
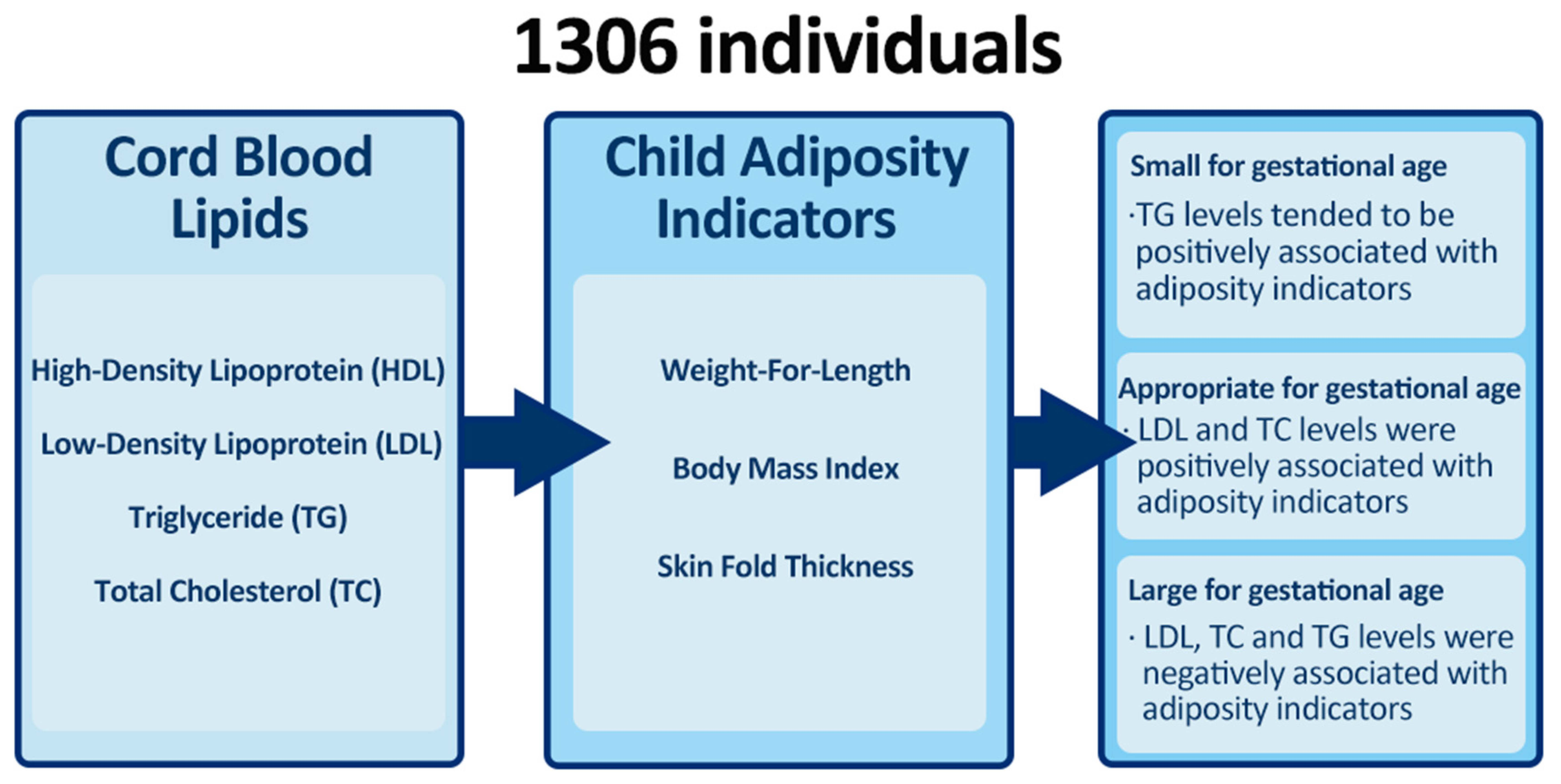
Associations of Cord Blood Lipids with Childhood Adiposity at the Age of Three Years: A Prospective Birth Cohort Study

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Results
2.1. Associations of Cord Blood Lipids and Childhood Adiposity Indicators
2.2. Stratified Associations by Birth Weight Categories
2.3. Other Stratified Analysis and Sensitivity Analyses
3. Discussion
3.1. Main Findings
3.2. Interpretation of the Results
3.3. Implications
3.4. Strengths and Limitations
4. Materials and Methods
4.1. Study Population
4.2. Child Adiposity Indicators
4.3. Cord Blood Lipids Measurements
4.4. Covariates
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. New Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Reinehr, T. Long-term effects of adolescent obesity: Time to act. Nat. Rev. Endocrinol. 2018, 14, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Han, J.C.; Lawlor, D.A.; Kimm, S.Y.S. Childhood obesity. Lancet 2010, 375, 1737–1748. [Google Scholar] [CrossRef]
- Orsso, C.E.; Colin-Ramirez, E.; Field, C.J.; Madsen, K.L.; Prado, C.M.; Haqq, A.M. Adipose Tissue Development and Expansion from the Womb to Adolescence: An Overview. Nutrients 2020, 12, 2735. [Google Scholar] [CrossRef]
- Retnakaran, R.; Ye, C.; Hanley, A.J.; Connelly, P.W.; Sermer, M.; Zinman, B.; Hamilton, J.K. Treating Gestational Diabetes Reduces Birth Weight but Does Not Affect Infant Adiposity Across the 1st Year of Life. Diabetes Care 2022, 45, 1230–1238. [Google Scholar] [CrossRef]
- Landon, M.B.; Rice, M.M.; Varner, M.W.; Casey, B.M.; Reddy, U.M.; Wapner, R.J.; Rouse, D.J.; Biggio, J.R.; Thorp, J.M.; Chien, E.K.; et al. Mild gestational diabetes mellitus and long-term child health. Diabetes Care 2015, 38, 445–452. [Google Scholar] [CrossRef]
- Barbour, L.A.; Hernandez, T.L. Maternal Lipids and Fetal Overgrowth: Making Fat from Fat. Clin. Ther. 2018, 40, 1638–1647. [Google Scholar] [CrossRef]
- Daraki, V.; Georgiou, V.; Papavasiliou, S.; Chalkiadaki, G.; Karahaliou, M.; Koinaki, S.; Sarri, K.; Vassilaki, M.; Kogevinas, M.; Chatzi, L. Metabolic profile in early pregnancy is associated with offspring adiposity at 4 years of age: The Rhea pregnancy cohort Crete, Greece. PLoS ONE 2015, 10, e0126327. [Google Scholar] [CrossRef]
- Gademan, M.G.J.; Vermeulen, M.; Oostvogels, A.J.J.M.; Roseboom, T.J.; Visscher, T.L.S.; van Eijsden, M.; Twickler, M.T.B.; Vrijkotte, T.G.M. Maternal prepregancy BMI and lipid profile during early pregnancy are independently associated with offspring’s body composition at age 5–6 years: The ABCD study. PLoS ONE 2014, 9, e94594. [Google Scholar] [CrossRef]
