
Efficacy of Urine Dipstick Test in Diagnosing Urinary Tract Infection and Detection of the blaCTX-M Gene among ESBL-Producing Escherichia coli

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample Collection, Processing and Identification
2.3. Antimicrobial Susceptibility Testing
2.4. Phenotypic Confirmation of ESBL Producers
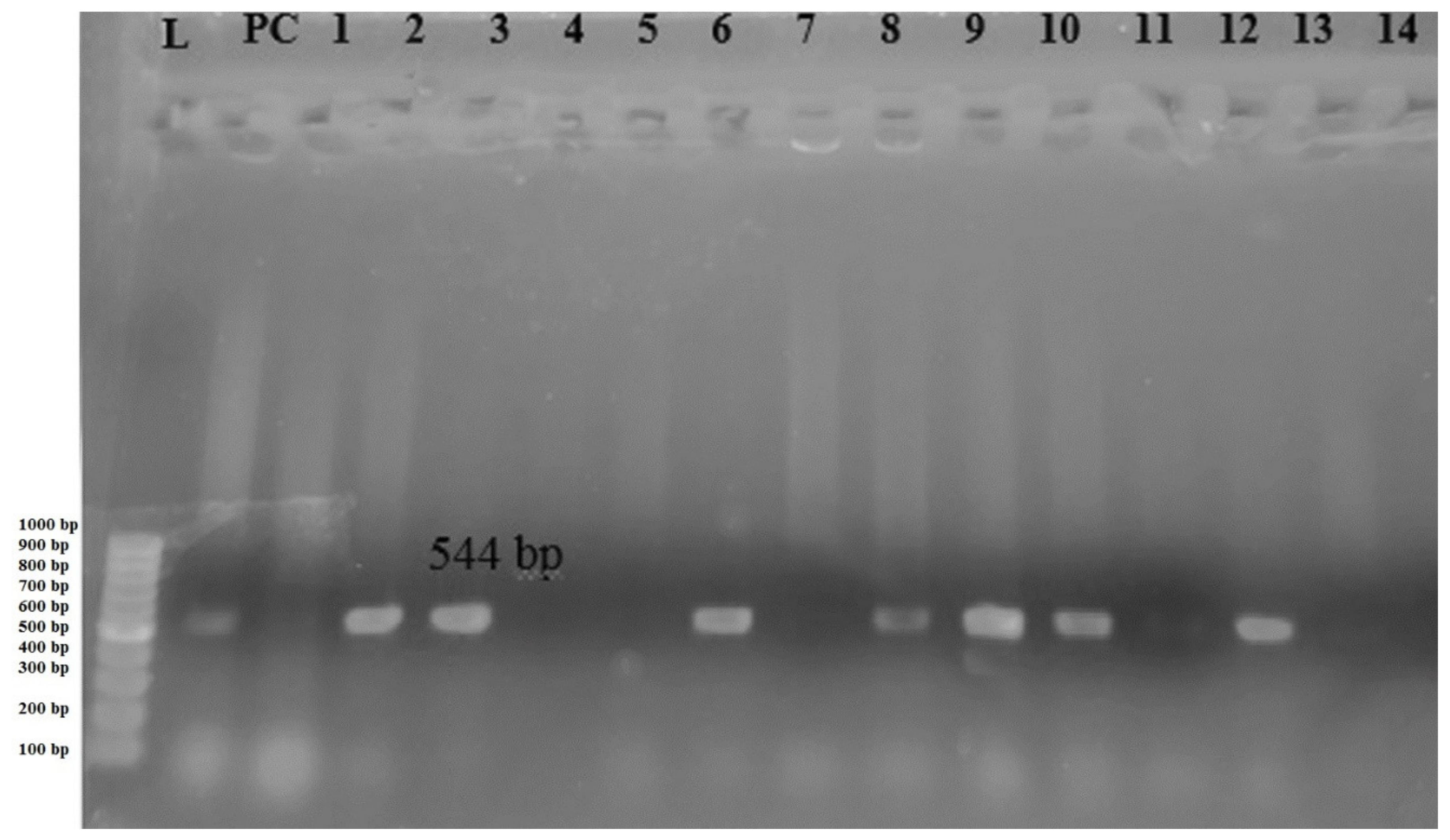
2.5. DNA Extraction and Amplification of blaCTX-M Gene by PCR
2.6. Quality Control
2.7. Data Analysis
3. Results
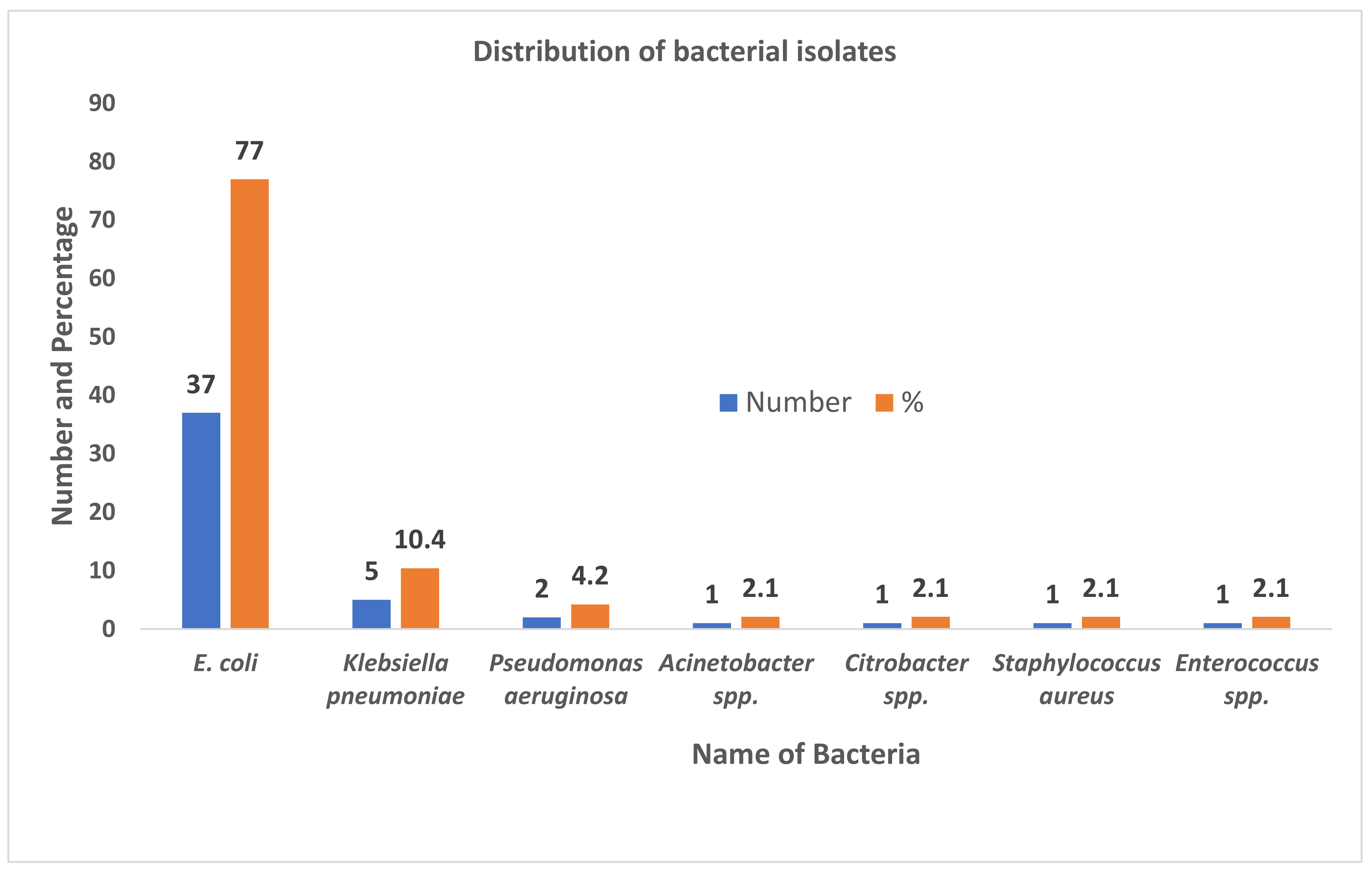
3.1. Distribution of Isolates
3.2. Sensitivity, Specificity, Positive Predictive Value and Negative Predictive Value for Urinary Dipstick Test
3.3. Association of UTI with Various Attributes
3.4. Antibiotic Susceptibility Pattern of Escherichia coli
3.5. Prevalence of ESBL Positive E. coli and blaCTX-M Gene
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Foxman, B.; Barlow, R.; D’Arcy, H.; Gillespie, B.; Sobel, J.D. Urinary tract infection: Self-reported incidence and associated costs. Ann. Epidemiol. 2000, 10, 509–515. [Google Scholar] [CrossRef]
- Forsyth, V.S.; Armbruster, C.E.; Smith, S.N.; Pirani, A.; Springman, A.C.; Walters, M.S.; Nielubowicz, G.R.; Himpsl, S.D.; Snitkin, E.S.; Mobley, H.L. Rapid growth of uropathogenic Escherichia coli during human urinary tract infection. mBio 2018, 9, e00186-18. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.; Khadka, S.; Sapkota, S.; Rana, J.C.; Khanal, S.; Neupane, A.; Sharma, B. Prevalence and Antibiograms of Uropathogens from the Suspected Cases of Urinary Tract Infections in Bharatpur Hospital, Nepal. J. Coll. Med Sci. 2019, 15, 260–266. [Google Scholar] [CrossRef]
- Shrestha, G.; Wei, X.; Hann, K.; Soe, K.T.; Satyanarayana, S.; Siwakoti, B.; Bastakoti, S.; Mulmi, R.; Rana, K.; Lamichhane, N. Bacterial Profile and Antibiotic Resistance among Cancer Patients with Urinary Tract Infection in a National Tertiary Cancer Hospital of Nepal. Trop. Med. Infect. Dis. 2021, 6, 49. [Google Scholar] [CrossRef]
- Upadhyaya, G.; Bhattarai, A.; Rijal, K.R.; Ghimire, P.; Upadhyaya, B. Urinary tract infections in Kidney transplant patients of Kathmandu Valley. Int. J. Microbiol. Res. Rev. 2013, 3, 1–6. [Google Scholar]
- Christenson, R.; Tucker, J.A.; Allen, E. Results of dipstick tests, visual inspection, microscopic examination of urine sediment, and microbiological cultures of urine compared for simplifying urinalysis. Clin. Chem. 1985, 31, 448–451. [Google Scholar] [CrossRef]
