Life-Cycle Contract as an Innovative Business Model for High-Tech Medical Organizations



 and
and
Abstract
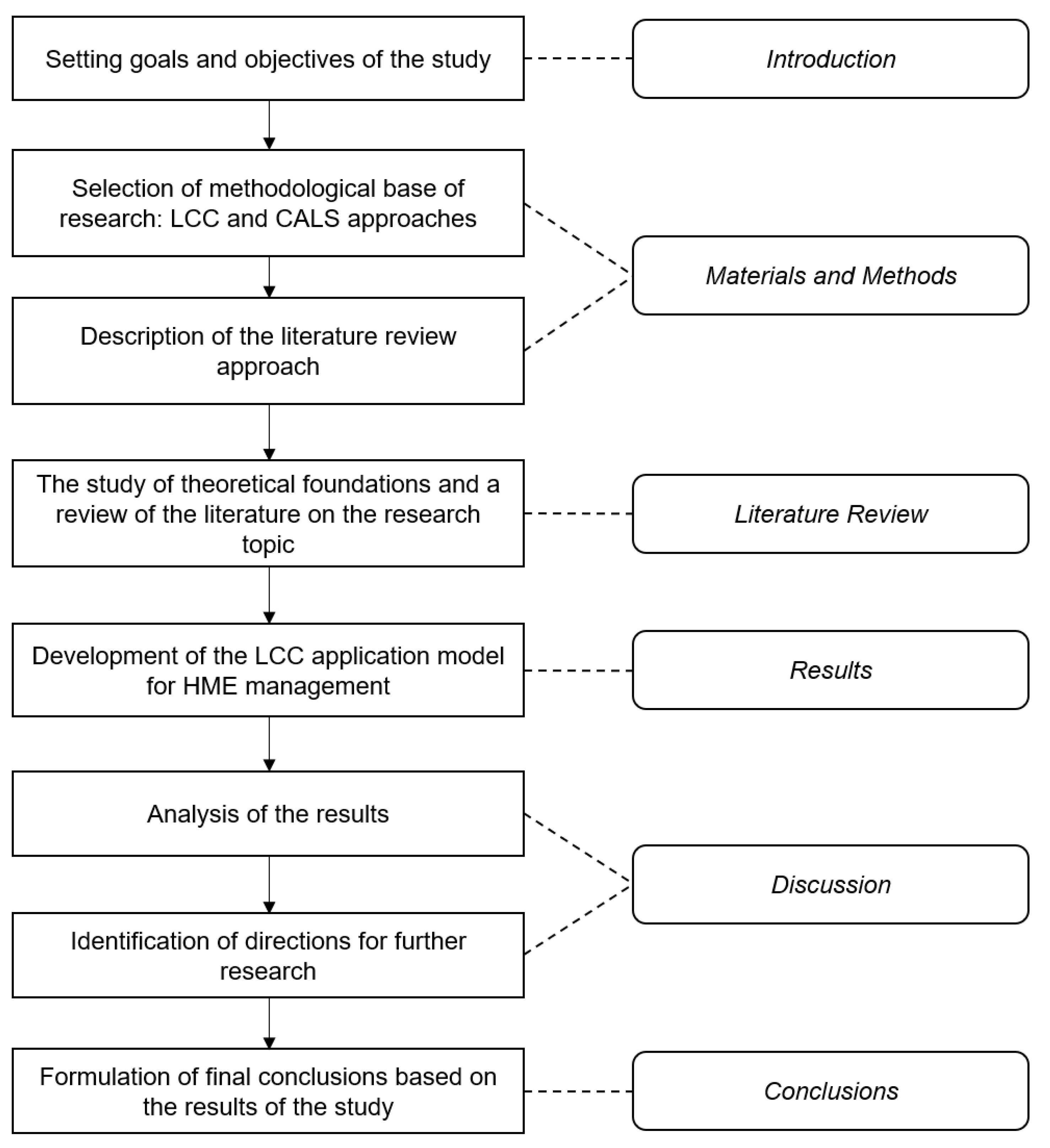
1. Introduction
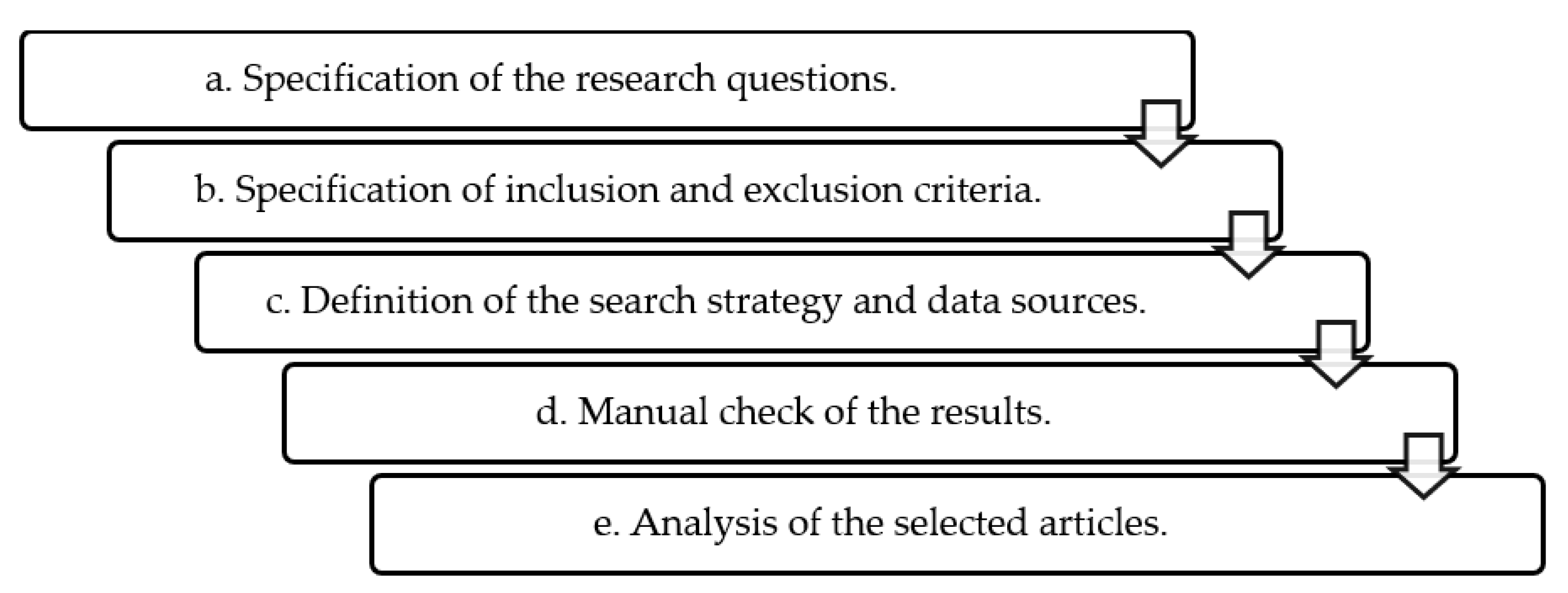
2. Materials and Methods
- Specification of the research questions.
