
Plasma Matrix Metalloproteinases Signature as Biomarkers for Pediatric Tuberculosis Diagnosis: A Prospective Case–Control Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Population and Procedures
2.2. Metalloproteinase Assays
2.3. Statistical Analysis
3. Results
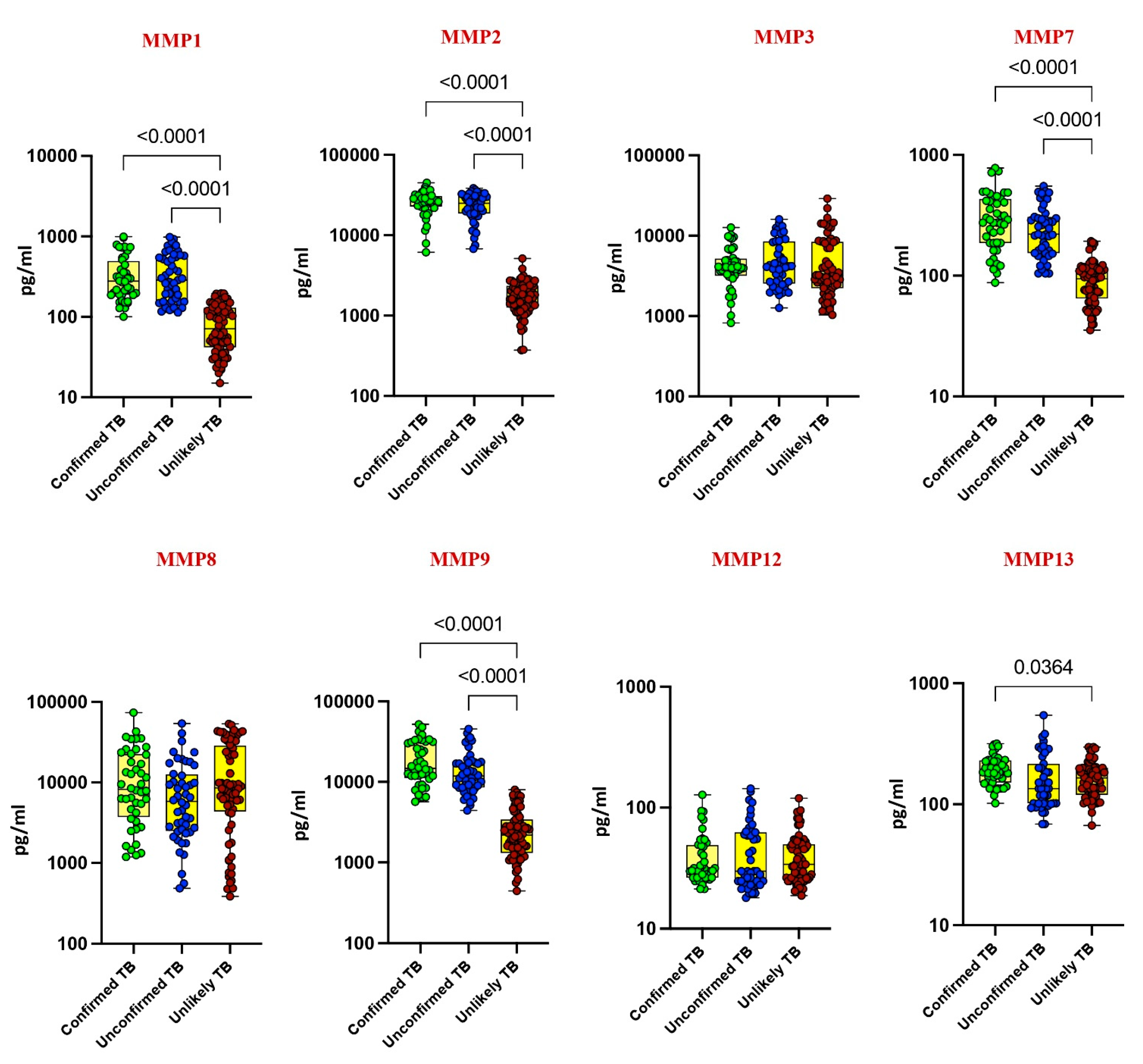
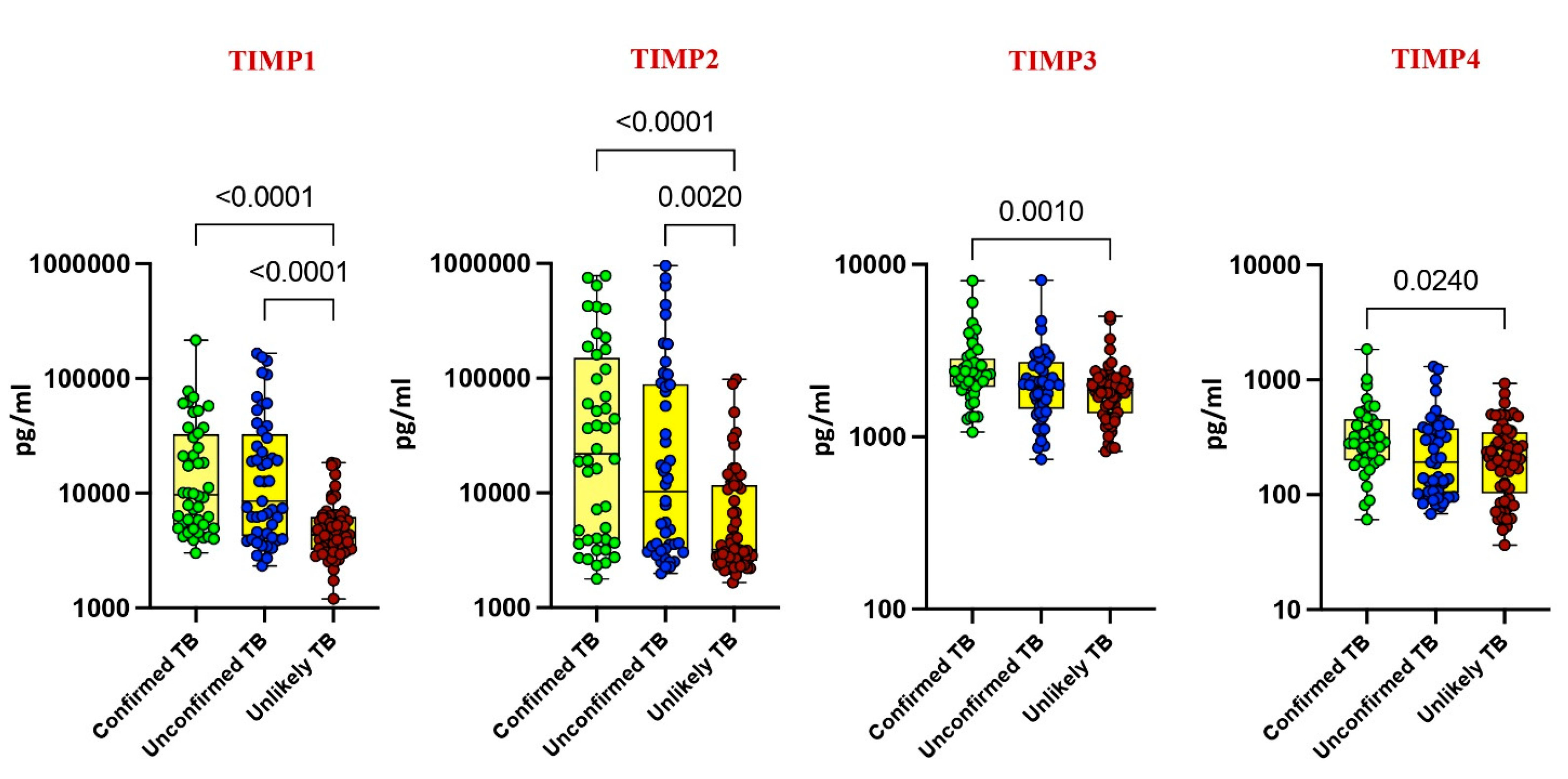
3.1. Elevated Plasma Levels of MMPs and TIMPs in Pediatric TB
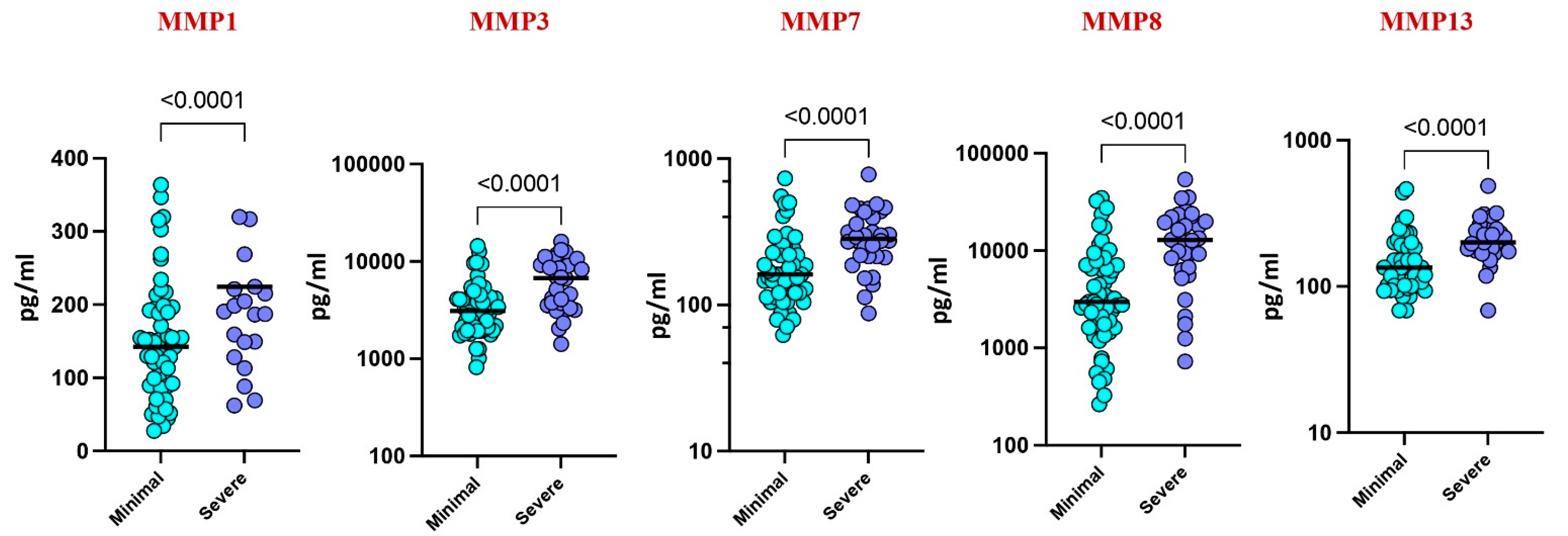
3.2. Plasma MMPs Associated with Disease Severity
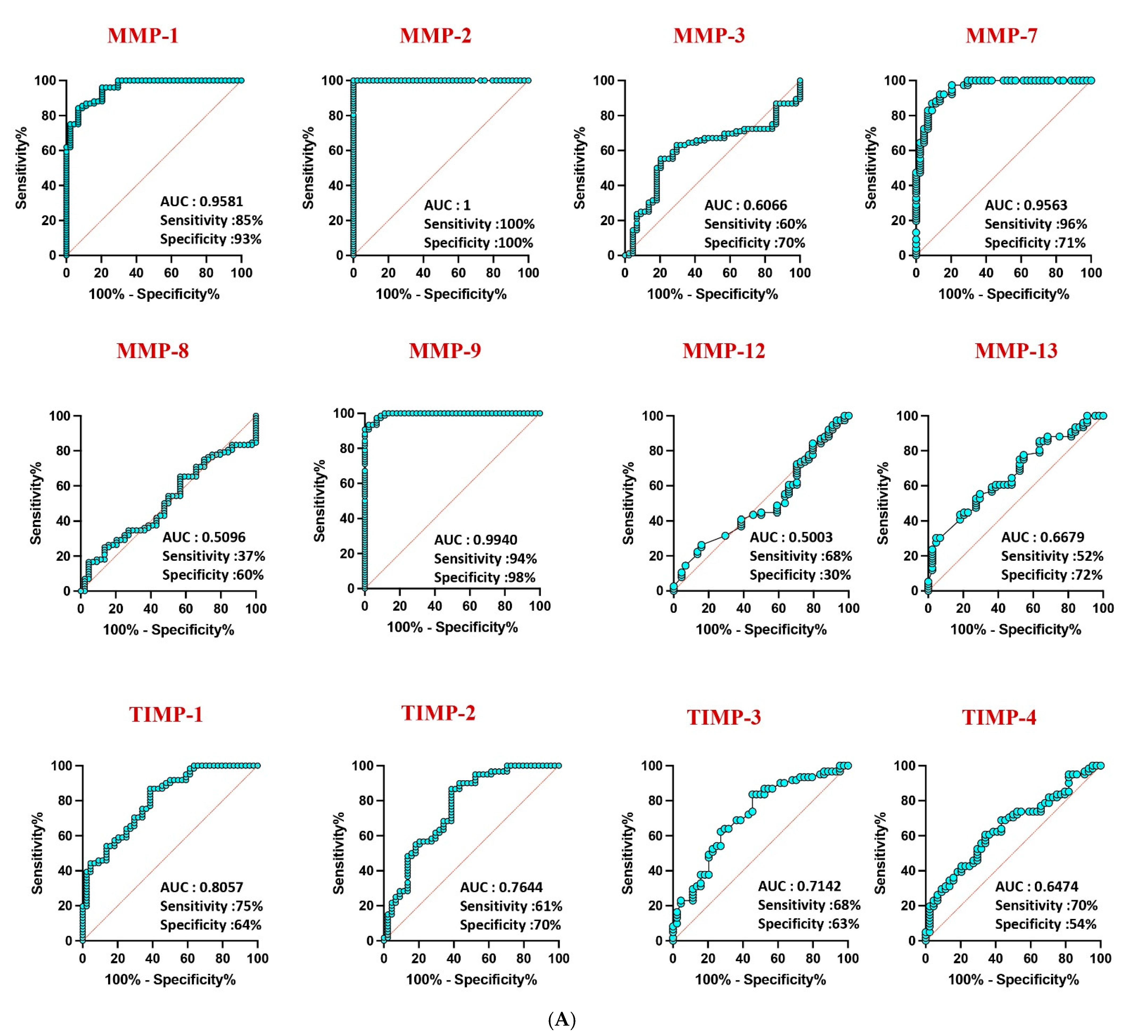
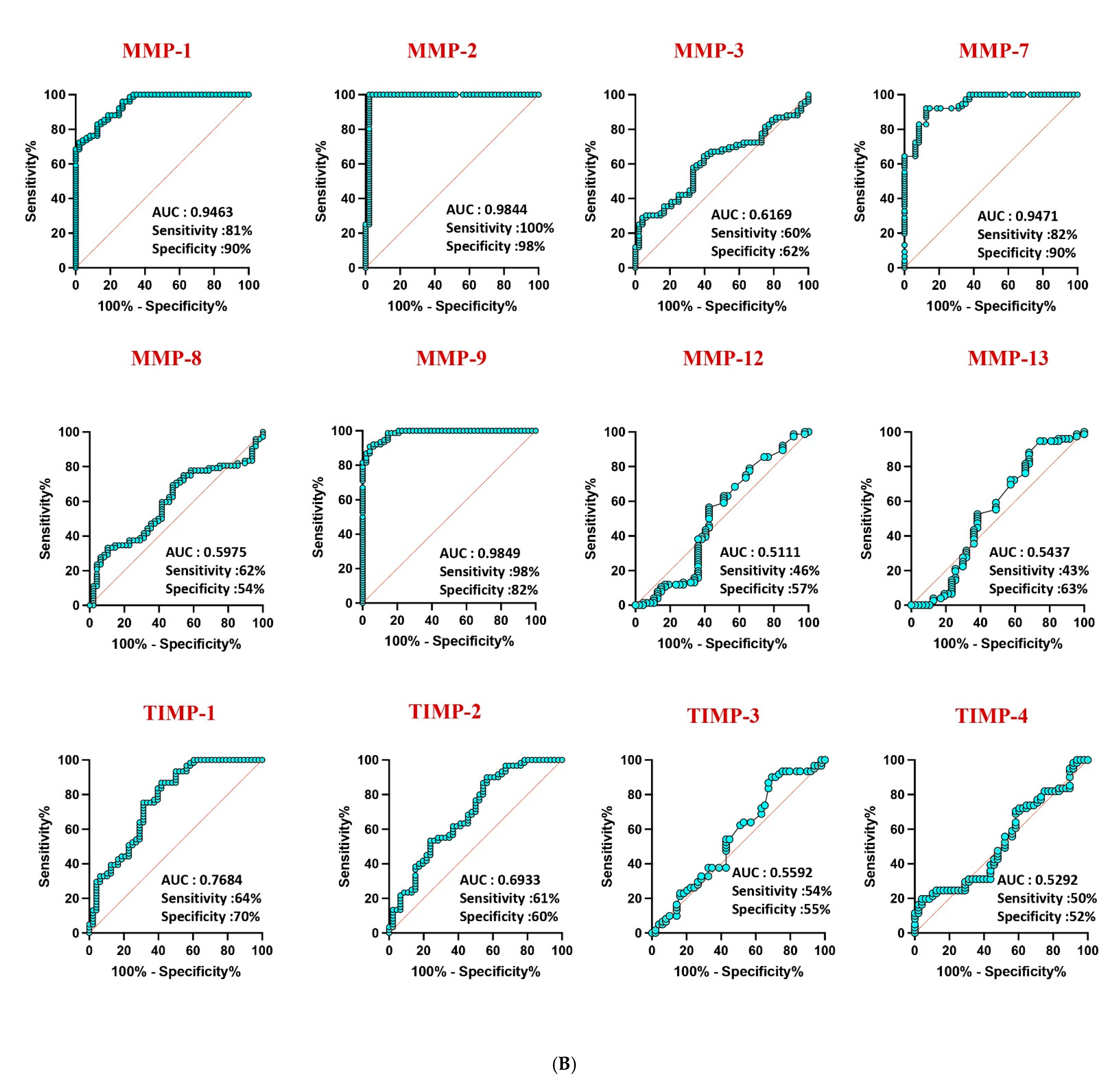
3.3. MMPs as Discriminatory Markers
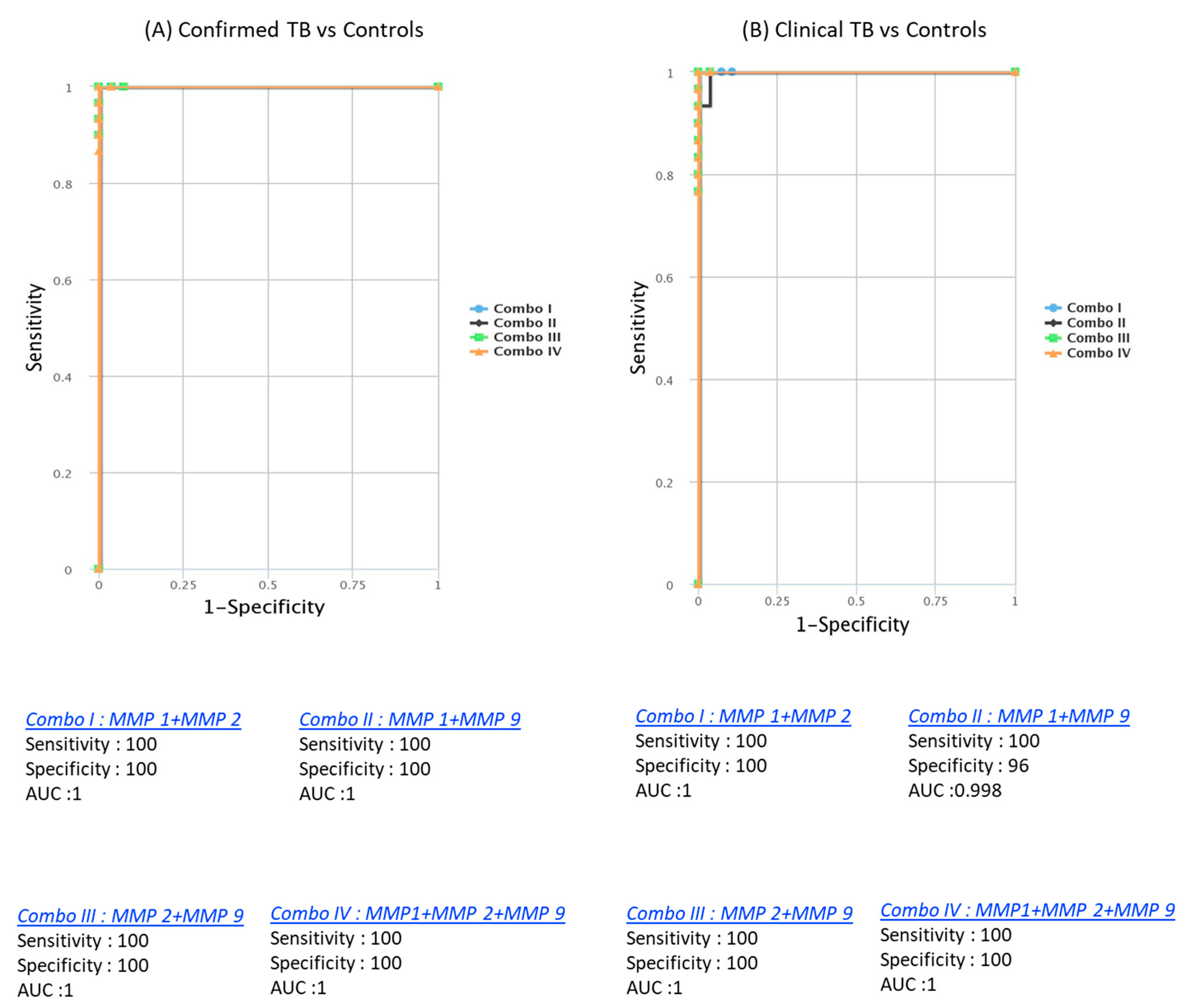
3.4. Enhanced Discrimination with Biomarker Combinations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dye, C.; Scheele, S.; Dolin, P.; Pathania, V.; Raviglione, M.C. Consensus statement. Global burden of tuberculosis: Estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA 1999, 282, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Newton, S.M.; Brent, A.J.; Anderson, S.; Whittaker, E.; Kampmann, B. Paediatric tuberculosis. Lancet Infect. Dis. 2008, 8, 498–510. [Google Scholar] [CrossRef]