- Vuljanić, D.; Dojder, A.; Špoljarić, V.; Saračević, A.; Dukić, L.; Leniček Krleža, J.; Vlašić Tanasković, J.; Maradin, I.; Grzunov, A.; Vogrinc, Ž. Analytical verification of 12 most commonly used urine dipsticks in Croatia: Comparability, repeatability and accuracy. Biochem. Med. 2019, 29, 123–132. [Google Scholar] [CrossRef]
- Liou, L.S.; Shi, T.; Duan, Z.-H.; Sadhukhan, P.; Der, S.D.; Novick, A.A.; Hissong, J.; Skacel, M.; Almasan, A.; Di Donato, J.A. Microarray gene expression profiling and analysis in renal cell carcinoma. BMC Urol. 2004, 4, 1–11. [Google Scholar] [CrossRef]
- Whiting, P.; Westwood, M.; Watt, I.; Cooper, J.; Kleijnen, J. Rapid tests and urine sampling techniques for the diagnosis of urinary tract infection (UTI) in children under five years: A systematic review. BMC Pediatr. 2005, 5, 1–13. [Google Scholar] [CrossRef]
- Demilie, T.; Beyene, G.; Melaku, S.; Tsegaye, W. Diagnostic accuracy of rapid urine dipstick test to predict urinary tract infection among pregnant women in Felege Hiwot Referral Hospital, Bahir Dar, North West Ethiopia. BMC Res. Notes 2014, 7, 1–5. [Google Scholar] [CrossRef]
- Ding, Y.; Wang, Y.; Hsia, Y.; Sharland, M.; Heath, P.T. Systematic review of carbapenem-resistant Enterobacteriaceae causing neonatal sepsis in China. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 1–8. [Google Scholar] [CrossRef]
- Li, Y.; Li, Q.; Du, Y.; Jiang, X.; Tang, J.; Wang, J.; Li, G.; Jiang, Y. Prevalence of plasmid-mediated AmpC β-lactamases in a Chinese university hospital from 2003 to 2005: First report of CMY-2-type AmpC β-lactamase resistance in China. J. Clin. Microbiol. 2008, 46, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Poole, K. Resistance to β-lactam antibiotics. Cell. Mol. Life Sci. 2004, 61, 2200–2223. [Google Scholar] [CrossRef] [PubMed]
- Ojdana, D.; Sacha, P.; Wieczorek, P.; Czaban, S.; Michalska, A.; Jaworowska, J.; Jurczak, A.; Poniatowski, B.; Tryniszewska, E. The occurrence of blaCTX-M, blaSHV, and blaTEM genes in extended-Spectrum β-lactamase-positive strains of Klebsiella pneumoniae, Escherichia coli, and Proteus mirabilis in Poland. Int. J. Antibiot. 2014, 2014, 935842. [Google Scholar] [CrossRef]
- Mokracka, J.; Oszyńska, A.; Kaznowski, A. Increased frequency of integrons and β-lactamase-coding genes among extraintestinal Escherichia coli isolated with a 7-year interval. Antonie Leeuwenhoek 2013, 103, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Tran, F.; Boedicker, J.Q. Plasmid characteristics modulate the propensity of gene exchange in bacterial vesicles. J. Bacteriol. 2019, 201, e00430-18. [Google Scholar] [CrossRef] [PubMed]
