
Long-Term Trends in Respiratory Syncytial Virus A Infections (2007–2024) in Korea


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Testing Process
2.4. Data Preprocessing
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
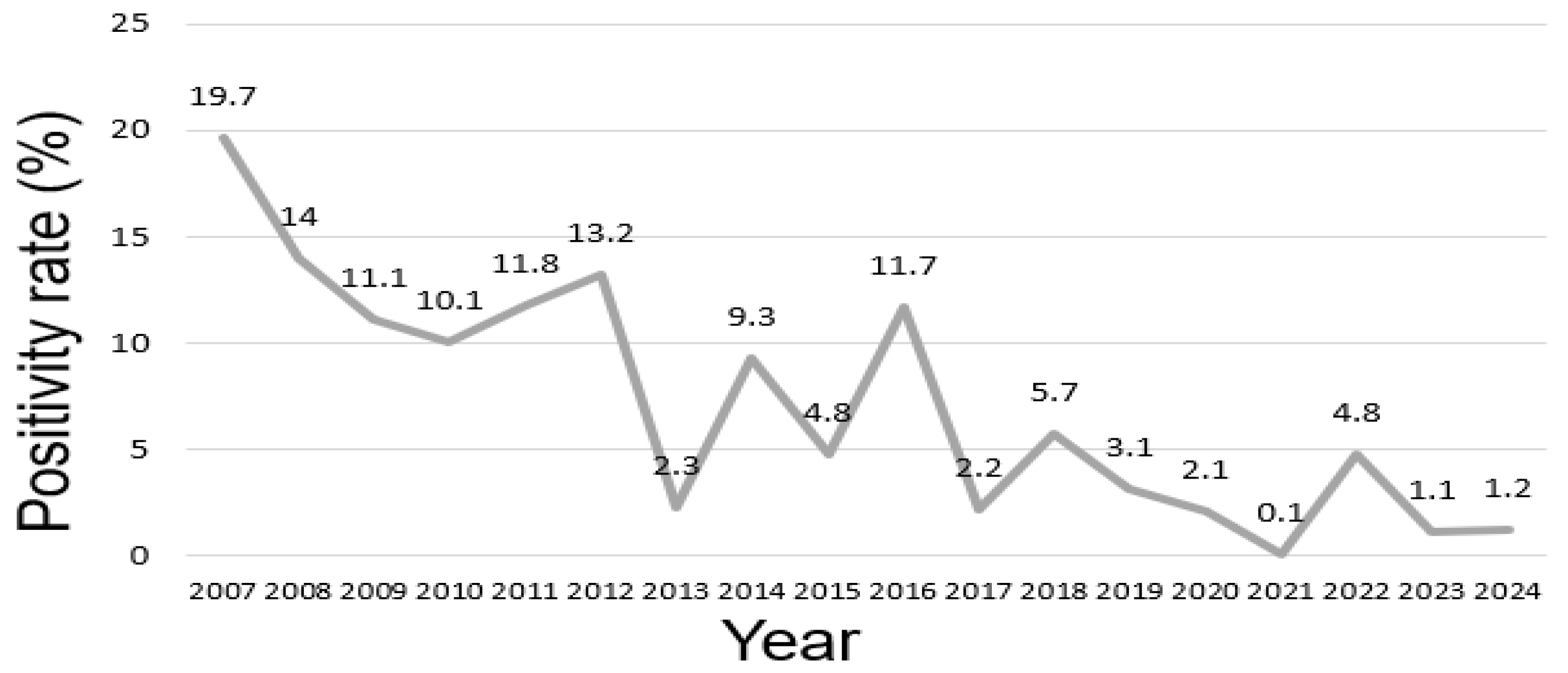
3.1. Annual Positivity Rate
3.2. Seasonal Positivity Rate
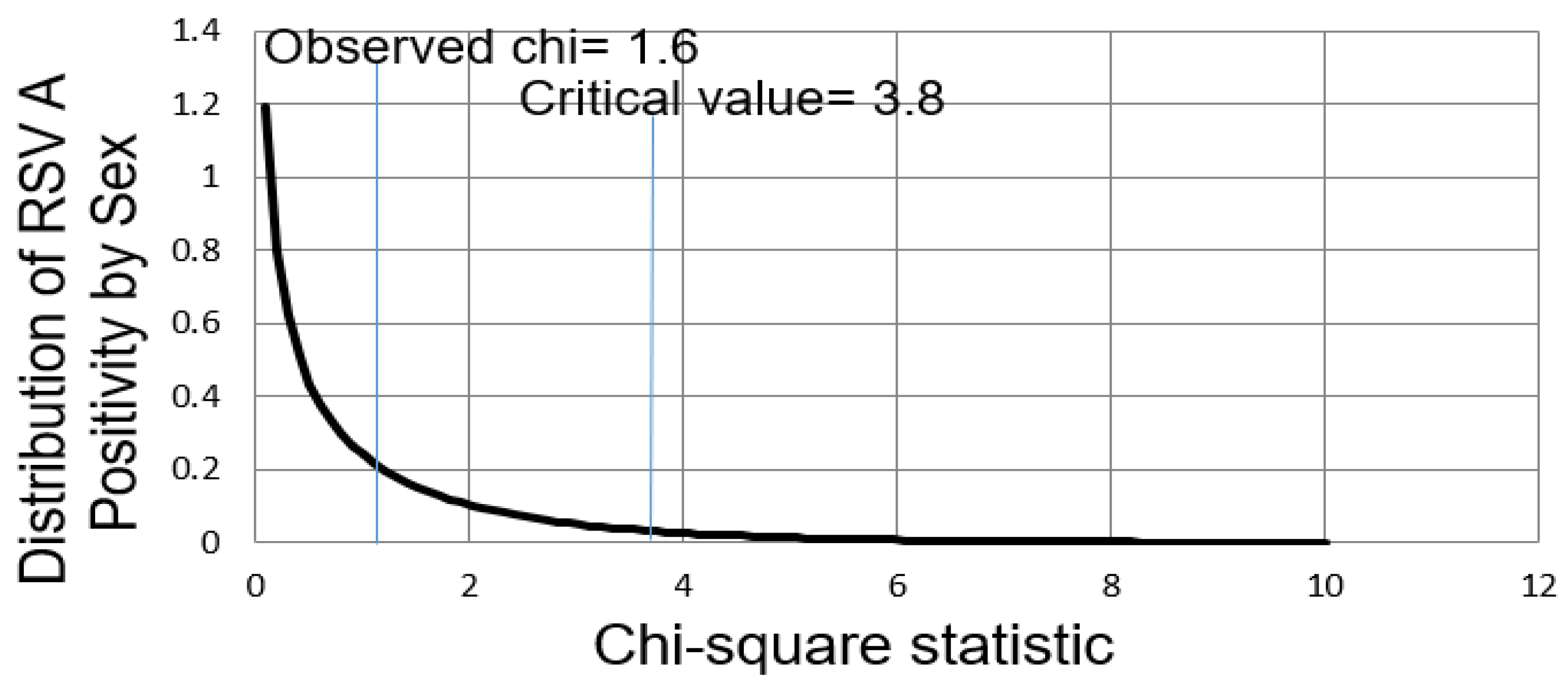
3.3. Positivity Rate by Sex
3.4. Positivity Rate by Age Group
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RSV | respiratory syncytial virus |
| RT-PCR | real-time polymerase chain reaction |
References
- Alfano, F.; Bigoni, T.; Caggiano, F.P.; Papi, A. Respiratory Syncytial Virus Infection in Older Adults: An Update. Drugs Aging 2024, 41, 487–505. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simoes, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Hanage, W.P.; Schaffner, W. Burden of Acute Respiratory Infections Caused by Influenza Virus, Respiratory Syncytial Virus, and SARS-CoV-2 with Consideration of Older Adults: A Narrative Review. Infect. Dis. Ther. 2025, 14, 5–37. [Google Scholar] [CrossRef]
- Nuttens, C.; Moyersoen, J.; Curcio, D.; Aponte-Torres, Z.; Baay, M.; Vroling, H.; Gessner, B.D.; Begier, E. Differences Between RSV A and RSV B Subgroups and Implications for Pharmaceutical Preventive Measures. Infect. Dis. Ther. 2024, 13, 1725–1742. [Google Scholar] [CrossRef] [PubMed]
- Langley, J.M.; Bianco, V.; Domachowske, J.B.; Madhi, S.A.; Stoszek, S.K.; Zaman, K.; Bueso, A.; Ceballos, A.; Cousin, L.; D’Andrea, U.; et al. Incidence of Respiratory Syncytial Virus Lower Respiratory Tract Infections During the First 2 Years of Life: A Prospective Study Across Diverse Global Settings. J. Infect. Dis. 2022, 226, 374–385. [Google Scholar] [CrossRef]
- Wrotek, A.; Kobialka, M.; Grochowski, B.; Kaminska, I.; Pedziwiatr, K.; Skoczek-Wojciechowska, A.; Godek, M.; Jackowska, T. Respiratory Complications in Children Hospitalized with Respiratory Syncytial Virus Infection. Adv. Exp. Med. Biol. 2020, 1279, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Zar, H.J.; Cacho, F.; Kootbodien, T.; Mejias, A.; Ortiz, J.R.; Stein, R.T.; Hartert, T.V. Early-life respiratory syncytial virus disease and long-term respiratory health. Lancet Respir. Med. 2024, 12, 810–821. [Google Scholar] [CrossRef]