- Boehme, C.C.; Nicol, M.P.; Nabeta, P.; Michael, J.S.; Gotuzzo, E.; Tahirli, R.; Gler, M.T.; Blakemore, R.; Worodria, W.; Gray, C.; et al. Feasibility, diagnostic accuracy, and effectiveness of decentralised use of the Xpert MTB/RIF test for diagnosis of tuberculosis and multidrug resistance: A multicentre implementation study. Lancet 2011, 377, 1495–1505. [Google Scholar] [CrossRef]
- Craig, V.J.; Zhang, L.; Hagood, J.S.; Owen, C.A. Matrix metalloproteinases as therapeutic targets for idiopathic pulmonary fibrosis. Am. J. Respir. Cell Mol. Biol. 2015, 53, 585–600. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.L.; Hattle, J.M.; Dreitz, S.A.; Troudt, J.M.; Izzo, L.S.; Basaraba, R.J.; Orme, I.M.; Matrisian, L.M.; Izzo, A.A. Role for matrix metalloproteinase 9 in granuloma formation during pulmonary Mycobacterium tuberculosis infection. Infect. Immun. 2006, 74, 6135–6144. [Google Scholar] [CrossRef] [PubMed]
- Brew, K.; Nagase, H. The tissue inhibitors of metalloproteinases (TIMPs): An ancient family with structural and functional diversity. Biochim. Biophys. Acta BBA Mol. Cell Res. 2010, 1803, 55–71. [Google Scholar] [CrossRef]
