
Optimizing Perioperative Care in Esophageal Surgery: The EUropean PErioperative MEdical Networking (EUPEMEN) Collaborative for Esophagectomy

 , , , , , , , , , , , , and
, , , , , , , , , , , , and
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Consensus Formation and Protocol Development
2.2. Technical Activities
3. Results
3.1. Pre-Admission Phase
3.2. Perioperative Phase
3.2.1. Immediate Preoperative Phase
3.2.2. Intraoperative Phase
3.2.3. Immediate Postoperative Phase
3.3. Postoperative Day 1
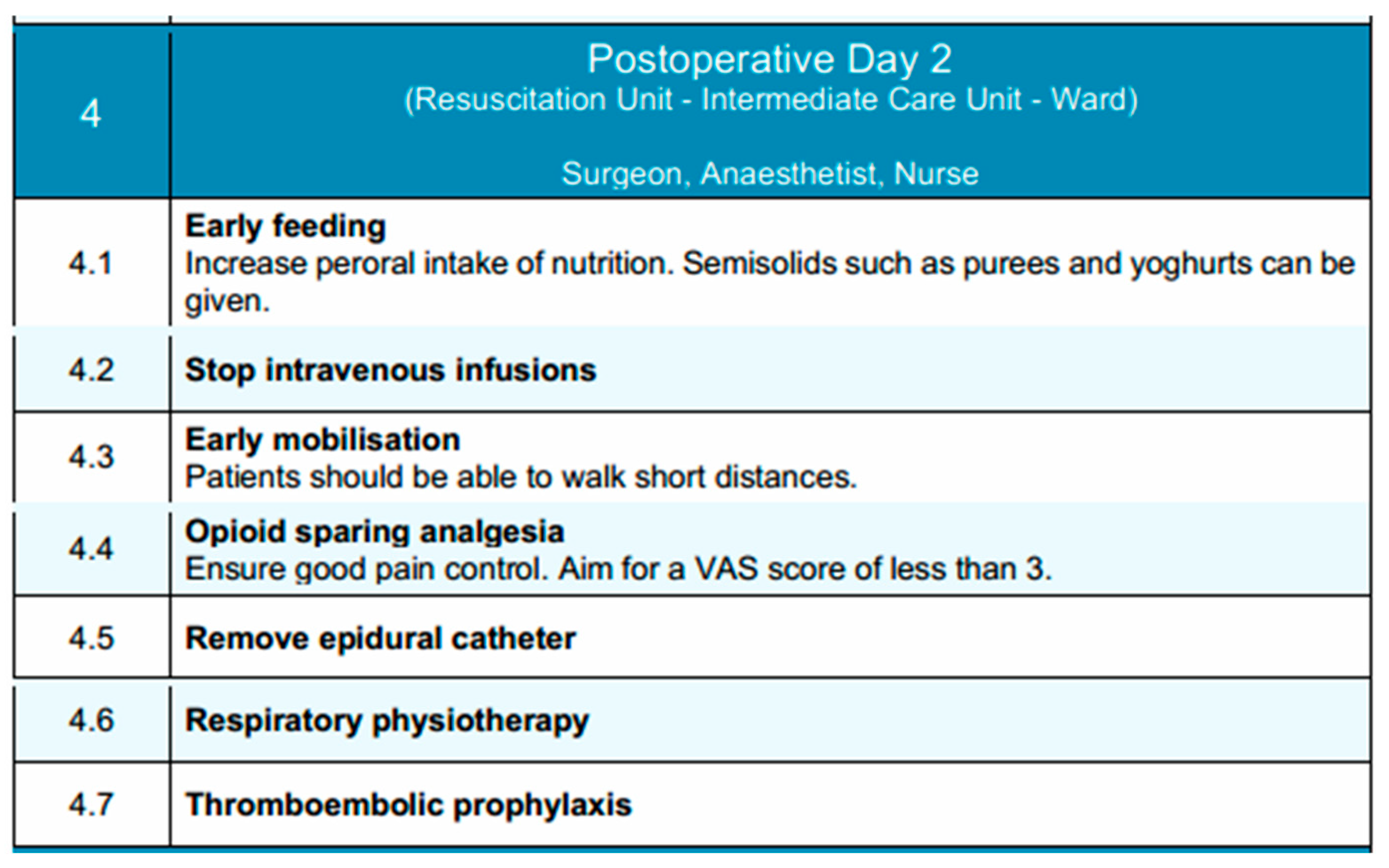
3.4. Postoperative Day 2
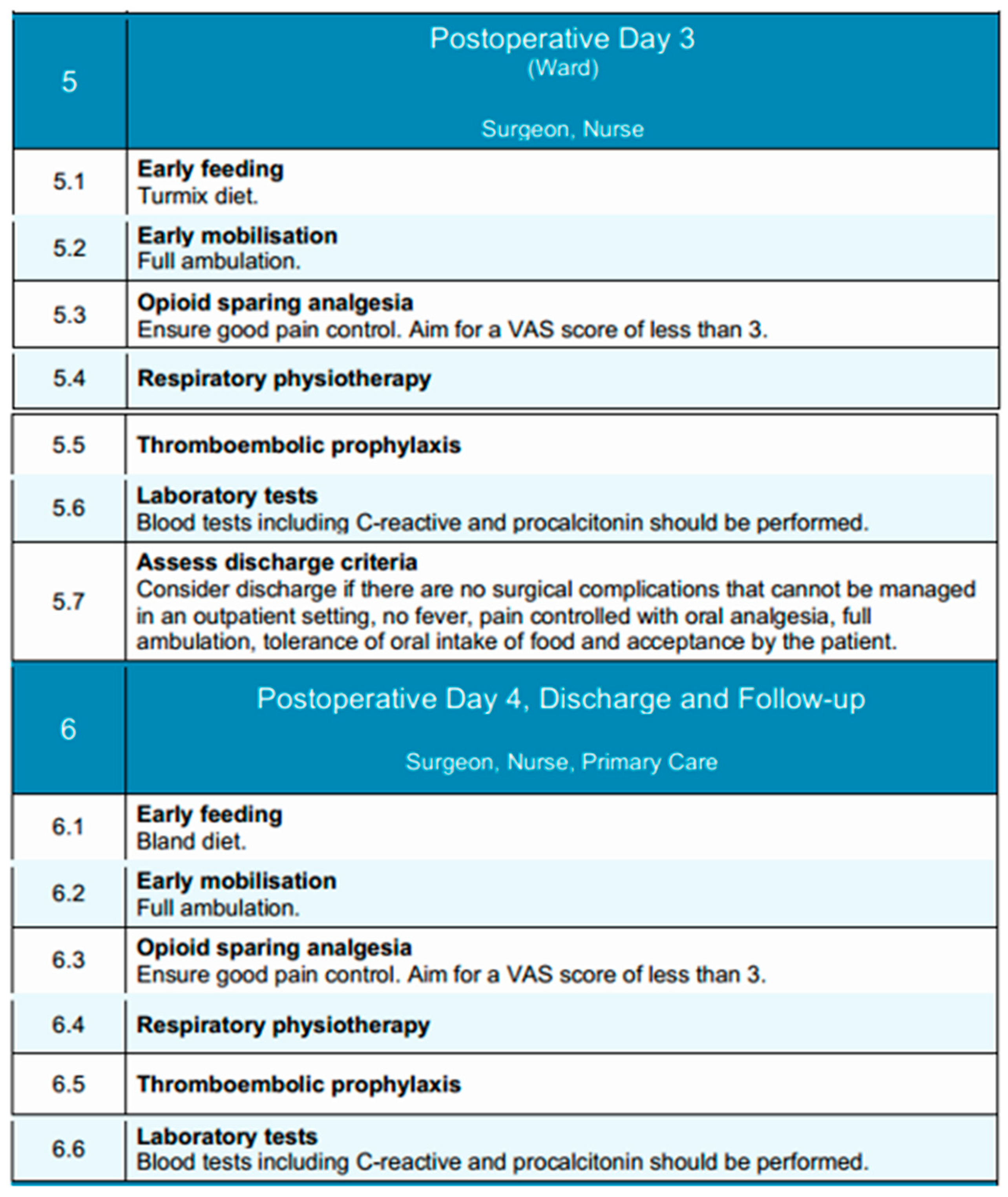
3.5. Postoperative Days 3 and 4
3.6. Discharge
4. Discussion
- –
- the development of multilingual educational materials and patient-facing documents to address language and literacy barriers;
- –
- the integration of a train-the-trainer model to promote local ownership, ensure sustainability, and facilitate iterative capacity building in varied institutional settings;
- –
- the implementation of structured audit tools and adherence-tracking mechanisms specifically adapted to cross-border benchmarking and quality assurance.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| CRP | C-reactive protein |
| EN | Enteral nutrition |
| ERAS | Enhanced recovery after surgery |
| EUPEMEN | European Perioperative Medicine Network |
| FiO2 | Fraction of inspired oxygen |
| HRQoL | Health-related quality of life |
| ICU | Intensive care unit |
| LMWH | Low molecular weight heparin |
| MDPI | Multidisciplinary Digital Publishing Institute |
| MIE | Minimally invasive esophagectomy |
| MUST | Malnutrition Universal Screening Tool |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| PACU | Post-anesthesia care unit |
| PONV | Postoperative nausea and vomiting |
| RICA | Recovery intensification for optimal care in adults |
| TAP block | Transversus abdominis plane block |
| TPN | Total parenteral nutrition |
| VAS | Visual analog scale |
| VTE | Venous thromboembolism |
References
- Abbas, G.; Krasna, M. Overview of Esophageal Cancer. Ann. Cardiothorac. Surg. 2017, 6, 131–136. [Google Scholar] [CrossRef]
- Fransen, L.F.C.; Berkelmans, G.H.K.; Asti, E.; van Berge Henegouwen, M.I.; Berlth, F.; Bonavina, L.; Brown, A.; Bruns, C.; van Daele, E.; Gisbertz, S.S.; et al. The Effect of Postoperative Complications After Minimally Invasive Esophagectomy on Long-Term Survival: An International Multicenter Cohort Study. Ann. Surg. 2021, 274, e1129–e1137. [Google Scholar] [CrossRef]
- Xing, X.; Wang, H.; Qu, S.; Huang, C.; Zhang, H.; Wang, H. The Value of Esophagectomy Surgical Apgar Score (ESAS) in Predicting the Risk of Major Morbidity after Open Esophagectomy. J. Thorac. Dis. 2016, 8, 1780–1787. [Google Scholar] [CrossRef]
- Lagergren, J.; Bottai, M.; Santoni, G. Patient Age and Survival After Surgery for Esophageal Cancer. Ann. Surg. Oncol. 2021, 28, 159–166. [Google Scholar] [CrossRef]
- Edmondson, J.; Hunter, J.; Bakis, G.; O’Connor, A.; Wood, S.; Qureshi, A.P. Understanding Post-Esophagectomy Complications and Their Management: The Early Complications. J. Clin. Med. 2023, 12, 7622. [Google Scholar] [CrossRef]
- Okamura, A.; Yamashita, K.; Kozuki, R.; Takahashi, K.; Toihata, T.; Imamura, Y.; Mine, S.; Watanabe, M. Inflammatory Response and Recurrence after Minimally Invasive Esophagectomy. Langenbeck’s Arch. Surg. 2019, 404, 761–769. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Endo, S.; Higashida, M.; Kubota, H.; Yoshimatsu, K.; Ueno, T. The Seven-Day Cumulative Post-Esophagectomy Inflammatory Response Predicts Cancer Recurrence. BMC Surg. 2024, 24, 289. [Google Scholar] [CrossRef]
- Mithany, R.H.; Daniel, N.; Shahid, M.H.; Aslam, S.; Abdelmaseeh, M.; Gerges, F.; Gill, M.U.; Abdallah, S.B.; Hannan, A.; Saeed, M.T.; et al. Revolutionizing Surgical Care: The Power of Enhanced Recovery After Surgery (ERAS). Cureus 2023, 15, e48795. [Google Scholar] [CrossRef]
- Ellwanger, M.P.; Ellwanger, M.P.; Jardine, M.B.; Bramucci, V.; Hammes, S.A.P.; Lopes, L.M.; Munhoz, A.C.M. Effectiveness of Enhanced Recovery After Surgery Protocol in Pancreatic Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Gastrointest. Surg. 2025, 29, 101939. [Google Scholar] [CrossRef]
- Puccetti, F.; Klevebro, F.; Kuppusamy, M.; Han, S.; Fagley, R.E.; Low, D.E.; Hubka, M. Analysis of Compliance with Enhanced Recovery After Surgery (ERAS) Protocol for Esophagectomy. World J. Surg. 2022, 46, 2839–2847. [Google Scholar] [CrossRef]
- Pesce, A.; Ramírez, J.M.; Fabbri, N.; Ubieto, J.M.; Bellosta, A.P.; Arroyo, A.; Sánchez-Guillén, L.; Whitley, A.; Kocián, P.; Rosetzka, K.; et al. The EUropean PErioperative MEdical Networking (EUPEMEN) Project and Recommendations for Perioperative Care in Colorectal Surgery: A Quality Improvement Study. Int. J. Surg. 2024, 110, 4796–4803. [Google Scholar] [CrossRef]
- Calvo-Vecino, J.M.; Hernández, E.; Ramirez, J.; Loinaz, C.; Trapero, C.; Quintas, C.; Antolín, A.; Rodriguez-Cuellar, E.; Aguado, J.; Ruiz-López, P.; et al. Vía Clínica de Recuperación Intensificada en Cirugía Abdominal (RICA); Ministerio de Sanidad, Servicios Sociales e Igualdad, Ed.; Instituto Aragonés de Ciencias de la Salud: Zaragoza, Spain, 2014; ISBN 680150855. [Google Scholar]
- Ioannidis, O.; Anestiadou, E.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; Kocián, P.; et al. Improving Perioperative Care in Gastric Surgery: Insights from the EUropean PErioperative MEdical Networking (EUPEMEN) Project. J. Clin. Med. 2025, 14, 2108. [Google Scholar] [CrossRef]
