
ProBDNF as an Indicator of Improvement among Women with Depressive Episodes


Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Studied Group
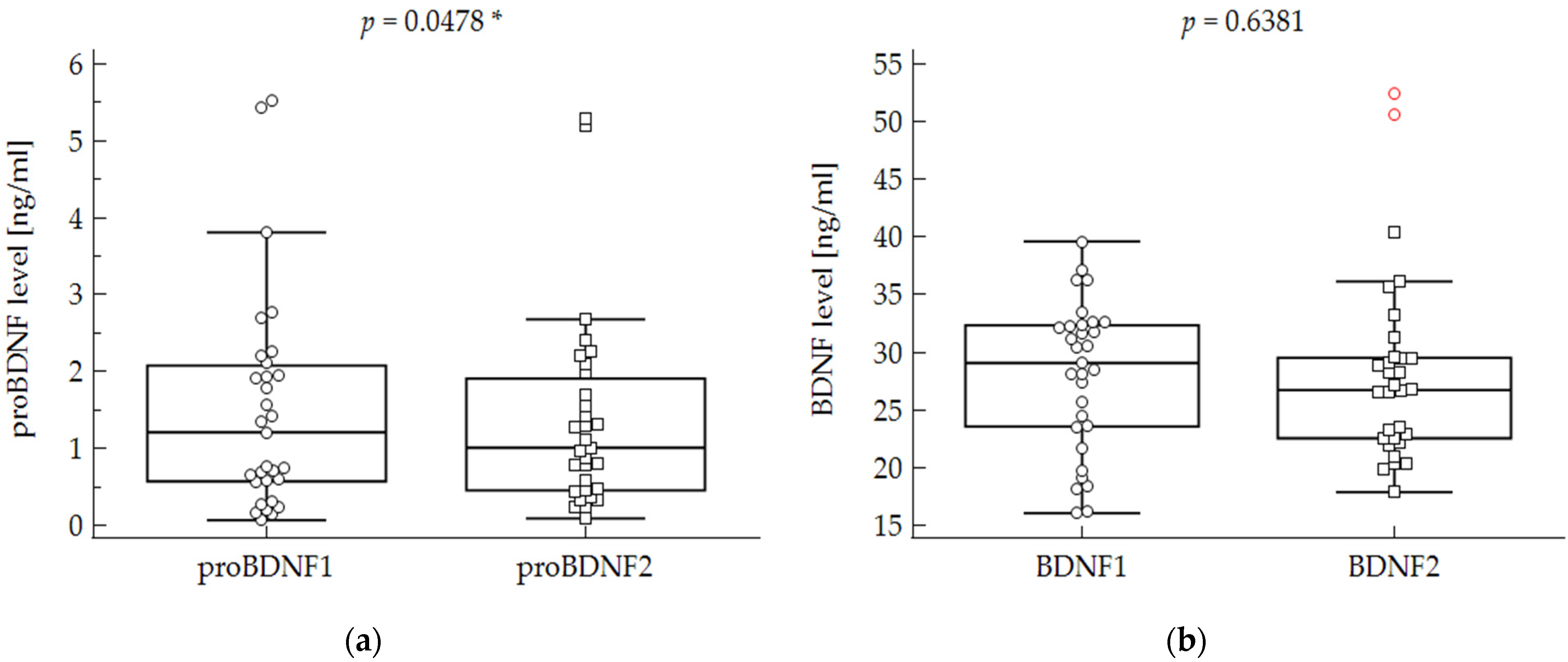
2.2. Biochemical Parameters
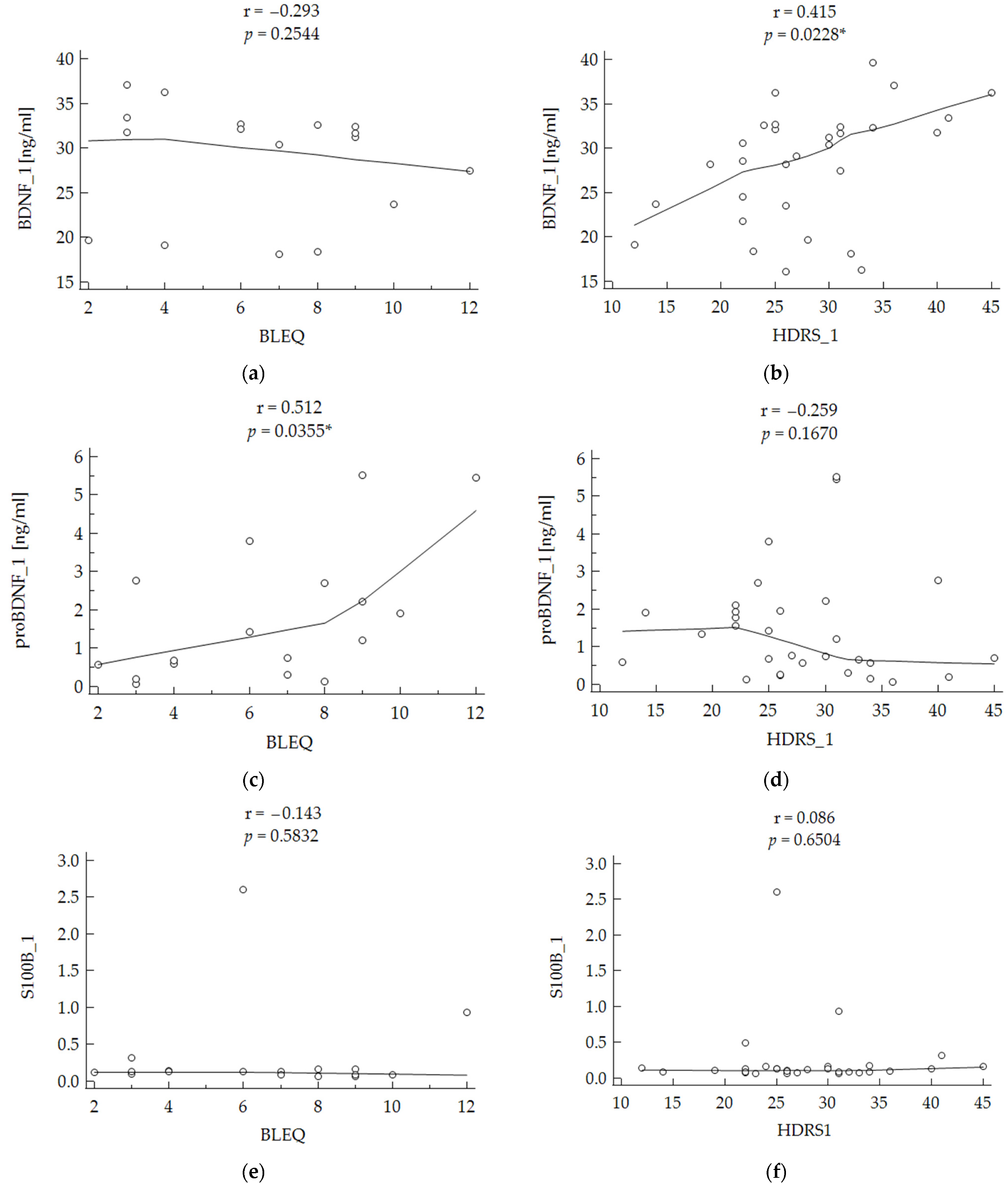
2.3. Correlation with Stress and Depressive Symptoms
3. Discussion
4. Materials and Methods
4.1. Population
4.2. Biochemical Analysis
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Datta, S.; Suryadevara, U.; Cheong, J. Mood Disorders. Continuum 2021, 27, 1712–1737. [Google Scholar] [CrossRef] [PubMed]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.; Nie, Z.; Shu, H.; Kuang, Y.; Chen, X.; Cheng, J.; Yu, S.; Liu, H. The Role of BDNF on Neural Plasticity in Depression. Front. Cell. Neurosci. 2020, 14, 82. [Google Scholar] [CrossRef]
- Molendijk, M.L.; Bus, B.A.; Spinhoven, P.; Penninx, B.W.; Kenis, G.; Prickaerts, J.; Voshaar, R.C.O.; Elzinga, B.M. Serum levels of brain-derived neurotrophic factor in major depressive disorder: State-trait issues, clinical features and pharmacological treatment. Mol. Psychiatry 2011, 16, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Polyakova, M.; Stuke, K.; Schuemberg, K.; Mueller, K.; Schoenknecht, P.; Schroeter, M.L. BDNF as a biomarker for successful treatment of mood disorders: A systematic & quantitative meta-analysis. J. Affect. Disord. 2015, 174, 432–440. [Google Scholar] [CrossRef]
- Fernandes, B.S.; Molendijk, M.L.; Kohler, C.A.; Soares, J.C.; Leite, C.M.G.S.; Machado-Vieira, R.; Ribeiro, T.L.; Silva, J.C.; Sales, P.M.G.; Quevedo, J.; et al. Peripheral brain-derived neurotrophic factor (BDNF) as a biomarker in bipolar disorder: A meta-analysis of 52 studies. BMC Med. 2015, 13, 289. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Xiong, J.; Lim, Y.; Ruan, Y.; Huang, C.; Zhu, Y.; Zhou, X.F. Upregulation of blood proBDNF and its receptors in major depression. J. Affect. Disord. 2013, 150, 776–784. [Google Scholar] [CrossRef]
- Yang, C.R.; Zhang, X.Y.; Liu, Y.; Du, J.Y.; Liang, R.; Yu, M.; Zhang, F.Q.; Mu, X.F.; Li, F.; Zhou, L.; et al. Antidepressant Drugs Correct the Imbalance Between proB-DNF/p75NTR/Sortilin and Mature BDNF/TrkB in the Brain of Mice with Chronic Stress. Neurotox Res. 2020, 37, 171–182. [Google Scholar] [CrossRef]
