
Identification of Exhaled Metabolites in Children with Cystic Fibrosis

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Compound Identification
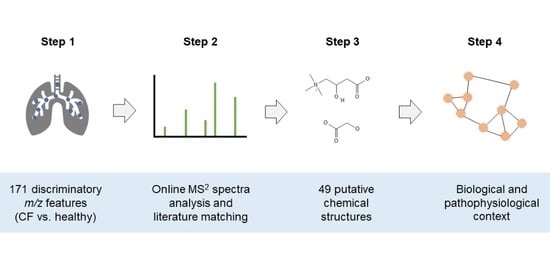
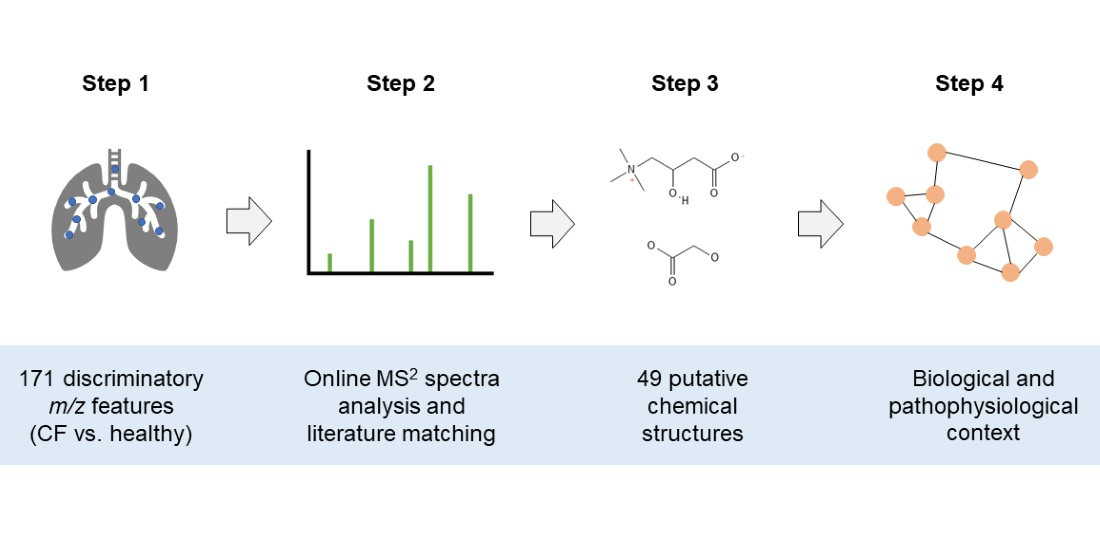
- List of significant m/z features differentiating children with CF from healthy controls.
- The m/z features were clustered in groups, according to their pairwise correlation, followed by a search of adduct and loss patterns in each group of m/z features based on differences of exact masses, as described in Kaeslin et al. [19].
- On-line breath data acquisition was carried out sequentially by:
- A full MS1 scan (m/z 50–500).
- MS2 scans of the target masses.
- The following criteria were considered, in order to decide whether or not to record an MS2 spectra:
- Presence and intensity of the target peak (>30 counts per second (cps)).
- The number of peaks (>30 cps) within the mass isolation window of 0.7 Dalton that would be co-fragmented.
- The intensities of the surrounding peaks from b. In relation to the intensity of the target peak (intensity target peak ≥ intensity of surrounding peaks).
- m/z features over 300 were excluded, due to the fact that their intensities were low, and the amount of possible molecular formulae and structures increases with higher masses, making the correct annotation based on on-line breath MS2 spectra less likely.
- On-line MS2 spectra of the peaks passing the quality control were recorded.
- The recorded MS2 spectra were analyzed with the SIRIUS software [34], using the following settings:
- Molecular formula search: instrument: Q-TOF mass deviation: 20 ppm database search: KEGG and HMDB ionization: [M + H] + elemental restrictions: C, H, O, N: 0–infinity; S: 0–2
- Structure elucidation: database search: KEGG and HMDB adducts: [M + H]+, [M + H2O + H]+, [M − H2O + H]+, [M + NH4]+, [M − H]−, [M + H2O − H]−, [M − H2O − H]−
- From step 6, MS2 spectra received potential putative structure candidates as suggested by SIRIUS. The remaining 9 did not receive a structure suggestion.
- In parallel, all significant m/z features were matched to compounds previously published by SESI-HRMS using exact mass comparison below a threshold of 10 parts per million (ppm).