- Prasad, M. Introduction to the GRADE Tool for Rating Certainty in Evidence and Recommendations. Clin. Epidemiol. Glob. Health 2024, 25, 101484. [Google Scholar] [CrossRef]
- Fish, L.S.; Busby, D.M. The Delphi Method. Res. Methods Fam. Ther. 1996, 469, 482. [Google Scholar]
- Ioannidis, O.; Ramirez, J.M.; Ubieto, J.M.; Feo, C.V.; Arroyo, A.; Kocián, P.; Sánchez-Guillén, L.; Bellosta, A.P.; Whitley, A.; Enguita, A.B.; et al. The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol for Bowel Obstruction: Recommendations for Perioperative Care. J. Clin. Med. 2023, 12, 4185. [Google Scholar] [CrossRef]
- Grantham, J.P.; Hii, A.; Shenfine, J. Preoperative Risk Modelling for Oesophagectomy: A Systematic Review. World J. Gastrointest. Surg. 2023, 15, 450–470. [Google Scholar] [CrossRef]
- Thiele, R.H.; Raghunathan, K.; Brudney, C.S.; Lobo, D.N.; Martin, D.; Senagore, A.; Cannesson, M.; Gan, T.J.; Mythen, M.M.G.; Shaw, A.D.; et al. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) Joint Consensus Statement on Perioperative Fluid Management within an Enhanced Recovery Pathway for Colorectal Surgery. Perioper. Med. 2016, 5, 24. [Google Scholar] [CrossRef]
- Minnella, E.M.; Carli, F. Prehabilitation and Functional Recovery for Colorectal Cancer Patients. Eur. J. Surg. Oncol. 2018, 44, 919–926. [Google Scholar] [CrossRef]
- Watson, D.J.; Ducheine, L. The Role of the Nurse in the Prehabilitation Unit. Semin. Oncol. Nurs. 2022, 38, 151332. [Google Scholar] [CrossRef]
- Steenhagen, E. Preoperative Nutritional Optimization of Esophageal Cancer Patients. J. Thorac. Dis. 2019, 11, S645–S653. [Google Scholar] [CrossRef]
- Kurian, F.S. American Journal of Surgery and Clinical Case Reports Effect of Preoperative Educational Counselling about Routine Elements of Peri Operative Care on Patients Experience Through Their First Surgical Journey: A Randomised Control Trial. Am. J. Surg. Clin. Case Rep. 2024, 8, 1–6. [Google Scholar]
- Sivanadarajah, N.; El-Daly, I.; Mamarelis, G.; Sohail, M.Z.; Bates, P. Informed Consent and the Readability of the Written Consent Form. Ann. R. Coll. Surg. Engl. 2017, 99, 645–649. [Google Scholar] [CrossRef]
- Murat, B.; Murat, S.; Guvenc, T. Preoperative Cardiovascular Assessment and Perioperative Management of Patients with Esophageal Cancer. In Risk Factors and Therapy of Esophagus Cancer; Springer Nature: Cham, Switzerland, 2024; pp. 263–291. ISBN 9783031470233. [Google Scholar]
- Wong, J.K.L.; Ke, Y.; Ong, Y.J.; Li, H.; Wong, T.H.; Abdullah, H.R. The Impact of Preoperative Glycated Hemoglobin (HbA1c) on Postoperative Complications after Elective Major Abdominal Surgery: A Meta-Analysis. Korean J. Anesthesiol. 2022, 75, 47–60. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, S.; Yang, J.; Ke, W. The Relationship between Preoperative Anemia and Length of Hospital Stay among Patients Undergoing Radical Surgery for Esophageal Carcinoma: A Single-Centre Retrospective Study. BMC Anesthesiol. 2023, 23, 322. [Google Scholar] [CrossRef]
- Cao, J.; Xu, H.; Li, W.; Guo, Z.; Lin, Y.; Shi, Y.; Hu, W.; Ba, Y.; Li, S.; Li, Z.; et al. Nutritional Assessment and Risk Factors Associated to Malnutrition in Patients with Esophageal Cancer. Curr. Probl. Cancer 2021, 45, 100638. [Google Scholar] [CrossRef]
- Chao, P.-C.; Chuang, H.-J.; Tsao, L.-Y.; Chen, P.-Y.; Hsu, C.-F.; Lin, H.-C.; Chang, C.-Y.; Lin, C.-F. The Malnutrition Universal Screening Tool (MUST) and a Nutrition Education Program for High Risk Cancer Patients: Strategies to Improve Dietary Intake in Cancer Patients. BioMedicine 2015, 5, 17. [Google Scholar] [CrossRef]
- Serrano, P.E.; Parpia, S.; Simunovic, M.; Duceppe, E.; Pinto-Sanchez, M.I.; Bhandari, M.; Levine, M. Perioperative Optimization with Nutritional Supplements in Patients Undergoing Gastrointestinal Surgery for Cancer: A Randomized, Placebo-Controlled Feasibility Clinical Trial. Surgery 2022, 172, 670–676. [Google Scholar] [CrossRef]
- Wan, R.; Juanjuan, Z.; Yi, S.; Xiaoqin, Z. Comparative Assessment of Skeletal Muscle Index and Sarcopenia in Patients with Gastric Cancer between Computed Tomography and Bioelectrical Impedance. Clin. Nutr. ESPEN 2025, 65, 494–495. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Cao, Y.; Han, D.; Yang, S.; Shi, Y.; Zhao, S.; Jin, Q.; Li, J.; Li, C.; Zhang, Y.; Shen, W.; et al. Effects of Pre-Operative Enteral Immunonutrition for Esophageal Cancer Patients Treated with Neoadjuvant Chemoradiotherapy: Protocol for a Multicenter Randomized Controlled Trial (Point Trial, Pre-Operative Immunonutrition Therapy). BMC Cancer 2022, 22, 650. [Google Scholar] [CrossRef]
- Kanekiyo, S.; Takeda, S.; Iida, M.; Nishiyama, M.; Kitahara, M.; Shindo, Y.; Tokumitsu, Y.; Tomochika, S.; Tsunedomi, R.; Suzuki, N.; et al. Efficacy of Perioperative Immunonutrition in Esophageal Cancer Patients Undergoing Esophagectomy. Nutrition 2019, 59, 96–102. [Google Scholar] [CrossRef]
- Yoshida, N.; Eto, K.; Horinouchi, T.; Harada, K.; Sawayama, H.; Ogawa, K.; Nagai, Y.; Iwatsuki, M.; Iwagami, S.; Ishimoto, T.; et al. Preoperative Smoking Cessation and Prognosis After Curative Esophagectomy for Esophageal Cancer: A Cross-Sectional Study. Ann. Surg. Oncol. 2022, 29, 8172–8180. [Google Scholar] [CrossRef] [PubMed]