- Thaware, P.K.; McKenna, S.; Patterson, C.C.; Casey, C.; McCance, D.R. Maternal Lipids at 28 Weeks’ Gestation and Offspring Adiposity at Age 5 to 7 Years. J. Clin. Endocrinol. Metab. 2018, 103, 3767–3772. [Google Scholar] [CrossRef]
- Geraghty, A.A.; Alberdi, G.; O’Sullivan, E.J.; O’Brien, E.C.; Crosbie, B.; Twomey, P.J.; McAuliffe, F.M. Maternal Blood Lipid Profile during Pregnancy and Associations with Child Adiposity: Findings from the ROLO Study. PLoS ONE 2016, 11, e0161206. [Google Scholar] [CrossRef] [PubMed]
- Meyer, D.M.; Brei, C.; Stecher, L.; Brunner, S.; Hauner, H. Maternal insulin resistance, triglycerides and cord blood insulin are not determinants of offspring growth and adiposity up to 5 years: A follow-up study. Diabet. Med. A J. Br. Diabet. Assoc. 2018, 35, 1399–1403. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Shen, S.; Price, M.J.; Lu, J.; Sumilo, D.; Kuang, Y.; Manolopoulos, K.; Xia, H.; Qiu, X.; Cheng, K.K.; et al. Glucose, Insulin, and Lipids in Cord Blood of Neonates and Their Association with Birthweight: Differential Metabolic Risk of Large for Gestational Age and Small for Gestational Age Babies. J. Pediatr. 2020, 220, 64–72. [Google Scholar] [CrossRef]
- Donahue, S.M.A.; Rifas-Shiman, S.L.; Gold, D.R.; Jouni, Z.E.; Gillman, M.W.; Oken, E. Prenatal fatty acid status and child adiposity at age 3 y: Results from a US pregnancy cohort. Am. J. Clin. Nutr. 2011, 93, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, M.C.; Jackman, M.R.; Presby, D.M.; Houck, J.A.; Webb, P.G.; Johnson, G.C.; Soderborg, T.K.; de la Houssaye, B.A.; Yang, I.V.; Friedman, J.E.; et al. Low Neonatal Plasma n-6/n-3 PUFA Ratios Regulate Offspring Adipogenic Potential and Condition Adult Obesity Resistance. Diabetes 2018, 67, 651–661. [Google Scholar] [CrossRef]
- Much, D.; Brunner, S.; Vollhardt, C.; Schmid, D.; Sedlmeier, E.M.; Brüderl, M.; Heimberg, E.; Bartke, N.; Boehm, G.; Bader, B.L.; et al. Effect of dietary intervention to reduce the n-6/n-3 fatty acid ratio on maternal and fetal fatty acid profile and its relation to offspring growth and body composition at 1 year of age. Eur. J. Clin. Nutr. 2013, 67, 282–288. [Google Scholar] [CrossRef]
- Bernard, J.Y.; Tint, M.-T.; Aris, I.M.; Chen, L.-W.; Quah, P.L.; Tan, K.H.; Yeo, G.S.-H.; Fortier, M.V.; Yap, F.; Shek, L.; et al. Maternal plasma phosphatidylcholine polyunsaturated fatty acids during pregnancy and offspring growth and adiposity. Prostaglandins Leukot. Essent. Fat. Acids 2017, 121, 21–29. [Google Scholar] [CrossRef]