- Gelle, T.; Samey, R.A.; Plansont, B.; Bessette, B.; Jauberteau-Marchan, M.-O.; Lalloué, F.; Girard, M. BDNF and pro-BDNF in serum and exosomes in major depression: Evolution after antidepressant treatment. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2020, 109, 110229. [Google Scholar] [CrossRef]
- Donato, R.; R cannon, B.; Sorci, G.; Riuzzi, F.; Hsu, K.; J Weber, D.; Geczy, C. Functions of S100 Proteins. Curr. Mol. Med. 2012, 13, 24–57. [Google Scholar] [CrossRef]
- Rajkowska, G. Postmortem studies in mood disorders indicate altered numbers of neurons and glial cells. Biol. Psychiatry 2000, 48, 766–777. [Google Scholar] [CrossRef]
- Schroeter, M.L.; Sacher, J.; Steiner, J.; Schoenknecht, P.; Mueller, K. Serum S100B Represents a New Biomarker for Mood Disorders. Curr. Drug Targets 2013, 14, 1237–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Rosa, M.I.; Simon, C.; Grande, A.J.; Barichello, T.; Oses, J.P.; Quevedo, J. Serum S100B in manic bipolar disorder patients: Systematic review and meta-analysis. J. Affect Disord. 2016, 206, 210–215. [Google Scholar] [CrossRef]
- Bartoli, F.; Misiak, B.; Crocamo, C.; Carrà, G. Glial and neuronal markers in bipolar disorder: A meta-analysis testing S100B and NSE peripheral blood levels. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2020, 101, 109922. [Google Scholar] [CrossRef]
- Andreazza, A.C.; Cassini, C.; Rosa, A.; Leite, M.C.; de Almeida, L.M.; Nardin, P.; Cunha, A.B.; Ceresér, K.M.; Santin, A.; Gottfried, C.; et al. Serum S100B and antioxidant enzymes in bipolar patients. J. Psychiatr. Res. 2007, 41, 523–529. [Google Scholar] [CrossRef]
- Ambrée, O.; Bergink, V.; Grosse, L.; Alferink, J.; Drexhage, H.A.; Rothermundt, M.; Arolt, V.; Birkenhäger, T.K. S100B Serum Levels Predict Treatment Response in Patients with Melancholic Depression. Int. J. Neuropsychopharmacol. 2016, 19, pyv103. [Google Scholar] [CrossRef] [Green Version]
- Jang, B.-S.; Kim, H.; Lim, S.-W.; Jang, K.-W.; Kimv, D.-K. Serum S100B Levels and Major Depressive Disorder: Its Characteristics and Role in Antidepressant Response. Psychiatry Investig. 2008, 5, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Rong, H.; Wang, G.; Liu, T.; Wang, H.; Wan, Q.; Weng, S. Chronic mild stress induces fluoxetine-reversible decreases in hippo-campal and cerebrospinal fluid levels of the neurotrophic factor S100B and its specific receptor. Int. J. Mol. Sci. 2010, 11, 5310–5322. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.-C.; Huang, T.-L. Decreased S100B serum levels after treatment in bipolar patients in a manic phase. Compr. Psychiatry 2017, 74, 27–34. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Lopes, M.; Fregni, F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: Implications for the role of neuroplasticity in depression. Int. J. Neuropsychopharmacol. 2008, 11, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Södersten, K.; Pålsson, E.; Ishima, T.; Funa, K.; Landén, M.; Hashimoto, K.; Ågren, H. Abnormality in serum levels of mature brain-derived neurotrophic factor (BDNF) and its precursor proBDNF in mood-stabilized patients with bipolar disorder: A study of two independent cohorts. J. Affect. Disord. 2014, 160, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.O.; Perestrelo, T.M.M.; Almeida, R.D. PROneurotrophins and CONSequences. Mol. Neurobiol. 2018, 55, 2934–2951. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Chen, S.; Li, C.; Lu, N.; Yue, Y.; Yin, Y.; Zhang, Y.; Zhi, X.; Zhang, D.; Yuan, Y. The serum protein levels of the tPA–BDNF pathway are implicated in depression and antidepressant treatment. Transl. Psychiatry 2017, 7, e1079. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, R.; Kishi, T.; Hori, H.; Atake, K.; Katsuki, A.; Nakano-Umene, W.; Ikenouchi-Sugita, A.; Iwata, N.; Nakamura, J. Serum proBDNF/BDNF and response to fluvoxamine in drug-naïve first-episode major depressive disorder patients. Ann. Gen. Psychiatry 2014, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Diniz, C.R.A.F.; Casarotto, P.C.; Resstel, L.; Joca, S.R.L. Beyond good and evil: A putative continuum-sorting hypothesis for the functional role of proBDNF/BDNF-propeptide/mBDNF in antidepressant treatment. Neurosci. Biobehav. Rev. 2018, 90, 70–83. [Google Scholar] [CrossRef] [Green Version]
- Duman, R.S.; Heninger, G.R.; Nestler, E.J. A Molecular and Cellular Theory of Depression. Arch. Gen. Psychiatry 1997, 54, 597–606. [Google Scholar] [CrossRef]
- Lin, L.; Fu, X.-Y.; Zhou, X.-F.; Liu, D.; Bobrovskaya, L.; Zhou, L. Analysis of blood mature BDNF and proBDNF in mood disorders with specific ELISA assays. J. Psychiatr. Res. 2021, 133, 166–173. [Google Scholar] [CrossRef]