- Piraux, E.; Reychler, G.; de Noordhout, L.M.; Forget, P.; Deswysen, Y.; Caty, G. What Are the Impact and the Optimal Design of a Physical Prehabilitation Program in Patients with Esophagogastric Cancer Awaiting Surgery ? A Systematic Review. BMC Sports Sci. Med. Rehabil. 2021, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Hellstadius, Y.; Lagergren, J.; Zylstra, J.; Gossage, J.; Davies, A.; Hultman, C.M.; Lagergren, P.; Wikman, A. A Longitudinal Assessment of Psychological Distress after Oesophageal Cancer Surgery. Acta Oncol. 2017, 56, 746–752. [Google Scholar] [CrossRef]
- Gu, C.; Lu, A.; Lei, C.; Wu, Q.; Zhang, X.; Wei, M.; Wang, Z. Frailty Index Is Useful for Predicting Postoperative Morbidity in Older Patients Undergoing Gastrointestinal Surgery: A Prospective Cohort Study. BMC Surg. 2022, 22, 57. [Google Scholar] [CrossRef]
- Hendrix, J.M.; Garmon, E.H. American Society of Anesthesiologists Physical Status Classification System. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Choy, R.; Pereira, K.; Silva, S.G.; Thomas, N.; Tola, D.H. Use of Apfel Simplified Risk Score to Guide Postoperative Nausea and Vomiting Prophylaxis in Adult Patients Undergoing Same-Day Surgery. J. Perianesthesia Nurs. 2022, 37, 445–451. [Google Scholar] [CrossRef]
- Gillis, C.; Coca-Martinez, M.; Santa Mina, D. Tailoring Prehabilitation to Address the Multifactorial Nature of Functional Capacity for Surgery. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2023, 36, 395–405. [Google Scholar] [CrossRef]
- Kubota, T.; Shoda, K.; Konishi, H.; Okamoto, K.; Otsuji, E. Nutrition Update in Gastric Cancer Surgery. Ann. Gastroenterol. Surg. 2020, 4, 360–368. [Google Scholar] [CrossRef]
- Zambouri, A. Preoperative Evaluation and Preparation for Anesthesia and Surgery. Hippokratia 2007, 11, 13–21. [Google Scholar]
- Zwischenberger, B.A.; Tzeng, C.-W.D.; Ward, N.D.; Zwischenberger, J.B.; Martin, J.T. Venous Thromboembolism Prophylaxis For Esophagectomy: A Survey of Practice Patterns Among Thoracic Surgeons. Ann. Thorac. Surg. 2016, 101, 489–494. [Google Scholar] [CrossRef]
- Afshari, A.; Ageno, W.; Ahmed, A.; Duranteau, J.; Faraoni, D.; Kozek-langenecker, S.; Llau, J.; Nizard, J.; Solca, M.; Stensballe, J.; et al. European Guidelines on Perioperative Venous Thromboembolism Prophylaxis Executive Summary. Eur. J. Anaesthesiol. | EJA 2018, 35, 77–83. [Google Scholar] [CrossRef]
- Awad, S.; Varadhan, K.K.; Ljungqvist, O.; Lobo, D.N. A Meta-Analysis of Randomised Controlled Trials on Preoperative Oral Carbohydrate Treatment in Elective Surgery. Clin. Nutr. 2013, 32, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Melis, G.C.; van Leeuwen, P.A.M.; von Blomberg-van der Flier, B.M.E.; Goedhart-Hiddinga, A.C.; Uitdehaag, B.M.J.; van Strack Schijndel, R.J.M.; Wuisman, P.I.J.M.; van Bokhorst-de van der Schueren, M.A.E. A Carbohydrate-Rich Beverage Prior to Surgery Prevents Surgery-Induced Immunodepression: A Randomized, Controlled, Clinical Trial. JPEN J. Parenter. Enteral Nutr. 2006, 30, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Sidik, A.I.; Faybushevich, A.G.; Hossain, M.L.; Samnang, E.; Dontsov, V.V. Enhancing Compliance with Preoperative Fasting Guidelines: A Closed-Loop Quality Improvement Initiative to Optimize Patient Safety and Outcomes. Cureus 2024, 16, e75250. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Konishi, T.; Kaneko, H.; Itoh, H.; Matsuda, S.; Kawakubo, H.; Uda, K.; Matsui, H.; Fushimi, K.; Daiko, H.; et al. Antimicrobial Prophylaxis with Ampicillin-Sulbactam Compared with Cefazolin for Esophagectomy: Nationwide Inpatient Database Study in Japan. Ann. Surg. 2024, 279, 640–647. [Google Scholar] [CrossRef]
- Higaki, E.; Abe, T.; Fujieda, H.; Hosoi, T. Significance of Antimicrobial Prophylaxis for the Prevention of Early-Onset Pneumonia After Radical Esophageal Cancer Resection: A Retrospective Analysis of 356 Patients Undergoing Thoracoscopic Esophagectomy. Ann. Surg. Oncol. 2022, 29, 1374–1387. [Google Scholar] [CrossRef]
- Hua, X.-H.; Shi, K.-F.; Yu, Y.-K.; Li, H.-M.; Ma, F.; Sun, H.-B.; Qian, R.-L.; Li, Y. Nutritional Assessment in Esophageal Fast-Track Surgery: Comparisons of 4 Objective Malnutrition Screening Tools. Ann. Transl. Med. 2022, 10, 20. [Google Scholar] [CrossRef]
- Chen, M.-J.; Wu, I.-C.; Chen, Y.-J.; Wang, T.-E.; Chang, Y.-F.; Yang, C.-L.; Huang, W.-C.; Chang, W.-K.; Sheu, B.-S.; Wu, M.-S.; et al. Nutrition Therapy in Esophageal Cancer-Consensus Statement of the Gastroenterological Society of Taiwan. Dis. Esophagus 2018, 31, doy016. [Google Scholar] [CrossRef]
- Liu, K.; Ji, S.; Xu, Y.; Diao, Q.; Shao, C.; Luo, J.; Zhu, Y.; Jiang, Z.; Diao, Y.; Cong, Z.; et al. Safety, Feasibility, and Effect of an Enhanced Nutritional Support Pathway Including Extended Preoperative and Home Enteral Nutrition in Patients Undergoing Enhanced Recovery after Esophagectomy: A Pilot Randomized Clinical Trial. Dis. Esophagus 2020, 33, doz030. [Google Scholar] [CrossRef]
- Álvarez-Sarrado, E.; Mingol Navarro, F.; J Rosellón, R.; Ballester Pla, N.; Vaqué Urbaneja, F.J.; Muniesa Gallardo, C.; López Rubio, M.; García-Granero Ximénez, E. Feeding Jejunostomy after Esophagectomy Cannot Be Routinely Recommended. Analysis of Nutritional Benefits and Catheter-Related Complications. Am. J. Surg. 2019, 217, 114–120. [Google Scholar] [CrossRef]