- b.
- Specification of inclusion and exclusion criteria.
- c.
- Definition of the search strategy and data sources.
- d.
- Manual check of the results.
- e.
- Analysis of the selected papers.
3. Literature Review
- The implementation of the various stages of the project is delegated to one private contractor through a comprehensive contract, while the selection of the contractor is carried out, as a rule, on a competitive basis.
- The private partner in the LCC independently makes all design and technical decisions necessary for the implementation of the project.
- The contract is concluded for a long time period (15–30 years on average). A long-term perspective is necessary for the contractor to be able to recover its investments in the project at the stages of commissioning and maintenance of the created asset.
- The private contractor is responsible for financing the project. The private party does not receive payment when the asset is created but receives a monthly fee for the availability of the asset during the term of the contract (availability fee).
- Project risks are distributed between the customer and the contractor and fall on the party that can best manage them.
- For the state:
- No dilution of responsibility for the result between different performers and, as a result, minimization of the risks of delaying the deadline (or complete failure) of the project;
- Simplification of the contract execution control process;
- No need to conduct competitive procedures at each stage of the project implementation and, as a result, the absence of these costs;
- Payment under the contract only if the object is maintained in accordance with the functional parameters;
- “Installment plan” of payment under the contract (payment occurs from the moment the facility is put into operation and is divided into relatively small payments paid in set periods of time, so the state does not need to reserve a significant amount in the budget);
- No unpredictable future costs for infrastructure support, as the private partner is also engaged in the maintenance of the created object;
- Increased motivation of the private partner to put the object into operation as soon as possible, since it is after commissioning that the contractor begins to receive cash payments.
- For a private partner (contractor):
- Freedom of choice of design technical solutions, project management meth-ods, organization of the production process, service operations, etc.;
- A higher chance of return on investment compared to an open market player, since the risks of market uncertainties are hedged with state guarantees (subject to the fulfillment of the terms of the contract);
- Financing of value creation activities outside the credit mechanism of bank financing, since in the case of a consortium of performers, the financial insti-tution provides direct financing for operating activities and creates reserves for success fees, which are possible under a long contract;