- Barbati, F.; Moriondo, M.; Pisano, L.; Calistri, E.; Lodi, L.; Ricci, S.; Giovannini, M.; Canessa, C.; Indolfi, G.; Azzari, C. Epidemiology of Respiratory Syncytial Virus-Related Hospitalization Over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution Before Vaccine Introduction. Vaccines 2020, 8, 15. [Google Scholar] [CrossRef]
- Chadha, M.; Hirve, S.; Bancej, C.; Barr, I.; Baumeister, E.; Caetano, B.; Chittaganpitch, M.; Darmaa, B.; Ellis, J.; Fasce, R.; et al. Human respiratory syncytial virus and influenza seasonality patterns-Early findings from the WHO global respiratory syncytial virus surveillance. Influenza Other Respir. Viruses 2020, 14, 638–646. [Google Scholar] [CrossRef]
- Chuang, Y.C.; Lin, K.P.; Wang, L.A.; Yeh, T.K.; Liu, P.Y. The Impact of the COVID-19 Pandemic on Respiratory Syncytial Virus Infection: A Narrative Review. Infect. Drug Resist. 2023, 16, 661–675. [Google Scholar] [CrossRef]
- Stein, R.T.; Zar, H.J. RSV through the COVID-19 pandemic: Burden, shifting epidemiology, and implications for the future. Pediatr. Pulmonol. 2023, 58, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hodgson, D.; Wang, X.; Atkins, K.E.; Feikin, D.R.; Nair, H. Respiratory syncytial virus seasonality and prevention strategy planning for passive immunisation of infants in low-income and middle-income countries: A modelling study. Lancet Infect. Dis. 2021, 21, 1303–1312. [Google Scholar] [CrossRef]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Checcucci Lisi, G.; et al. Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef]
- Fourgeaud, J.; Toubiana, J.; Chappuy, H.; Delacourt, C.; Moulin, F.; Parize, P.; Scemla, A.; Abid, H.; Leruez-Ville, M.; Frange, P. Impact of public health measures on the post-COVID-19 respiratory syncytial virus epidemics in France. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2389–2395. [Google Scholar] [CrossRef]
- Britton, P.N.; Hu, N.; Saravanos, G.; Shrapnel, J.; Davis, J.; Snelling, T.; Dalby-Payne, J.; Kesson, A.M.; Wood, N.; Macartney, K.; et al. COVID-19 public health measures and respiratory syncytial virus. Lancet Child. Adolesc. Health 2020, 4, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Arango-Franco, C.A.; Feng, G.; Shen, K.; Xu, B. Upsurge of acute respiratory infections among children post-COVID-19 pandemic. Innov. Med. 2024, 2, 100070. [Google Scholar] [CrossRef]