- Weijs, T.J.; Berkelmans, G.H.K.; Nieuwenhuijzen, G.A.P.; Ruurda, J.P.; van Hillegersberg, R.; Soeters, P.B.; Luyer, M.D.P. Routes for Early Enteral Nutrition after Esophagectomy. A Systematic Review. Clin. Nutr. 2015, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lorimer, P.D.; Motz, B.M.; Watson, M.; Trufan, S.J.; Prabhu, R.S.; Hill, J.S.; Salo, J.C. Enteral Feeding Access Has an Impact on Outcomes for Patients with Esophageal Cancer Undergoing Esophagectomy: An Analysis of SEER-Medicare. Ann. Surg. Oncol. 2019, 26, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Avinash, S.H.; Krishna, H.M. The Impact of the Apfel Scoring System for Prophylaxis of Post-Operative Nausea and Vomiting: A Randomized Controlled Trial. J. Anaesthesiol. Clin. Pharmacol. 2023, 39, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Muraoka, K.; Sato, M.; Yonezawa, R.; Kurihara, T.; Higuchi, S.; Kogo, M. Risk Factors for Postoperative Nausea and Vomiting after Video-Assisted Thoracic Surgery Esophagectomy: A Prospective Cohort Study. Die Pharm.-Int. J. Pharm. Sci. 2024, 79, 17–23. [Google Scholar] [CrossRef]
- Sotto, K.T.; Burian, B.K.; Brindle, M.E. Impact of the WHO Surgical Safety Checklist Relative to Its Design and Intended Use: A Systematic Review and Meta-Meta-Analysis. J. Am. Coll. Surg. 2021, 233, 794–809.e8. [Google Scholar] [CrossRef]
- Boyce, J.M. Tag EdFi Ur Tag EdFi Ur Tag EdH1 Best Products for Skin Antisepsis Tag EdEn. AJIC Am. J. Infect. Control 2023, 51, A58–A63. [Google Scholar] [CrossRef]
- Haffey, S.; Quinlivan, L.; O’Donovan, C.A. Intraoperative Monitoring. Arch. Neurol. 2005, 62, 1636–1637. [Google Scholar] [CrossRef]
- Mann, C.; Berlth, F.; Hadzijusufovic, E.; Lang, H.; Grimminger, P.P. Minimally Invasive Esophagectomy: Clinical Evidence and Surgical Techniques. Langenbeck’s Arch. Surg. 2020, 405, 1061–1067. [Google Scholar] [CrossRef]
- Jackson, J.C.; Molena, D.; Amar, D. Evolving Perspectives on Esophagectomy Care: Clinical Update. Anesthesiology 2023, 139, 868–879. [Google Scholar] [CrossRef]
- Saito, K.; Nakajima, Y.; Kawada, K.; Tokairin, Y.; Kawano, T. Is a Central Venous Catheter Necessary for the Perioperative Management of Esophagectomy? A Prospective Randomized Pilot Study Comparing Two Different Perioperative Regimens. Dig. Surg. 2016, 33, 478–487. [Google Scholar] [CrossRef]
- Fujiwara, D.; Watanabe, M.; Kanie, Y.; Maruyama, S.; Sakamoto, K.; Okamura, A.; Kanamori, J.; Imamura, Y.; Mine, S. Is Prophylactic Cervical Drainage Effective in Patients Undergoing McKeown Esophagectomy Reconstructed Through the Retrosternal Route with Two-Field Lymphadenectomy? World J. Surg. 2022, 46, 1944–1951. [Google Scholar] [CrossRef]
- Oshikiri, T.; Takiguchi, G.; Miura, S.; Takase, N.; Hasegawa, H.; Yamamoto, M.; Kanaji, S.; Yamashita, K.; Matsuda, Y.; Matsuda, T.; et al. Non-Placement versus Placement of a Drainage Tube around the Cervical Anastomosis in McKeown Esophagectomy: Study Protocol for a Randomized Controlled Trial. Trials 2019, 20, 758. [Google Scholar] [CrossRef] [PubMed]
- Oshikiri, T.; Goto, H.; Kato, T.; Takiguchi, G.; Koterazawa, Y.; Hasegawa, H.; Kanaji, S.; Yamashita, K.; Matsuda, T.; Nakamura, T.; et al. A Randomized Controlled Trial Exploring the Effect of Placement versus Nonplacement of a Drainage Tube around the Cervical Anastomosis in McKeown Esophagectomy. Sci. Rep. 2025, 15, 19698. [Google Scholar] [CrossRef] [PubMed]
- Verstegen, M.H.P.; Bouwense, S.A.W.; van Workum, F.; Ten Broek, R.; Siersema, P.D.; Rovers, M.; Rosman, C. Management of Intrathoracic and Cervical Anastomotic Leakage after Esophagectomy for Esophageal Cancer: A Systematic Review. World J. Emerg. Surg. 2019, 14, 17. [Google Scholar] [CrossRef] [PubMed]
- Linden, P.A.; Towe, C.W.; Worrell, S.G.; Jiang, B.; Ho, V.P.; Argote-Greene, L.; Bachman, K.; Perry, Y. Drain Amylase: A Simple and Versatile Method of Detecting Esophageal Anastomotic Leaks. Ann. Thorac. Surg. 2022, 113, 1794–1800. [Google Scholar] [CrossRef]
- De Pasqual, C.A.; Weindelmayer, J.; Laiti, S.; La Mendola, R.; Bencivenga, M.; Alberti, L.; Giacopuzzi, S.; de Manzoni, G. Perianastomotic Drainage in Ivor-Lewis Esophagectomy, Does Habit Affect Utility? An 11-Year Single-Center Experience. Updates Surg. 2020, 72, 47–53. [Google Scholar] [CrossRef]
- Gómez-Caro, A.; Roca, M.J.; Torres, J.; Cascales, P.; Terol, E.; Castañer, J.; Piñero, A.; Parrilla, P. Successful Use of a Single Chest Drain Postlobectomy Instead of Two Classical Drains: A Randomized Study. Eur. J. Cardio-Thorac. Surg. 2006, 29, 562–566. [Google Scholar] [CrossRef]
- Refai, M.; Brunelli, A.; Salati, M.; Xiumè, F.; Pompili, C.; Sabbatini, A. The Impact of Chest Tube Removal on Pain and Pulmonary Function after Pulmonary Resection. Eur. J. Cardio-Thorac. Surg. 2012, 41, 820–822. [Google Scholar] [CrossRef]
- Johansson, J.; Lindberg, C.G.; Johnsson, F.; von Holstein, C.S.; Zilling, T.; Walther, B. Active or Passive Chest Drainage after Oesophagectomy in 101 Patients: A Prospective Randomized Study. Br. J. Surg. 1998, 85, 1143–1146. [Google Scholar] [CrossRef]
- Findlay, J.M.; Gillies, R.S.; Millo, J.; Sgromo, B.; Marshall, R.E.K.; Maynard, N.D. Enhanced Recovery for Esophagectomy: A Systematic Review and Evidence-Based Guidelines. Ann. Surg. 2014, 259, 413–431. [Google Scholar] [CrossRef]
- Hessami, M.A.; Najafi, F.; Hatami, S. Volume Threshold for Chest Tube Removal: A Randomized Controlled Trial. J. Inj. Violence Res. 2009, 1, 33–36. [Google Scholar] [CrossRef]
- Novoa, N.M.; Jiménez, M.F.; Varela, G. When to Remove a Chest Tube. Thorac. Surg. Clin. 2017, 27, 41–46. [Google Scholar] [CrossRef]