- Yoshida, T.; Ishikawa, M.; Niitsu, T.; Nakazato, M.; Watanabe, H.; Shiraishi, T.; Shiina, A.; Hashimoto, T.; Kanahara, N.; Hasegawa, T.; et al. Decreased Serum Levels of Mature Brain-Derived Neurotrophic Factor (BDNF), but Not Its Precursor proBDNF, in Patients with Major Depressive Disorder. PLoS ONE 2012, 7, e42676. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Su, Y.; Zhou, R.; Wang, F.; Xia, W.; Huang, J.; Hu, Y.; Cao, L.; Yuan, C.; Yi, Z.; et al. Ratio of mBDNF to proBDNF for Differential Diagnosis of Major Depressive Disorder and Bipolar Depression. Mol. Neurobiol. 2016, 54, 5573–5582. [Google Scholar] [CrossRef]
- Vega, P.; Barbeito, S.; de Azúa, S.R.; Martínez-Cengotitabengoa, M.; González–Ortega, I.; Saenz, M.; González-Pinto, A. Bipolar Disorder Differences between Genders: Special Considerations for Women. Women’s Health 2011, 7, 663–676. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J. Structured Clinical Interview for DSM IV Axis I Disorders, Clinician Version (SCID-CV); American Psychiatric Press, Inc.: Washington, DC, USA, 1996. [Google Scholar]
- McGuffin, P.; Farmer, A.; Harvey, I. A Polydiagnostic Application of Operational Criteria in Studies of Psychotic Illness. Development and reliability of the OPCRIT system. Arch. Gen. Psychiatry 1991, 48, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brugha, T.; Bebbington, P.; Tennant, C.; Hurry, J. The List of Threatening Experiences: A subset of 12 life event categories with considerable long-term contextual threat. Psychol. Med. 1985, 15, 189–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Bipolar Disorder (BD) | Major Depressive Disorder (MDD) | p-Value (BD vs. MDD) | |
|---|---|---|---|
| Number (n) | 16 | 15 | |
| Sex | females | females | |
| Age (years) | 34.44 ± 14.27 | 44.67 ± 17.36 | 0.0749 |
| BMI (kg/m2) | 22.78 ± 3.83 | 25.39 ± 5.10 | 0.1063 |
| Tobacco smokers (yes/no/no data) (n) | 4/10/2 | 5/10/0 | 0.7855 |
| Educational level (n) None or low | 2 | 3 | 0.8319 |
| Middle | 10 | 8 | |
| High | 4 | 4 | |
| Marital status (n) | 0.2828 | ||
| single | 9 | 5 | |
| married | 4 | 8 | |
| divorced | 2 | 1 | |
| widowed | 0 | 1 | |
| no data | 1 | 0 | |
| Somatic disease (yes/no) | 9/7 | 9/6 | 0.4719 |
| Family history of psychiatric illness (yes/no) | 12/4 | 10/5 | 0.6153 |