- Albuquerque, V.V.; Kumar, N.P.; Fukutani, K.F.; Vasconcelos, B.; Arriaga, M.B.; Silveira-Mattos, P.S.; Babu, S.; Andrade, B.B. Plasma levels of C-reactive protein, matrix metalloproteinase-7 and lipo-polysaccharide-binding protein distinguish active pulmonary or extrapulmonary tuberculosis from uninfected controls in children. Cytokine 2019, 123, 154773. [Google Scholar] [CrossRef]
- Kumar, N.P.; Anuradha, R.; Andrade, B.B.; Suresh, N.; Ganesh, R.; Shankar, J.; Kumaraswami, V.; Nutman, T.B.; Babu, S. Circulating biomarkers of pulmonary and extrapulmonary tuberculosis in Children. Clin. Vaccine Immunol. 2013, 20, 704–711. [Google Scholar] [CrossRef]
- Kumar, N.P.; Moideen, K.; Viswanathan, V.; Shruthi, B.S.; Sivakumar, S.; Menon, P.A.; Kornfeld, H.; Babu, S. Elevated levels of matrix metalloproteinases reflect severity and extent of disease in tuberculosis-diabetes co-morbidity and are predominantly reversed following standard anti-tuberculosis or metformin treatment. BMC Infect. Dis. 2018, 18, 345. [Google Scholar] [CrossRef]
