
Functional Status in Elderly Kidney Transplant Recipients: A Systematic Review Evaluating Physical Function, Frailty, and Cognitive Impairment as Predictors of Post-Transplant Outcomes

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Collection and Presentation
2.3. Quality Appraisal
2.4. Ethics Approval and Role of Funders
3. Results
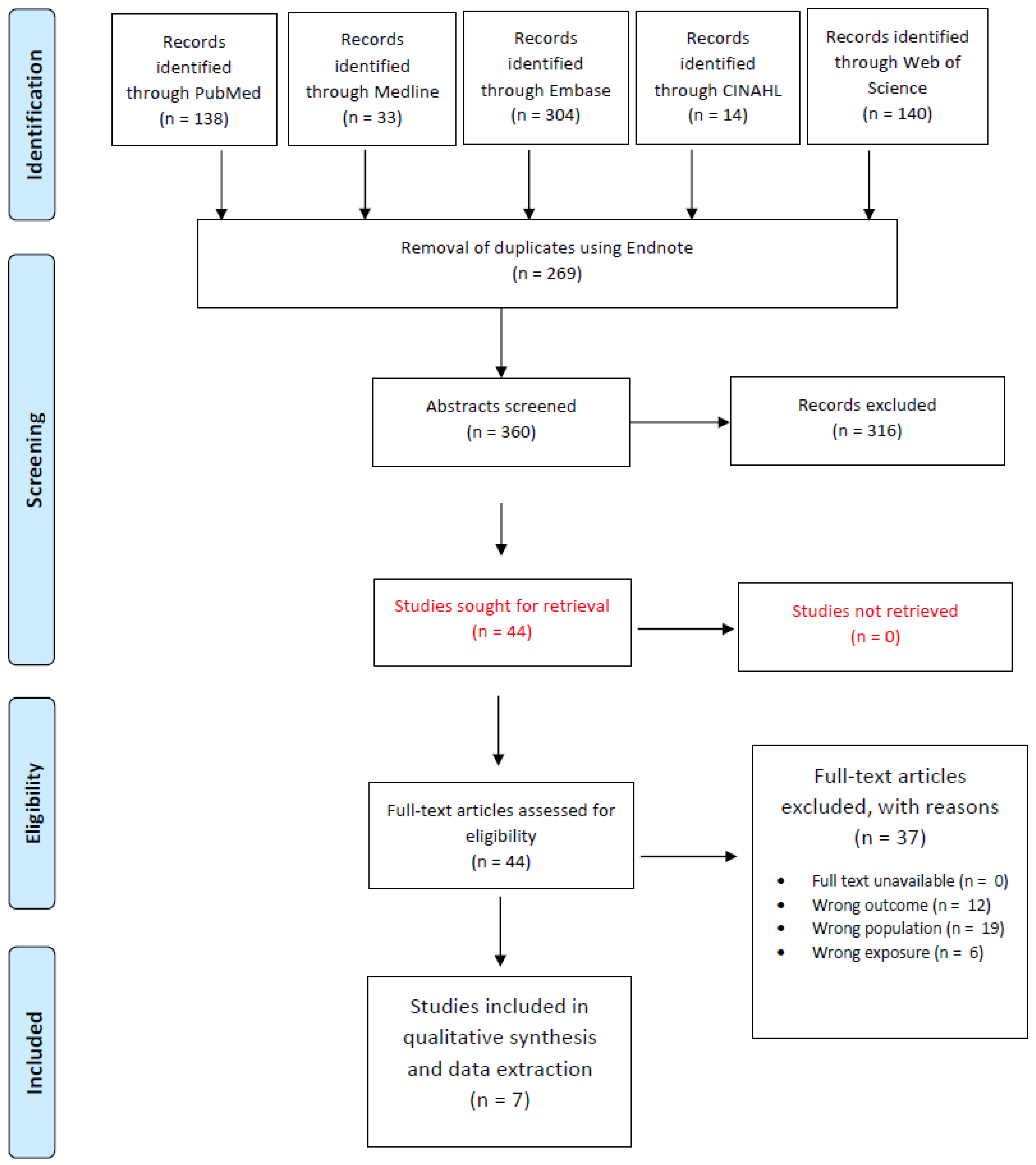
3.1. Literature Search
3.2. Quality Assessment
3.3. Overview of Findings
3.3.1. Physical Function and Post-Transplant Outcomes
3.3.2. Frailty as a Predictor of Transplant Outcomes
3.3.3. Cognitive Function and Transplant Outcomes
4. Discussion
4.1. Physical Function and Post-Transplant Outcomes
4.2. Frailty and Post-Transplant Outcomes
4.3. Cognitive Impairment and Post-Transplant Outcomes
4.4. Clinical and Public Health Implications
4.5. Strengths and Limitations
4.6. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United States Renal Data System (USRDS). 2024 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. Am. J. Kidney Dis. 2025, 85, S1–S565. Available online: https://usrds-adr.niddk.nih.gov/2024 (accessed on 20 January 2025).