- Innovative nature of activities to create added value: innovation is the key to higher efficiency: design, production and service.
- The long-term nature of the project;
- The existing potential for delegating several project stages to one contractor;
- The complexity of the control of each individual stage;
- Guaranteed availability of demand for equipment for a long period of time;
- The need for support, repair and modernization of equipment during the entire period of operation;
- Improvement in product quality;
- Reduction in material and time costs for the implementation of various stages of the product life cycle;
- Guaranteed security of work results that are due to the implementation of the principle of succession and safety of work results at all stages of the product life cycle;
- Increased flexibility to respond to changes;
- Reduction in calendar terms for bringing new competitive products to the market.
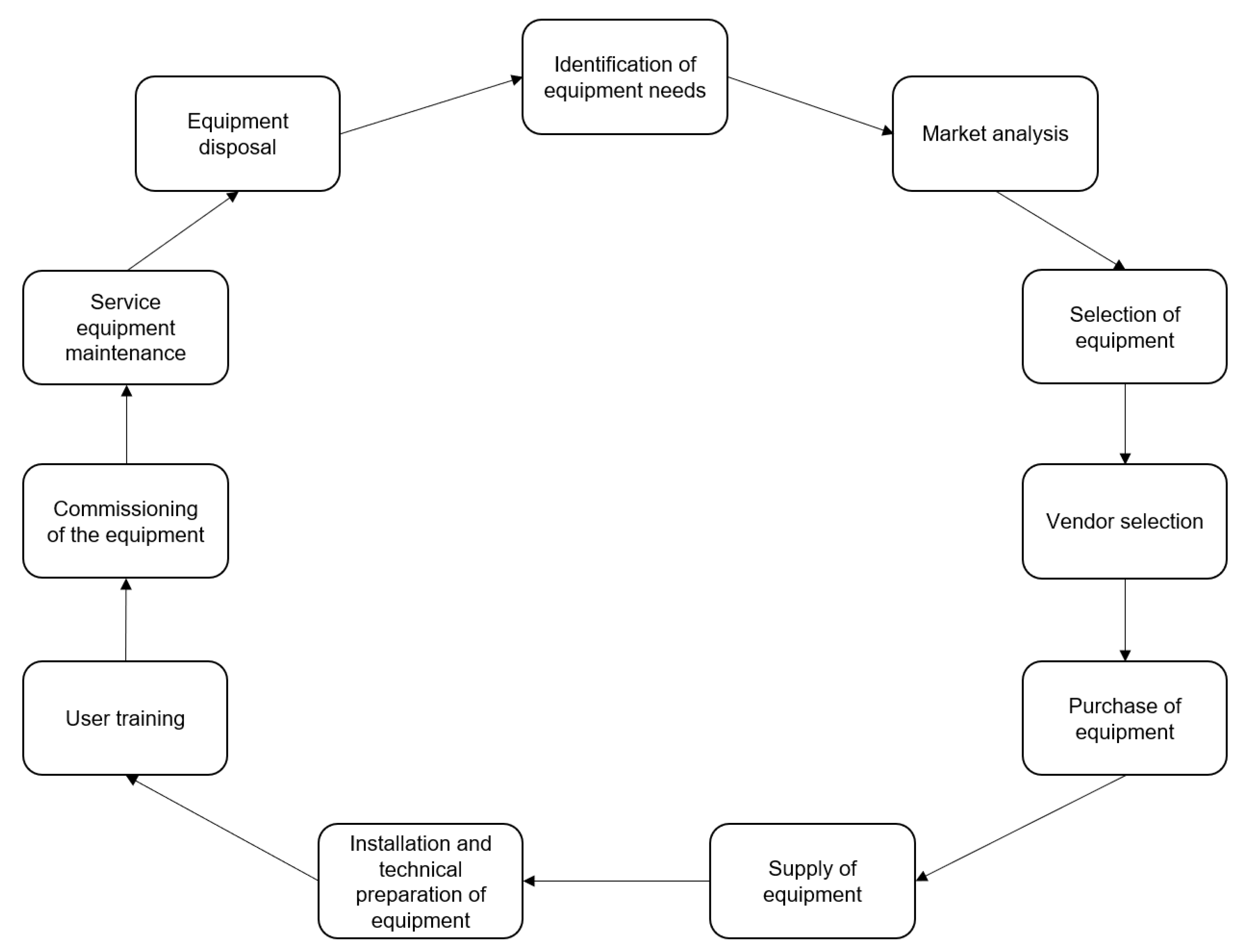
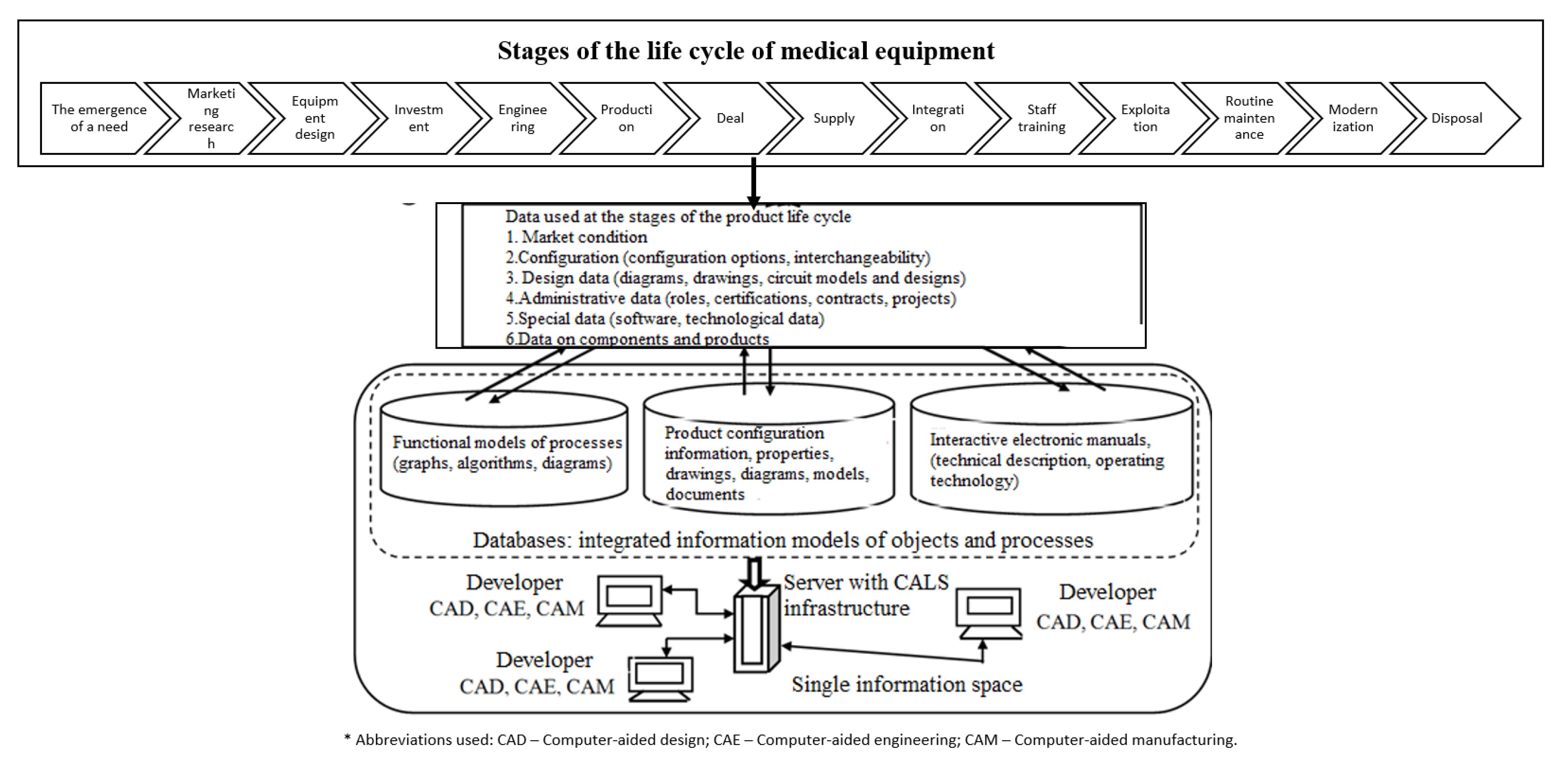
4. Results
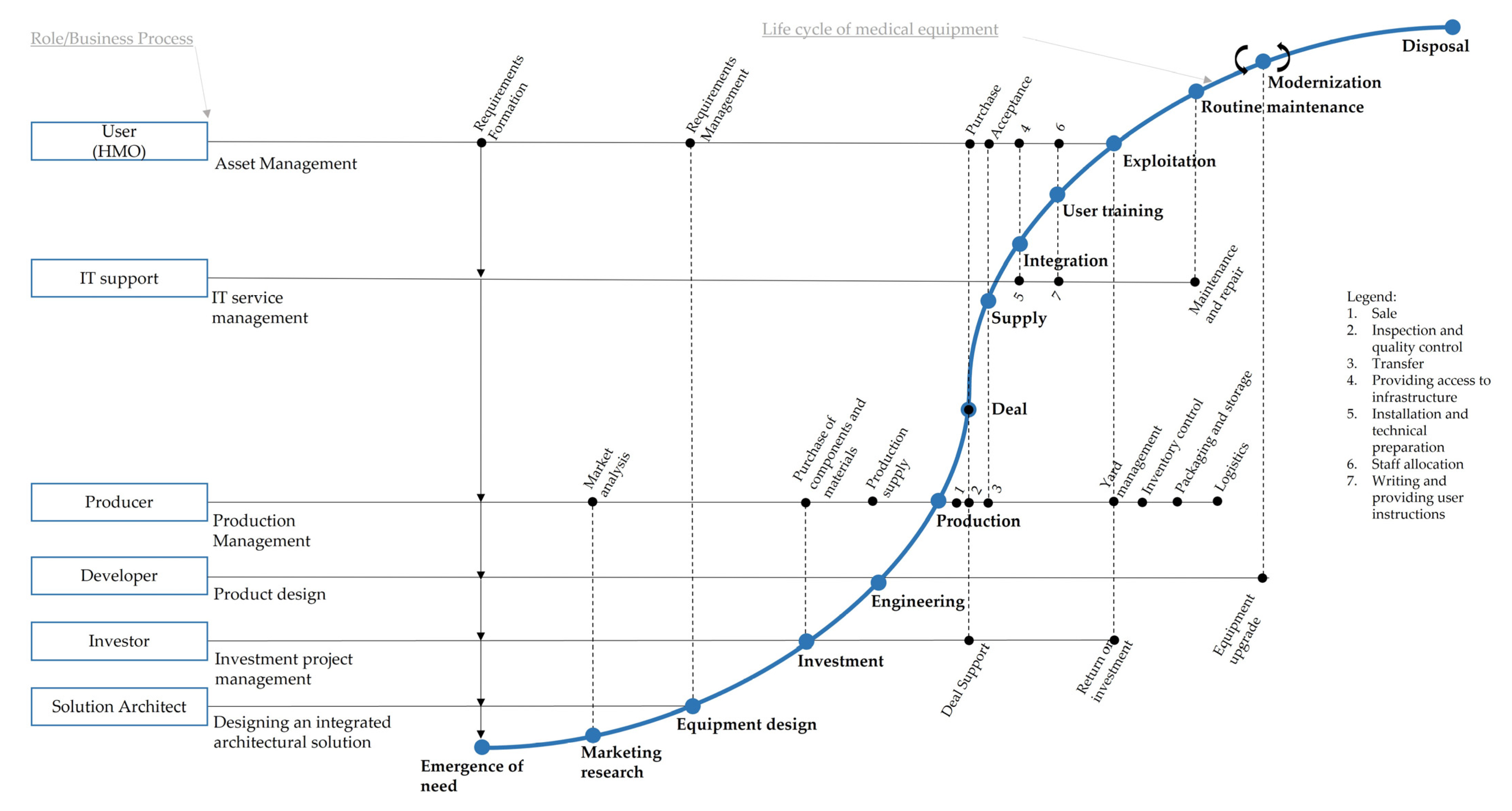
- Identification of the need for equipment: at this stage, the medical organization determines the equipment needs, and also formulates the requirements for this equipment.
- Market analysis: representatives of the medical organization conduct a market analysis to identify and select suitable equipment options, which meet the requirements mentioned at stage 1.
- Equipment selection: at this stage, a comparative analysis of the previously selected options is carried out and the most suitable option for a particular medical organization is selected, involving, however, several modifications of the equipment.
- Vendor selection: if the selected equipment can be purchased from several different suppliers, a comparative analysis of the terms of cooperation and further ranking and selection of the supplier is carried out. The supply contract with the selected supplier is carried out. Delivery logistics can be the subject of a separate contract.
- Purchase of equipment: payment procedures and documentary support of the purchase contract are carried out.
- Supply of equipment: at this stage, the purchased equipment is delivered in the proper form to the medical organization as part of a delivery contract or as part of a purchase contract.
- Installation and technical preparation of equipment: carrying out activities to prepare equipment for commissioning: preliminary preparation of the premises, installation of equipment, configuration, commissioning, etc.
- User training: training of personnel to work with new equipment.
- Commissioning of the equipment.
- Service equipment maintenance: activities for the maintenance of equipment throughout the entire period of its operation (repair, maintenance, software updates, etc.) [36].
- Disposal of equipment: equipment decommissioning and subsequent disposal.
- Modernization of equipment: an optional step that is applicable to certain types of HME.
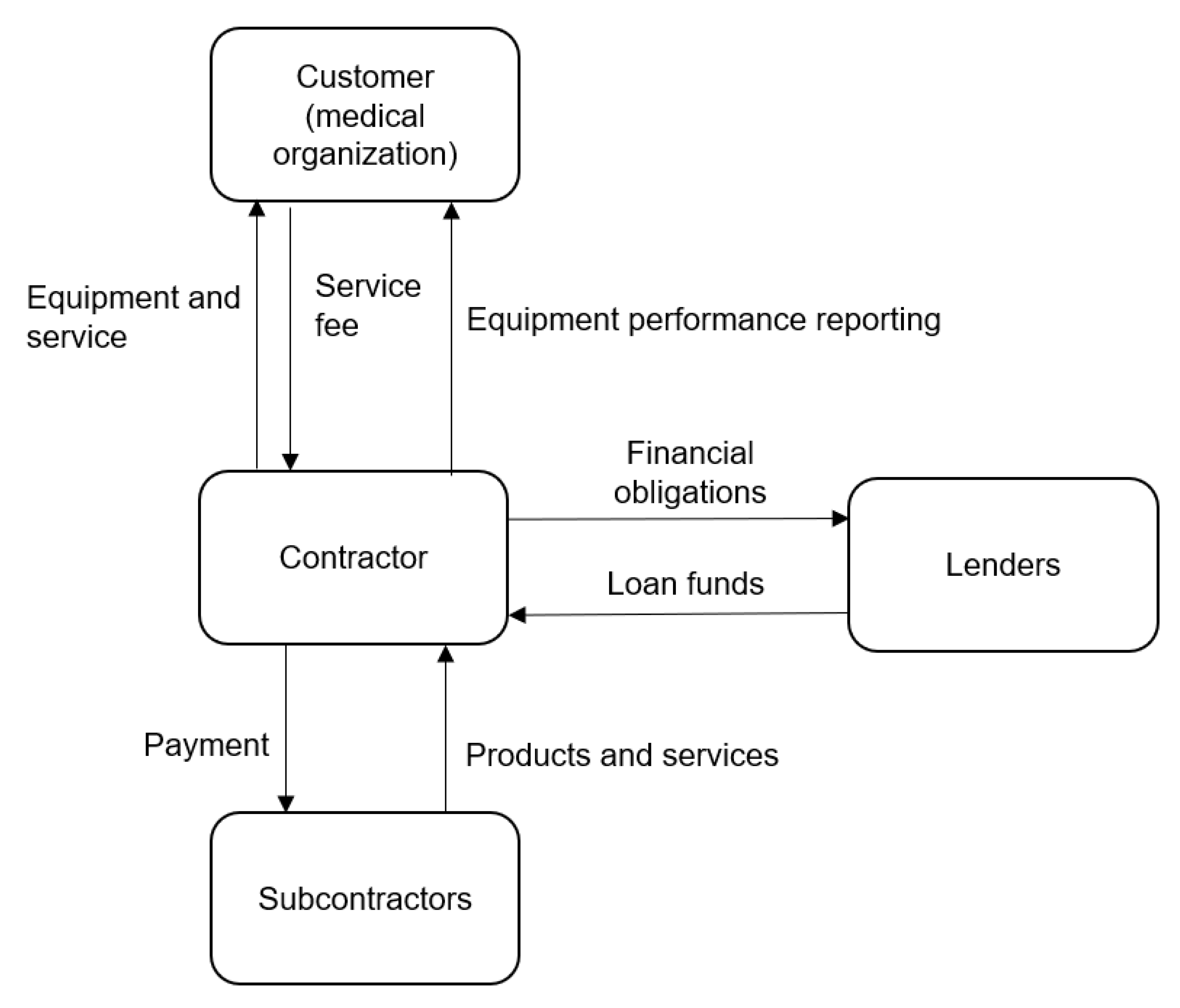