- Hawkey, P.M.; Jones, A.M. The changing epidemiology of resistance. J. Antimicrob. Chemother. 2009, 64, i3–i10. [Google Scholar] [CrossRef]
- Rijal, K.R.; Banjara, M.R.; Dhungel, B.; Kafle, S.; Gautam, K.; Ghimire, B.; Ghimire, P.; Dhungel, S.; Adhikari, N.; Shrestha, U.T.; et al. Use of antimicrobials and antimicrobial resistance in Nepal: A nationwide survey. Sci. Rep. 2021, 11, 11554. [Google Scholar] [CrossRef] [PubMed]
- Kayastha, K.; Dhungel, B.; Karki, S.; Adhikari, B.; Banjara, M.R.; Rijal, K.R.; Ghimire, P. Extended-Spectrum beta-Lactamase-Producing Escherichia coli and Klebsiella Species in Pediatric Patients Visiting International Friendship Children’s Hospital, Kathmandu, Nepal. Infect. Dis. 2020, 13, 1178633720909798. [Google Scholar] [CrossRef]
- Raut, S.; Rijal, K.R.; Khatiwada, S.; Karna, S.; Khanal, R.; Adhikari, J.; Adhikari, B. Trend and Characteristics of Acinetobacter baumannii Infections in Patients Attending Universal College of Medical Sciences, Bhairahawa, Western Nepal: A Longitudinal Study of 2018. Infect. Drug Resist. 2020, 13, 1631–1641. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.S.P.; Dhungel, B.; Yadav, B.K.; Adhikari, N.; Thapa Shrestha, U.; Lekhak, B.; Banjara, M.R.; Adhikari, B.; Ghimire, P.; Rijal, K.R. Detection of TEM and CTX-M Genes in Escherichia coli Isolated from Clinical Specimens at Tertiary Care Heart Hospital, Kathmandu, Nepal. Diseases 2021, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Forbes, B.A.; Sahm, D.F.; Weissfeld, A.S. Diagnostic Microbiology; Mosby: St. Louis, MO, USA, 2007. [Google Scholar]
- Magiorakos, A.-P.; Srinivasan, A.; Carey Rt Carmeli, Y.; Falagas Mt Giske Ct Harbarth, S.; Hindler Jt Kahlmeter, G.; Olsson-Liljequist, B. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Sambrook, J.; Fritsch, E.F.; Maniatis, T. Molecular Cloning: A Laboratory Manual; Cold Spring Harbor Laboratory Press: New York, NY, USA, 1989. [Google Scholar]
- Edelstein, M.; Pimkin, M.; Palagin, I.; Edelstein, I.; Stratchounski, L. Prevalence and molecular epidemiology of CTX-M extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae in Russian hospitals. Antimicrob. Agents Chemother. 2003, 47, 3724–3732. [Google Scholar] [CrossRef]