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Cereda, D.; Anselmi, G.; Binda, S.; Gramegna, M.; Pariani, E. Respiratory syncytial virus in influenza-like illness cases: Epidemiology and molecular analyses of four consecutive winter seasons (2014-2015/2017-2018) in Lombardy (Northern Italy). J. Med. Virol. 2020, 92, 2999–3006. [Google Scholar] [CrossRef]
- Wang, S.; Wang, Y.; Zou, Y.; Yin, C.L. Relationship between RSV-hospitalized children and meteorological factors: A time series analysis from 2017 to 2023. Biomed. Eng. Online 2025, 24, 10. [Google Scholar] [CrossRef]
- Hamid, S.; Winn, A.; Parikh, R.; Jones, J.M.; McMorrow, M.; Prill, M.M.; Silk, B.J.; Scobie, H.M.; Hall, A.J. Seasonality of Respiratory Syncytial Virus—United States, 2017–2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 355–361. [Google Scholar] [CrossRef]
- Pasanen, T.P.; Kajosaari, A. Special Issue: Place, Space, and Mental Health. Int. J. Environ. Res. Public Health 2023, 20, 5055. [Google Scholar] [CrossRef]
- Ren, S.; Chen, Q.; Zhang, Y.; Yi, L.; Qian, C.; Lu, Y.; Shen, J.; Liu, X.; Jiang, M.; Wang, B.; et al. Modeling the optimal seasonal monoclonal antibody administration strategy for respiratory syncytial virus (RSV) prevention based on age-season specific hospitalization rate of RSV in Suzhou, China, 2016–2022. Vaccine 2024, 42, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.; Koltai, M.; Krauer, F.; Flasche, S.; Jit, M.; Atkins, K.E. Optimal Respiratory Syncytial Virus intervention programmes using Nirsevimab in England and Wales. Vaccine 2022, 40, 7151–7157. [Google Scholar] [CrossRef]
- Ursin, R.L.; Klein, S.L. Sex Differences in Respiratory Viral Pathogenesis and Treatments. Annu. Rev. Virol. 2021, 8, 393–414. [Google Scholar] [CrossRef]
- Ramzali, M.; Salimi, V.; Cheraghali, F.; Hosseini, S.D.; Yasaghi, M.; Samadizadeh, S.; Rastegar, M.; Nakstad, B.; Tahamtan, A. Epidemiology and clinical features of respiratory syncytial virus (RSV) infection in hospitalized children during the COVID-19 pandemic in Gorgan, Iran. Health Sci. Rep. 2024, 7, e1787. [Google Scholar] [CrossRef]
- Redondo, E.; Rivero-Calle, I.; Mascaros, E.; Ocana, D.; Jimeno, I.; Gil, A.; Linares, M.; Onieva-Garcia, M.A.; Gonzalez-Romo, F.; Yuste, J.; et al. Respiratory Syncytial Virus Vaccination Recommendations for Adults Aged 60 Years and Older: The NeumoExperts Prevention Group Position Paper. Arch. Bronconeumol. 2024, 60, 161–170. [Google Scholar] [CrossRef]