- Yao, F.; Wang, J.; Yao, J.; Hang, F.; Cao, S.; Qian, J.; Xu, L. Early Chest Tube Removal After Thoracoscopic Esophagectomy with High Output. J. Laparoendosc. Adv. Surg. Tech. A 2016, 26, 17–22. [Google Scholar] [CrossRef]
- Alvarez Uslar, R.; Molina, H.; Torres, O.; Cancino, A. Total Gastrectomy with or without Abdominal Drains. A Prospective Randomized Trial. Rev. Esp. Enfermedades Dig. 2005, 97, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, J.; Hyung, W.J.; Cheong, J.H.; Chen, J.; Choi, S.H.; Noh, S.H. Gastric Cancer Surgery without Drains: A Prospective Randomized Trial. J. Gastrointest. Surg. 2004, 8, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, J.; Su, K.; Dong, Z. Abdominal Drainage versus No Drainage Post-Gastrectomy for Gastric Cancer. Cochrane Database Syst. Rev. 2015, 2015, CD008788. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, C.L.; Dos Santos, L.L.; Tavares, G.; Tristão, L.S.; Orlandini, M.F.; Serafim, M.C.A.; Datrino, L.N.; Bernardo, W.M.; Tustumi, F. Prophylactic Thoracic Duct Obliteration and Resection during Esophagectomy: What Is the Impact on Perioperative Risks and Long-Term Survival? A Systematic Review and Meta-Analysis. J. Surg. Oncol. 2022, 126, 90–98. [Google Scholar] [CrossRef]
- Okamoto, K.; Ninomiya, I.; Maruzen, S.; Makino, I.; Fujimura, T.; Ohta, T. Usefulness of a Short-Acting β1-Selective Blocker, Landiolol Hydrochloride, for Tachyarrhythmia after Thoracoscopic Esophagectomy. Nihon Rinsho Geka Gakkai Zasshi J. Jpn. Surg. Assoc. 2013, 74, 874–879. [Google Scholar] [CrossRef]
- Mukai, A.; Suehiro, K.; Watanabe, R.; Juri, T.; Hayashi, Y.; Tanaka, K.; Fujii, T.; Ohira, N.; Oda, Y.; Okutani, R.; et al. Impact of Intraoperative Goal-Directed Fluid Therapy on Major Morbidity and Mortality after Transthoracic Oesophagectomy: A Multicentre, Randomised Controlled Trial. Br. J. Anaesth. 2020, 125, 953–961. [Google Scholar] [CrossRef]
- Takahashi, M.; Toyama, H.; Takahashi, K.; Kaiho, Y.; Ejima, Y.; Yamauchi, M. Impact of Intraoperative Fluid Management on Postoperative Complications in Patients Undergoing Minimally Invasive Esophagectomy for Esophageal Cancer: A Retrospective Single—Center Study. BMC Anesthesiol. 2024, 24, 29. [Google Scholar] [CrossRef]
- Menéndez-Jiménez, M.; Bruna-Esteban, M.; Mingol, F.; Vaqué, J.; Hervas Marin, D.; Álvarez-Sarrado, E.; Navasquillo-Tamarit, M.; Hurtado-Pardo, L.; Garcia-Granero, A. Uso de Sonda Nasogástrica En Pacientes Sometidos a Esofaguectomía: ¿Un Gesto Innecesario? Cirugía Española 2020, 98, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Mistry, R.C.; Vijayabhaskar, R.; Karimundackal, G.; Jiwnani, S.; Pramesh, C.S. Effect of Short-Term vs Prolonged Nasogastric Decompression on Major Postesophagectomy Complications: A Parallel-Group, Randomized Trial. Arch. Surg. 2012, 147, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Kawakubo, H.; Shoji, Y.; Mayanagi, S.; Nakamura, R.; Suda, K.; Wada, N.; Takeuchi, H.; Kitagawa, Y. Analysis of the Effect of Early Versus Conventional Nasogastric Tube Removal on Postoperative Complications After Transthoracic Esophagectomy: A Single-Center, Randomized Controlled Trial. World J. Surg. 2019, 43, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, H.; Tanaka, K.; Funai, Y.; Suehiro, K.; Ikenaga, K.; Mori, T.; Osugi, H.; Nishikawa, K. The Impact of Intraoperative Hypothermia on Early Postoperative Adverse Events after Radical Esophagectomy for Cancer: A Retrospective Cohort Study. J. Cardiothorac. Vasc. Anesth. 2014, 28, 943–947. [Google Scholar] [CrossRef]
- Feenstra, M.L.; van Berge Henegouwen, M.I.; Hollmann, M.W.; Hermanides, J.; Eshuis, W.J. Analgesia in Esophagectomy: A Narrative Review. J. Thorac. Dis. 2023, 15, 5099–5111. [Google Scholar] [CrossRef]
- Qiu, Y.; Lu, X.; Liu, Y.; Chen, X.; Wu, J. Efficacy of the Intraoperative Opioid-Sparing Anesthesia on Quality of Patients ’ Recovery in Video-Assisted Thoracoscopic Surgery: A Randomized Trial. J. Thorac. Dis. 2022, 14, 2544–2555. [Google Scholar] [CrossRef]
- Berhe, Y.W.; Gebregzi, A.H.; Endalew, N.S. Guideline on Peri-Operative Glycemic Control for Adult Patient with Diabetic Mellitus: Resource Limited Areas. Int. J. Surg. Open 2017, 9, 1–6. [Google Scholar] [CrossRef]
- Qin, J.; Li, Y.; Xing, W.; Yan, M.; Jiang, Q. Fast Track Program for Esophagectomy Patients. Thorac. Cancer 2012, 3, 55–59. [Google Scholar] [CrossRef]
- Lehtinen, S.J.; Onicescu, G.; Kuhn, K.M.; Cole, D.J.; Esnaola, N.F. Normothermia to Prevent Surgical Site Infections after Gastrointestinal Surgery: Holy Grail or False Idol? Ann. Surg. 2010, 252, 696–704. [Google Scholar] [CrossRef]
- Drinhaus, H.; Lambertz, R.; Schröder, W.; Annecke, T. Analgesia During and After Esophagectomy: The Surgical Approach Matters. Ann. Thorac. Surg. 2018, 106, 1259. [Google Scholar] [CrossRef]
- Hospital, B.F. Advantages and Application of Restricted Fluid Therapy after Resection of Esophageal Carcinoma. Chin. J. Clin. Thorac. Cardiovasc. Surg. 2022, 29, 257–261. [Google Scholar]
- Raju, T.A.; Torjman, M.C.; Goldberg, M.E. Perioperative Blood Glucose Monitoring in the General Surgical Population. J. Diabetes Sci. Technol. 2009, 3, 1282–1287. [Google Scholar] [CrossRef] [PubMed]
- Tukanova, K.H.; Chidambaram, S.; Guidozzi, N.; Hanna, G.B.; McGregor, A.H.; Markar, S.R. Physiotherapy Regimens in Esophagectomy and Gastrectomy: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2022, 29, 3148–3167. [Google Scholar] [CrossRef] [PubMed]