- Muktan, B.; Shrestha, U.T.; Dhungel, B.; Mishra, B.C.; Shrestha, N.; Adhikari, N.; Banjara, M.R.; Adhikari, B.; Rijal, K.R.; Ghimire, P. Plasmid mediated colistin resistant mcr-1 and co-existence of OXA-48 among Escherichia coli from clinical and poultry isolates: First report from Nepal. Gut Pathog. 2020, 12, 1–9. [Google Scholar] [CrossRef]
- Garrido, D.; Garrido, S.; Gutiérrez, M.; Calvopiña, L.; Harrison, A.S.; Fuseau, M.; Irigoyen, R.S. Clinical characterization and antimicrobial resistance of Escherichia coli in pediatric patients with urinary tract infection at a third level hospital of Quito, Ecuador. Bol. Med. Hosp. Infant. Mex. 2017, 74, 265–271. [Google Scholar] [CrossRef]
- Guragain, N.; Pradhan, A.; Dhungel, B.; Banjara, M.R.; Rijal, K.R.; Ghimire, P. Extended spectrum β-lactamase producing Gram negative bacterial isolates from urine of patients visiting Everest Hospital, Kathmandu, Nepal. Tribhuvan Uni. J. Microbiol. 2019, 6, 26–31. [Google Scholar] [CrossRef]
- Thakur, P.; Ghimire, P.; Rijal, K.R.; Singh, G.K. Antimicrobial resistance pattern of Escherichia coli isolated from urine samples in patients visiting tertiary health care centre in eastern Nepal. Sunsari Tech. Coll. J. 2012, 1, 22–26. [Google Scholar] [CrossRef]
- Aryal, S.C.; Upreti, M.K.; Sah, A.K.; Ansari, M.; Nepal, K.; Dhungel, B.; Adhikari, N.; Lekhak, B.; Rijal, K.R. Plasmid-Mediated AmpC beta-Lactamase CITM and DHAM Genes Among Gram-Negative Clinical Isolates. Infect. Drug Resist. 2020, 13, 4249–4261. [Google Scholar] [CrossRef]
- Odongo, I.; Ssemambo, R.; Kungu, J.M. Prevalence of Escherichia Coli and its antimicrobial susceptibility profiles among patients with UTI at Mulago Hospital, Kampala, Uganda. Interdiscip. Perspect. Infect. Dis. 2020, 2020, 8042540. [Google Scholar] [CrossRef]
- Gurung, S.; Kafle, S.; Dhungel, B.; Adhikari, N.; Thapa Shrestha, U.; Adhikari, B.; Banjara, M.R.; Rijal, K.R.; Ghimire, P. Detection of OXA-48 Gene in Carbapenem-Resistant Escherichia coli and Klebsiella pneumoniae from Urine Samples. Infect. Drug Resist. 2020, 13, 2311–2321. [Google Scholar] [CrossRef] [PubMed]
- Mobley, H.L.; Jarvis, K.G.; Elwood, J.P.; Whittle, D.I.; Lockatell, C.V.; Russell, R.G.; Johnson, D.E.; Donnenberg, M.S.; Warren, J.W. Isogenic P-fimbrial deletion mutants of pyelonephritogenic Escherichia coli: The role of α Gal (1–4) β Gal binding in virulence of a wild-type strain. Mol. Microbiol. 1993, 10, 143–155. [Google Scholar] [CrossRef]