- Medical organization—acts as a customer who has a need for certain high-tech equipment.
- Equipment supplier—transfers the equipment to the ownership of the medical organization after the customer pays the contractual cost of the equipment.
- Transport organization—delivers equipment to the place of operation.
- An organization providing maintenance services for medical equipment—performs installation and commissioning.
- Responsible for personnel training—organizes training and certification of personnel on the basics and principles of the operation of new equipment and issues of correct functional operation of equipment.
- Service organization—ensuring the smooth operation of equipment as part of a set of maintenance and repair activities.
- Recycling company—disposes of equipment.
- Financial organizations—can be involved in the process to support a financial flow to finance the design, production, service, disposal and, possibly, modernization of equipment. A financial institution can be a bank that provides financial security in the form of a bank loan or the own treasury of participants in the creation of equipment if own funds are used for financing.
- State body—can act as an investor or a guarantor within certain obligations.
- In the case of leasing, the technical readiness of the equipment is not taken into account when accruing the operator’s debt: if the equipment breaks down, the customer still pays according to the payment schedule. In the case of the life cycle, payment is made for the time the equipment with operational properties is available.
- In the case of leasing, the operator independently decides on maintenance and repair issues. Yes, in this case there are many options for organizing this process, but they have little effect on the financial obligations of the operator to the leasing company. In the LCC option, the operator does not participate in any service agreements as a direct participant.
- In leasing, there are no strict technical transparency requirements for the operator: although he is obliged to comply with technical regulations, in case of disputes, technical expertise is the arbiter in disputes related to compliance with regulations. This exists also in cases of an LCC, but its conclusions are based on objective data obtained using communication tools: IoT, data obtained from an array of control parameters, recorded in a temporary storage and uploaded to the control system through controllers.
- In the case of leasing, the HME is not the property of the customer (operator): he only gets the right to use a share of the rights: the right to use, the right to income and the right to safety. In this sense, the end of the leasing agreement opens up for the HME operator the opportunity to buy the equipment at residual value, which is valuable if the evolution of the types of such equipment is conservative. In the case of the LCC, another bundle of property rights for the customer is relevant: the right to own, the right to use and the right to income (with restrictions). The right to perpetual possession and the right to inheritance arise only in the case of appropriate clauses in the LCC: the agreement may allow the transfer of equipment in favor of the counterparty providing HME disposal. Comparative analysis of an LCC and leasing is given in Table 2.