- Weijs, T.J.; Berkelmans, G.H.K.; Nieuwenhuijzen, G.A.P.; Dolmans, A.C.P.; Kouwenhoven, E.A.; Rosman, C.; Ruurda, J.P.; van Workum, F.; van Det, M.J.; Silva Corten, L.C.; et al. Immediate Postoperative Oral Nutrition Following Esophagectomy: A Multicenter Clinical Trial. Ann. Thorac. Surg. 2016, 102, 1141–1148. [Google Scholar] [CrossRef]
- Li, X.; Yan, S.; Ma, Y.; Li, S.; Wang, Y.; Wang, X.; Wang, Y.; Wang, J.; Lv, C.; Yang, Y.; et al. Impact of Early Oral Feeding on Anastomotic Leakage Rate After Esophagectomy: A Systematic Review and Meta-Analysis. World J. Surg. 2020, 44, 2709–2718. [Google Scholar] [CrossRef]
- Kingma, B.F.; Steenhagen, E.; Ruurda, J.P.; van Hillegersberg, R. Nutritional Aspects of Enhanced Recovery after Esophagectomy with Gastric Conduit Reconstruction. J. Surg. Oncol. 2017, 116, 623–629. [Google Scholar] [CrossRef]
- Tomaszek, S.C.; Cassivi, S.D.; Allen, M.S.; Shen, K.R.; Nichols, F.C., 3rd; Deschamps, C.; Wigle, D.A. An Alternative Postoperative Pathway Reduces Length of Hospitalisation Following Oesophagectomy. Eur. J. Cardio-Thorac. Surg. 2010, 37, 807–813. [Google Scholar] [CrossRef]
- Giacopuzzi, S.; Weindelmayer, J.; Treppiedi, E.; Bencivenga, M.; Ceola, M.; Priolo, S.; Carlini, M.; de Manzoni, G. Enhanced Recovery after Surgery Protocol in Patients Undergoing Esophagectomy for Cancer: A Single Center Experience. Dis. Esophagus 2017, 30, 1–6. [Google Scholar] [CrossRef]
- Sun, H.-B.; Li, Y.; Liu, X.-B.; Zhang, R.-X.; Wang, Z.-F.; Lerut, T.; Liu, C.-C.; Fiorelli, A.; Chao, Y.-K.; Molena, D.; et al. Early Oral Feeding Following McKeown Minimally Invasive Esophagectomy: An Open-Label, Randomized, Controlled, Noninferiority Trial. Ann. Surg. 2018, 267, 435–442. [Google Scholar] [CrossRef]
- Berkelmans, G.H.K.; Fransen, L.F.C.; Dolmans-Zwartjes, A.C.P.; Kouwenhoven, E.A.; van Det, M.J.; Nilsson, M.; Nieuwenhuijzen, G.A.P.; Luyer, M.D.P. Direct Oral Feeding Following Minimally Invasive Esophagectomy (NUTRIENT II Trial): An International, Multicenter, Open-Label Randomized Controlled Trial. Ann. Surg. 2020, 271, 41–47. [Google Scholar] [CrossRef]
- Hong, Z.; Lu, Y.; Li, H.; Cheng, T.; Sheng, Y. Effect of Early Versus Late Oral Feeding on Postoperative Complications and Recovery Outcomes for Patients with Esophageal Cancer: A Systematic Evaluation and Meta—Analysis. Ann. Surg. Oncol. 2023, 30, 8251–8260. [Google Scholar] [CrossRef] [PubMed]
- Sims, C.R.; Abou Chaar, M.K.; Kerfeld, M.H.; Cassivi, S.D.; Hofer, R.E.; Nichols, F.C.; Reisenauer, J.; Saddoughi, S.S.; Shen, K.R.; Stewart, T.M.; et al. Esophagectomy Enhanced Recovery After Surgery Initiative Results in Improved Outcomes. Ann. Thorac. Surg. 2024, 117, 847–857. [Google Scholar] [CrossRef] [PubMed]
- Sahm, E.; Olutola, O.; Ata, A.; Fabian, T.; Marthy, A.; Deroo, A.; Edwards, K.; Tafen, M. When Is Intensive Care Unit Admission Needed After an Esophagectomy? J. Surg. Res. 2024, 300, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, H.; Gershengorn, H.B.; Cooke, C.R.; Guerra, C.; Angus, D.C.; Rowe, J.W.; Li, G. Use of Intensive Care Services for Medicare Beneficiaries Undergoing Major Surgical Procedures. Anesthesiology 2016, 124, 899–907. [Google Scholar] [CrossRef]
- Stephens, M.R.; Lewis, W.G.; Brewster, A.E.; Lord, I.; Blackshaw, G.R.J.C.; Hodzovic, I.; Thomas, G.V.; Roberts, S.A.; Crosby, T.D.L.; Gent, C.; et al. Multidisciplinary Team Management Is Associated with Improved Outcomes after Surgery for Esophageal Cancer. Dis. Esophagus 2006, 19, 164–171. [Google Scholar] [CrossRef]
- El-Sourani, N.; Bruns, H.; Troja, A.; Raab, H.-R.; Antolovic, D. Routine Use of Contrast Swallow After Total Gastrectomy and Esophagectomy: Is It Justified? Polish J. Radiol. 2017, 82, 170–173. [Google Scholar] [CrossRef]
- Wouters, M.W.; Wijnhoven, B.P.; Karim-Kos, H.E.; Blaauwgeers, H.G.; Stassen, L.P.; Steup, W.-H.; Tilanus, H.W.; Tollenaar, R.A. High-Volume versus Low-Volume for Esophageal Resections for Cancer: The Essential Role of Case-Mix Adjustments Based on Clinical Data. Ann. Surg. Oncol. 2008, 15, 80–87. [Google Scholar] [CrossRef]
- McCahill, L.E.; May, M.; Morrow, J.B.; Khandavalli, S.; Shabahang, B.; Kemmeter, P.; Pimiento, J.M. Esophagectomy Outcomes at a Mid-Volume Cancer Center Utilizing Prospective Multidisciplinary Care and a 2-Surgeon Team Approach. Am. J. Surg. 2014, 207, 380–386. [Google Scholar] [CrossRef]
- Hamai, Y.; Hihara, J.U.N.; Emi, M.; Ibuki, Y.; Kurokawa, T. Prospective Randomized Trial of Early Postoperative Enteral and Total Parenteral Nutrition for Treating Esophageal Cancer. Anticancer Res. 2021, 6246, 6237–6246. [Google Scholar] [CrossRef]
- de Boer, A.G.E.M.; van Lanschot, J.J.B.; Stalmeier, P.F.M.; van Sandick, J.W.; Hulscher, J.B.F.; de Haes, J.C.J.M.; Sprangers, M.A.G. Is a Single-Item Visual Analogue Scale as Valid, Reliable and Responsive as Multi-Item Scales in Measuring Quality of Life? Qual. Life Res. 2004, 13, 311–320. [Google Scholar] [CrossRef]
- Schuring, N.; Gisbertz, S. Can Goals for Early Postoperative Ambulation After Esophagectomy Be Established? In Difficult Decisions in Thoracic Surgery: An Evidence-Based Approach; Springer Nature: Cham, Switzerland, 2025; pp. 439–447. ISBN 978-3-031-78662-4. [Google Scholar]
- Jiwnani, S.; Karthik, V. Does Early Postoperative Ambulation Improve Surgical Outcomes After Esophagectomy? In Difficult Decisions in Thoracic Surgery: An Evidence-Based Approach; Ferguson, M.K., Ed.; Springer Nature: Cham, Switzerland, 2024; pp. 125–133. ISBN 978-3-031-78663-1. [Google Scholar]