- Marques, A.G.; Pasternak, J.; Damascena, M.D.S.; França, C.N.; Martino, M.D.V. Performance of the dipstick screening test as a predictor of negative urine culture. Einstein 2017, 15, 34–39. [Google Scholar] [CrossRef]
- Bellazreg, F.; Abid, M.; Lasfar, N.B.; Hattab, Z.; Hachfi, W.; Letaief, A. Diagnostic value of dipstick test in adult symptomatic urinary tract infections: Results of a cross-sectional Tunisian study. Pan Afr. Med. J. 2019, 33, 131. [Google Scholar] [CrossRef]
- Awasthi, T.R.; Pant, N.D.; Dahal, P.R. Prevalence of multidrug resistant bacteria in causing community acquired urinary tract infection among the patients attending outpatient Department of Seti Zonal Hospital, Dhangadi, Nepal. Nepal J. Biotechnol. 2015, 3, 55–59. [Google Scholar] [CrossRef][Green Version]
- Yadav, K.; Prakash, S. Screening of ESBL producing multidrug resistant E. coli from urinary tract infection suspected cases in southern Terai of Nepal. J. Infect. Dis. Diagn. 2017, 2, 116. [Google Scholar] [CrossRef]
- Zubair, K.U.; Shah, A.H.; Fawwad, A.; Sabir, R.; Butt, A. Frequency of urinary tract infection and antibiotic sensitivity of uropathogens in patients with diabetes. Pak. J. Med. Sci. 2019, 35, 1664. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, R.; Shrestha, D.; Bhattachan, B.; Rai, G. Epidemiology of urinary tract infection and antimicrobial resistance in a pediatric hospital in Nepal. BMC Infect. Dis. 2019, 19, 1–5. [Google Scholar] [CrossRef]
- Sedhain, A.; Sapkota, A.; Shrestha, B. Antibiotic sensitivity pattern in urinary tract infection among adults in central part of Nepal. J. Chitwan Med. Coll. 2019, 9, 18–23. [Google Scholar] [CrossRef][Green Version]
- Storme, O.; Tiran Saucedo, J.; Garcia-Mora, A.; Dehesa-Davila, M.; Naber, K.G. Risk factors and predisposing conditions for urinary tract infection. Adv. Urol. 2019, 11, 1756287218814382. [Google Scholar] [CrossRef]
- Laupland, K.; Ross, T.; Pitout, J.; Church, D.; Gregson, D. Community-onset urinary tract infections: A population-based assessment. Infection 2007, 35, 150–153. [Google Scholar] [CrossRef]
- Sharma, M.; Pathak, S.; Srivastava, P. Prevalence and antibiogram of Extended Spectrum β-Lactamase (ESBL) producing Gram negative bacilli and further molecular characterization of ESBL producing Escherichia coli and Klebsiella spp. J. Clin. Diagn. Res. 2013, 7, 2173. [Google Scholar] [CrossRef]
- Nerurkar, A.; Solanky, P.; Naik, S.S. Bacterial pathogens in urinary tract infection and antibiotic susceptibility pattern. J. Pharm. Biomed. Sci. 2012, 21, 1–3. [Google Scholar]