5. Discussion
- For simplicity, we consider that an LCC is concluded between the customer and a single contractor, who undertakes complex obligations to perform the operations stipulated by the CALS model: from the idea, through design to production, service and maintenance of the equipment delivered to the customer.
- A competitive or noncompetitive nature of the relationship between the parties is not essential for the purpose of this paper.
- The contractor has a right to make necessary design, technical, production, service, logistic decisions independently or to involve third parties for this purpose.
- The contract is concluded for the term, which is estimated on the basis of the contractor’s need to perform the actions, as stipulated by an LCC: production of the ordered equipment units, modernization and provision of service operations (including post-warranty period). Taking into account the fact that an LCC is expedient in the context of capital-intensive production, the life cycle of which consists of years, the LCC period is also long and extends for a period of 10 or more years.
- The long-term nature of an LCC entails the peculiarities of exit from the contract: as a rule, an LCC involves the possibility of replacing a partner without changing the essence of the participants’ obligations.
- The actual way of financing an LCC is the attraction of a financial institution within a consortium of participants of the LCC, providing financing of the measures provided by the model of creation and use of added value according to CALS: design, production, service and modernization (if applicable). The financial institution involved to create a cash flow to ensure the operational activities is not motivated to apply the mechanism of credit financing because by entering into a long-term relationship within the consortium, it provides itself a long financial contract, which provides it with an incoming cash flow, formed by the use for the intended purpose of the created value added. A simpler financing scheme can be applied when the contractor provides the implementation of this function independently (own funds, loans, etc.). The widespread scheme of return on investment is the periodic payment to the contractor (or the financial operator of the consortium) of the amount calculated according to a transparent rule, the key parameter of which is the availability of the equipment transferred to the customer with the agreed indicator of its technical readiness. In this regard, it is relevant to fix the communication aspect of operation, such as the use of IoT technologies to control the modes of operation of the equipment provided to the customer.