- Kumar, N.P.; Moideen, K.; Nancy, A.; Viswanathan, V.; Thiruvengadam, K.; Sivakumar, S.; Hissar, S.; Nair, D.; Banurekha, V.V.; Kornfeld, H.; et al. Association of Plasma Matrix Metalloproteinase and Tissue Inhibitors of Matrix Metalloproteinase Levels With Adverse Treatment Outcomes Among Patients With Pulmonary Tuberculosis. JAMA Netw. Open 2020, 3, e2027754. [Google Scholar] [CrossRef]
- Graham, S.M.; Cuevas, L.E.; Jean-Philippe, P.; Browning, R.; Casenghi, M.; Detjen, A.K.; Gnanashanmugam, D.; Hesseling, A.C.; Kampmann, B.; Mandalakas, A.; et al. Clinical Case Definitions for Classification of Intrathoracic Tuberculosis in Chil-dren: An Update. Clin. Infect. Dis. 2015, 61 (Suppl. S3), S179–S187. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.P.; Hissar, S.; Thiruvengadam, K.; Banurekha, V.V.; Balaji, S.; Elilarasi, S.; Gomathi, N.S.; Ganesh, J.; Aravind, M.A.; Baskaran, D.; et al. Plasma chemokines as immune biomarkers for diagnosis of pediatric tuberculosis. BMC Infect. Dis. 2021, 21, 1055. [Google Scholar] [CrossRef]