- The compound suggestions from the MS2 spectra analysis (step 6/7) and the literature comparison (step 8) were integrated to receive the most plausible final compound suggestion:
- m/z features that only had compound hit(s) from MS2 analysis by SIRIUS: the putative compound suggestion with the best CSI:FingerID score [35] and protonated or deprotonated ionization, the most common ionization form in SESI [13,39], was selected. Where a different ion species had a CSI:FingerID with a magnitude of at least 30 units better than the [M + H] +/[M − H]− ionization, the corresponding putative compound suggestion was selected instead, due to the higher probability score according to the structure prediction by SIRIUS.
- m/z features that had only a compound hit from literature: the proposed compound from the literature was selected.
- m/z features that had hits from both the MS2 analysis and the literature: comparison of all possible compound suggestions from SIRIUS with that from the literature. Selection of the most plausible putative compound.
- Additional matches to chemical groups that were represented by more than three compounds were searched by exact mass comparison with database entries in KEGG and HMDB.
- Known compounds with high molecular weights (m/z > 300) and high intensities that were automatically excluded in step 4, were identified by exact mass comparison with a list of common mass spectrometry contaminants by Keller et al. [40] and further confirmed by on-line MS2 fragment spectra analysis.
- A list of compounds that could be assigned with putative structures. The final compounds were assigned with an identification (ID) level according to Schymanski et al. [41] (ID 1 = highest certainty, ID 5 = lowest certainty). Putative compound suggestions from on-line MS2 analysis = ID 3, from exact mass and chemical group matching = ID 4. For compounds from the literature, the ID level was adapted to the identification certainty in the literature.
2.2. Data Analysis
3. Results
3.1. Compound Identification Workflow
3.2. Putative Chemical Structures
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armstrong, D.S.; Hook, S.M.; Jamsen, K.M.; Nixon, G.M.; Carzino, R.; Carlin, J.B.; Robertson, C.F.; Grimwood, K. Lower Airway Inflammation in Infants with Cystic Fibrosis Detected by Newborn Screening. Pediatr. Pulmonol. 2005, 40, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Goss, C.H. Acute Pulmonary Exacerbations in Cystic Fibrosis. Semin. Respir. Crit. Care Med. 2019, 40, 792–803. [Google Scholar] [CrossRef] [PubMed]
- Laguna, T.A.; Wagner, B.D.; Williams, C.B.; Stevens, M.J.; Robertson, C.E.; Welchlin, C.W.; Moen, C.E.; Zemanick, E.T.; Harris, J.K. Airway Microbiota in Bronchoalveolar Lavage Fluid from Clinically Well Infants with Cystic Fibrosis. PLoS ONE 2016, 11, e0167649. [Google Scholar] [CrossRef] [PubMed]
- Popov, T.A. Human Exhaled Breath Analysis. Ann. Allergy Asthma Immunol. 2011, 106, 451–456. [Google Scholar] [CrossRef]
- Singh, K.D.; Tancev, G.; Decrue, F.; Usemann, J.; Appenzeller, R.; Barreiro, P.; Jaumà, G.; Macia Santiago, M.; Vidal de Miguel, G.; Frey, U.; et al. Standardization Procedures for Real-Time Breath Analysis by Secondary Electrospray Ionization High-Resolution Mass Spectrometry. Anal. Bioanal. Chem. 2019, 411, 4883–4898. [Google Scholar] [CrossRef]
- Martinez-Lozano Sinues, P.; Meier, L.; Berchtold, C.; Ivanov, M.; Sievi, N.; Camen, G.; Kohler, M.; Zenobi, R. Breath Analysis in Real Time by Mass Spectrometry in Chronic Obstructive Pulmonary Disease. Respiration 2014, 87, 301–310. [Google Scholar] [CrossRef]