- Organ Procurement and Transplantation Network (OPTN) 2025 National Data, U.S. Department of Health and Human Services. Available online: https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/ (accessed on 20 January 2025).
- Centers for Medicare; Medicaid Services. 2025 ESRD Treatment Choices Model, U.S. Department of Health and Human Services. Available online: https://www.cms.gov/priorities/innovation/innovation-models/esrd-treatment-choices-model (accessed on 20 January 2025).
- International Society of Nephrology-Global Kidney Health Atlas. Available online: https://www.theisn.org/in-action/research/global-kidney-health-atlas/ (accessed on 20 June 2025).
- Noordzij, M.; Jager, K.J.; van der Veer, S.N.; Kramar, R.; Collart, F.; Heaf, J.G.; Stojceva-Taneva, O.; Leivestad, T.; Buturovic-Ponikvar, J.; Benítez Sánchez, M.; et al. Use of vascular access for haemodialysis in Europe: A report from the ERA-EDTA Registry. Nephrol. Dial. Transplant. 2014, 29, 1956–1964. [Google Scholar] [CrossRef] [PubMed]
- ERA Registry Annual Report. 2025. Available online: https://www.era-online.org/wp-content/uploads/2025/05/AnnRep22_250507_1500.pdf?_gl=1*dt2g7z*_up*MQ..*_ga*MjUwNjQ2NDk1LjE3NTA5MTQ0NjY.*_ga_EKLMSCV50T*czE3NTA5MTQ0NjIkbzEkZzAkdDE3NTA5MTQ0ODgkajM0JGwwJGgw (accessed on 20 June 2025).
- Heaf, J. Current trends in European renal epidemiology. Clin. Kidney J. 2017, 10, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C.; Podestà, M.A.; Graziani, G. Renal transplantation in elderly patients. How to select the candidates to the waiting list? Transplant. Rev. 2014, 28, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Kodali, L.; Turner, A. When are you too old to get a kidney transplants? Curr. Opin. Nephrol. Hypertens. 2019, 28, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, S.; Long, A.; Zhang, H.; Monaghan, C.; Larkin, J.W.; Kotanko, P.; Kalaskar, S.; Kooman, J.P.; van der Sande, F.M.; Maddux, F.W.; et al. Artificial intelligence enabled applications in kidney disease. Semin. Dial. 2021, 34, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, Y.; Hirakawa, Y.; Nangaku, M. Telemedicine in nephrology: Future perspective and solutions. Clin. Kidney J. 2024, 17 (Suppl. S2), ii1–ii8. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.S.N.; Brown, E.A.; Cheung, M.; Figueiredo, A.E.; Hurst, H.; King, J.M.; Mehrotra, R.; Pryor, L.; Walker, R.C.; Wasylynuk, B.A.; et al. The Role of Nephrology Nurses in Symptom Management–Reflections on the Kidney Disease: Improving Global Outcomes Controversies Conference on Symptom-Based Complications in Dialysis Care. Kidney Int. Rep. 2023, 8, 1903–1906. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, C.; Malvica, S.; Cesari, M.; Vettoretti, S.; Benedetti, M.; Cicero, E.; Miglio, R.; Caldiroli, L.; Perna, A.; Cervesato, A.; et al. Frailty in kidney transplantation: A review on its evaluation, variation and long-term impact. Clin. Kidney J. 2022, 15, 2020–2026. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.G.; Ruck, J.M.; Shaffer, A.A.; Haugen, C.E.; Ying, H.; Warsame, F.; Chu, N.; Carlson, M.C.; Gross, A.L.; Norman, S.P.; et al. Kidney Transplant Outcomes in Recipients With Cognitive Impairment: A National Registry and Prospective Cohort Study. Transplantation 2019, 103, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Basu, A. Role of Physical Performance Assessments and Need for a Standardized Protocol for Selection of Older Kidney Transplant Candidates. Kidney Int. Rep. 2019, 4, 1666–1676. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; Volume 2, pp. 1–12. [Google Scholar]