- Kumar, N.P.; Hissar, S.; Thiruvengadam, K.; Banurekha, V.V.; Suresh, N.; Shankar, J.; Elilarasi, S.; Gomathi, N.S.; Kalpana, S.; Ganesh, J.; et al. Discovery and Validation of a Three-Cytokine Plasma Signature as a Biomarker for Diagnosis of Pediatric Tuberculosis. Front. Immunol. 2021, 12, 653898. [Google Scholar] [CrossRef] [PubMed]
- Dodd, P.J.; Sismanidis, C.; A Seddon, J. Global burden of drug-resistant tuberculosis in children: A mathematical modelling study. Lancet Infect. Dis. 2016, 16, 1193–1201. [Google Scholar] [CrossRef]
- Chiang, S.S.; Khan, F.A.; Milstein, M.B.; Tolman, A.W.; Benedetti, A.; Starke, J.R.; Becerra, M.C. Treatment outcomes of childhood tuberculous meningitis: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 947–957. [Google Scholar] [CrossRef]
- Marais, B.J.; Gie, R.P.; Schaaf, H.S.; Hesseling, A.C.; Obihara, C.C.; Starke, J.J.; A Enarson, D.; Donald, P.R.; Beyers, N. The natural history of childhood intra-thoracic tuberculosis: A critical review of literature from the pre-chemotherapy era. Int. J. Tuberc. Lung Dis. 2004, 8, 392–402. [Google Scholar] [PubMed]
- Parrish, N.M.; Carroll, K.C. Role of the clinical mycobacteriology laboratory in diagnosis and management of tuberculosis in low-prevalence settings. J. Clin. Microbiol. 2011, 49, 772–776. [Google Scholar] [CrossRef]
