRef]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef]
- Cardner, M.; Yalcinkaya, M.; Goetze, S.; Luca, E.; Balaz, M.; Hunjadi, M.; Hartung, J.; Shemet, A.; Kraenkel, N.; Radosavljevic, S.; et al. Structure-Function Relationships of HDL in Diabetes and Coronary Heart Disease. JCI Insight 2020, 5, e131491. [Google Scholar] [CrossRef]


{kind=link}
| Composition of Lipoprotein Particles and Metabolites | Mean for LP | Mean for HC | Wilcox-Test LP vs. HC, p < 0.0029 |
|---|---|---|---|
| Large LDL | |||
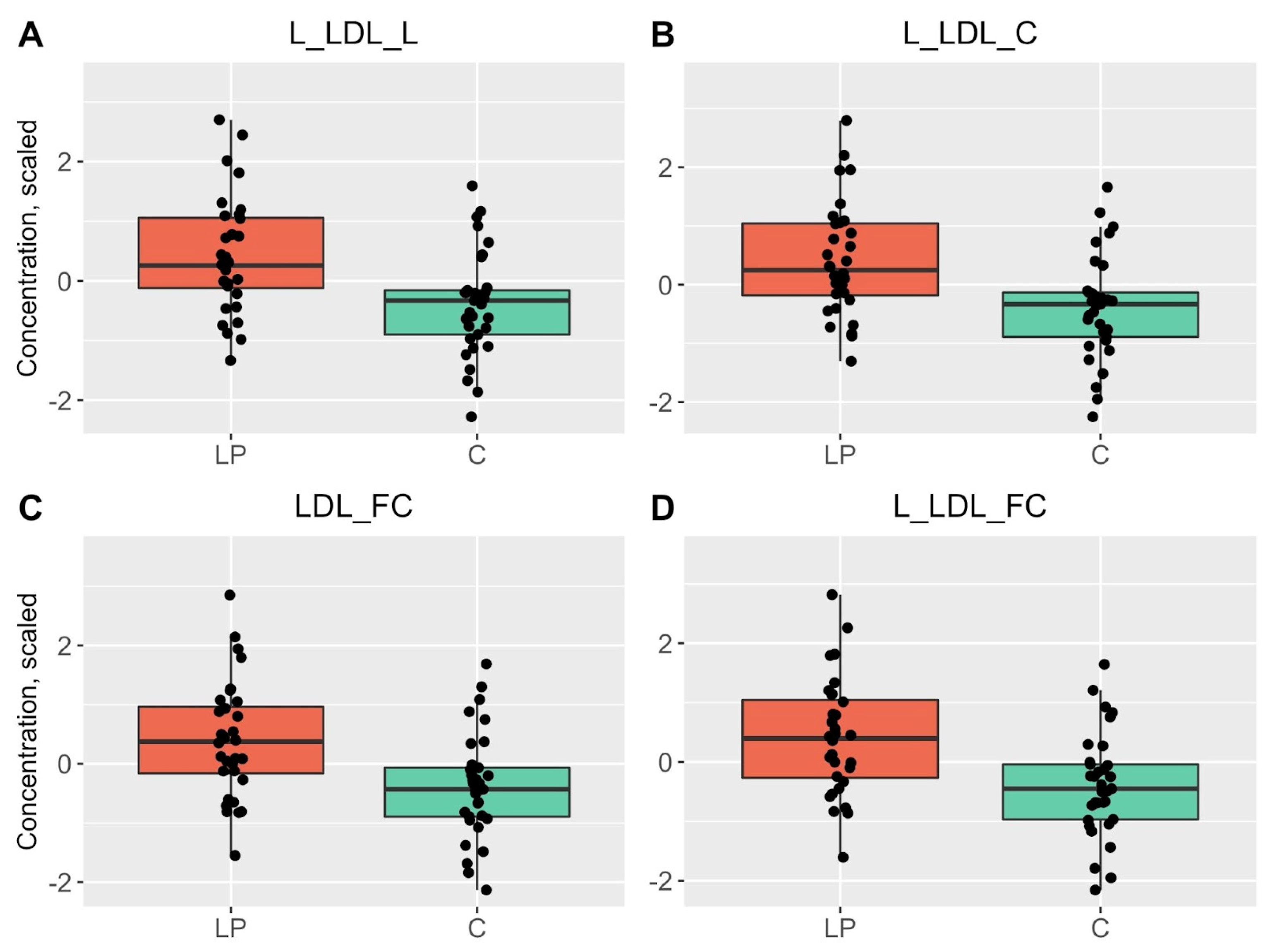
| L-LDL-L | 0.4 | −0.39 | 0.0007 |
| L-LDL-C | 0.41 | −0.4 | 0.0008 |
| L-LDL-FC | 0.41 | −0.39 | 0.0008 |
| L-LDL-CE | 0.4 | −0.39 | 0.001 |
| L-LDL-PL | 0.4 | −0.38 | 0.0011 |
| LDL | |||
| LDL-FC | 0.39 | −0.38 | 0.0008 |
| LDL-C | 0.38 | −0.37 | 0.0024 |
| LDL-L | 0.38 | −0.37 | 0.0027 |
| IDL | |||
| IDL-PL | 0.4 | −0.39 | 0.0013 |
| IDL-CE | 0.4 | −0.39 | 0.0021 |
| IDL-C | 0.4 | −0.39 | 0.0023 |
| IDL-FC | 0.39 | −0.38 | 0.0027 |
| Clinical LDL cholesterol and its values | |||
| Clinical LDL-C * | 0.39 | −0.38 | 0.0014 |
| Total C | 0.41 | −0.4 | 0.0016 |
| Cholesteryl esters | |||
| Total CE | 0.41 | −0.39 | 0.0013 |
| Free cholesterol | |||
| Total FC | 0.4 | −0.39 | 0.0028 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilves, L.; Ottas, A.; Raam, L.; Zilmer, M.; Traks, T.; Jaks, V.; Kingo, K. Changes in Lipoprotein Particles in the Blood Serum of Patients with Lichen Planus. Metabolites 2023, 13, 91. https://doi.org/10.3390/metabo13010091
Ilves L, Ottas A, Raam L, Zilmer M, Traks T, Jaks V, Kingo K. Changes in Lipoprotein Particles in the Blood Serum of Patients with Lichen Planus. Metabolites. 2023; 13(1):91. https://doi.org/10.3390/metabo13010091
Chicago/Turabian StyleIlves, Liis, Aigar Ottas, Liisi Raam, Mihkel Zilmer, Tanel Traks, Viljar Jaks, and Külli Kingo. 2023. "Changes in Lipoprotein Particles in the Blood Serum of Patients with Lichen Planus" Metabolites 13, no. 1: 91. https://doi.org/10.3390/metabo13010091
APA StyleIlves, L., Ottas, A., Raam, L., Zilmer, M., Traks, T., Jaks, V., & Kingo, K. (2023). Changes in Lipoprotein Particles in the Blood Serum of Patients with Lichen Planus. Metabolites, 13(1), 91. https://doi.org/10.3390/metabo13010091