- Schwarz, E.I.; Martinez-Lozano Sinues, P.; Bregy, L.; Gaisl, T.; Garcia Gomez, D.; Gaugg, M.T.; Suter, Y.; Stebler, N.; Nussbaumer-Ochsner, Y.; Bloch, K.E.; et al. Effects of CPAP Therapy Withdrawal on Exhaled Breath Pattern in Obstructive Sleep Apnoea. Thorax 2016, 71, 110. [Google Scholar] [CrossRef]
- Gaugg, M.T.; Engler, A.; Bregy, L.; Nussbaumer-Ochsner, Y.; Eiffert, L.; Bruderer, T.; Zenobi, R.; Sinues, P.; Kohler, M. Molecular Breath Analysis Supports Altered Amino Acid Metabolism in Idiopathic Pulmonary Fibrosis. Respirology 2019, 24, 437–444. [Google Scholar] [CrossRef]
- Gaisl, T.; Bregy, L.; Stebler, N.; Gaugg, M.; Bruderer, T.; Garc\’\ia-Gómez, D.; Möller, A.; Singer, F.; Schwarz, E.; Benden, C.; et al. Real-Time Exhaled Breath Analysis Identifies Altered Metabolic Signature in Cystic Fibrosis. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef]
- Gaugg, M.T.; Nussbaumer-Ochsner, Y.; Bregy, L.; Engler, A.; Stebler, N.; Gaisl, T.; Bruderer, T.; Nowak, N.; Sinues, P.; Zenobi, R.; et al. Real-Time Breath Analysis Reveals Specific Metabolic Signatures of COPD Exacerbations. Chest 2019, 156, 269–276. [Google Scholar] [CrossRef]
- García-Gómez, D.; Gaisl, T.; Bregy, L.; Cremonesi, A.; Sinues, P.M.-L.; Kohler, M.; Zenobi, R. Real-Time Quantification of Amino Acids in the Exhalome by Secondary Electrospray Ionization–Mass Spectrometry: A Proof-of-Principle Study. Clin. Chem. 2016, 62, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- García-Gómez, D.; Martínez-Lozano Sinues, P.; Barrios-Collado, C.; Vidal-de-Miguel, G.; Gaugg, M.; Zenobi, R. Identification of 2-Alkenals, 4-Hydroxy-2-Alkenals, and 4-Hydroxy-2,6-Alkadienals in Exhaled Breath Condensate by UHPLC-HRMS and in Breath by Real-Time HRMS. Anal. Chem. 2015, 87, 3087–3093. [Google Scholar] [CrossRef]
- Gaugg, M.T.; Bruderer, T.; Nowak, N.; Eiffert, L.; Martinez-Lozano Sinues, P.; Kohler, M.; Zenobi, R. Mass-Spectrometric Detection of Omega-Oxidation Products of Aliphatic Fatty Acids in Exhaled Breath. Anal. Chem. 2017, 89, 10329–10334. [Google Scholar] [CrossRef] [PubMed]
- Nowak, N.; Engler, A.; Thiel, S.; Stöberl, A.S.; Sinues, P.; Zenobi, R.; Kohler, M. Validation of Breath Biomarkers for Obstructive Sleep Apnea. Sleep Med. 2021, 85, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Gaugg, M.T.; Gomez, D.G.; Barrios-Collado, C.; Vidal-de-Miguel, G.; Kohler, M.; Zenobi, R.; Sinues, P.M.-L. Expanding Metabolite Coverage of Real-Time Breath Analysis by Coupling a Universal Secondary Electrospray Ionization Source and High Resolution Mass Spectrometrya Pilot Study on Tobacco Smokers. J. Breath Res. 2016, 10, 16010. [Google Scholar] [CrossRef] [PubMed]
- Sindelar, M.; Patti, G.J. Chemical Discovery in the Era of Metabolomics. J. Am. Chem. Soc. 2020, 142, 9097–9105. [Google Scholar] [CrossRef]
- Kaeslin, J.; Zenobi, R. Resolving Isobaric Interferences in Direct Infusion Tandem Mass Spectrometry. Rapid Commun. Mass Spectrom. 2022, 36, e9266. [Google Scholar] [CrossRef]
- Nowak, N.; Gaisl, T.; Miladinovic, D.; Marcinkevics, R.; Osswald, M.; Bauer, S.; Buhmann, J.; Zenobi, R.; Sinues, P.; Brown, S.A.; et al. Rapid and Reversible Control of Human Metabolism by Individual Sleep States. Cell Rep. 2021, 37. [Google Scholar] [CrossRef]