- Parsons, E.L.; Kim, J.S.; Malloy, A.M.W. Development of innate and adaptive immunity to RSV in young children. Cell Immunol. 2024, 399–400, 104824. [Google Scholar] [CrossRef] [PubMed]
- Stambas, J.; Lu, C.; Tripp, R.A. Innate and adaptive immune responses in respiratory virus infection: Implications for the clinic. Expert Rev. Respir. Med. 2020, 14, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Mei, C.; Chen, S.; Wang, C.; Gao, Y.; Ma, J.; Zhong, L.; Luo, T.; Zhao, X.; Bu, H.; et al. Protective or limited? Maternal antibodies and RSV-associated lower respiratory tract infection in hospitalized infants aged 28–90 days. Front. Immunol. 2024, 15, 1437616. [Google Scholar] [CrossRef]
- Chedid, K.; Arts, P.; Blair, C.; Hashikawa, A.; Clack, H.; Wigginton, K.; Lauring, A.S.; Marr, L.; Prussin, A.; Lakdawala, S.; et al. 890. Environmental Air and Surface Sampling of Respiratory Viruses in Child Care Centers. Open Forum Infect. Dis. 2023, 10, 500–935. [Google Scholar] [CrossRef]
- Walsh, E.; Lee, N.; Sander, I.; Stolper, R.; Zakar, J.; Wyffels, V.; Myers, D.; Fleischhackl, R. RSV-associated hospitalization in adults in the USA: A retrospective chart review investigating burden, management strategies, and outcomes. Health Sci. Rep. 2022, 5, e556. [Google Scholar] [CrossRef]
- Tseng, H.F.; Sy, L.S.; Ackerson, B.; Solano, Z.; Slezak, J.; Luo, Y.; Fischetti, C.A.; Shinde, V. Severe Morbidity and Short- and Mid- to Long-term Mortality in Older Adults Hospitalized with Respiratory Syncytial Virus Infection. J. Infect. Dis. 2020, 222, 1298–1310. [Google Scholar] [CrossRef] [PubMed]
- Zhi, W.; Xu, Q.; Chen, Z.; Jiang, W.; Wang, T.; Zhou, Y.; Yu, H.; Yan, Y.; Pan, T. Respiratory syncytial virus infection in children and its correlation with climatic and environmental factors. J. Int. Med. Res. 2021, 49, 3000605211044593. [Google Scholar] [CrossRef] [PubMed]
- Rios-Guzman, E.; Simons, L.M.; Dean, T.J.; Agnes, F.; Pawlowski, A.; Alisoltanidehkordi, A.; Nam, H.H.; Ison, M.G.; Ozer, E.A.; Lorenzo-Redondo, R.; et al. Deviations in RSV epidemiological patterns and population structures in the United States following the COVID-19 pandemic. Nat. Commun. 2024, 15, 3374. [Google Scholar] [CrossRef]