- Weijs, T.J.; Ruurda, J.P.; Nieuwenhuijzen, G.A.P.; van Hillegersberg, R.; Luyer, M.D.P. Strategies to Reduce Pulmonary Complications after Esophagectomy. World J. Gastroenterol. 2013, 19, 6509–6514. [Google Scholar] [CrossRef] [PubMed]
- Theochari, N.A.; Theochari, C.A.; Kokkinidis, D.G.; Kechagias, A.; Lyros, O.; Giannopoulos, S.; Mantziari, S.; Schizas, D. Venous Thromboembolism after Esophagectomy for Cancer: A Systematic Review of the Literature to Evaluate Incidence, Risk Factors, and Prophylaxis. Surg. Today 2022, 52, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; French, D.G.; Costache, I. Pain Management within an Enhanced Recovery Program after Thoracic Surgery. J. Thorac. Dis. 2018, 10, 3773–3780. [Google Scholar] [CrossRef] [PubMed]
- Guinan, E.; Dowds, J.; Donohoe, C.; Reynolds, J.; Hussey, J. The Physiotherapist and the Esophageal Cancer Patient: From Prehabilitation to Rehabilitation: Physiotherapy and Esophageal Cancer. Dis. Esophagus 2016, 30, 1–12. [Google Scholar] [CrossRef]
- Shirinzadeh, A.; Talebi, Y. Pulmonary Complications Due to Esophagectomy. J. Cardiovasc. Thorac. Res. 2011, 3, 93–96. [Google Scholar] [CrossRef]
- Yamashita, K.; Yamasaki, M.; Miyazaki, Y.; Matsuura, N.; Tanaka, K.; Makino, T.; Saito, T.; Yamamoto, K.; Takahashi, T.; Motoori, M.; et al. Protein-Enhanced Feeds after Esophagectomy for Esophageal Cancer Attenuate Postoperative Catabolism: A Prospective Observational Study. Surg. Today 2022, 52, 624–632. [Google Scholar] [CrossRef]
- Niihara, M.; Tsubosa, Y.; Yamashita, A.; Mori, K.; Tsumaki, H.; Onozawa, Y.; Fukuda, H. Supplemental Enteral Tube Feeding Nutrition after Hospital Discharge of Esophageal Cancer Patients Who Have Undergone Esophagectomy. Esophagus 2021, 18, 504–512. [Google Scholar] [CrossRef]
- Rosner, A.K.; van der Sluis, P.C.; Meyer, L.; Wittenmeier, E.; Engelhard, K.; Grimminger, P.P.; Griemert, E.-V. Pain Management after Robot-Assisted Minimally Invasive Esophagectomy. Heliyon 2023, 9, e13842. [Google Scholar] [CrossRef]
- Hu, Z.-H.; Li, R.-X.; Wang, J.-T.; Wang, G.-J.; Deng, X.-M.; Zhu, T.-Y.; Gao, B.-L.; Zhang, Y.-F. Thoracolaparoscopic Esophagectomy for Esophageal Cancer with a Cervical or Abdominal Incision to Extract Specimen. Medicine 2022, 101, e31131. [Google Scholar] [CrossRef]
- Gyldenholm, T.; Madsen, N.; Katballe, N.; Kjær, D.W.; Christensen, T.D.; Hvas, A.-M. Prolonged vs Standard Thromboprophylaxis in Patients with Esophageal Cancer Undergoing Surgery: A Randomized Controlled Study. J. Thromb. Haemost. 2025, 23, 1367–1378. [Google Scholar] [CrossRef]
- Hoeboer, S.H.; Groeneveld, A.B.J.; Engels, N.; van Genderen, M.; Wijnhoven, B.P.L.; van Bommel, J. Rising C-Reactive Protein and Procalcitonin Levels Precede Early Complications After Esophagectomy. J. Gastrointest. Surg. 2015, 19, 613–624. [Google Scholar] [CrossRef]
- Li, K.; Wang, K.; Wei, X.; Leng, X.; Fang, Q. Optimal Discharge Planning for Esophagectomy Patients with Enhanced Recovery after Surgery: Recommendations. Front. Surg. 2023, 10, 1112675. [Google Scholar] [CrossRef]
- Moyes, L.H.; Anderson, J.E.; Forshaw, M.J. Proposed Follow up Programme after Curative Resection for Lower Third Oesophageal Cancer. World J. Surg. Oncol. 2010, 8, 75. [Google Scholar] [CrossRef]
- Collard, J.M.; Otte, J.B.; Reynaert, M.; Kestens, P.J. Quality of Life Three Years or More after Esophagectomy for Cancer. J. Thorac. Cardiovasc. Surg. 1992, 104, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Then, E.O.; Lopez, M.; Saleem, S.; Gayam, V.; Sunkara, T.; Culliford, A.; Gaduputi, V. Esophageal Cancer: An Updated Surveillance Epidemiology and End Results Database Analysis. World J. Oncol. 2020, 11, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Gisbertz, S.S.; Hagens, E.R.C.; Ruurda, J.P.; Schneider, P.M.; Tan, L.J.; Domrachev, S.A.; Hoeppner, J.; van Berge Henegouwen, M.I. The Evolution of Surgical Approach for Esophageal Cancer. Ann. N. Y. Acad. Sci. 2018, 1434, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.E.; DʼJourno, X.B.; Griffin, S.M.; Hölscher, A.H.; Hofstetter, W.L.; Jobe, B.A.; et al. International Consensus on Standardization of Data Collection for Complications Associated with Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann. Surg. 2015, 262, 286–294. [Google Scholar] [CrossRef]
- Perroni, G.; Johnson, C.; Khandhar, S.; Veronesi, G.; Ambrogi, V.; Fernando, H.C. Implementation of Eras for Patients Undergoing Esophagectomy: A Narrative Review of the Current Literature and Latest Evidence. Curr. Chall. Thorac. Surg. 2021, 3. [Google Scholar] [CrossRef]
- Janssen, T.; Fransen, L.; Heesakkers, F.; Dolmans-Zwartjes, A.; Moorthy, K.; Nieuwenhuijzen, G.; Luyer, M. Effect of a Multimodal Prehabilitation Program on Postoperative Recovery and Morbidity in Patients Undergoing a Totally Minimally Invasive Esophagectomy. Dis. Esophagus 2021, 35, doab082. [Google Scholar] [CrossRef]
- Golder, H.J.; Papalois, V. Enhanced Recovery after Surgery: History, Key Advancements and Developments in Transplant Surgery. J. Clin. Med. 2021, 10, 1634. [Google Scholar] [CrossRef]
- Ashok, A.; Niyogi, D.; Ranganathan, P.; Tandon, S.; Bhaskar, M.; Karimundackal, G.; Jiwnani, S.; Shetmahajan, M.; Pramesh, C.S. The Enhanced Recovery after Surgery (ERAS) Protocol to Promote Recovery Following Esophageal Cancer Resection. Surg. Today 2020, 50, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Grimminger, P.P. Enhanced Recovery After Surgery (ERAS) for Esophagectomy: A Paradigm Shift in Perioperative Care. Ann. Surg. Oncol. 2024, 31, 8504–8505. [Google Scholar] [CrossRef] [PubMed]