- Bitew, A.; Molalign, T.; Chanie, M. Species distribution and antibiotic susceptibility profile of bacterial uropathogens among patients complaining urinary tract infections. BMC Infect. Dis. 2017, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pandit, R.; Awal, B.; Shrestha, S.S.; Joshi, G.; Rijal, B.P.; Parajuli, N.P. Extended-spectrum β-lactamase (ESBL) genotypes among multidrug-resistant uropathogenic Escherichia coli clinical isolates from a teaching hospital of Nepal. Interdiscip. Perspect. Infect. Dis. 2020, 2020, 6525826. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, C.; Rafi, M.A.; Salam, M.A. High prevalence of multidrug resistant uropathogens: A recent audit of antimicrobial susceptibility testing from a tertiary care hospital in Bangladesh. Pak. J. Med. Sci. 2020, 36, 1297. [Google Scholar] [CrossRef] [PubMed]
- Zaman, S.B.; Hussain, M.A.; Nye, R.; Mehta, V.; Mamun, K.T.; Hossain, N. A Review on Antibiotic Resistance: Alarm Bells are Ringing. Cureus 2017, 9, e1403. [Google Scholar] [CrossRef] [PubMed]
- Ugbo, E.; Anyamene, C.; Moses, I.; Ariom, T.; Agumah, N.; Chukwunwejim, C.; Egbule, C.; Emioye, A.; Okata-Nwali, O.; Aneke, C. Isolation and molecular characteristics of extended spectrum beta-lactamase-producing uropathogenic Escherichia coli isolated from hospital attendees in Ebonyi State, Abakaliki. Afr. J. Biotechnol. 2020, 19, 829–835. [Google Scholar] [CrossRef]
- Jabalameli, L.; Beigverdi, R.; Ranjbar, H.H.; Pouriran, R.; Jabalameli, F.; Emaneini, M. Phenotypic and genotypic prevalence of extended-spectrum β-Lactamase-Producing Escherichia coli: A systematic review and meta-analysis in Iran. Microb. Drug Resist. 2021, 27, 73–86. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gene | Primer (5′-3′) | Amplicon Size (bp) | Reference |
|---|---|---|---|
| CTX-M | F: 5′-TTTGCGATGTGCAGTACCAGTAA-3′ | 544 | [26] |
| R: 5′-CGATATCGTTGGTGGTGCCATA-3′ |
| Culture | ||||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| Dipstick test | Positive | 21 | 38 | 59 |
| Negative | 27 | 131 | 158 | |
| Total | 48 | 169 | 217 | |
| Attributes | Sample Size | UTI Infection n (%) | p-Value | |
|---|---|---|---|---|
| Gender | Male | 61 | 9 (14.75) | 0.103 |
| Female | 156 | 39 (25.00) | ||
| Age-group | 1–19 | 37 | 9 (24.32) | 0.019 * |
| 20–39 | 103 | 24 (23.30) | ||
| 40–59 | 50 | 8 (16.00) | ||
| 60–79 | 24 | 7 (29.17) | ||
| >80 | 3 | 0 | ||
| Department | In-patients | 79 | 11 (13.92) | 0.028 * |
| Out-patients | 138 | 37 (26.81) | ||