- McConihay, J.A.; Honkomp, A.M.; Granholm, N.A.; Woollett, L.A. Maternal high density lipoproteins affect fetal mass and extra-embryonic fetal tissue sterol metabolism in the mouse. J. Lipid. Res. 2000, 41, 424–432. [Google Scholar] [CrossRef]
- Kadakia, R.; Talbot, O.; Kuang, A.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Ilkayeva, O.R.; Lowe, L.P.; Metzger, B.E.; Newgard, C.B.; et al. Cord Blood Metabolomics: Association With Newborn Anthropometrics and C-Peptide Across Ancestries. J. Clin. Endocrinol. Metab. 2019, 104, 4459–4472. [Google Scholar] [CrossRef]
- Cao, T.; Zhao, J.; Hong, X.; Wang, G.; Hu, F.B.; Wang, X.; Liang, L. Cord Blood Metabolome and BMI Trajectory from Birth to Adolescence: A Prospective Birth Cohort Study on Early Life Biomarkers of Persistent Obesity. Metabolites 2021, 11, 739. [Google Scholar] [CrossRef]
- Katragadda, T.; Mahabala, R.S.; Shetty, S.; Baliga, S. Comparison of Cord Blood Lipid Profile in Preterm Small for Gestational Age and Appropriate for Gestational Age Newborns. J. Clin. Diagn. Res. 2017, 11, SC05–SC07. [Google Scholar] [CrossRef] [PubMed]
- Lobo, L.L.; Kumar, H.U.; Mishra, T.; Sundari, T.; Singh, A.; Kumar, C.V.; Rao, G.K.; Jahangir, B.; Misale, V.; Prashant, P.; et al. Small-for-gestational-age versus appropriate-for-gestational-age: Comparison of cord blood lipid profile & insulin levels in term newborns (SAGA-ACT study). Indian J. Med. Res. 2016, 144, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A. The IUGR newborn. Semin. Perinatol. 2008, 32, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Hay, W.W. Placental-fetal glucose exchange and fetal glucose metabolism. Trans. Am. Clin. Clim. Assoc. 2006, 117, 321–340. [Google Scholar]
- Magnusson, A.L.; Waterman, I.J.; Wennergren, M.; Jansson, T.; Powell, T.L. Triglyceride hydrolase activities and expression of fatty acid binding proteins in the human placenta in pregnancies complicated by intrauterine growth restriction and diabetes. J. Clin. Endocrinol. Metab. 2004, 89, 4607–4614. [Google Scholar] [CrossRef]
- Olivecrona, T.; Bergö, M.; Hultin, M.; Olivecrona, G. Nutritional regulation of lipoprotein lipase. Can. J. Cardiol. 1995, 11 (Suppl. G), 73G–78G. [Google Scholar]
- Meas, T. Fetal origins of insulin resistance and the metabolic syndrome: A key role for adipose tissue? Diabetes Metab. 2010, 36, 11–20. [Google Scholar] [CrossRef]