- Kaeslin, J.; Micic, S.; Weber, R.; Müller, S.; Perkins, N.; Berger, C.; Zenobi, R.; Bruderer, T.; Moeller, A. Differentiation of Cystic Fibrosis-Related Pathogens by Volatile Organic Compound Analysis with Secondary Electrospray Ionization Mass Spectrometry. Metabolites 2021, 11, 773. [Google Scholar] [CrossRef]
- Weber, R.; Streckenbach, B.; Welt, L.; Inci, D.; Kohler, M.; Perkins, N.; Zenobi, R.; Micic, S.; Moeller, A. Metabolic Signatures for Allergic Asthma in Children by Online Breath Analysis. Division of Respiratory Medicine, University Children’s Hospital Zurich: Zurich, Switzerland, 2022; to be submitted. [Google Scholar]
- Singh, K.D.; Osswald, M.; Ziesenitz, V.C.; Awchi, M.; Usemann, J.; Imbach, L.L.; Kohler, M.; García-Gómez, D.; van den Anker, J.; Frey, U.; et al. Personalised Therapeutic Management of Epileptic Patients Guided by Pathway-Driven Breath Metabolomics. Commun. Med. 2021, 1, 21. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Meinardi, S.; Blake, D.; Whiteson, K. Bacteria in the Airways of Patients with Cystic Fibrosis Are Genetically Capable of Producing VOCs in Breath. J. Breath Res. 2016, 10, 47103. [Google Scholar] [CrossRef] [PubMed]
- Neerincx, A.H.; Geurts, B.P.; van Loon, J.; Tiemes, V.; Jansen, J.J.; Harren, F.J.M.; Kluijtmans, L.A.J.; Merkus, P.J.F.M.; Cristescu, S.M.; Buydens, L.M.C.; et al. Detection of Staphylococcus Aureus in Cystic Fibrosis Patients Using Breath VOC Profiles. J. Breath Res. 2016, 10, 046014. [Google Scholar] [CrossRef] [PubMed]
- Enderby, B.; Smith, D.; Carroll, W.; Lenney, W. Hydrogen Cyanide as a Biomarker for Pseudomonas Aeruginosa in the Breath of Children with Cystic Fibrosis. Pediatr. Pulmonol. 2009, 44, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Shestivska, V.; Nemec, A.; Dřevínek, P.; Sovová, K.; Dryahina, K.; Španěl, P. Quantification of Methyl Thiocyanate in the Headspace of Pseudomonas Aeruginosa Cultures and in the Breath of Cystic Fibrosis Patients by Selected Ion Flow Tube Mass Spectrometry. Rapid Commun. Mass Spectrom. 2011, 25, 2459–2467. [Google Scholar] [CrossRef]
- Kos, R.; Brinkman, P.; Neerincx, A.H.; Paff, T.; Gerritsen, M.G.; Lammers, A.; Kraneveld, A.D.; Heijerman, H.G.M.; Janssens, H.M.; Davies, J.C.; et al. Targeted Exhaled Breath Analysis for Detection of Pseudomonas Aeruginosa in Cystic Fibrosis Patients. J. Cyst. Fibros. 2022, 21, e28–e34. [Google Scholar] [CrossRef] [PubMed]
- Barker, M.; Hengst, M.; Schmid, J.; Buers, H.-J.; Mittermaier, B.; Klemp, D.; Koppmann, R. Volatile Organic Compounds in the Exhaled Breath of Young Patients with Cystic Fibrosis. Eur. Respir. J. 2006, 27, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Robroeks, C.M.H.H.T.; van Berkel, J.J.B.N.; Dallinga, J.W.; Jöbsis, Q.; Zimmermann, L.J.I.; Hendriks, H.J.E.; Wouters, M.F.M.; van der Grinten, C.P.M.; van de Kant, K.D.G.; van Schooten, F.-J.; et al. Metabolomics of Volatile Organic Compounds in Cystic Fibrosis Patients and Controls. Pediatr. Res. 2010, 68, 75–80. [Google Scholar] [CrossRef]
- van Mastrigt, E.; Reyes-Reyes, A.; Brand, K.; Bhattacharya, N.; Urbach, H.P.; Stubbs, A.P.; de Jongste, J.C.; Pijnenburg, M.W. Exhaled Breath Profiling Using Broadband Quantum Cascade Laser-Based Spectroscopy in Healthy Children and Children with Asthma and Cystic Fibrosis. J. Breath Res. 2016, 10, 026003. [Google Scholar] [CrossRef]
- Weber, R.; Haas, N.; Baghdasaryan, A.; Bruderer, T.; Inci, D.; Micic, S.; Perkins, N.; Spinas, R.; Zenobi, R.; Moeller, A. Volatile Organic Compound Breath Signatures of Children with Cystic Fibrosis by Real-Time SESI-HRMS. ERJ Open Res. 2020, 6, 00171–02019. [Google Scholar] [CrossRef]