- Brar, A.; Gruessner, A.; Adey, D.; Tedla, F.; Yap, E.; Kaul, D.; Sumrani, N.; John, D.; Salifu, M.O. Association of Physical Function and Survival in Older-Adult Renal Transplant Recipients. Transplant. Proc. 2021, 53, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Tsarpali, V.M.; Midtvedt, K.; Lønning, K.; Bernklev, T.D.; Åsberg, A.; Fawad, H.M.; von der Lippe, N.; Reisæter, A.V.; Røysland, K.; Heldal, K. A Comorbidity Index and Pretransplant Physical Status Predict Survival in Older Kidney Transplant Recipients: A National Prospective Study. Transplant. Direct 2022, 8, e1307. [Google Scholar] [CrossRef] [PubMed]
- Reese, P.P.; Bloom, R.D.; Shults, J.; Thomasson, A.; Mussell, A.; Rosas, S.E.; Johansen, K.L.; Abt, P.; Levine, M.; Caplan, A.; et al. Functional status and survival after kidney transplantation. Transplantation 2014, 97, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Tsarpali, V.M.; Midtvedt, K.; Lønning, K.; Bernklev, T.D.; Åsberg, A.; von der Lippe, N.; Reisæter, A.V.; Heldal, K. Poor Physical Function Trajectory Predicts Impaired Patient Survival in Older Recipients of Deceased Donor Kidneys: A Prospective Cohort Study. Transplant. Direct 2022, 8, e1374. [Google Scholar] [CrossRef] [PubMed]
- Nastasi, A.J.; McAdams-DeMarco, M.A.; Schrack, J.; Ying, H.; Olorundare, I.; Warsame, F.; Mountford, A.; Haugen, C.E.; Fernández, M.G.; Norman, S.P.; et al. Pre-Kidney Transplant Lower Extremity Impairment and Post-Kidney Transplant Mortality. Am. J. Transplant. 2018, 18, 189–196. [Google Scholar] [CrossRef] [PubMed]
- McAdams-DeMarco, M.A.; Law, A.; King, E.; Orandi, B.; Salter, M.; Gupta, N.; Chow, E.; Alachkar, N.; Desai, N.; Varadhan, R.; et al. Frailty and Mortality in Kidney Transplant Recipients. Am. J. Transplant. 2015, 15, 149–154. [Google Scholar] [CrossRef] [PubMed]
- McAdams-DeMarco, M.A.; Olorundare, I.O.; Ying, H.; Warsame, F.; Haugen, C.E.; Hall, R.; Garonzik-Wang, J.M.; Desai, N.M.; Walston, J.D.; Norman, S.P.; et al. Frailty and Postkidney Transplant Health-Related Quality of Life. Transplantation 2018, 102, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Golenia, A.; Malyszko, J.S.; Malyszko, J. Cognitive Impairment and Kidney Transplantation: Underestimated, Underrecognized but Clinically Relevant Problem. Kidney Blood Press. Res. 2022, 47, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Quint, E.E.; Ferreira, M.; van Munster, B.C.; Nieuwenhuijs-Moeke, G.; Velde-Keyzer, C.T.; Bakker, S.J.L.; Annema, C.; Mathur, S.; Pol, R.A. Prehabilitation in Adult Solid Organ Transplant Candidates. Curr. Transplant. Rep. 2023, 10, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Mina, D.S.; Scheede-Bergdahl, C.; Gillis, C.; Carli, F. Optimization of surgical outcomes with prehabilitation. Appl. Physiol. Nutr. Metab. 2015, 40, 966–969. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; De Asteasu, M.L.S.; Morley, J.E.; Cano-Gutierrez, C.A.; Izquierdo, M. Performance of the Short Physical Performance Battery in Identifying the Frailty Phenotype and Predicting Geriatric Syndromes in Community-Dwelling Elderly. J. Nutr. Health Aging 2021, 25, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xie, L.; Guo, R.; Wang, J.; Lin, J.; Sun, Z.; Duan, S.; Lin, Z.; Li, H.; Ma, S. Abnormal brain activity patterns during spatial working memory task in patients with end-stage renal disease on maintenance hemodialysis: A fMRI study. Brain Imaging Behav. 2021, 15, 1898–1911. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Jiao, Z.; Dai, J.; Liu, T.; Shi, H. Abnormal cerebral micro-structures in end-stage renal disease patients related to mild cognitive impairment. Eur. J. Radiol. 2022, 157, 110597. [Google Scholar] [CrossRef] [PubMed]