| History of hospitalizations (n) | 0.5710 | ||
| 1–4 | 12 | 14 | |
| 5–10 | 1 | 0 | |
| >10 | 1 | 1 | |
| Time to achieve remission (days) | 52 (±30) | 61 (±73) | 0.6783 |
| BDI (t1/t2) * | 31.5 (19–44)/6 (0–29) | 28 (13–53)/10.5 (3–26) | 0.2848/0.0506 |
| HDRS (t1/t2) * | 30 (12–45)/3 (0–6) | 26 (14–36)/3 (1–19) | 0.4541/0.3661 |
| BLEQ * | 7 (2–9) | 7 (3–12) | 0.3323 |
| proBDNF ** | 1.56 (±1.49) | 1.46 (±1.38) | 0.8744 |
| BDNF ** | 30.04 (±5.99) | 26.12 (±6.46) | 0.0913 |
| S100B ** | 0.33 (±0.66) | 0.15 (±0.11) | 0.9525 |
| Medication Status of the Studied Group | T1/T2 |
|---|---|
| none | 1/0 |
| AD | 6/4 |
| AP | 2/0 |
| AD + AP | 5/8 |
| AD + Li | 1/1 |
| AD + AC | 1/2 |
| AP + AC | 0/1 |
| AD + AP + Li | 1/4 |
| AD + AC + Li | 2/2 |
| AD + AP + AC | 1/6 |
| AD + AP + AC + Li | 0/1 |
| No data | 11/2 |
| Measure (ng/mL) | MDD | p-Value T1/T2 | BD | p-Value T1/T2 | Patients Overall | p-Value T1/T2 | |||
|---|---|---|---|---|---|---|---|---|---|
| T-1 | T-2 | T-1 | T-2 | T-1 | T-2 | ||||
| BDNF | 30.04 (±5.99) | 29.57 (±8.21) | 0.3303 | 26.12 (±6.46) | 26.94 (±8.09) | 0.7436 | 28.02 (±6.45) | 28.21 (±8.12) | 0.6381 |
| proBDNF | 1.56 (±1.49) | 1.39 (±1.26) | 0.1205 | 1.46 (±1.38) | 1.36 (±1.30) | 0.2522 | 1.51 (±1.41) | 1.37 (±1.26) | 0.0478 |
| S100B | 0.33 (±0.66) | 0.32 (±0.62) | 0.6221 | 0.15 (±0.11) | 0.15 (±0.10) | 0.3910 | 0.24 (±0.48) | 0.23 (±0.44) | 0.7800 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwolińska, W.; Skibinska, M.; Słopień, A.; Dmitrzak-Węglarz, M. ProBDNF as an Indicator of Improvement among Women with Depressive Episodes. Metabolites 2022, 12, 358. https://doi.org/10.3390/metabo12040358
Zwolińska W, Skibinska M, Słopień A, Dmitrzak-Węglarz M. ProBDNF as an Indicator of Improvement among Women with Depressive Episodes. Metabolites. 2022; 12(4):358. https://doi.org/10.3390/metabo12040358
Chicago/Turabian StyleZwolińska, Weronika, Maria Skibinska, Agnieszka Słopień, and Monika Dmitrzak-Węglarz. 2022. "ProBDNF as an Indicator of Improvement among Women with Depressive Episodes" Metabolites 12, no. 4: 358. https://doi.org/10.3390/metabo12040358
APA StyleZwolińska, W., Skibinska, M., Słopień, A., & Dmitrzak-Węglarz, M. (2022). ProBDNF as an Indicator of Improvement among Women with Depressive Episodes. Metabolites, 12(4), 358. https://doi.org/10.3390/metabo12040358