- Geroin, C.; Weindelmayer, J.; Camozzi, S.; Leone, B.; Turolo, C.; Bencivenga, M.; Sacco, M.; De Pasqual, C.A.; Vedovi, E.; Priolo, S.; et al. Association between ERAS Protocol and Major Postoperative Complications and Reasons for Non-Compliance in Patients with Esophageal Cancer. Eur. J. Surg. Oncol. 2025, 51, 109707. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, O.; Anestiadou, E.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; Kocián, P.; et al. The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol for Acute Appendicitis: Recommendations for Perioperative Care. J. Clin Med. 2024, 13, 6943. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ioannidis, O.; Koltsida, A.; Anestiadou, E.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; et al. Recommendations for Perioperative Care in Liver Resection: The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol. Medicina 2025, 61, 978. [Google Scholar] [CrossRef]
- Busweiler, L.A.D.; Wijnhoven, B.P.L.; van Berge Henegouwen, M.I.; Henneman, D.; van Grieken, N.C.T.; Wouters, M.W.J.M.; van Hillegersberg, R.; van Sandick, J.W. Early Outcomes from the Dutch Upper Gastrointestinal Cancer Audit. Br. J. Surg. 2016, 103, 1855–1863. [Google Scholar] [CrossRef]
- Ebrahimian, S.; Chervu, N.; Hadaya, J.; Cho, N.Y.; Kronen, E.; Sakowitz, S.; Verma, A.; Bakhtiyar, S.S.; Sanaiha, Y.; Benharash, P. National Outcomes of Expedited Discharge Following Esophagectomy for Malignancy. PLoS ONE 2024, 19, e0297470. [Google Scholar] [CrossRef]
- Altman, A.D.; Helpman, L.; McGee, J.; Samouëlian, V.; Auclair, M.-H.; Brar, H.; Nelson, G.S. Enhanced Recovery after Surgery: Implementing a New Standard of Surgical Care. Cmaj 2019, 191, E469–E475. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aspect | Standard ERAS Protocol | EUPEMEN Protocol |
|---|---|---|
| Scope of Application | Globally oriented recommendations with broadly applicable care pathways | Adapted to the European context with procedure-specific protocols tailored for regional and institutional diversity |
| Development Process | Formulated through international expert consensus led by surgical societies | Developed via a collaborative European network with input from multiple disciplines and clinical experience |
| Procedure Specificity | Offers adaptable general principles across surgeries | Provides detailed, operation-specific protocols (e.g., for liver, gastric, bowel, emergency cases) |
| Implementation Tools | Primarily guideline documents and clinical flowcharts | Includes digital tools, multilingual resources, structured training programs, and routine auditing practices |
| Target Audience | Focuses on surgical and anesthetic perioperative teams | Involves full care teams—surgeons, anesthesiologists, dietitians, nurses, physiotherapists, and general practitioners |
| Barriers Addressed | Acknowledges implementation challenges but offers limited practical solutions | Actively addresses cultural, administrative, and logistical barriers to adoption through adaptable strategies |
| Monitoring and Sustainability | Inconsistently applied; auditing often lacking or optional | Built-in monitoring tools and regular audits ensure continuous feedback and protocol adherence |
| Patient Engagement | Encouraged but implemented variably across institutions | Includes standardized educational materials, structured counseling, and shared decision-making processes |
| Aim | To support enhanced recovery and reduce hospital length of stay | To harmonize perioperative practice in Europe, improve outcomes, and optimize use of healthcare resources |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannidis, O.; Anestiadou, E.; Koltsida, A.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; et al. Optimizing Perioperative Care in Esophageal Surgery: The EUropean PErioperative MEdical Networking (EUPEMEN) Collaborative for Esophagectomy. Diseases 2025, 13, 231. https://doi.org/10.3390/diseases13080231
Ioannidis O, Anestiadou E, Koltsida A, Ramirez JM, Fabbri N, Ubieto JM, Feo CV, Pesce A, Rosetzka K, Arroyo A, et al. Optimizing Perioperative Care in Esophageal Surgery: The EUropean PErioperative MEdical Networking (EUPEMEN) Collaborative for Esophagectomy. Diseases. 2025; 13(8):231. https://doi.org/10.3390/diseases13080231
Chicago/Turabian StyleIoannidis, Orestis, Elissavet Anestiadou, Angeliki Koltsida, Jose M. Ramirez, Nicolò Fabbri, Javier Martínez Ubieto, Carlo Vittorio Feo, Antonio Pesce, Kristyna Rosetzka, Antonio Arroyo, and et al. 2025. "Optimizing Perioperative Care in Esophageal Surgery: The EUropean PErioperative MEdical Networking (EUPEMEN) Collaborative for Esophagectomy" Diseases 13, no. 8: 231. https://doi.org/10.3390/diseases13080231
APA StyleIoannidis, O., Anestiadou, E., Koltsida, A., Ramirez, J. M., Fabbri, N., Ubieto, J. M., Feo, C. V., Pesce, A., Rosetzka, K., Arroyo, A., Kocián, P., Sánchez-Guillén, L., Bellosta, A. P., Whitley, A., Enguita, A. B., Teresa-Fernandéz, M., Bitsianis, S., & Symeonidis, S. (2025). Optimizing Perioperative Care in Esophageal Surgery: The EUropean PErioperative MEdical Networking (EUPEMEN) Collaborative for Esophagectomy. Diseases, 13(8), 231. https://doi.org/10.3390/diseases13080231