- Yamagata, K.; Hoshino, J.; Sugiyama, H.; Hanafusa, N.; Shibagaki, Y.; Komatsu, Y.; Konta, T.; Fujii, N.; Kanda, E.; Sofue, T.; et al. Clinical practice guideline for renal rehabilitation: Systematic reviews and recommendations of exercise therapies in patients with kidney diseases. Ren. Replace. Ther. 2019, 5, 4. [Google Scholar] [CrossRef]

{kind=link}
| Author(s) | Year | Country | Study Design | Sample Size (Kidney Transplant Recipients) | Age Range | Mean Age | % of Recipients Were Aged ≥65 Years | % Gender Distribution (% Women) | Number of Participants on Dialysis | Time on Dialysis | Participants Not Yet on Dialysis at the Time of Evaluation | Median Follow-Up Time Post-Transplant |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reese et al. [20] | 2014 | U.S. | observational study (retrospective cohort study) | 10,875 | 50 | 14 | 37 | 10,875 | >1 years | 0 | 1631 days | |
| Brar et al. [18] | 2021 | U.S. | observational study (retrospective cohort study) | 26,721 | 65 to 96 | 100 | 37 | 21,427 | 5226 | |||
| Nastasi et al. [22] | 2018 | U.S. | observational study (prospective, two-center, longitudinal study) | 719 | 18.7 to 86.0 yrs | 51.6 (SD = 14.2) | 20 | 38 | 581 | 138 | 2 years | |
| Tsarpali et al. [19] | 2022 | Norway | observational study (prospective, single-center, longitudinal study) | 192 | 65 to 84 yrs | 72.1 (SD = 4.1) | 100 | 31 | 145 | median = 27.5 months (17.6–43.2 months) | 47 | 4.6 years |
| Tsarpali et al. * [21] | 2022 | Norway | observational study (prospective, single-center, longitudinal study) | 181 | 65 to 84 yrs | 72 | 100 | 31 | median = 27.4 months (17.3–43.2 months) | 4.9 years |
| Author(s) | Year | Physical Function Assessment Method | Benefits | Limitations |
|---|---|---|---|---|
| Reese et al. [20] | 2014 | Physical Function (PF) Subscale of the Medical Outcomes Study Short Form-36 (SF-36) questionnaire | SF-36 has been validated for use in elderly patients and dialysis patients | PF scale is a subjective, self-reported measure |
| Continuous measure that classifies patients over a spectrum of severity | ||||
| Brar et al. [18] | 2021 | Level of assistance (total assistance, moderate assistance, no assistance) | A straightforward categorization of physical status | A classification system is relatively crude |
| Nastasi et al. [22] | 2018 | Short Physical Performance Battery (SPPB) | Objective assessment of lower extremity function | Focuses on lower extremity function |
| Well-validated physical assessment tool | May not capture the full spectrum of physical function | |||
| Test takes approximately 5 to 10 min to complete | ||||
| Tsarpali et al. [19] | 2022 | Kidney Disease Quality of Life Short Form, version 1.3 (KDQOL-SF v1.3) | Relatively straightforward to administer and score | All HRQOL data are self-reported and may be subjected to bias |
| Tsarpali et al. * [21] | 2022 | Captures the patient’s perspective on their physical function and QoL |
| Author(s) | Year | Primary Outcome | Primary Exposure | Main Finding for Subgroup >65 Years of Age |
|---|---|---|---|---|