- Ugarte-Gil, C.A.; Elkington, P.; Gilman, R.H.; Coronel, J.; Tezera, L.B.; Bernabe-Ortiz, A.; Gotuzzo, E.; Friedland, J.S.; Moore, D.A.J. Induced Sputum MMP-1, -3 & -8 Concentrations during Treatment of Tuberculosis. PLoS ONE 2013, 8, e61333. [Google Scholar] [CrossRef]
- Hoheisel, G.; Sack, U.; Hui, D.S.; Huse, K.; Chan, K.S.; Chan, K.K.; Hartwig, K.; Schuster, E.; Scholz, G.H.; Schauer, J. Occurrence of matrix metalloproteinases and tissue inhibitors of metalloproteinases in tu-berculous pleuritis. Tuberculosis 2001, 81, 203–209. [Google Scholar] [CrossRef]
- Hrabec, E.; Strek, M.; Zieba, M.; Kwiatkowska, S.; Hrabec, Z. Circulation level of matrix metalloproteinase-9 is correlated with disease severity in tuberculosis patients. Int. J. Tuberc. Lung Dis. 2002, 6, 713–719. [Google Scholar]
- Thuong, N.T.; Dunstan, S.J.; Chau, T.T.; Thorsson, V.; Simmons, C.P.; Quyen, N.T.; Thwaites, G.E.; Thi Ngoc Lan, N.; Hibberd, M.; Teo, Y.Y.; et al. Identification of tuberculosis susceptibility genes with human macrophage gene ex-pression profiles. PLoS Pathog. 