- The risks of an LCC are distributed between the customer and the contractor (contractors, if we are talking about a consortium of participants) and fall on the party that can best manage them. For example, the designer is responsible for design errors, the manufacturer for manufacturing defects, the service agent for maintenance and the customer for operation.
- –
- Analysis of how the concept of the life cycle can be applied to other health problems (for example, development and production of vaccines and vaccination of the population);
- –
- An important function of the LCC—financial—is not explicitly presented in Figure 5 as it is a subject of separate research. One of the important tasks in this area is the development of a system of mathematical models for financing HME LCC;
- –
- Aspects of the development of the LCC as a concept and supplementing it with innovative IT solutions, for example, ERP 4, is an actual area of research and is considered by the authors as a vector for future publications.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shlyakhto, E.; Ilin, I.; Iliashenko, O.; Karaptan, D.; Tick, A. Digital Platforms as a Key Factor of the Medical Organizations Activities Development. In Algorithms and Solutions Based on Computer Technology; Springer: Cham, Switzerland, 2022; pp. 327–343. [Google Scholar]
- Ilin, I.; Levina, A.; Iliashenko, V. Innovation Hub and Its IT Support: Architecture Model. In Digitalization of Society, Economics and Management; Springer: Cham, Switzerland, 2022; pp. 49–67. [Google Scholar]
- Ilin, I.; Levina, A.; Frolov, K. Innovative Ecosystem Model of Vaccine Lifecycle Management. J. Open Innov. Technol. Mark. Complex. 2022, 8, 5. [Google Scholar] [CrossRef]
- European Union. Directive 2014/24/EU of the European Parliament and of the Council. Official Journal of the European Union, 26 February 2014; pp. 65–242. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32014L0024 (accessed on 10 July 2022).
- European Union. Directive 2014/25/EU of the European Parliament and of the Council. Official Journal of the European Union, 26 February 2014; pp. 243–374. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32014L0025 (accessed on 10 July 2022).
- Yoon, S.; Jeong, S. Effects to Implement the Open-Innovation Coordinative Strategies between Manufacturer and Retailer in Reverse Supply Chain. J. Open Innov. Technol. Mark. Complex. 2017, 3, 2. [Google Scholar] [CrossRef]
- Grzyl, B.; Siemaszko, A. The Life Cycle Assessment and Life Cycle Cost in Public Works Contracts. In Proceedings of the 10th Conference on Interdisciplinary Problems in Environmental Protection and Engineering EKO-DOK 2018—E3S Web of Conferences, Polanica-Zdroj, Poland, 16–18 April 2018; Volume 44, p. 00047. [Google Scholar] [CrossRef]
- Russian Federation. Federal Law No. 44-FZ of 05.04.2013 “On the Contract System in the Field of Procurement of Goods, Works, Services to Meet State and Municipal Needs”. Rossiyskaya Gazeta, 11 April 2013. Available online: https://rg.ru/documents/2013/04/12/goszakupki-dok.html (accessed on 10 October 2022).
- Astafiev, A.V. Life Cycle Contract—A New Form of Public-Private Partnership for Organizing Regular Piggyback Traffic. In Ekonomika Zheleznykh Dorog; Prometei: Moscow, Russia, 2015; Volume 12, pp. 55–65. Available online: https://www.elibrary.ru/item.asp?id=24869616 (accessed on 10 July 2022).
- Zhao, J. Transaction Cost in PPPs Project: Exploration of Influence Factors for Both Public and Private Sectors in Different Countries with Whole Life Cycle. In IOP Conference Series: Earth and Environmental Science; IOP Publishing: Bristol, UK, 2019; Volume 242, p. 052043. [Google Scholar]
- Loomans, O. How a Projects’ Organization Stimulates Innovation in Public Private Infrastructure Development. Master’s Thesis, University of Groningen, Groningen, The Netherlands, 2018. [Google Scholar]
- da Costa, V.A.M.; Ribeiro, D.C. Alternatives for Airport Management in Brazil: The Case of the Innovative Management Model of the Zona da Mata Regional Airport. Innov. Manag. Rev. 2019, 16, 298–322. [Google Scholar] [CrossRef]
- Kostin, A.S. The Impact of the Life Cycle Contract on Reducing the Cost of Maintaining a Fleet of Passenger Locomotives. In Stoimost’ Sobstvennosti: Otsenka Upravleniye; Sinergy: Moscow, Russia, 2019; pp. 263–266. Available online: https://www.elibrary.ru/item.asp?id=44722070 (accessed on 10 July 2022).
- Gladilina, I.P.; Valentinovich, D.G.; Sergeeva, S.A. Life Cycle Contracts in the Development of Procurement in the Russian Federation: World Experience. Asian Soc. Sci. 2015, 11, 343–348. [Google Scholar] [CrossRef]
- Ushakov, D.V.; Maksimov, V.A.; Solntsev, A.A. Overview of the Application of the Bus Life Cycle Contract Model in the City of Moscow. In Problemy Tekhnicheskoy Ekspluatatsii I Avtoservisa Podvizhnogo Sostava Avtomobil’nogo Transporta; MADI: Moscow, Russia, 2020; pp. 64–67. Available online: https://www.elibrary.ru/item.asp?id=43066150 (accessed on 10 July 2022).
- Bessonov, I.V.; Lavrova, A.P. Life Cycle Contract as a Tool for Increasing Investment Security of SUE ‘Moscow Metro, In Vklad Transporta V Natsional’nuyu Ekonomicheskuyu Bezopasnost’; Russian University of Transport: Moscow, Russia, 2018; pp. 85–88. Available online: https://www.elibrary.ru/item.asp?id=37052729 (accessed on 10 July 2022).
- Yuen, B. Public-Private Partnership in Singapore Sports Hub. In Zur Ökonomik von Spitzenleistungen im Internationalen Sport, 3rd ed.; Büch, M.P., Maennig, W., Wolfgang Schulke, H.-J., Eds.; Hamburg University Press: Hanburg, Germany, 2012; pp. 207–229. Available online: https://hdl.handle.net/10419/61506 (accessed on 15 September 2022).