| Antibiotics Used | Susceptibility Pattern | ||
|---|---|---|---|
| Sensitive n (%) | Intermediate n (%) | Resistant n (%) | |
| Amikacin | 30 (81.08) | 0 | 7 (18.92) |
| Amoxyclav | 17 (45.95) | 1 (2.70) | 19 (51.35) |
| Ciprofloxacin | 16 (43.24) | 1 (2.70) | 20 (54.05) |
| Cotrimoxazole | 17 (45.95) | 0 | 20 (54.05) |
| Gentamicin | 23 (62.16) | 2 (5.40) | 12 (32.43) |
| Cefixime | 15 (40.54) | 0 | 22 (59.46) |
| Nitrofurantoin | 26 (70.27) | 1 (2.70) | 10 (27.03) |
| Cefazolin | 13 (35.14) | 1 (2.70) | 23 (62.16) |
| Ceftriaxone | 20 (54.05) | 0 | 17 (45.95) |
| Cefotaxime | 20 (54.05) | 0 | 17 (45.95) |
| Ceftazidime | 18 (48.65) | 0 | 19 (51.35) |
| Nalidixic acid | 13 (35.14) | 2 (5.40) | 22 (59.46) |
| Piperacillin/Tazobactam | 23 (62.16) | 0 | 14 (37.84) |
| Organism | Total Isolates | ESBL Producers | ||
|---|---|---|---|---|
| Presumptive n (%) | Confirmatory n (%) | blaCTX-M Gene n (%) | ||
| E. coli | 37 | 19 (51.35) | 14 (37.84) | 8 (21.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gurung, R.; Adhikari, S.; Adhikari, N.; Sapkota, S.; Rana, J.C.; Dhungel, B.; Thapa Shrestha, U.; Banjara, M.R.; Ghimire, P.; Rijal, K.R. Efficacy of Urine Dipstick Test in Diagnosing Urinary Tract Infection and Detection of the blaCTX-M Gene among ESBL-Producing Escherichia coli. Diseases 2021, 9, 59. https://doi.org/10.3390/diseases9030059
Gurung R, Adhikari S, Adhikari N, Sapkota S, Rana JC, Dhungel B, Thapa Shrestha U, Banjara MR, Ghimire P, Rijal KR. Efficacy of Urine Dipstick Test in Diagnosing Urinary Tract Infection and Detection of the blaCTX-M Gene among ESBL-Producing Escherichia coli. Diseases. 2021; 9(3):59. https://doi.org/10.3390/diseases9030059
Chicago/Turabian StyleGurung, Rubina, Sanjib Adhikari, Nabaraj Adhikari, Sanjeep Sapkota, Jid Chani Rana, Binod Dhungel, Upendra Thapa Shrestha, Megha Raj Banjara, Prakash Ghimire, and Komal Raj Rijal. 2021. "Efficacy of Urine Dipstick Test in Diagnosing Urinary Tract Infection and Detection of the blaCTX-M Gene among ESBL-Producing Escherichia coli" Diseases 9, no. 3: 59. https://doi.org/10.3390/diseases9030059
APA StyleGurung, R., Adhikari, S., Adhikari, N., Sapkota, S., Rana, J. C., Dhungel, B., Thapa Shrestha, U., Banjara, M. R., Ghimire, P., & Rijal, K. R. (2021). Efficacy of Urine Dipstick Test in Diagnosing Urinary Tract Infection and Detection of the blaCTX-M Gene among ESBL-Producing Escherichia coli. Diseases, 9(3), 59. https://doi.org/10.3390/diseases9030059