2008, 4, e1000229. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-F.; Chu, S.-C.; Chiang, I.-C.; Kuo, W.-F.; Chiou, H.-L.; Chou, F.-P.; Kuo, W.-H.; Hsieh, Y.-S. Excessive matrix metalloproteinase-9 in the plasma of community-acquired pneumonia. Clin. Chim. Acta 2005, 352, 209–215. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | Confirmed TB | Unconfirmed TB | Unlikely TB |
|---|---|---|---|
| Number of subjects recruited | 44 | 47 | 76 |
| Gender (Male/Female) | 16/28 | 28/19 | 36/40 |
| Median Age (Range) (in years) | 7 (1–13) | 8 (1–12) | 6 (1–14) |
| Bacterial Burden: | 11/33/0 | 0/0/47 | - |
| High burden/Low burden/No burden | |||
| Tuberculin Skin Test: (Positive/Negative) | 32/16 | 35/12 | 45/31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavan Kumar, N.; Hissar, S.; Nancy, A.; Thiruvengadam, K.; Banurekha, V.V.; Balaji, S.; Elilarasi, S.; Gomathi, N.S.; Ganesh, J.; Aravind, M.A.; et al. Plasma Matrix Metalloproteinases Signature as Biomarkers for Pediatric Tuberculosis Diagnosis: A Prospective Case–Control Study. Diseases 2025, 13, 171. https://doi.org/10.3390/diseases13060171