- Chirita, R. Financing Large Scale Public Projects—What Is New in the Romanian PPP Law. Rom. Pub.Priv. Partnersh. L. Rev. 2013, 7, 43. [Google Scholar]
- Zibaoui, A. Mediterranean Logistics Post-COVID-19: Opportunities Come with Challenges. In Mediterranean Transport and Logistics in a Post-COVID-19 Era: Prospects and Opportunities; Apprioual, A., Ibáñez, M., Palacios, A., Pons, A., Eds.; IEMed: Barcelona, Spain, 2021. [Google Scholar]
- González, M.; Bianchi, C.P.R.; Rius, A.P.R.; Pittagula, L. Public-Private Collaboration on Productive Development in Uruguay. IDB Publ. Work. Pap. 2014, 1–60, IDB-WP-501. [Google Scholar]
- Electric Buses and Medical Equipment: 52 Life Cycle Contracts Signed in 2021. In Official Website of the Mayor of Moscow; 2022. Available online: https://www.mos.ru/news/item/102749073/ (accessed on 10 July 2022).
- Rakuta, N.V. The Use of Life Cycle Contracts in Public Procurement. Experience of Developed Countries. Issues State Munic. Adm. 2015, 2, 53–78. [Google Scholar]
- Koppenjan, J.; Klijn, E.-H.; Verweij, S.; Duijn, M.; van Meerkerk, I.; Metselaar, S.; Warsen, R. The Performance of Public–Private Partnerships: An Evaluation of 15 Years DBFM in Dutch Infrastructure Governance. Public Perform. Manag. Rev. 2022, 45, 998–1028. [Google Scholar] [CrossRef]
- Rekenkamer, A. Contract Management of DBFMO Projects; The Netherlands Court of Audit: The Hague, The Netherlands, 2013; Available online: https://english.rekenkamer.nl/publications/reports/2013/06/06/contract-management-of-dbfmo-projects (accessed on 10 July 2022).
- Wijnker, L. Design, Build, Finance and Maintain: Public Private Partnership in the Beatrixsluis Project in the Netherlands. In Hydraulik der Wasserbauwerke—Neues aus Praxis und Forschung; Bundesanstalt für Wasserbau: Karlsruhe, Germany, 2019; pp. 7–14. Available online: https://hdl.handle.net/20.500.11970/106408 (accessed on 15 September 2022).
- Hoppe, E.I.; Kusterer, D.J.; Schmitz, P.W. Public-Private Partnerships versus Traditional Procurement: An Experimental Investigation. J. Econ. Behav. Organ. 2011, 89, 145–166. [Google Scholar] [CrossRef]
- Atmo, G.U.; Duffield, C.; Zhang, L.; Wilson, D.I. Comparative Performance of PPPs and Traditional Procurement Projects in Indonesia. Int. J. Public Sect. Manag. 2017, 30, 118–136. [Google Scholar] [CrossRef]
- Hong, S. When Does a Public-Private Partnership (PPP) Lead to Inefficient Cost Management? Evidence from the Korean Urban Rail Transit System. Public Money Manag. 2015, 36, 447–454. [Google Scholar] [CrossRef]
- Baronin, S.A.; Yankov, A.G. Life Cycle Contracts: Conceptual Analysis, Foreign Experience and Prospects for Development in Russia. In Modern Problems of Science and Education; Akademia Estestvoznania: Moscow, Russia, 2013; p. 520. Available online: https://www.elibrary.ru/item.asp?id=21162955 (accessed on 10 July 2022).
- Sokolov, Y.I. Life Cycle Contract and Investment Risks. Transp. Russ. Federation. J. Sci. Pract. Econ. 2011, 2, 32–34. [Google Scholar]
- Nikitin, Y.A.; Vasiliev, N.I.; Detkov, G.B. Features of the Life Cycle Contract. Theory Pract. Serv. Econ. Soc. Sphere Technol. 2019, 2, 33–40. [Google Scholar]
- Hutiz, Z.M. Life Cycle Contract as a Form of Public-Private Partnership. Bull. Acad. Knowl. 2017, 23, 196–199. [Google Scholar]
- O’Shea, C.; Palcic, D.; Reeves, E. Comparing PPP with Traditional Procurement: The Case of Schools Procurement in Ireland. Ann. Public Coop. Econ. 2018, 90, 245–267. [Google Scholar] [CrossRef]
- Verweij, S.; van Meerkerk, I. Do Public–Private Partnerships Achieve Better Time and Cost Performance than Regular Contracts? Public Money Manag. 2021, 41, 286–295. [Google Scholar] [CrossRef]
- Ilin, I.; Iliashenko, V.M.; Dubgorn, A.; Esser, M. Critical Factors and Challenges of Healthcare Digital Transformation. In Digital Transformation and the World Economy; Springer: Berlin/Heidelberg, Germany, 2022; pp. 205–220. [Google Scholar]
- Udroiu, G. Efficient Strategies in Medical Equipment Management. Bull. Carol I Natl. Def. Univ. 2020, 9, 36–42. [Google Scholar] [CrossRef]
- Aslesen, H.W.; Freel, M. Industrial Knowledge Bases as Drivers of Open Innovation? Ind. Innov. 2012, 19, 563–584. [Google Scholar] [CrossRef]
- Virlée, J.; Hammedi, W.; Parida, V. Open Innovation Implementation in the Service Industry: Exploring Practices, Sub-Practices and Contextual. J. Innov. Manag. 2015, 3, 106–130. [Google Scholar] [CrossRef]
- Sarkar, S.; Costa, A.I. Dynamics of Open Innovation in the Food Industry. Trends Food Sci. Technol. 2008, 19, 574–580. [Google Scholar] [CrossRef]
- Yu, J.J.; Won, D.; Park, K. Entrepreneurial Cyclical Dynamics of Open Innovation. J. Evol. Econ. 2018, 28, 1151–1174. [Google Scholar] [CrossRef]
- Bullinger, A.C.; Rass, M.; Adamczyk, S.; Moeslein, K.M.; Sohn, S. Open Innovation in Health Care: Analysis of an Open Health Platform. Health Policy 2012, 105, 165–175. [Google Scholar] [CrossRef]
- Wass, S.; Vimarlund, V. Healthcare in the Age of Open Innovation—A Literature Review. Health Inf. Manag. J. 2016, 45, 121–133. [Google Scholar] [CrossRef]
- Orlando, B.; Ballestra, L.V.; Magni, D.; Ciampi, F. Open Innovation and Patenting Activity in Health Care. J. Intellect. Cap. 2020, 22, 384–402. [Google Scholar] [CrossRef]