- Segers, K.; Slosse, A.; Viaene, J.; Bannier, M.A.G.E.; van de Kant, K.D.G.; Dompeling, E.; van Eeckhaut, A.; Vercammen, J.; vander Heyden, Y. Feasibility Study on Exhaled-Breath Analysis by Untargeted Selected-Ion Flow-Tube Mass Spectrometry in Children with Cystic Fibrosis, Asthma, and Healthy Controls: Comparison of Data Pretreatment and Classification Techniques. Talanta 2021, 225, 122080. [Google Scholar] [CrossRef]
- Kramer, R.; Sauer-Heilborn, A.; Welte, T.; Guzman, C.A.; Höfle, M.G.; Abraham, W.-R. A Rapid Method for Breath Analysis in Cystic Fibrosis Patients. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Kessner, D.; Chambers, M.; Burke, R.; Agus, D.; Mallick, P. ProteoWizard: Open Source Software for Rapid Proteomics Tools Development. Bioinformatics 2008, 24, 2534–2536. [Google Scholar] [CrossRef]
- Dührkop, K.; Fleischauer, M.; Ludwig, M.; Aksenov, A.A.; Melnik, A.V.; Meusel, M.; Dorrestein, P.C.; Rousu, J.; Böcker, S. SIRIUS 4: A Rapid Tool for Turning Tandem Mass Spectra into Metabolite Structure Information. Nat. Methods 2019, 16, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Kai, D.; Huibin, S.; Marvin, M.; Juho, R.; Sebastian, B. Searching Molecular Structure Databases with Tandem Mass Spectra Using CSI:FingerID. Proc. Natl. Acad. Sci. USA 2015, 112, 12580–12585. [Google Scholar] [CrossRef]
- Hoffmann, M.A.; Nothias, L.-F.; Ludwig, M.; Fleischauer, M.; Gentry, E.C.; Witting, M.; Dorrestein, P.C.; Dührkop, K.; Böcker, S. Assigning Confidence to Structural Annotations from Mass Spectra with COSMIC. bioRxiv 2021. [Google Scholar] [CrossRef]
- Kanehisa, M.; Goto, S. KEGG: Kyoto Encyclopedia of Genes and Genomes. Nucleic Acids Res. 2000, 28, 27–30. [Google Scholar] [CrossRef]
- Wishart, D.S.; Guo, A.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucleic Acids Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- Rioseras, A.T.; Gaugg, M.T.; Martinez-Lozano Sinues, P. Secondary Electrospray Ionization Proceeds via Gas-Phase Chemical Ionization. Anal. Methods 2017, 9, 5052–5057. [Google Scholar] [CrossRef]
- Keller, B.O.; Sui, J.; Young, A.B.; Whittal, R.M. Interferences and Contaminants Encountered in Modern Mass Spectrometry. Anal. Chim. Acta 2008, 627, 71–81. [Google Scholar] [CrossRef]
- Schymanski, E.L.; Jeon, J.; Gulde, R.; Fenner, K.; Ruff, M.; Singer, H.P.; Hollender, J. Identifying Small Molecules via High Resolution Mass Spectrometry: Communicating Confidence. Environ. Sci. Technol. 2014, 48, 2097–2098. [Google Scholar] [CrossRef]
- Gu, Z.; Eils, R.; Schlesner, M. Complex Heatmaps Reveal Patterns and Correlations in Multidimensional Genomic Data. Bioinformatics 2016, 32, 2847–2849. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. Qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef]
- Berchtold, C.; Meier, L.; Steinhoff, R.; Zenobi, R. A New Strategy Based on Real-Time Secondary Electrospray Ionization and High-Resolution Mass Spectrometry to Discriminate Endogenous and Exogenous Compounds in Exhaled Breath. Metabolomics 2014, 10, 291–301. [Google Scholar] [CrossRef]
- Martínez-Lozano, P.; Zingaro, L.; Finiguerra, A.; Cristoni, S. Secondary Electrospray Ionization-Mass Spectrometry: Breath Study on a Control Group. J. Breath Res. 2011, 5, 016002. [Google Scholar] [CrossRef] [PubMed]
- Bonferroni Carlo, E. Teoria Statistica Delle Classi e Calcolo Delle Probabilità. Pubbl. Del R Ist. Super. Di Sci. Econ. E Commer. Di Firenze 1936, 8, 1–62. [Google Scholar]
- Dunn, O.J. Multiple Comparisons among Means. J. Am. Stat. Assoc. 1961, 56, 52–64. [Google Scholar] [CrossRef]