- Barker, D.J.P. The developmental origins of adult disease. J. Am. Coll. Nutr. 2004, 23, 588S–595S. [Google Scholar] [CrossRef]
- McDonald, E.C.; Pollitt, E.; Mueller, W.; Hsueh, A.M.; Sherwin, R. The Bacon Chow study: Maternal nutrition supplementation and birth weight of offspring. Am. J. Clin. Nutr. 1981, 34, 2133–2144. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, G.; Zhang, H.; Karin, M.; Bai, H.; Cai, D. Hypothalamic IKKbeta/NF-kappaB and ER stress link overnutrition to energy imbalance and obesity. Cell 2008, 135, 61–73. [Google Scholar] [CrossRef]
- Cai, D. Neuroinflammation and neurodegeneration in overnutrition-induced diseases. Trends Endocrinol. Metab. 2013, 24, 40–47. [Google Scholar] [CrossRef]
- Kass, I.J.; Sampson, N.S. The importance of GLU361 position in the reaction catalyzed by cholesterol oxidase. Bioorg. Med. Chem. Lett. 1998, 8, 2663–2668. [Google Scholar] [CrossRef]
- Nagao, K.; Inoue, N.; Suzuki, K.; Shimizu, T.; Yanagita, T. The Cholesterol Metabolite Cholest-5-en-3-One Alleviates Hyperglycemia and Hyperinsulinemia in Obese (/) Mice. Metabolites 2021, 12, 26. [Google Scholar] [CrossRef]
- Qiu, X.; Lu, J.-H.; He, J.-R.; Lam, K.-B.H.; Shen, S.-Y.; Guo, Y.; Kuang, Y.-S.; Yuan, M.-Y.; Qiu, L.; Chen, N.-N.; et al. The Born in Guangzhou Cohort Study (BIGCS). Eur. J. Epidemiol. 2017, 32, 337–346. [Google Scholar] [CrossRef]
- Huang, J.-S.; Chen, Q.-Z.; Zheng, S.-Y.; Ramakrishnan, R.; Zeng, J.-Y.; Zhuo, C.-P.; Lai, Y.-M.; Kuang, Y.-S.; Lu, J.-H.; He, J.-R.; et al. Associations of Longitudinal Fetal Growth Patterns With Cardiometabolic Factors at Birth. Front. Endocrinol. 2021, 12, 771193. [Google Scholar] [CrossRef]
- Li, H.; Ji, C.-y.; Zong, X.-n.; Zhang, Y.-q. Height and weight standardized growth charts for Chinese children and adolescents aged 0 to 18 year. Chin. J. Pediatr. 2009, 47, 487–492. [Google Scholar] [CrossRef]
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Berger, H.; Gagnon, R.; Sermer, M. Guideline No. 393-Diabetes in Pregnancy. J. Obs. Gynaecol. Can. 2019, 41, 1814–1825. [Google Scholar] [CrossRef]
- Zhu, W.-W.; Yang, H.-X. Diagnosis of gestational diabetes mellitus in China. Diabetes Care 2013, 36, e76. [Google Scholar] [CrossRef]

{kind=link}
| Variables | All N = 1306 | Boys N = 699 | Girls N = 607 |
|---|---|---|---|
| Maternal characteristics | |||
| Age mean (SD), years | 29.8 (3.4) | 29.9 (3.5) | 29.7 (3.2) |
| Educational level (%) | |||
| Middle school or below | 77 (5.9) | 38 (5.4) | 39 (6.4) |