Pavan Kumar N, Hissar S, Nancy A, Thiruvengadam K, Banurekha VV, Balaji S, Elilarasi S, Gomathi NS, Ganesh J, Aravind MA, et al. Plasma Matrix Metalloproteinases Signature as Biomarkers for Pediatric Tuberculosis Diagnosis: A Prospective Case–Control Study. Diseases. 2025; 13(6):171. https://doi.org/10.3390/diseases13060171
Chicago/Turabian StylePavan Kumar, Nathella, Syed Hissar, Arul Nancy, Kannan Thiruvengadam, Velayuthum V. Banurekha, Sarath Balaji, S. Elilarasi, N. S. Gomathi, J. Ganesh, M. A. Aravind, and et al. 2025. "Plasma Matrix Metalloproteinases Signature as Biomarkers for Pediatric Tuberculosis Diagnosis: A Prospective Case–Control Study" Diseases 13, no. 6: 171. https://doi.org/10.3390/diseases13060171
APA StylePavan Kumar, N., Hissar, S., Nancy, A., Thiruvengadam, K., Banurekha, V. V., Balaji, S., Elilarasi, S., Gomathi, N. S., Ganesh, J., Aravind, M. A., Baskaran, D., Swaminathan, S., & Babu, S. (2025). Plasma Matrix Metalloproteinases Signature as Biomarkers for Pediatric Tuberculosis Diagnosis: A Prospective Case–Control Study. Diseases, 13(6), 171. https://doi.org/10.3390/diseases13060171