- Hoppe, B.; Leumann, E.; von Unruh, G.; Laube, N.; Hesse, A. Diagnostic and Therapeutic Approaches in Patients with Secondary Hyperoxaluria. Front. Biosci. 2003, 8, e437-43. [Google Scholar] [CrossRef]
- Terribile, M.; Capuano, M.; Cangiano, G.; Carnovale, V.; Ferrara, P.; Petrarulo, M.; Marangella, M. Factors Increasing the Risk for Stone Formation in Adult Patients with Cystic Fibrosis. Nephrol. Dial. Transplant. 2006, 21, 1870–1875. [Google Scholar] [CrossRef]
- Turner, M.A.; Goldwater, D.; David, T.J. Oxalate and Calcium Excretion in Cystic Fibrosis. Arch. Dis. Child. 2000, 83, 244. [Google Scholar] [CrossRef]
- Kopp, B.T.; Joseloff, E.; Goetz, D.; Ingram, B.; Heltshe, S.L.; Leung, D.H.; Ramsey, B.W.; McCoy, K.; Borowitz, D. Urinary Metabolomics Reveals Unique Metabolic Signatures in Infants with Cystic Fibrosis. J. Cyst. Fibros. 2019, 18, 507–515. [Google Scholar] [CrossRef]
- Hagopian, K.; Ramsey, J.J.; Weindruch, R. Enzymes of Glycerol and Glyceraldehyde Metabolism in Mouse Liver: Effects of Caloric Restriction and Age on Activities. Biosci. Rep. 2008, 28, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Esther, C.R.; Turkovic, L.; Rosenow, T.; Muhlebach, M.S.; Boucher, R.C.; Ranganathan, S.; Stick, S.M. Metabolomic Biomarkers Predictive of Early Structural Lung Disease in Cystic Fibrosis. Eur. Respir. J. 2016, 48, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Wetmore, D.R.; Joseloff, E.; Pilewski, J.; Lee, D.P.; Lawton, K.A.; Mitchell, M.W.; Milburn, M.V.; Ryals, J.A.; Guo, L. Metabolomic Profiling Reveals Biochemical Pathways and Biomarkers Associated with Pathogenesis in Cystic Fibrosis Cells*. J. Biol. Chem. 2010, 285, 30516–30522. [Google Scholar] [CrossRef] [PubMed]
- Brothers, H.M., Jr.; Boehmer, T.; Campbell, R.A.; Dorn, S.; Kerbleski, J.J.; Lewis, S.; Mund, C.; Pero, D.; Saito, K.; Wieser, M.; et al. Determination of Cyclic Volatile Methylsiloxanes in Personal Care Products by Gas Chromatography. Int. J. Cosmet. Sci. 2017, 39, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Mark, J.E.; Allcock, H.R.; West, R. Polysiloxanes and Related Polymers. In Inorganic Polymers; Oxford Academic: New York, NY, USA, 2005; pp. 154–199. [Google Scholar] [CrossRef]
- Beauchamp, J. Inhaled Today, Not Gone Tomorrow: Pharmacokinetics and Environmental Exposure of Volatiles in Exhaled Breath. J. Breath Res. 2011, 5, 037103. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.B.; Mottlowitz, M.; Kruk, M.E.; Mickelson, A.; Wagner, B.D.; Harris, J.K.; Wendt, C.H.; Laguna, T.A. Network Analysis to Identify Multi-Omic Correlations in the Lower Airways of Children with Cystic Fibrosis. Front. Cell. Infect. Microbiol. 2022, 12. [Google Scholar] [CrossRef]
- Joseloff, E.; Sha, W.; Bell, S.C.; Wetmore, D.R.; Lawton, K.A.; Milburn, M.V.; Ryals, J.A.; Guo, L.; Muhlebach, M.S. Serum Metabolomics Indicate Altered Cellular Energy Metabolism in Children with Cystic Fibrosis. Pediatr. Pulmonol. 2014, 49, 463–472. [Google Scholar] [CrossRef]
- DiBattista, A.; McIntosh, N.; Lamoureux, M.; Al-Dirbashi, O.Y.; Chakraborty, P.; Britz-McKibbin, P. Metabolic Signatures of Cystic Fibrosis Identified in Dried Blood Spots For Newborn Screening without Carrier Identification. J. Proteome Res. 2019, 18, 841–854. [Google Scholar] [CrossRef]
- Dambrova, M.; Makrecka-Kuka, M.; Kuka, J.; Vilskersts, R.; Nordberg, D.; Attwood, M.M.; Smesny, S.; Sen, Z.D.; Guo, A.C.; Oler, E.; et al. Acylcarnitines: Nomenclature, Biomarkers, Therapeutic Potential, Drug Targets, and Clinical Trials. Pharmacol. Rev. 2022, 74, 506–551. [Google Scholar] [CrossRef]