| College | 252 (19.3) | 141 (20.2) | 111 (18.3) |
| Undergraduate | 773 (59.2) | 417 (59.7) | 356 (58.6) |
| Postgraduate | 204 (15.6) | 103 (14.7) | 101 (16.6) |
| Pre-pregnancy BMI | |||
| Mean (SD), kg/m2 | 20.5 (2.7) | 20.5 (2.7) | 20.6 (2.7) |
| Underweight (%) | 310 (23.7) | 172 (24.6) | 138 (22.7) |
| Normal weight (%) | 853 (65.3) | 450 (64.4) | 403 (66.4) |
| Overweight/obesity (%) | 143 (10.9) | 77 (11.0) | 66 (10.9) |
| Nulliparous (%) | 1003 (76.8) | 532 (76.1) | 471 (77.6) |
| GDM (%) | 163 (12.5) | 81 (11.6) | 82 (13.5) |
| Pregnancy-induced hypertension (%) | 48 (3.7) | 25 (3.6) | 23 (3.8) |
| Child’s characteristics | |||
| Gestational age | |||
| Median (25th–75th), weeks | 39.0 (38.0, 40.0) | 39.0 (38.0, 40.0) | 39.0 (38.0, 40.0) |
| Preterm (%) | 58 (4.4) | 38 (5.4) | 20 (3.3) |
| Term (%) | 1248 (95.6) | 661 (94.6) | 587 (96.7) |
| Birth weight | |||
| SGA (%) | 85 (6.5%) | 40 (5.7%) | 45 (7.4%) |
| AGA (%) | 1135 (86.9%) | 617 (88.3%) | 518 (85.3%) |
| LGA (%) | 86 (6.6%) | 42 (6.0%) | 44 (7.2%) |
| Child growth measurements | |||
| Age at measurement | |||
| Mean (SD), months | 34.7 (3.2) | 34.7 (3.1) | 34.7 (3.3) |
| Length mean (SD), cm | 94.9 (7.5) | 95.6 (7.0) | 94.1 (8.0) |
| Weight mean (SD), kg | 13.9 (2.8) | 14.1 (2.1) | 13.7 (3.3) |
| BMI mean (SD), kg/m2 | 15.2 (1.23) | 15.3 (1.21) | 15,1 (1.23) |
| SST mean (SD), mm | 6.8 (1.9) | 6.7 (2.0) | 7.0 (1.8) |
| TST mean (SD), mm | 10.1 (2.3) | 10.1 (2.3) | 10.1 (2.2) |
| Lipids level in cord blood, median (25th–75th) | |||
| Total cholesterol, mmol/L | 1.68 (1.44–1.96) | 1.61 (1.36–1.92) | 1.73 (1.51–2.00) |
| Triglycerides, mmol/L | 0.33 (0.27–0.41) | 0.33 (0.27–0.41) | 0.33 (0.27–0.41) |
| HDL, mmol/L | 0.87 (0.72–1.05) | 0.83 (0.70–1.02) | 0.92 (0.74–1.10) |
| LDL, mmol/L | 0.58 (0.45–0.73) | 0.56 (0.42–0.71) | 0.60 (0.47–0.75) |
| Cord Blood Metabolic Factors | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Beta (95% CI) | p | Beta (95% CI) | p | |
| Total cholesterol | ||||
| Weight-for-length z-score | 0.03 (−0.02, 0.09) | 0.23 | 0.02 (−0.04, 0.07) | 0.56 |
| BMI-for-age z-score | 0.03 (−0.02, 0.09) | 0.27 | 0.02 (−0.04, 0.07) | 0.59 |
| TST-for-age z-score | 0.06 (−0.02, 0.14) | 0.15 | 0.06 (−0.03, 0.14) | 0.18 |
| SST-for-age z-score | 0.09 (−0.02, 0.19) | 0.12 | 0.07 (−0.03, 0.18) | 0.18 |
| SSFT-for-age z-score | 0.10 (−0.04, 0.24) | 0.16 | 0.09 (−0.05, 0.23) | 0.21 |
| Triglycerides | ||||
| Weight-for-length z-score | −0.08 (−0.13, −0.02) | <0.01 | 0.00 (−0.05, 0.06) | 0.94 |