| Reese et al. [20] | 2014 | Patient survival after transplantation | Pre-transplant Physical Function (PF) score | Functional status predicted survival across all age groups, but recipients aged ≥65 years had the greatest risk difference between low and high PF quartiles |
| Brar et al. [18] | 2021 | Patient survival after transplantation | Assistance level, classified into 3 groups | Patient survival was significantly higher in recipients who needed no assistance and lowest in patients in need of total assistance |
| Nastasi et al. [22] | 2018 | Post-kidney transplant mortality | Short Physical Performance Battery (SPPB) score | Compared to younger unimpaired recipients, older impaired recipients (≥65 years) had a 2.60-fold higher risk of post-KT mortality |
| Tsarpali et al. [19] | 2022 | Patient survival after transplantation | Health-related quality of life, with a focus on the physical function component | A PF score ≤ 60 was associated with a 2-fold increase in mortality risk |
| Tsarpali et al. * [21] | 2022 | Patient survival after transplantation | Longitudinal HRQOL trajectories during the first post-KT year, particularly PF domain | Older recipients who experienced a poor PF trajectory during the first post-KT year had a 2.4 times higher mortality risk compared to those with a good PF trajectory |
| Author(s) | Year | Country | Study Design | Sample Size (Kidney Transplant Recipients) | Age Range | Mean Age | % of Recipients Were Aged ≥65 Years | % Gender Distribution (% women) | Number of Participants on Dialysis | Time on Dialysis | Participants Not Yet on Dialysis at the Time of Evaluation | Median Follow-Up Time Post-Transplant |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| McAdams-DeMarco et al. [23] | 2015 | U.S. | observational study (prospective, single-center, longitudinal study) | 537 | 53 (SD = 14.0) | 40 | 2.7 years | |||||
| McAdams-DeMarco et al. [24] | 2018 | U.S. | observational study (prospective, two-center, longitudinal study) | 443 | 19.9 to 86.0 yrs | 52 (SD = 14.1) | 37 | 379 | Median = 3.26 years | 64 | 7.7 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araji, H.; Al-Ajlouni, Y.A.; Nusier, J.; Sange, W.; El-Charabaty, E.; El-Sayegh, S. Functional Status in Elderly Kidney Transplant Recipients: A Systematic Review Evaluating Physical Function, Frailty, and Cognitive Impairment as Predictors of Post-Transplant Outcomes. Diseases 2025, 13, 229. https://doi.org/10.3390/diseases13070229
Araji H, Al-Ajlouni YA, Nusier J, Sange W, El-Charabaty E, El-Sayegh S. Functional Status in Elderly Kidney Transplant Recipients: A Systematic Review Evaluating Physical Function, Frailty, and Cognitive Impairment as Predictors of Post-Transplant Outcomes. Diseases. 2025; 13(7):229. https://doi.org/10.3390/diseases13070229
Chicago/Turabian StyleAraji, Hachem, Yazan A. Al-Ajlouni, Jana Nusier, Walid Sange, Elie El-Charabaty, and Suzanne El-Sayegh. 2025. "Functional Status in Elderly Kidney Transplant Recipients: A Systematic Review Evaluating Physical Function, Frailty, and Cognitive Impairment as Predictors of Post-Transplant Outcomes" Diseases 13, no. 7: 229. https://doi.org/10.3390/diseases13070229
APA StyleAraji, H., Al-Ajlouni, Y. A., Nusier, J., Sange, W., El-Charabaty, E., & El-Sayegh, S. (2025). Functional Status in Elderly Kidney Transplant Recipients: A Systematic Review Evaluating Physical Function, Frailty, and Cognitive Impairment as Predictors of Post-Transplant Outcomes. Diseases, 13(7), 229. https://doi.org/10.3390/diseases13070229