- Rutkowsky, J.M.; Knotts, T.A.; Ono-Moore, K.D.; McCoin, C.S.; Huang, S.; Schneider, D.; Singh, S.; Adams, S.H.; Hwang, D.H. Acylcarnitines Activate Proinflammatory Signaling Pathways. Am. J. Physiol. -Endocrinol. Metab. 2014, 306, E1378–E1387. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid Peroxidation: Production, Metabolism, and Signaling Mechanisms of Malondialdehyde and 4-Hydroxy-2-Nonenal. Oxid. Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef] [PubMed]
- Galli, F.; Battistoni, A.; Gambari, R.; Pompella, A.; Bragonzi, A.; Pilolli, F.; Iuliano, L.; Piroddi, M.; Dechecchi, M.C.; Cabrini, G. Oxidative Stress and Antioxidant Therapy in Cystic Fibrosis. Biochim. Et Biophys. Acta (BBA)—Mol. Basis Dis. 2012, 1822, 690–713. [Google Scholar] [CrossRef] [PubMed]
- Antus, B.; Drozdovszky, O.; Barta, I.; Kelemen, K. Comparison of Airway and Systemic Malondialdehyde Levels for Assessment of Oxidative Stress in Cystic Fibrosis. Lung 2015, 193, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Galiniak, S.; Mołoń, M.; Rachel, M. Links between Disease Severity, Bacterial Infections and Oxidative Stress in Cystic Fibrosis. Antioxidants 2022, 11, 887. [Google Scholar] [CrossRef] [PubMed]
- Sinharoy, P.; McAllister, S.L.; Vasu, M.; Gross, E.R. Environmental Aldehyde Sources and the Health Implications of Exposure. In Aldehyde Dehydrogenases: From Alcohol Metabolism to Human Health and Precision Medicine; Ren, J., Zhang, Y., Ge, J., Eds.; Springer: Singapore, 2019; pp. 35–52. ISBN 978-981-13-6260-6. [Google Scholar]
- Brugha, R.; Edmondson, C.; Davies, J.C. Outdoor Air Pollution and Cystic Fibrosis. Paediatr. Respir. Rev. 2018, 28, 80–86. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Mode | m/z | Adj. p-Value | Class | Compound | Formula | Ionization | ID Level | ID Source |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Positive | 160.0965 | 0.014 | Acylcarnitines | Dehydrocarnitine | C7H13NO3 | [M + H]+ | ID4 | [18] |
| 2 | 162.1123 | 0.025 | Carnitine | C7H15NO3 | [M + H]+ | ID1 | [18], MS2 | ||
| 3 | 204.123 | 0.020 | Acetylcarnitine | C9H17NO4 | [M + H]+ | ID1 | [18] | ||
| 4 | 216.1235 | 0.025 | Acryloylcarnitine Propenoylcarnitine | C10H17NO4 | [M + H]+ | ID4 | [18], HMDB | ||
| 5 | 218.1388 | 0.035 | Propionylcarnitine | C10H19NO4 | [M + H]+ | ID1 | [18] | ||
| 6 | 230.1392 | 0.020 | Butenylcarnitine | C11H19NO4 | [M + H]+ | ID4 | HMDB | ||
| 7 | 232.154 | 0.020 | Butyrylcarnitine | C11H21NO4 | [M + H]+ | ID4 | [18] | ||
| 8 | 234.1335 | 0.022 | Hydroxypropionylcarnitine | C10H19NO5 | [M + H]+ | ID4 | HMDB | ||
| 9 | 234.1697 | 0.025 | Tiglylcarnitine | C12H21NO | [M + H]+ | ID4 | HMDB | ||
| 10 | 246.17 | 0.035 | 2-Methylbutyrylcarnitine | C12H23NO4 | [M + H]+ | ID4 | HMDB | ||
| 11 | 260.222 | 0.030 | Octanoylcarnitine | C15H30NO4 | [M − CO + H]+ | ID4 | [20] | ||
| 12 | 262.1648 | 0.049 | Hydroxyisovaleroyl carnitine | C12H23NO5 | [M + H]+ | ID4 | HMDB | ||
| 13 | 286.201 | 0.018 | Octenoylcarnitine | C15H27NO4 | [M + H]+ | ID4 | HMDB | ||
| 14 | 304.2115 | 0.035 | 3-Hydroxyoctanoyl carnitine | C15H29NO5 | [M + H]+ | ID4 | HMDB | ||
| 15 | 318.221 | 0.044 | 3 -Hydroxynonanoyl carnitine | C16H31NO5 | [M + H]+ | ID4 | HMDB | ||
| 16 | 332.2448 | 0.048 | 3-Hydroxydecanoyl carnitine | C17H33NO5 | [M + H]+ | ID4 | HMDB | ||
| 17 | 144.138 | 0.005 | Aldehydes | Octenal | C8H14O | [M + NH4]+ | ID4 | HMDB, MS2 | |