| BMI-for-age z-score | −0.07 (−0.13, −0.02) | 0.01 | 0.00 (−0.06, 0.06) | 0.96 |
| TST-for-age z-score | −0.04 (−0.12, 0.04) | 0.29 | −0.03 (−0.11, 0.05) | 0.46 |
| SST-for-age z-score | −0.08 (−0.18, 0.03) | 0.15 | −0.04 (−0.15, 0.07) | 0.49 |
| SSFT-for-age z-score | −0.13 (−0.27, 0.00) | 0.06 | −0.10 (−0.24, 0.04) | 0.17 |
| HDL | ||||
| Weight-for-length z-score | 0.06 (0.01, 0.12) | 0.03 | 0.03 (−0.03, 0.08) | 0.30 |
| BMI-for-age z-score | 0.06 (0.00, 0.11) | 0.05 | 0.03 (−0.03, 0.08) | 0.32 |
| TST-for-age z-score | 0.10 (0.02, 0.18) | 0.01 | 0.10 (0.02, 0.18) | 0.02 |
| SST-for-age z-score | 0.08 (−0.03, 0.19) | 0.14 | 0.06 (−0.04, 0.17) | 0.23 |
| SSFT-for-age z-score | 0.15 (0.01, 0.29) | 0.04 | 0.13 (−0.01, 0.27) | 0.06 |
| LDL | ||||
| Weight-for-length z-score | 0.03 (−0.03, 0.08) | 0.33 | 0.02 (−0.04, 0.07) | 0.54 |
| BMI-for-age z-score | 0.03 (−0.03, 0.08) | 0.35 | 0.02 (−0.04, 0.07) | 0.55 |
| TST-for-age z-score | 0.00 (−0.08, 0.08) | 0.95 | −0.01 (−0.09, 0.08) | 0.90 |
| SST-for-age z-score | 0.08 (−0.03, 0.19) | 0.14 | 0.07 (−0.04, 0.18) | 0.20 |
| SSFT-for-age z-score | −0.02 (−0.16, 0.12) | 0.73 | −0.03 (−0.17, 0.11) | 0.64 |
| Cord Blood Lipids | Regression Coefficients (95% Confidence Interval) | pinteraction | ||||
|---|---|---|---|---|---|---|
| SGA (N = 85) | AGA (N = 1135) | LGA (N = 86) | SGA vs. AGA | LGA vs. AGA | SGA vs. LGA | |
| Total cholesterol | ||||||
| Weight-for-length z-score | 0.07 (−0.12, 0.25) | 0.06 (0.01, 0.12) | −0.15 (−0.35, 0.04) | 0.55 | 0.01 | 0.16 |
| BMI-for-age z-score | 0.08 (−0.11, 0.26) | 0.06 (0.00, 0.12) | −0.17 (−0.36, 0.03) | 0.61 | <0.01 | 0.12 |
| TST-for-age z-score | −0.01 (−0.34, 0.32) | 0.09 (−0.01, 0.18) | −0.08 (−0.47, 0.32) | 0.15 | 0.24 | 0.86 |
| SST-for-age z-score | 0.02 (−0.41, 0.45) | 0.13 (0.01, 0.25) | −0.39 (−0.78, 0.00) | 0.17 | 0.04 | 0.55 |
| SSFT-for-age z-score | −0.02 (−0.36, 0.32) | 0.11 (−0.02, 0.23) | 0.09 (−1.78, 1.96) | 0.75 | 0.18 | 0.16 |
| Triglycerides | ||||||
| Weight-for-length z-score | 0.12 (−0.06, 0.31) | −0.04 (−0.10, 0.02) | −0.25 (−0.46, −0.05) | 0.09 | 0.08 | 0.01 |
| BMI-for-age z-score | 0.12 (−0.07, 0.30) | −0.04 (−0.10, 0.03) | −0.25 (−0.46, −0.04) | 0.11 | 0.09 | 0.02 |
| TST-for-age z-score | 0.01 (−0.28, 0.30) | −0.03 (−0.12, 0.06) | −0.31 (−0.61, 0.00) | 0.75 | 0.23 | 0.28 |
| SST-for-age z-score | 0.06 (−0.34, 0.46) | −0.09 (−0.21, 0.03) | −0.08 (−0.43, 0.26) | 0.18 | 0.66 | 0.46 |
| SSFT-for-age z-score | 0.05 (−0.35, 0.24) | −0.04 (−0.16, 0.09) | −1.01 (−2.43, 0.41) | 0.78 | 0.47 | 0.42 |