- Bullinger, A.; Rass, M.; Moeslein, K. Towards Open Innovation in Health Care. In Proceedings of the European Conference on Information Systems, Barcelona, Spain, 10–13 June 2012; pp. 5–15. [Google Scholar] [CrossRef]
- Kankanhalli, A.; Zuiderwijk, A.; Tayi, G.K. Open Innovation in the Public Sector: A Research Agenda. Gov. Inf. Q. 2017, 34, 84–89. [Google Scholar] [CrossRef]
- Dandonoli, P. Open Innovation as a New Paradigm for Global Collaborations in Health. Glob. Health 2013, 9, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Melese, T.; Lin, S.M.; Chang, J.L.; Cohen, N.H. Open Innovation Networks between Academia and Industry: An Imperative for Breakthrough Therapies. Nat. Med. 2009, 15, 502–507. [Google Scholar] [CrossRef]
- Wassrin, S.; Lindgren, I.; Melin, U. Open Innovation Contests for Improving Healthcare—An Explorative Case Study Focusing on Challenges in a Testbed Initiative. In International Conference on Electronic Government; Springer: Cham, Switzerland, 2015; pp. 91–104. [Google Scholar] [CrossRef]
- Wan, H.H.; Quan, X.I. Toward a Framework of the Process of Open Innovation—Case of Acclarent in the Medical Device Industry. Int. J. Innov. Technol. Manag. 2014, 11, 1450032. [Google Scholar] [CrossRef]
- Fuglsang, L. Capturing the Benefits of Open Innovation in Public Innovation: A Case Study. Int. J. Serv. Technol. Manag. 2008, 9, 234–248. [Google Scholar] [CrossRef]
- Gabriel, M.; Stanley, I.; Saunders, T. Open Innovation in Health. A Guide to Transforming Healthcare through Collaboration; Nesta: London, UK, 2017. [Google Scholar]
- Thakur, R.; Hsu, S.H.; Fontenot, G. Innovation in Healthcare: Issues and Future Trends. J. Bus. Res. 2012, 65, 562–569. [Google Scholar] [CrossRef]
- Yang, J.; Chesbrough, H.; Hurmelinna-Laukkanen, P. How to Appropriate Value from General-Purpose Technology by Applying Open Innovation. Calif. Manag. Rev. 2022, 64, 24–48. [Google Scholar] [CrossRef]
- Urbinati, A.; Chiaroni, D.; Chiesa, V.; Frattini, F. The Role of Digital Technologies in Open Innovation Processes: An Exploratory Multiple Case Study Analysis. RD Manag. 2020, 50, 136–160. [Google Scholar] [CrossRef]
- Mu, R.; Wang, H. A Systematic Literature Review of Open Innovation in the Public Sector: Comparing Barriers and Governance Strategies of Digital and Non-Digital Open Innovation. Public Manag. Rev. 2022, 24, 489–511. [Google Scholar] [CrossRef]
- Pedersen, K. What Can Open Innovation Be Used for and How Does It Create Value? Gov. Inf. Q. 2020, 37, 101459. [Google Scholar] [CrossRef]
- Mubarak, M.F.; Petraite, M. Industry 4.0 Technologies, Digital Trust and Technological Orientation: What Matters in Open Innovation? Technol. Forecast. Soc. Chang. 2020, 161, 120332. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Source Number |
|---|---|
| Transport | [9,10,11,12,13,14,15,16] |
| Construction of sports facilities | [17] |
| Medicine | [18,19,20,21] |
| Parameter | LCC | Leasing |
|---|---|---|
| Prepaid expense | From a financial institution/from own funds, and not from the customer | From 10% |
| Ownership | According to share of rights of LCC | According to the share of rights of leasing. Possibility of redemption (including ahead of schedule) |
| Contract term | By the duration of the life cycle of equipment (from 5 to 30 years) | Usually up to 8 years |
| Contracts for equipment service, purchase of spare parts/consumables | Included in one contract, are the responsibility of the contractor | Individual contracts and purchases |
| Organizations providing maintenance and repair services | Service member of the consortium | At the choice of the operator (possibly subject to the recommendation of the lessor) |
| Price, tariff, tax, inflationary, currency risks | Compensation by state jurisdictions (guarantees, subsidies, direct compensation, etc.), insurance indemnities in terms of certain risks | Insurance indemnities in terms of risks considered as force majeure (limited) |
| Maintenance and repair fee | According to a complex formula when confirming a violation of the rules of operation | Fixed under the contract (is agreed with the lessor) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilin, I.; Levina, A.; Frolov, K.; Borremans, A.; Ershova, A.; Tick, A.; Averina, M. Life-Cycle Contract as an Innovative Business Model for High-Tech Medical Organizations. J. Open Innov. Technol. Mark. Complex. 2022, 8, 207. https://doi.org/10.3390/joitmc8040207
Ilin I, Levina A, Frolov K, Borremans A, Ershova A, Tick A, Averina M. Life-Cycle Contract as an Innovative Business Model for High-Tech Medical Organizations. Journal of Open Innovation: Technology, Market, and Complexity. 2022; 8(4):207. https://doi.org/10.3390/joitmc8040207
Chicago/Turabian StyleIlin, Igor, Anastasia Levina, Konstantin Frolov, Alexandra Borremans, Alyona Ershova, Andrea Tick, and Mariia Averina. 2022. "Life-Cycle Contract as an Innovative Business Model for High-Tech Medical Organizations" Journal of Open Innovation: Technology, Market, and Complexity 8, no. 4: 207. https://doi.org/10.3390/joitmc8040207
APA StyleIlin, I., Levina, A., Frolov, K., Borremans, A., Ershova, A., Tick, A., & Averina, M. (2022). Life-Cycle Contract as an Innovative Business Model for High-Tech Medical Organizations. Journal of Open Innovation: Technology, Market, and Complexity, 8(4), 207. https://doi.org/10.3390/joitmc8040207