| 18 | 172.1693 | 0.035 | 2-Decenal | C10H18O | [M + NH4]+ | ID1 | [12] | ||
| 19 | 132.101 | 0.022 | 4-Hydroxy-2-hexenal | C6H10O2 | [M + NH4]+ | ID4 | [12] | ||
| 20 | 146.1175 | 0.018 | 4-Hydroxy-2-heptenal | C7H12O2 | [M + NH4]+ | ID4 | [12] | ||
| 21 | 160.133 | 0.039 | 4-Hydroxy-2-octenal | C8H14O2 | [M + NH4]+ | ID4 | [12] | ||
| 22 | 188.1645 | 0.002 | 4-Hydroxy-2-decenal | C10H18O2 | [M + NH4]+ | ID1 | [12] | ||
| 23 | 230.2117 | 0.046 | 4-Hydroxy-2-tridecenal | C13H24O2 | [M + NH4]+ | ID4 | [12] | ||
| 24 | 244.227 | 0.047 | 4-Hydroxy-2-tetradecenal | C14H26O2 | [M + NH4]+ | ID4 | [12] | ||
| 25 | 144.1022 | 0.050 | 4-Hydroxy-2,6-heptadienal | C7H10O2 | [M + NH4]+ | ID4 | [12] | ||
| 26 | 211.1688 | 0.047 | 4-Hydroxy-2,6-tridecadienal | C13H22O2 | [M + H]+ | ID1 | [12] | ||
| 27 | 60.0808 | 0.012 | Trimethylamine | C3H9N | [M + H]+ | ID3 | MS2 | ||
| 31 | 340.2482 | 0.015 | Evocarpine | C23H33NO | [M + H]+ | ID4 | [44] | ||
| 28 | 146.0813 | 0.047 | Acids | 4-Acetamidobutyric acid | C6H11NO3 | [M + H]+ | ID3 | MS2 | |
| 29 | 162.0757 | 0.032 | 2-Aminoadipic acid | C6H11NO4 | [M + H]+ | ID3 | [20], MS2 | ||
| 30 | 188.128 | 0.047 | 8-Amino-7-oxononanoic acid | C9H17NO3 | [M + H]+ | ID3 | MS2 | ||
| 32 | Negative | 115.0763 | 0.022 | Hexanoic acid | C6H12O2 | [M − H]− | ID4 | [45] | |
| 33 | 171.1028 | 0.014 | 9-Oxononanoic acid | C9H16O3 | [M − H]− | ID1 | [13], MS2 | ||
| 34 | 199.134 | 0.050 | 11-Oxoundecanoic acid | C11H20O3 | [M − H]− | ID1 | [13], MS2 |
| No. | Mode | m/z | Adj. p-Value | Class | Compound | Formula | Ionization | ID Level | ID Source |
|---|---|---|---|---|---|---|---|---|---|
| 1a | Negative | 75.0085 | <0.001 | Acids | Glycolic acid | C2H4O3 | [M − H]− | ID3 | MS2 |
| 1b | 121.0143 | <0.001 | Glycolic acid | C2H4O3 | [M + CH2O2 − H]− | ID4 | Adduct/loss | ||
| 2 | 105.0188 | 0.002 | Glyceric acid | C3H6O4 | [M − H]− | ID3 | [44], MS2 | ||
| 3 | 151.0247 | <0.001 | Xanthine | C5H4N4O2 | [M − H]− | ID1 | [10], MS2 | ||
| 4 | 137.009 | 0.012 | 5-Diazouracil | C4H2N4O2 | [M − H]− | ID3 | MS2 | ||
| 5 | Positive | 106.0858 | 0.043 | Diethanolamine. | C4H11NO2 | [M + H]+ | ID3 | [19], MS2 | |
| 6 | 163.0965 | 0.018 | 7-Oxohepatnoic acid | C7H12O3 | [M + H2O + H]+ | ID3 | MS2 | ||
| 7 | 225.0428 | 0.009 | Sideretin | C10H8O6 | [M + H]+ | ID3 | MS2 | ||
| 8 | 429.088 | 0.002 | Plasticizers | Polysiloxane | [C2H6SiO]6 | [M − CH4 + H]+ | ID2 | [40], MS2 | |
| 9 | 445.12 | 0.001 | Polysiloxane | [C2H6SiO]6 | [M + H]+ | ID2 | [40], MS2 | ||
| 10 | 462.1462 | 0.027 | Polysiloxane | [C2H6SiO]6 | [M + NH4]+ | ID2 | [40], MS2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weber, R.; Perkins, N.; Bruderer, T.; Micic, S.; Moeller, A. Identification of Exhaled Metabolites in Children with Cystic Fibrosis. Metabolites 2022, 12, 980. https://doi.org/10.3390/metabo12100980
Weber R, Perkins N, Bruderer T, Micic S, Moeller A. Identification of Exhaled Metabolites in Children with Cystic Fibrosis. Metabolites. 2022; 12(10):980. https://doi.org/10.3390/metabo12100980
Chicago/Turabian StyleWeber, Ronja, Nathan Perkins, Tobias Bruderer, Srdjan Micic, and Alexander Moeller. 2022. "Identification of Exhaled Metabolites in Children with Cystic Fibrosis" Metabolites 12, no. 10: 980. https://doi.org/10.3390/metabo12100980
APA StyleWeber, R., Perkins, N., Bruderer, T., Micic, S., & Moeller, A. (2022). Identification of Exhaled Metabolites in Children with Cystic Fibrosis. Metabolites, 12(10), 980. https://doi.org/10.3390/metabo12100980