| HDL | ||||||
| Weight-for-length z-score | 0.09 (−0.08, 0.27) | 0.07 (0.01, 0.13) | −0.11 (−0.34, 0.11) | 0.92 | 0.07 | 0.19 |
| BMI-for-age z-score | 0.09 (−0.09, 0.26) | 0.06 (0.00, 0.12) | −0.12 (−0.35, 0.11) | 0.89 | 0.07 | 0.19 |
| TST-for-age z-score | −0.04 (−0.31, 0.22) | 0.11 (0.02, 0.20) | 0.22 (−0.17, 0.61) | 0.23 | 0.76 | 0.29 |
| SST-for-age z-score | −0.04 (−0.39, 0.30) | 0.11 (−0.01, 0.23) | −0.18 (−0.64, 0.29) | 0.17 | 0.13 | 0.75 |
| SSFT-for-age z-score | −0.04 (−0.31, 0.23) | 0.09 (−0.04, 0.22) | 1.15 (−0.79, 3.10) | 0.29 | 0.47 | 0.19 |
| LDL | ||||||
| Weight-for-length z-score | 0.02 (−0.18, 0.21) | 0.06 (0.00, 0.13) | −0.16 (−0.34, 0.02) | 0.23 | <0.01 | 0.28 |
| BMI-for-age z-score | 0.04 (−0.16, 0.23) | 0.06 (0.00, 0.13) | −0.18 (−0.36, 0.01) | 0.31 | <0.01 | 0.19 |
| TST-for-age z-score | 0.07 (−0.27, 0.41) | 0.04 (−0.06, 0.13) | −0.30 (−0.62, 0.03) | 0.27 | 0.04 | 0.48 |
| SST-for-age z-score | 0.14 (−0.29, 0.58) | 0.13 (0.01, 0.25) | −0.48 (−0.79, −0.17) | 0.33 | 0.02 | 0.26 |
| SSFT-for-age z-score | 0.07 (−0.27, 0.42) | 0.11 (−0.02, 0.23) | −1.43 (−2.86, −0.01) | 0.54 | 0.10 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, Q.-Q.; Kong, S.-M.; Yin, X.; Gao, C.; Lu, M.-S.; Ramakrishnan, R.; Guo, C.; Yao, W.; Zeng, J.-Y.; Kuang, Y.-S.; et al. Associations of Cord Blood Lipids with Childhood Adiposity at the Age of Three Years: A Prospective Birth Cohort Study. Metabolites 2022, 12, 522. https://doi.org/10.3390/metabo12060522
Ye Q-Q, Kong S-M, Yin X, Gao C, Lu M-S, Ramakrishnan R, Guo C, Yao W, Zeng J-Y, Kuang Y-S, et al. Associations of Cord Blood Lipids with Childhood Adiposity at the Age of Three Years: A Prospective Birth Cohort Study. Metabolites. 2022; 12(6):522. https://doi.org/10.3390/metabo12060522
Chicago/Turabian StyleYe, Qi-Qing, Shao-Min Kong, Xin Yin, Chang Gao, Min-Shan Lu, Rema Ramakrishnan, Cheng Guo, Wang Yao, Ji-Yuan Zeng, Ya-Shu Kuang, and et al. 2022. "Associations of Cord Blood Lipids with Childhood Adiposity at the Age of Three Years: A Prospective Birth Cohort Study" Metabolites 12, no. 6: 522. https://doi.org/10.3390/metabo12060522
APA StyleYe, Q.-Q., Kong, S.-M., Yin, X., Gao, C., Lu, M.-S., Ramakrishnan, R., Guo, C., Yao, W., Zeng, J.-Y., Kuang, Y.-S., Lu, J.-H., He, J.-R., & Qiu, X. (2022). Associations of Cord Blood Lipids with Childhood Adiposity at the Age of Three Years: A Prospective Birth Cohort Study. Metabolites, 12(6), 522. https://doi.org/10.3390/metabo12060522