- Loaiza-Ceballos, M.C.; Marin-Palma, D.; Zapata, W.; Hernandez, J.C. Viral respiratory infections and air pollutants. Air Qual. Atmos. Health 2022, 15, 105–114. [Google Scholar] [CrossRef]
- Manti, S.; Piedimonte, G. An overview on the RSV-mediated mechanisms in the onset of non-allergic asthma. Front. Pediatr. 2022, 10, 998296. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Season | Total | Positive | Negative | Positivity Rate (%) |
|---|---|---|---|---|
| Spring | 6391 | 189 | 6202 | 2.9 |
| Summer | 4810 | 41 | 4769 | 0.8 |
| Autumn | 5607 | 719 | 4888 | 14.7 |
| Winter | 6476 | 862 | 5614 | 15.3 |
| Season | Positive Expected | Negative Expected |
|---|---|---|
| Spring | 14.5 | 6376.5 |
| Summer | 3.1 | 4806.9 |
| Autumn | 55.3 | 5551.7 |
| Winter | 66.3 | 6409.7 |
| Sex | Total | Positive | Negative | Positivity Rate (%) |
|---|---|---|---|---|
| Male | 13,961 | 1060 | 12,901 | 7.5 |
| Female | 9323 | 751 | 8572 | 8.0 |
| Age Group | Total | Positive | Negative | Positivity Rate (%) |
|---|---|---|---|---|
| Infants (0 years) | 4556 | 846 | 3710 | 18.5 |
| Children (1–19 years) | 11,137 | 896 | 10,241 | 8.0 |
| Adults (20–64 years) | 2899 | 23 | 2876 | 0.7 |
| Older adults (≥65 years) | 4692 | 46 | 4646 | 0.9 |
| Age Group | Positive (Expected) | Negative (Expected) |
|---|---|---|
| Infants (0 years) | 354.3 | 4201.6 |
| Children (1–19 years) | 886.2 | 10,270.7 |
| Adults (20–64 years) | 225.4 | 2673.5 |
| Older adults (≥65 years) | 364.9 | 4327.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.S.; Jang, S.H.; Jeon, J.-S.; Kim, J.K. Long-Term Trends in Respiratory Syncytial Virus A Infections (2007–2024) in Korea. Diseases 2025, 13, 147. https://doi.org/10.3390/diseases13050147
Han JS, Jang SH, Jeon J-S, Kim JK. Long-Term Trends in Respiratory Syncytial Virus A Infections (2007–2024) in Korea. Diseases. 2025; 13(5):147. https://doi.org/10.3390/diseases13050147
Chicago/Turabian StyleHan, Jeong Su, Sung Hun Jang, Jae-Sik Jeon, and Jae Kyung Kim. 2025. "Long-Term Trends in Respiratory Syncytial Virus A Infections (2007–2024) in Korea" Diseases 13, no. 5: 147. https://doi.org/10.3390/diseases13050147
APA StyleHan, J. S., Jang, S. H., Jeon, J.-S., & Kim, J. K. (2025). Long-Term Trends in Respiratory Syncytial Virus A Infections (2007–2024) in Korea. Diseases, 13(5), 147. https://doi.org/10.3390/diseases13050147